
Abstract
Objective:
To examine the prevalence and characteristics of pregnant women with borderline personality pathology (defined as borderline personality disorder and borderline personality traits) referred to a perinatal consultation-liaison psychiatry service.
Method:
Socio-demographic and clinical data, and diagnoses made according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.) criteria were recorded for all women referred to and seen by the perinatal consultation-liaison psychiatry service over an 18-month period. Data were analysed using descriptive statistics and logistic regression analysis.
Results:
A total of 318 women were seen. The most common diagnoses found were depressive disorder (25.5%) and anxiety disorder (15.1%). Borderline personality disorder was found in 10.1% of women and almost one in five women had two or more borderline personality traits (19.5%). When compared to women with other diagnoses, women with borderline personality pathology had higher rates of unplanned pregnancy, being unpartnered, substance use during pregnancy and higher rates of child safety services involvement as a child or in a previous pregnancy. Over 40% of women with borderline personality pathology were referred to child safety services in the current pregnancy and a diagnosis of borderline personality pathology increased the risk of child safety services involvement by almost sixfold (odds ratio: 5.5; 95% confidence interval = [1.50, 20.17]).
Conclusion:
The prevalence of borderline personality pathology in antenatal women identified at antenatal screening and the recognition that women with borderline personality pathology are ‘high-risk’ caregivers argue for borderline personality pathology to be recognised as a high priority for investment in service development.
Introduction
Over the past two decades, there has been increasing recognition of the importance of the perinatal period and infancy for development of neurological and psychological capacities and for functioning in later life. The quality of the caregiver–infant relationship and interactions within this context, as well as presence or absence of adverse influences in utero, are critically important in determining neurological, psychological and social development and long-term mental well-being (Dvir et al., 2014; Newman et al., 2016; Schore, 1996). It is well recognised that distortions of early experiences, such as insecure or disorganised attachment, insensitive interactions, neglect and trauma, may adversely impact development (Lyons-Ruth et al., 1993). Particular interest has focused on disorganised infant attachment, which may develop as a result of frightening, frightened and dissociative parental behaviours, repeated absences or maltreatment (Granqvist et al., 2017).
Attachment research is exploring a model of ‘transgenerational transmission’ of attachment disturbance in which parents who have experienced early adversity may develop difficulties with respect to recognising and responding to their infant’s needs and are therefore at risk of repeating parenting disturbances (Holmes, 1999; Newman and Stevenson, 2005, 2008). This transgenerational framework has contributed to current understanding about the repetition of dysfunctional relationship patterns, such as child abuse and disturbances of attachment across generations (Berthelot et al., 2015; Newcomb and Locke, 2001), and has broadened the understanding of early difficulties in parenting.
This research supports the proposal that increased efforts should focus on identifying and working with ‘high-risk’ caregivers, that is, caregivers who are likely to have more complex difficulties, such as attachment and relationship difficulties with their infant (Judd et al., 2018). One group identified as ‘high-risk’ caregivers are women with borderline personality pathology (BPP), who have frequently experienced early trauma and disorganised attachment with resulting personality dysfunction and parenting identity disturbances, often complicated by co-morbid substance use, depression and anxiety (Chlebowski, 2013; Tomko et al., 2014; Zanarini, 2000).
BPP encompasses both borderline personality disorder (BPD), a serious disturbance of personality functioning characterised by affective instability and emotional dysregulation, identity disturbance, poor impulse control and difficulties in interpersonal functioning (American Psychiatric Association, 2013), and subthreshold borderline personality symptoms or traits. Making a diagnosis of BPD can be challenging due to the heterogeneity of the condition and concerns about appropriate thresholds (Leichsenring et al., 2011; Widiger, 1992). There is evidence that even subthreshold BPD features are clinically significant and that early intervention programmes should have broad inclusion criteria (Chanen and McCutcheon, 2013; Zimmerman et al., 2012). Some clinicians and researchers therefore prefer a dimensional approach to conceptualising BPD (Trull et al., 1990) and inclusion of subclinical BPD symptoms, as captured by BPP (Eyden et al., 2016).
Newman et al, (2011) proposed BPD as a model of disturbed parenting, referring to possible neurodevelopmental effects of early childhood trauma seen in adults with BPD. Affect dysregulation and deficits in socio-emotional processing have been recognised as key elements relating to parenting difficulties in these individuals (Newman et al., 2011).
Consistent with the proposed transgenerational transmission of attachment disturbance, exploration of interactional patterns between women with BPD and their infants has found these mothers show disrupted affective communication with their infants, are less sensitive in interactions with their infant and more likely to engage in maladaptive interactions with their children (Eyden et al., 2016; Hobson et al., 2009; Newman et al., 2007).
Studies demonstrate offspring of women with BPP may be at risk of negative outcomes across a wide range of domains throughout different developmental stages. There are associations between maternal BPD and higher prevalence of psychiatric disorders in offspring (Weiss et al., 1996), as well as difficulties with psychosocial functioning later in life (Herr et al., 2008). Subclinical levels of parental personality disorder also predict symptoms of behavioural and emotional diagnoses in the children (Berg-Nielsen and Wichstrom, 2012). Barnow et al. (2013) found maternal BPD, as well as subthreshold BPD symptoms, predicted offspring BPD symptoms in adolescence and early adulthood, again supporting the theory of a transgenerational transmission.
The difficulties and risk experienced by offspring of women with BPP may relate not only to the emotional interactions in the mother–infant relationship but also to adverse influences in utero and postnatally, such as exposure to maternal substance use, maternal stress and domestic violence. In a retrospective case review, Blankley et al. (2015) found women with BPD had high rates of co-morbid substance use in the perinatal period and the overall perinatal experiences of these women were rated as more distressing than in the control group. These findings confirm that ‘high-risk’ caregivers experience significant challenges, which may harbour the potential for child maltreatment in the form of neglect, rejection or physical abuse (Newman et al., 2007).
Despite emerging recognition that women with BPP are one group of ‘high-risk’ caregivers, there is little data available regarding child safety services (CSS) involvement in mothers with BPP. Existing data indicates relatively high rates; Blankley et al. (2015) found over 50% of women with BPD, who were referred to a perinatal psychiatric service and examined in a retrospective case review study, were referred to CSS. A retrospective cohort study by O’Donnell et al. (2015) found a diagnosis of personality disorder, among other psychiatric diagnoses, was a risk factor for child maltreatment allegations. In a Canadian study, Laporte and colleagues surveyed 291 caseworkers working with mothers whose children were involved with CSS and found the prevalence of maternal BPD was 34.3%. In addition, 48.9% of mothers with BPD had a history of CSS involvement in their own childhood (Laporte et al., 2018). In a cohort study, Perepletchikova and colleagues examined the history of childhood maltreatment and BPD in mothers whose children were removed from home by CSS and compared them to community controls without CSS involvement. The findings showed that 50% of mothers with CSS involvement self-reported elevated BPD features compared with only 15% of the controls. Furthermore, mothers involved with CSS scored significantly higher on measures of self-reported childhood maltreatment history than the controls (Perepletchikova et al., 2012).
This study sought to add to existing literature regarding women with BPP in the perinatal period. Consistent with previous research, the study included both women with BPD and those with borderline personality traits – here summarised as BPP.
Aims
The aims of this study were to examine the prevalence and characteristics of pregnant women with BPP (defined as BPD and borderline personality traits), including frequency of CSS involvement in this patient group, among pregnant women referred to a perinatal consultation-liaison psychiatry service.
Method
Setting
This study was undertaken through the perinatal consultation-liaison psychiatry (PCLP) service of The Royal Hobart Hospital (RHH). The RHH services a population of over 250,000 people, and within the maternity service there are approximately 2000 deliveries per year. Women attending the maternity service are offered routine antenatal screening using the Edinburgh Postnatal Depression Scale (EPDS) at the antenatal booking-in visit. All women are also asked a series of questions about their current and past mental health and psychosocial circumstances. This practice is in accordance with the current Clinical Practice Guideline for Mental Health Care in the Perinatal Period (Austin et al., 2017).
Participants
Study participants were all women who were referred in the antenatal period and who were seen by the PCLP team over an 18-month period. Women routinely referred to the PCLP service were those who scored ⩾13 on the EPDS; women who had a known or self-reported past history and/or current diagnosis of depression, anxiety, personality disorder or major mental illness, such as bipolar disorder or schizophrenia; and women currently prescribed psychotropic medications.
Procedure
All women were seen for assessment by the consultant psychiatrist or psychiatric registrar. The assessment included a clinical diagnostic interview and review of past psychiatric history. Following the initial assessment, women continued to be seen as frequently as clinically indicated.
Socio-demographic data collected included age and relationship status. It was also recorded whether the pregnancy was planned or unplanned, and whether there had been any previous involvement with CSS either as a child or in previous pregnancies.
Following the clinical interview, diagnoses were made according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria (American Psychiatric Association, 2013). Of note, when present, both personality disorder and clinically significant personality traits were recorded.
Statistical analysis
Descriptive statistics were used to analyse the socio-demographic and clinical characteristics of the sample. A hierarchical binary logistic regression was performed, looking at the impact of various risk factors as dependent variables that together might predict notification to CSS in the current pregnancy. Predictor variables entered initially were age, unplanned pregnancy, being unpartnered, CSS involvement as a child, CSS involvement in previous pregnancy and DSM-5 (American Psychiatric Association, 2013) diagnosis (substance use disorder, anxiety disorder, depressive disorder and ‘other’ DSM-5 (American Psychiatric Association, 2013) diagnoses, except BPD and borderline personality traits). These predictors were entered into the equation simultaneously to determine the influence of predictor variables in the presence of other variables. BPP was entered in a second step to look at the effect of BPP adjusted for the confounding role of the other variables.
Ethics
Approval for the study was granted by the University of Tasmania Human Research Ethics Committee.
Results
Over the study period, 459 women were referred to the service. Of these, 318 (69.3%) were seen for assessment, and 141 (30.7%) declined the offered appointment or did not attend a scheduled appointment.
Socio-demographic and clinical characteristics of the total sample
Characteristics of the women involved in the study are presented in Table 1. The mean age was 27.5 years with a range between 13 and 43 years. Almost two-thirds of pregnancies were unplanned (n = 193; 60.7%) and a significant number of women were unpartnered (n = 58; 18.2%). Substance use in pregnancy was substantial with 43 women (13.5%) describing any substance use; cannabis was most commonly used (n = 28; 8.8%), followed by alcohol (n = 14; 4.4%). Relatively high rates of CSS notification for the current pregnancy were found (n = 53; 16.7%), and 37 women (11.6%) had been involved with CSS as a child.
Sample characteristics.
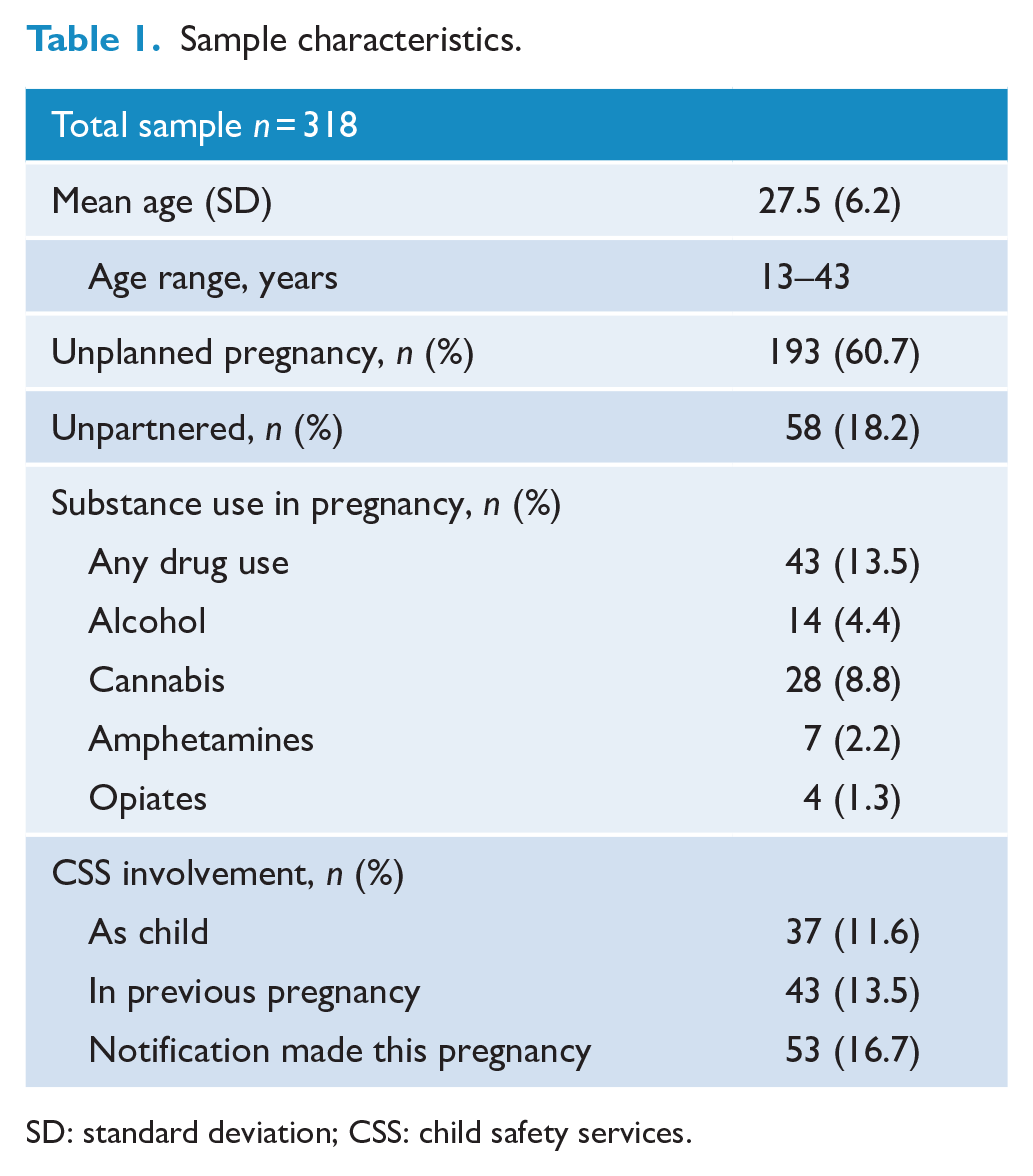
SD: standard deviation; CSS: child safety services.
Reasons for referral
The reasons for referral for the total sample are shown in Table 2. The main reason for referral was past anxiety or depression (n = 153; 48.1%), followed by an elevated EPDS score (n = 117; 36.8%) and current symptoms of anxiety or depression (n = 80; 25.2%). Of note, only a very small number of women were referred for personality issues or aggression (n = 4; 1.3%). Frequently more than one reason was given for referral; therefore, the total number of reasons for referral was larger than the total sample size.
Reason for referral.
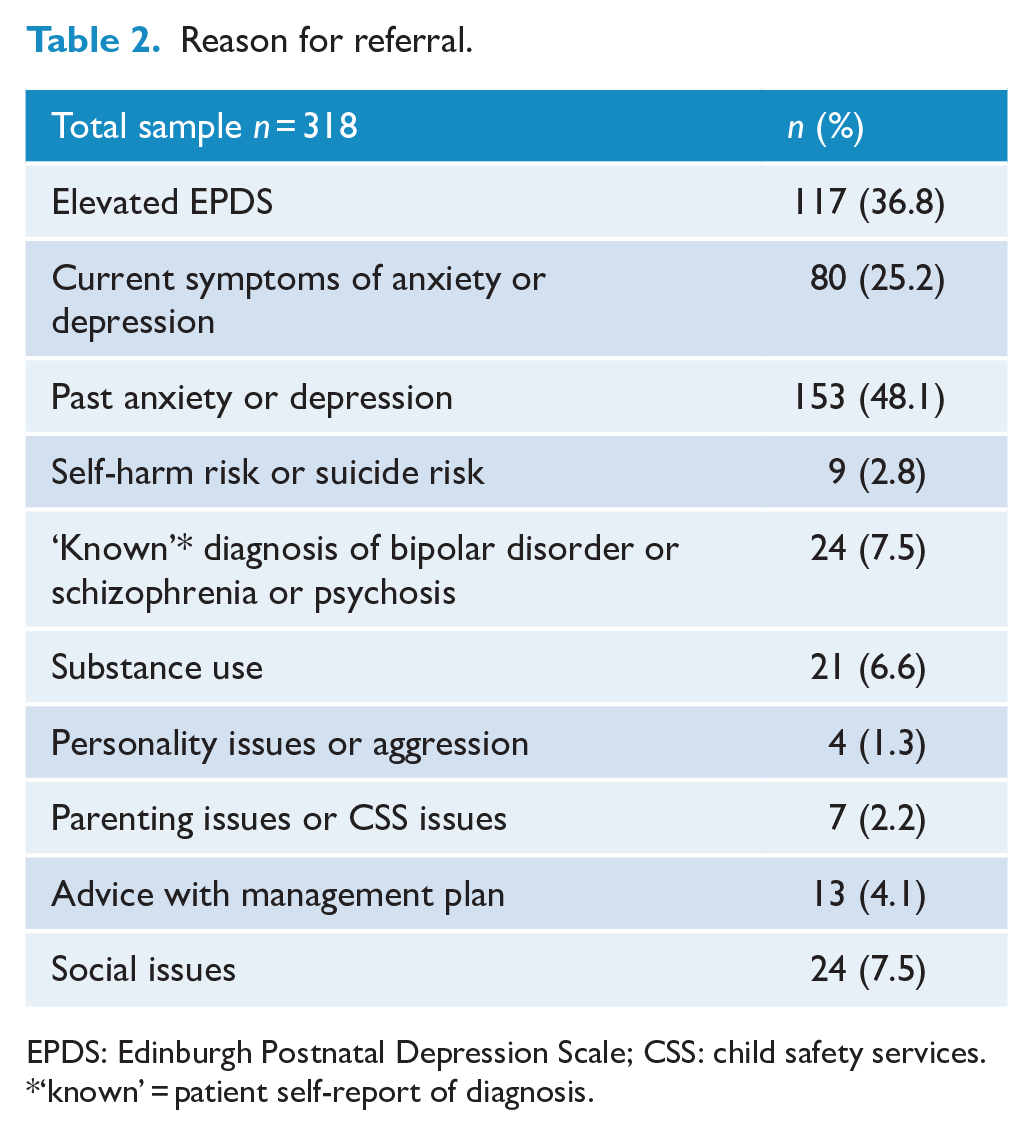
EPDS: Edinburgh Postnatal Depression Scale; CSS: child safety services.
‘known’ = patient self-report of diagnosis.
Diagnoses
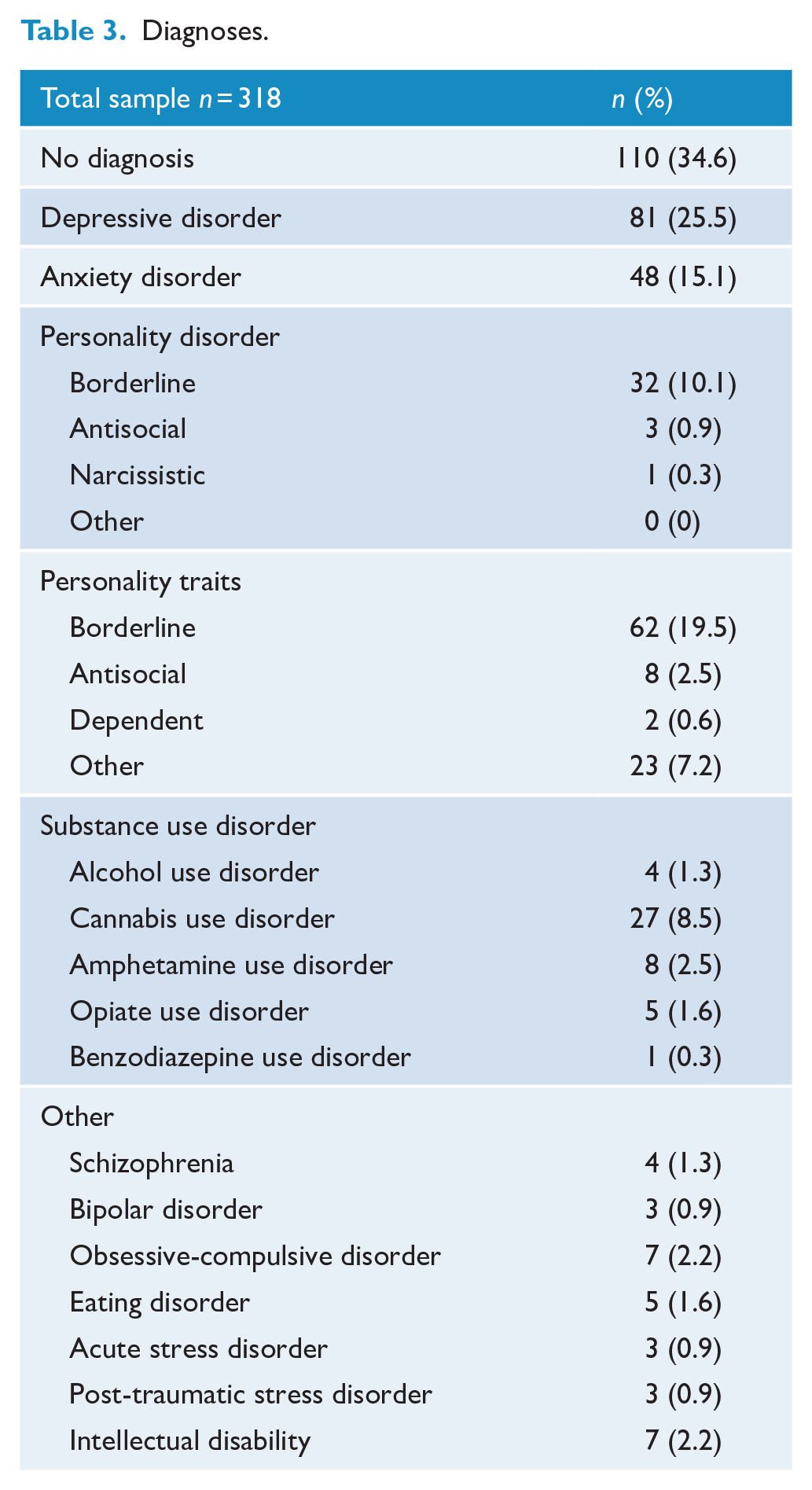
Approximately one-third of women (n = 110; 34.6%) were found to have no diagnosis (Table 3). One-third of this group were women with an EPDS ⩾ 13, who were ‘false positives’, the remainder were predominantly women referred because they reported a past history of anxiety/depression but who had no current disorder. A quarter (n = 81; 25.5%) of the women had a depressive disorder and 48 women (15.1%) had an anxiety disorder. A substantial number of women were found to have BPD (n = 32; 10.1%), and almost one in five women had clinically significant borderline personality traits (n = 62; 19.5%). The latter were noted in the list of diagnoses if two or more traits were present, most commonly affective instability and inappropriate intense anger. Comorbidity was common and so the total number of diagnoses exceeded the number of patients.
Diagnoses.
Socio-demographic and clinical characteristics of women with BPP versus no BPP
Table 4 compares socio-demographic and clinical characteristics of women with BPD, borderline personality traits, BPP and no BPP in separate columns. BPP (n = 94; 29.6%) is the sum of BPD and borderline personality traits. There were no major differences in age between the groups. A higher percentage of women with BPP had an unplanned pregnancy compared to women without BPP (77.7% vs 53.6%). The rate of being unpartnered was slightly lower in the no BPP group compared to the other three groups.
Sample characteristics by group.
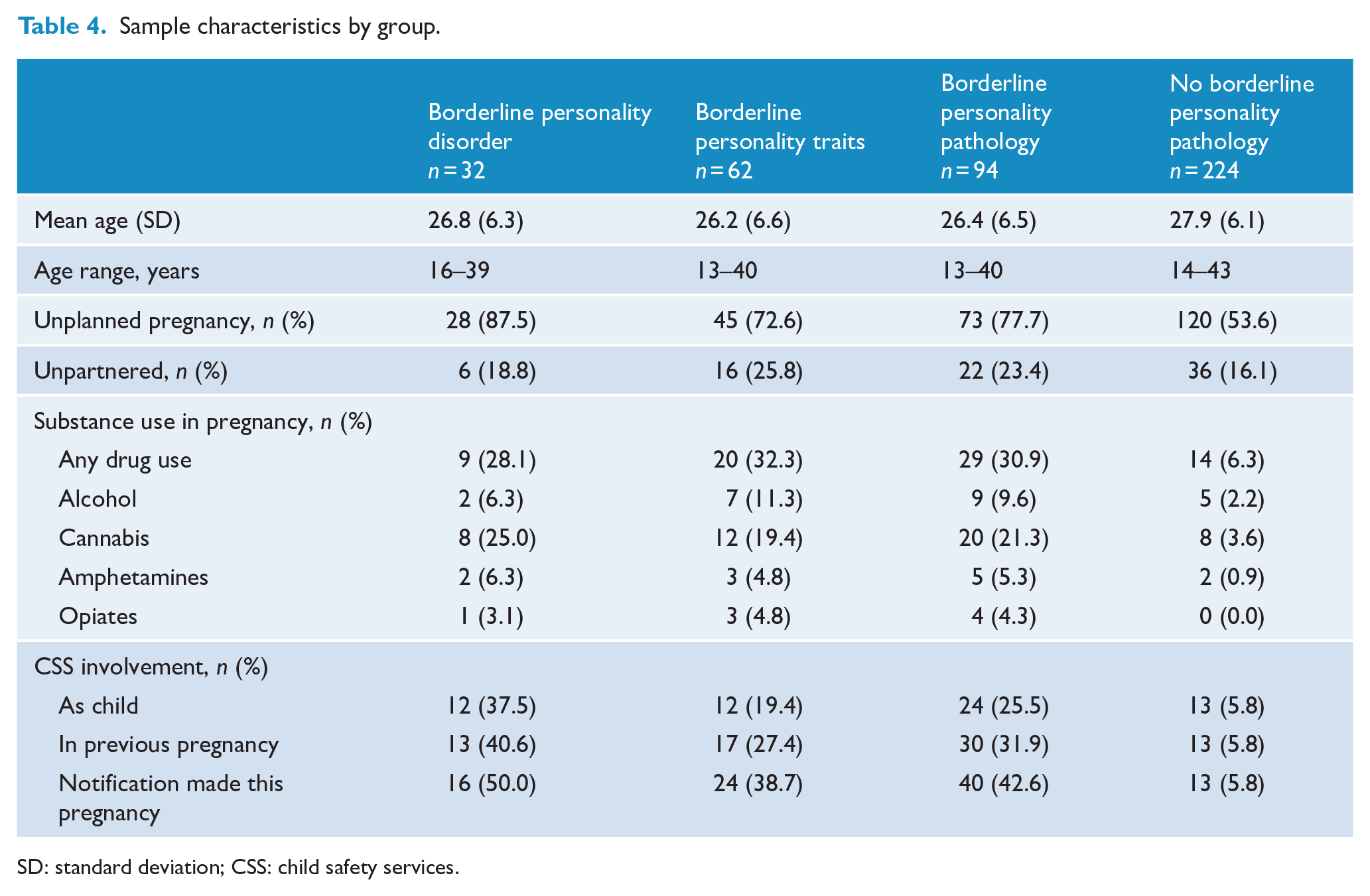
SD: standard deviation; CSS: child safety services.
Women with BPP consistently had a higher percentage of substance use during pregnancy; the difference was particularly marked when comparing cannabis use in women with BPP to women with no BPP (21.3% vs 3.6%).
CSS involvement was more common in women with BPP. A quarter of the women with BPP had CSS involvement as a child (25.5%) versus 5.8% of women with no BPP. Almost a third of women with BPP had a CSS notification made in a previous pregnancy (31.9%) and 42.6% were notified to CSS in the current pregnancy. Women with no BPP only had a notification made in 5.8% of both cases. Women who had a diagnosis of BPD were notified to CSS in 50% of cases.
Likelihood of CSS notification in current pregnancy (BPP vs no BPP)
Results of the hierarchical binary logistic regression analysis, performed to examine the influence of identified risk factors to predict CSS notification in the current pregnancy, are displayed in Table 5. After accounting for all the variables in the equation, factors that were independent predictors of CSS notification were involvement with CSS as a child, CSS notification in a previous pregnancy, substance use disorder, ‘other’ DSM-5 (American Psychiatric Association, 2013) diagnoses and BPP. BPP was responsible for an almost sixfold increase in risk of notification to CSS (odds ratio [OR] = 5.5; 95% confidence interval [CI] = [1.50, 20.17]). Overall, the model accounted for 70.5% of the variance (Nagelkerke R2). The full model was a good fit (Hosmer and Lemeshow p = 0.887).
Hierarchical binary logistic regression.
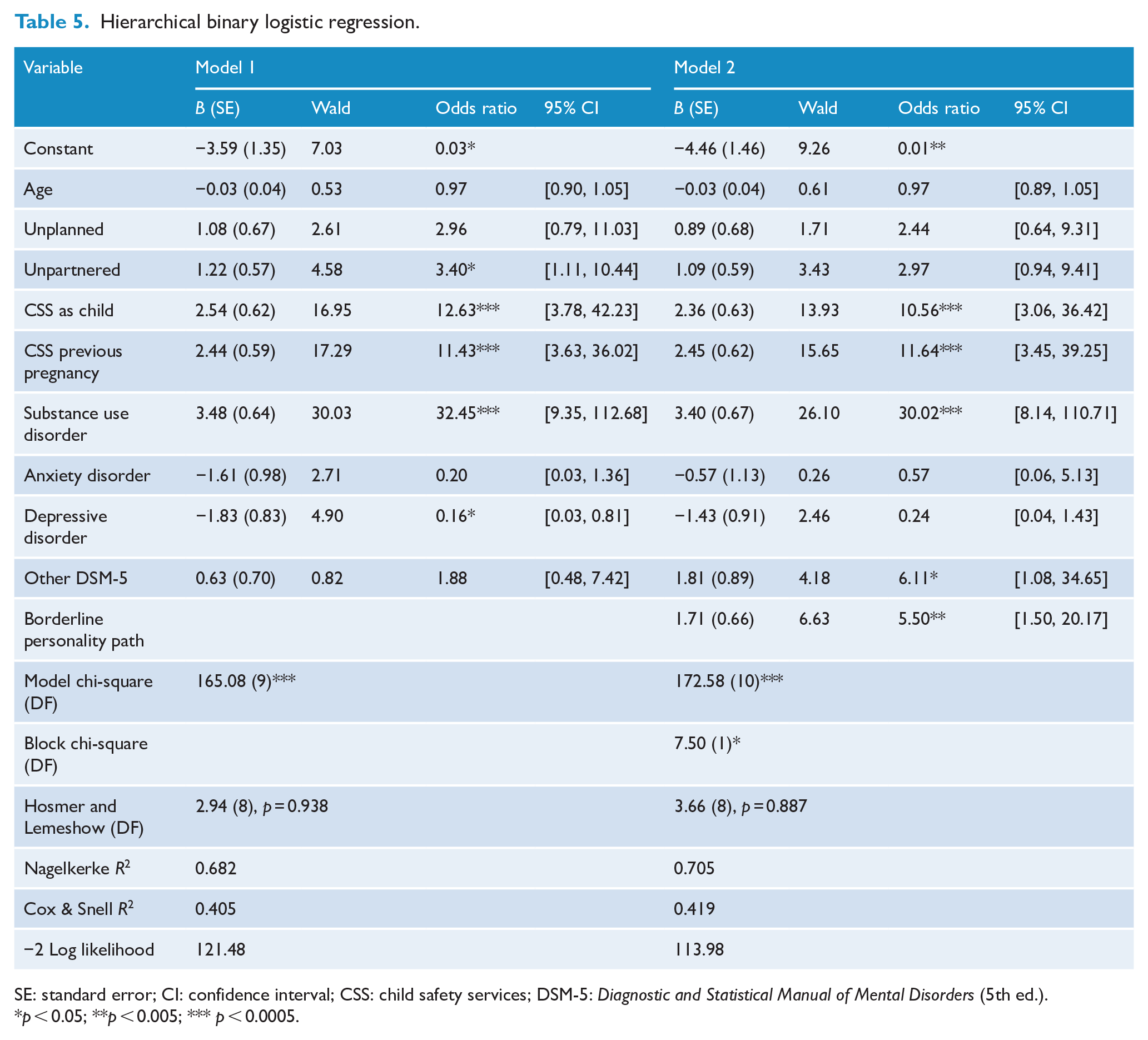
SE: standard error; CI: confidence interval; CSS: child safety services; DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.).
p < 0.05; **p < 0.005; *** p < 0.0005.
Discussion
This study sought to expand the existing literature around BPP in the perinatal period by examining prevalence and characteristics of pregnant women with BPP referred to a PCLP service.
The rate of BPD found (10.1%) is between general population rates and psychiatric outpatient rates (Korzekwa et al., 2008; National Health and Medical Research Council, 2012). In addition, clinically significant borderline personality traits were identified in 19.5% of women; therefore, almost one-third of women referred to the service were found to have BPP. Several studies examining postnatal women referred to Mother-Baby-Units found higher rates of BPD than in this study (Nair et al., 2010; Yelland et al., 2015), which is to be expected, as these populations would likely include a higher percentage of women with acute psychiatric illness, whereas the sample of this study was derived largely through routine antenatal screening.
Of note were the socio-demographic characteristics of the sample. There were high rates of unplanned pregnancy in women with BPP (77.7%), whereas the rates for women without BPP (53.6%) were closer to general population rates of approximately 50% (Sved Williams, 2019).
The study also found that women with BPP had higher rates of being unpartnered, compared with other women referred to the service. These findings are not surprising, considering problems with interpersonal relationships are a central aspect of BPP. This may make women with BPP more vulnerable to lacking emotional and social supports and may exacerbate parenting difficulties.
Substance use during pregnancy was common, with higher rates in women with BPP compared to women without BPP (30.9% vs 6.3%), reflecting established associations between BPP and substance use (Leichsenring et al., 2011; Nair et al., 2010; Tomko et al., 2014). Cannabis was the most commonly used substance, followed by alcohol. The rate of cannabis use by women with BPP during pregnancy (21.3%) was more than twice the rate of recent use in the general population (Australian Government Department of Health, 2019).
CSS involvement in the current pregnancy or in previous pregnancies was considerably higher in women with BPP and over 40% were notified to CSS in the current pregnancy. BPP alone increased the risk of CSS notification by almost sixfold. Several other studies have shown equally high rates of CSS involvement (Blankley et al., 2015; Laporte et al., 2018).
A quarter of women with BPP had CSS involvement in their childhood, with the rate being greater in those with BPD. These findings are consistent with previous research, which has demonstrated higher rates of abuse and neglect in individuals with BPD (Laporte et al., 2018; Perepletchikova et al., 2012). Children who experience maltreatment, abuse and neglect inflicted by a caregiver may develop an insecure or disorganised attachment style with effects on emotional development, development of self-concept, self-regulation and reflective functioning, and later their role as parents (Fonagy et al., 2000). These childhood experiences inflicted by their caregiver are thus hypothesised to mediate the association between BPD symptoms in parents and their offspring, that is, in the transgenerational transmission of BPD (Eyden et al., 2016; Steele et al., 2019).
Although high rates of BPD have been identified in women who score above the ‘cut-off’ on the EPDS when used in antenatal women (di Giacomo et al., 2020; Judd et al., 2019), only a few studies have examined the range of diagnoses other than depression and anxiety identified at routine antenatal screening (Harvey and Pun, 2007; Judd et al., 2019; Lydsdottir et al., 2014). The findings here indicate that BPP is not uncommon among women identified by antenatal screening and referred for mental health assessment during pregnancy. The prevalence of BPP in antenatal women identified at antenatal screening and the recognition that women with BPP are ‘high-risk’ caregivers argue for BPP to be recognised as a high priority for investment in service development. The 2017 Australian Clinical Practice Guidelines for Mental Health Care in the Perinatal Period (Austin et al., 2017) include information about BPD and emotional dysregulation but information about psychosocial assessment and screening remains focused on anxiety and depression. These guidelines need to be expanded and services for pregnant women with BPP need to be developed and funded.
Strengths and limitations
This study was conducted in a tertiary hospital which provided public antenatal care for all of Southern Tasmania. All women identified at routine antenatal screening were referred to the PCLP service for assessment and management. The major limitations of the study are that the study population was a convenience sample and that diagnoses were not made using operational definitions or a structured clinical interview for personality disorders, but by clinical interview. Interviewer bias cannot be excluded.
Footnotes
Acknowledgements
The authors thank Drs Anisha Grover, Daya Sadiq and Kishor Sivasankaran for assistance with psychiatric assessment of women in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Psychiatry trainee K.N. received financial support for data analyses initially undertaken for the RANZCP Scholarly Project through Specialist Training Program: Training More Specialist Doctors in Tasmania.