
Abstract
Available evidence suggests that persons with serious forms of mental illness are 4–10 times more likely to commit homicide as compared to non-affected members of the general population. The relationship between homicide and psychotic illness has now been subject to longitudinal investigation in six different populations across eight studies covering time periods over the last six decades. With the exception of one study, these investigations demonstrate that homicide associated with psychotic illness appears relatively stable through time and, in most populations, is not related to factors that contribute to the rise and fall of total population homicide (TPH) rates. This suggests that illness and treatment factors are of most importance if we are to reduce the prevalence of this tragic illness complication.
Keywords
Psychosis and violence
Available evidence suggests that persons with serious forms of mental illness (SMI; typically, psychotic and some major mood disorders) are 2–8 times more likely to commit violence as compared to non-affected members of the general population (Whiting et al., 2021), and that approximately 3–10% of violent crime is statistically attributable to SMI (Fazel et al., 2009). This risk is particularly elevated in the context of untreated symptoms and substance misuse (Fazel et al., 2009; Large and Nielssen, 2011; Nielssen and Large, 2010). Contrasting this are a number of studies of criminal justice involved persons with psychosis which find that factors that predict violence in the general population also are risk factors in persons with psychosis (Skeem et al., 2016), and that the contributory role of psychosis to violence is weak when compared to other criminogenic risk factors (e.g. criminal history, substance use, relationship and employment problems; Bonta et al., 2014).
Mental health services must be committed to excellence in clinical care and research to reduce the frequency of violence in the lives of people with SMI. Notably, persons with SMI are more likely to be victimized by violence than perpetrate violence, and the experience of victimization is shown to predict subsequent violent offending in those with schizophrenia (Latalova et al., 2014). Reasons to study homicide, rather than less serious violence, are threefold. First, homicide appears to be the violent offence that has the highest over-representation of people with SMI. Second, it is arguably the offence which carries the highest burden of suffering and impact, burdens which are often shared among victims and perpetrators, as well as society at large. Finally, there are few, if any, reporting issues with homicide. Unlike less serious violence, details surrounding homicide offences are typically of higher quality and comprehensiveness, they are not significantly under-reported, and in most developed countries clearance rates exceed 80%. For these reasons, homicide has been an important offence to study for what it may tell us about the nature of the risk conferred by psychosis (e.g. is it causal?). Furthermore, studying temporal trends in rates of homicide over time can elucidate how changing mental health sector policies and general societal trends may impact that risk.
Despite their infrequency, events of lethal violence committed by people with psychosis attract political and media attention, heightening public concern and stigma towards community-dwelling persons with psychotic illness. The message underlying these sensationalized portrayals is that the association between illness and violence is common, direct, and causal. The public struggles in an age of higher media scrutiny to know whether this problem is increasing (in the post-deinstitutionalization era) and this often drives fear and stigma against people with psychosis in the community.
Homicide in the context of psychotic illness: a distinct phenomenon?
Understanding the association between rates of homicide committed by people with and without psychotic illness can help clarify the extent to which these events share common aetiological underpinnings, how much additional risk psychosis confers and under what circumstances. This, in turn, has substantial implications for risk management and service delivery to people with psychosis. If homicide associated with psychosis varies with TPH, preventive strategies should be aimed at the same factors that are correlated with fatal violence in the general community (e.g. substance or alcohol use, and weapon availability). But if homicide associated with psychosis is independent of general population homicide, then illness-related factors including ensuring early and effective mental health service delivery may be of most importance.
Beginning with the overall magnitude of the relationship between psychosis and homicide, persons with psychosis are found to be 4–10 times more likely to perpetrate a homicide than persons who do not have such a diagnosis (Fazel and Grann, 2004; Large et al., 2009). Furthermore, the risk of homicide is approximately 15 times higher during the first episode of psychosis than later in the course of the illness, with approximately one-third (38.5%; 95% confidence interval [CI] = [31.1%, 46.5%]) of such homicides occurring prior to treatment onset (Nielssen and Large, 2010). As compared to homicides in the general population, victims of homicide by people with psychosis are most commonly people known to the person, especially family members and caregivers (Penney et al., 2018; Simpson et al., 2004; Taylor and Gunn, 1999).
Turning then to the question of whether rates of psychosis-related homicide (PRH) are correlated with or independent of TPH rates, this was first addressed in Coid’s (1983) seminal review of 15 longitudinal studies from several international jurisdictions. The main conclusion of this review was that the rate of homicide associated with serious mental illness (PRH) was more similar across countries than was the TPH rate. A major implication of this early work was to differentiate homicides associated with psychosis from those in the general population, noting that PRH may be caused by different factors than TPH. Such factors may account for the observed independence in PRH/TPH rates, differences in victim type (which much less commonly involves strangers in PRH) and when in the illness course that the homicide occurs (many pre-treatment). It also follows from this that more effective mental health services and earlier provision of care to people experiencing a first episode of psychosis may be the most effective way to reduce PRH.
In contrast to Coid’s (1983) findings, a more contemporary systematic review of cross-sectional studies by Large et al. (2009) found a strong association between TPH and homicide by people diagnosed with schizophrenia (r = .87, p < .001). Data were gathered across several developed nations and aggregated across time. This finding would suggest that PRH and TPH are in fact related, not distinct phenomena, and that preventive strategies might be better aimed at ones that lower TPH risk, such as addressing alcohol and substance use, weapons availability, as well as socioeconomic disadvantage and exposure to community violence. Rather than reflecting heightened risk that is inherently generated by psychotic illness, the results from Large et al. (2009) would suggest that the homicidal behaviour by persons with psychosis is better understood as a heightened vulnerability to those variables associated with an increased risk of all homicides.
In order to distinguish between these divergent observations, there are now eight well-designed longitudinal studies that can help to better understand these dynamics, notably Nielssen et al. (2021) in this journal and the recently published Golenkov et al. (2021). In contrast to cross-sectional studies, longitudinal investigations permit an analysis of homicide rates over time and thus can more sensitively examine the nature of the association between TPH and PRH. These studies are presented in Table 1. The populations from which these studies draw have at times been overlapping, with more than one publication on the same jurisdiction. The most recent or comprehensive analysis of each population has been included for the purposes of this synthesis.
Longitudinal studies of psychosis-associated homicide.
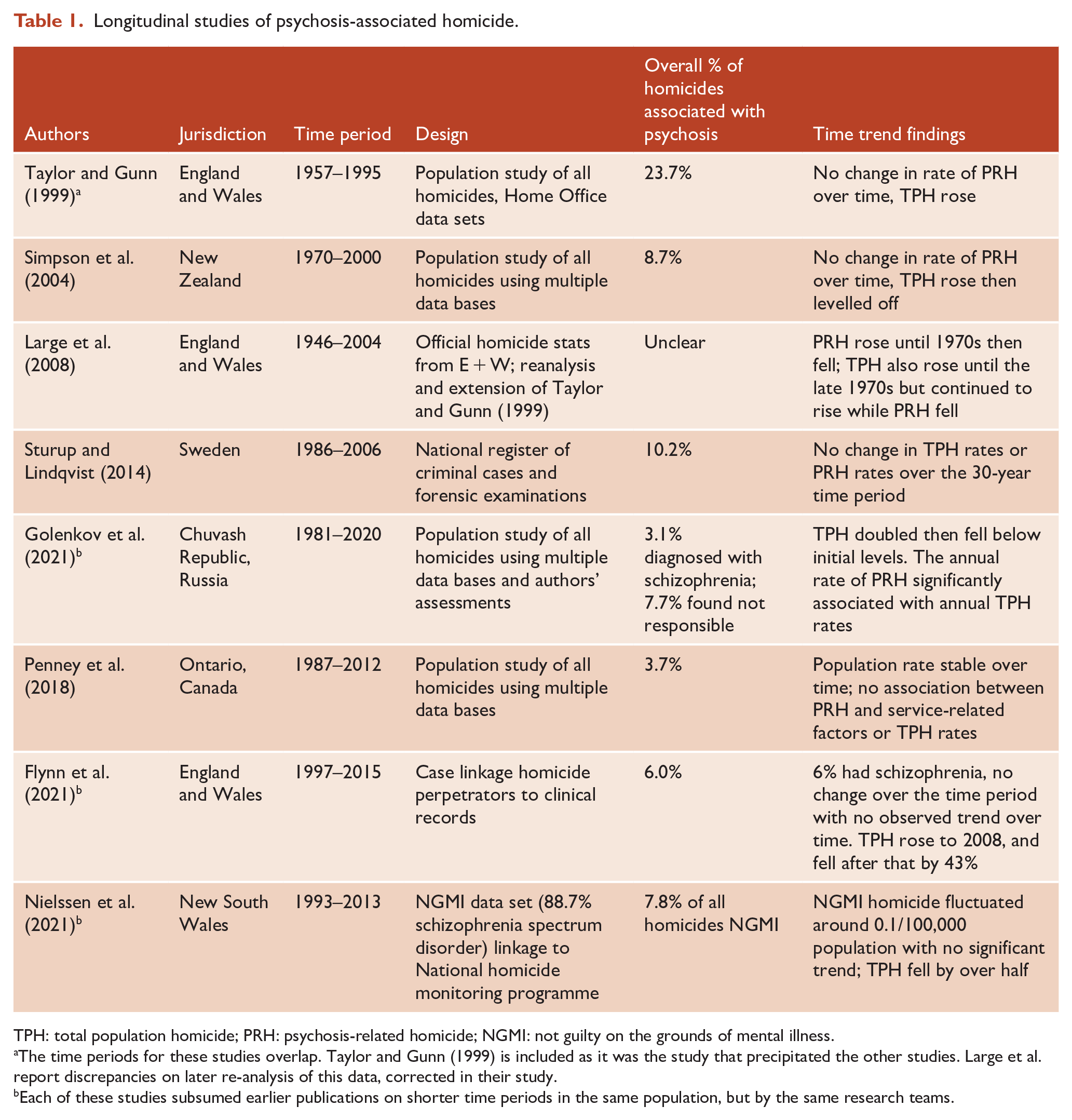
TPH: total population homicide; PRH: psychosis-related homicide; NGMI: not guilty on the grounds of mental illness.
The time periods for these studies overlap. Taylor and Gunn (1999) is included as it was the study that precipitated the other studies. Large et al. report discrepancies on later re-analysis of this data, corrected in their study.
Each of these studies subsumed earlier publications on shorter time periods in the same population, but by the same research teams.
What have we found?
The longitudinal studies permit a test of the relationship between TPH and PRH across time in the same setting, and most usefully by studying periods when TPH rises and falls. As noted, Coid (1983) proposed that PRH is relatively stable over time and not related to TPH. Flowing from this we would hypothesize that particular patterns in PRH would be observed should TPH be static, increasing or decreasing over the time period. Specifically, if TPH and PRH are unrelated, we would hypothesize that:
(a) If TPH rises, PRH will change little;
(b) If TPH falls, PRH will change little;
(c) If both TPH and PRH change little, they will appear, spuriously, to be associated;
(d) Alternatively, to support the conclusions drawn from Large et al. (2009), both TPH and PRH will co-vary.
What, then, do we find from the eight time trend studies shown in Table 1? Overall, rates of PRH have been relatively stable through time, with minor fluctuations as compared to the significant variability in TPH rates. Specifically:
(a) Sturup and Lindqvist (2014) and Flynn et al. (2021) are both studies where TPH was relatively stable and there was little change in PRH rates;
(b) Taylor and Gunn (1999), Simpson et al. (2004) and Large et al. (2008) each describe the trend where rates of TPH rose while PRH rates were static;
(c) Penney et al. (2018) and Nielssen et al. (2021) observed falling TPH rates during their time series but PRH rates did not change.
(d) Golenkov et al. (2021) found that the rate of PRH rose and fell along with the TPH rate, examined annually from 1981 to 2020 in the Chuvash Republic of Russia. Large et al. (2008) also found time periods in England and Wales where the two rates were correlated.
Thus, at least six of the eight studies appear consistent with Coid’s (1983) hypothesis that TPH and PRH are largely subject to different time-based effects. In the Golenkov et al., the study period encompassed a time when TPH rose significantly in this region (associated with major political change and a rapid rise in alcohol consumption) and then stabilized and declined to lower than initial rates by the most recent decade.
Taken together, much of this evidence converges to suggest that the rate of PRH is stable within different jurisdictions over time and may reflect a separate epidemiological domain to TPH. During the time periods of six of these studies, TPH varied markedly while PRH varied little. It also appears that while PRH and TPH generally follow different time trends, people with psychotic illness are not immune from some of the same causal factors and social pressures that drive homicide rates in the general population. The fallouts associated with major sociopolitical instability, for example, and which was seen in Golenkov et al. (2021), included rapid social upheaval and increases in alcohol consumption that appeared to heighten risk for people with a psychotic illness just as for other members of this society. Shaw et al. (2006) point out that simply because one has a lifetime diagnosis of a psychotic illness does not mean that there is an abnormal mental state at the time of the homicide. People who have a lifetime diagnosis of a psychotic illness may commit homicide for non-illness-related reasons.
If PRH is then a separate phenomenon to TPH, it should follow that changes in mental health service provision (particularly associated with de-institutionalization, and more recently, improved community services) might have impacted the rate of PRH. This has not been shown. Studies that have covered the period of de-institutionalization, where expected rises in PRH rates may be expected, have not found such effects (Large et al., 2008; Penney et al., 2018; Simpson et al., 2004; Taylor and Gunn, 1999). Similarly, expected declines in PRH rates resulting from better community care and first-episode services in the post de-institutionalization era have also not materialized (e.g. Flynn et al., 2021; Nielssen et al., 2021).
Why may these be separate phenomena?
It has long been posited that offenders with and without psychosis are impacted by similar criminogenic risk factors that increase the likelihood of crime and violence (Skeem et al., 2016) and that the excess violence observed in people with psychosis is the result of being disproportionately exposed, or vulnerable to, these risk factors (Bonta et al., 2014). This point is illustrated by the Golenkov et al. (2021) study and the Large et al. (2009) review of cross-sectional studies. In contrast, persons with psychosis who commit serious or lethal violence, and who are adjudged to have offended as a result of illness, appear to represent a distinct subgroup whose rates of violence may be unrelated to rates of crime in the general population. Five of the eight longitudinal studies citied here support this perspective. This scenario of there being ‘truth in both positions’ aligns with the framework described by Skeem et al. (2011), where the effect of mental illness on criminal behaviour reflects ‘moderated mediation’; that is, the link is direct and causal in one subgroup, but mediated by other factors in another subgroup.
It is notable that, in general, outcomes for people with psychotic illness have not improved significantly in the last 40 years. We might have hoped that increased community mental health services would have reduced the rate of PRH, but sadly that has yet to be demonstrated in any population. Similarly, the more widespread availability of first-episode services aimed at shortening the duration of untreated psychosis (DUP) would have been expected to reduce a substantial proportion of PRH related to first-episode events (e.g. one-third of all psychosis-associated homicides found in Nielssen and Large, 2010). At present, population-based data are required to link the effects of these early and more assertive community interventions to PRH rates.
One unique study that addresses these issues cross-sectionally is that of Segal (2012). Segal (2012) found that TPH rates were lower in US states when the quality and availability of mental health services was higher and mental health legislation was broader and less restrictive. There have been no recent long-term studies of homicide and mental illness in the United States, so this study introduces intriguing questions about the relationship of better mental health services with lowering rates of PRH. This work requires replication across other jurisdictions and in individual jurisdictions over time.
Conclusion and future research
Studies of homicide and psychotic illness demonstrate an increased risk of lethal violence by people with psychosis, but that the illness makes a modest contribution to total societal homicide, and is rare, overall, among all people with a psychotic illness. Active untreated symptoms appear to be the strongest risk factor, while conditions that exacerbate such symptoms (e.g. substance misuse, inadequate or delayed care) will heighten this risk. Effective responses to manage the risk of serious violence conferred by psychosis will need to encompass a constellation of services that span illness-related (e.g. improved access to services, lessened DUP, better maintenance in care) and criminogenic (e.g. sufficiently assertive substance use treatment, employment and vocation services, psychosocial supports) domains. Although the preponderance of evidence reviewed here appears to support an illness-specific component to the risk of homicide, it is also clear that the factors giving rise to these tragic events are multi-faceted and interact with each other in complex ways.
Acknowledging the complex and layered nature of this risk also encourages us to think more holistically about improving the prognosis for all people with psychotic illness in a manner that both reduces the risk of adversity and promotes recovery, resilience and well-being. It would be expected that tailored, balanced and multi-modal interventions will be associated with decreased rates of homicide over the long term, but this remains to be shown. Future research which elucidates the patterns and pathways to violence in people with psychosis, to better understand its precipitants and motivations, will offer valuable guidance to more finely tune and evaluate effective service responses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.