
Abstract
Objective:
To describe the characteristics of offenders found not guilty on the grounds of mental illness (NGMI) in New South Wales and rates of NGMI and other homicide verdicts.
Method:
Demographic, legal and clinical data after referral to the NSW Mental Health Review Tribunal following an NGMI verdict for homicide matched with results from the National Homicide Monitoring Program.
Results:
Between 1993 and 2016, a total of 2159 homicide offenders were dealt with by the NSW courts, including 169 (7.8%) who were found NGMI. Over this period, the rate of non-NGMI homicide convictions fell from 1.83 per 100,000 per annum to 0.65 per 100,000 per annum (Kendall’s tau = −0.79, p ⩽ 0.001) while the rate of NGMI homicide fluctuated, with an average annual rate of about 0.1 per 100,000 per annum (Kendall’s tau = 0.17, p = 0.23). There was no association between the annual rates of NGMI and non-NGMI homicides (Pearson r = −0.3, p = 0.16) but falling rate of non-NGMI homicide meant that the proportion of NGMI offences doubled from 5.5% in the first 12 years to 11% in the second 12 years. Nearly all (88.7%) of those found NGMI had a schizophrenia-related psychosis. However, there were high rates of psychiatric comorbidity including substance use disorder (60.7%) and a history of a prior head injury (41.1%). Most (83.4%) of the NGMI offenders had previous contact with mental health services, but only half of these had received treatment with antipsychotic medication.
Conclusion:
The fall in conviction for homicide offences in the last 24 years has not been matched by a reduction in NGMI homicide verdicts. More assertive treatment of emerging psychosis and comorbid substance use disorders, and improved continuity of care of chronic psychosis might prevent some homicides.
Introduction
Most people with a psychotic illness will never be violent and homicides by people with an established diagnosis of schizophrenia are rare events (Nielssen and Large, 2010). However, the odds of homicide by people with schizophrenia is higher than that of the general community (Fazel et al., 2009), and it has been estimated that about 6.5% (95% confidence interval [CI] = [5.6%, 7.5%]) of all homicides are by people diagnosed with schizophrenia (Large et al., 2009).
The most widely accepted explanation for the increased incidence of serious violence associated with schizophrenia is that the violence is motivated by thought processes that are intrinsic to psychosis such as delusional beliefs, often arising from auditory hallucinations (Coid et al., 2013; Tanay, 1987). In extreme cases, psychotic symptoms can deprive offenders of the knowledge that killing another person is wrong and opens the possibility of a verdict of not guilty on the grounds of mental illness (NGMI) (McNaughten, 1843). The belief that homicide is a rare but intrinsic complication of psychotic illnesses was supported by an influential paper asserting that rates of mentally ill homicides in England remained stable while non-mentally ill homicide increased in the second half of the 20th century (Taylor and Gunn, 1999) and a widely cited review suggesting that rates of homicide by the mentally ill were similar between nations (Coid, 1983). However, not all studies have found that rates of homicide by the mentally ill are stable and unrelated to other homicide rates, with some studies reporting a rise in homicides by the mentally ill along with the rates of other homicides (Gottlieb et al., 1987; Gudjonsson and Petursson, 1986), some reporting the rate mentally ill homicide to be stable when other homicides declined (Flynn et al., 2020; Penney et al., 2018), and others reporting changing relationships between mentally ill and non-mentally ill homicide rates in different periods (Large et al., 2008; Simpson et al., 2004). Furthermore, a meta-analysis of 18 population-based studies showed large differences in rates of homicide by people diagnosed with schizophrenia between geographic regions and that these rates were strongly correlated with rates of homicide by people without schizophrenia (Large et al., 2009).
Understanding the relationship between rates of homicide by the mentally ill and non-mentally ill homicide has implications for how some homicides are understood and potentially prevented. If mentally ill homicides rates are closely related to rates of other homicides, they are likely to share common etiological factors, such as patterns of substance use, weapon availability and the level of violence in the community. Hence, general measures to reduce violence would also be expected to reduce the number of homicides committed by people with mental illness. On the contrary, if the rate of homicide by the mentally ill is not linked to rates of other homicides, then reducing mentally ill homicide may depend more on changes in the way mental health services are delivered.
To date, there has been no Australian study reporting changes in rates of homicide by people with mental illness in over time. Previous Australian studies of homicide associated with psychosis in New South Wales between 1993 and 2002 (Nielssen et al., 2007) and schizophrenia in Victoria 1997 and 2005 (Bennett et al., 2011) were not conducted over long enough periods to meaningfully consider temporal trends.
We hypothesised that there had been a decline in the rate of homicide by people with mental illness in NSW in the last two decades because of the well-publicised decline in the rate of homicide in Australia (Bricknell, 2020) and because of the increased availability of early intervention and other community mental health services for people with psychosis (Galletly et al., 2016). In order to test this hypothesis, we examined the rates of homicide by people who were either convicted or found to be NGMI of a homicide offence in NSW between 1993 and 2016. We also examined the clinical characteristics of the NGMI offenders, with particular attention to the presence of known risk factors for violence, including substance use and prior criminal history, and potentially protective factors including contact with health services.
Method
The NSW Mental Health Review Tribunal (MHRT) supervises the care of all people found NGMI by the higher courts in NSW, and holds a range of demographic, legal and clinical information about each case. The defence of NGMI in NSW can be raised if the common law tests set out in R v McNaughten (McNaughten, 1843) and R v Porter (Porter, 1933) can be established. These tests require the defence to show the presence of both a mental disorder and that the defendant was unable to reason about whether the act was wrong. Not everyone with a mental illness charged with a homicide offence relies on the defence of mental illness. However, the test did not change during the 24 years of the study and the number of NGMI verdicts is a fair indicator of the number of homicides committed due to the effect of mental illness.
The annual number of non-mentally ill offenders was calculated by subtracting the number of NGMI offenders from the total number offenders dealt with by the courts each year reported by the National Homicide Monitoring Program published by the Australian Institute of Criminology (AIC) (Bricknell, 2020). Australian Bureau of Statistics (ABS, 2020) figures were used for the annual populations of NSW. Un-standardised homicide rates were calculated using the number of homicide NGMI and non-NGMI offenders and the total NSW population. Changes in NGMI and non-NGMI homicide rates were examined using Kendall’s tau and the correlation between rates of NGMI and non-NGMI homicide convictions were examined using a Pearson correlation coefficient.
Details of the offenders found NGMI were extracted from the NSW MHRT electronic records and paper case files, and included age, sex, indigenous status, place of birth, the relationship to the victim, age at diagnosis, recent substance use, whether substance affected at the time of the offence, psychiatric diagnosis, past treatment with antipsychotic medication, history of acquired brain injury, intellectual disability, forensic history and whether found unfit for trial prior to the NGMI verdict.
Using a record-linkage process, the NGMI offender sample was matched to the Bureau of Crime Statistics and Research (BoCSaR) Reoffending Database (ROD) to obtain de-identified criminal history from 1994 onwards, in order to examine criminal charges and imprisonment prior to the index offence. The sample was also linked to administrative health datasets held by the Centre for Health Record Linkage to examine hospital admissions and contact with outpatient mental health services from 2001 onwards. This included the Admitted Patient Data Collection, which contains records from all NSW public, private, psychiatric and repatriation hospitals in NSW, and the Ambulatory Mental Health Data Collection, which contains information on the assessment, treatment, rehabilitation or care of non-admitted mental health patients.
Approval to conduct the study was obtained from the University of New South Wales Human Research Ethics Committee (reference no. HC12505) and the NSW Population and Health Services Research Ethics Committee (AU RED Reference: HREC/18/CIPHS/48; Cancer Institute NSW Reference: 2018HRE1003).
Results
Rates of all homicide offenders and NGMI offenders over time
A total of 2159 people were found to have committed a homicide offence in NSW between 1993 and 2016, including 169 (7.8%) who were found to be NGMI. During this period, the total rate of homicide offending fell from 1.8 per 100,000 per annum in 1993 to 0.65 per 100,000 per annum in 2016 (Kendall’s tau = −0.79, p ⩽ 0.001) while the rate of NGMI homicide fluctuated without an overall trend upwards or downwards, and with an average annual rate of about 0.1 per 100,000 per annum (standard deviation 0.05 per 100,000 per annum, Kendall’s tau = 0.17, p = 0.23). There was a non-significant association between the rates of NGMI and non-NGMI homicides (Pearson r = −0.3, p = 0.16). As a result of declining rate of non-NGMI homicide, those found NGMI comprised an increasing proportion of all homicide offenders (Table 1, Figure 1). In the first 12 years of the study between 1993 and 2004, there were 70 (5.5%) NGMI offenders among a total of 1248 homicide offenders, while in the second 12 years between 2005 and 2016 there were 99 (11%) NGMI offenders among a total of 911 homicide offenders (χ2 = 20.2, df = 1, p < 0.001).
Number of NGMI and non-NGMI verdicts for homicide offences in NSW 1993–2016.
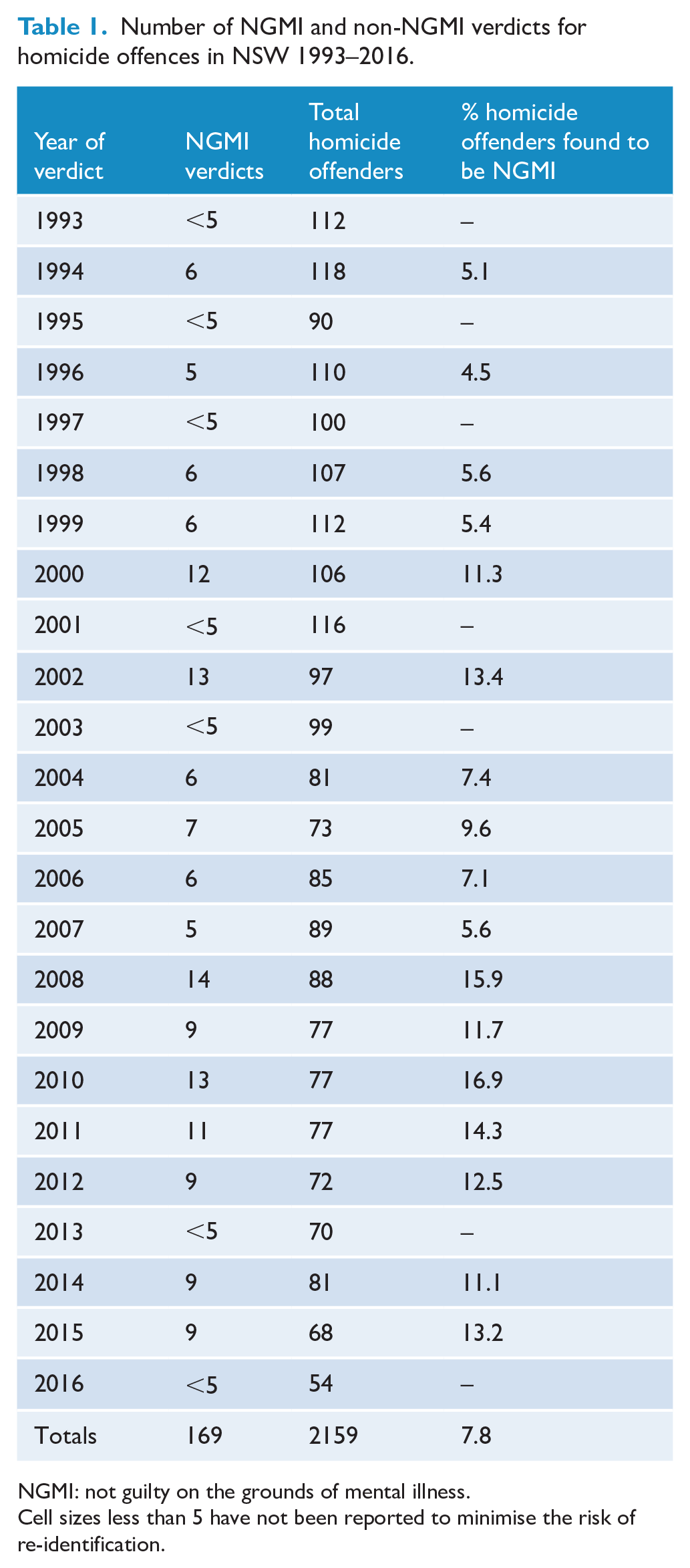
NGMI: not guilty on the grounds of mental illness.
Cell sizes less than 5 have not been reported to minimise the risk of re-identification.
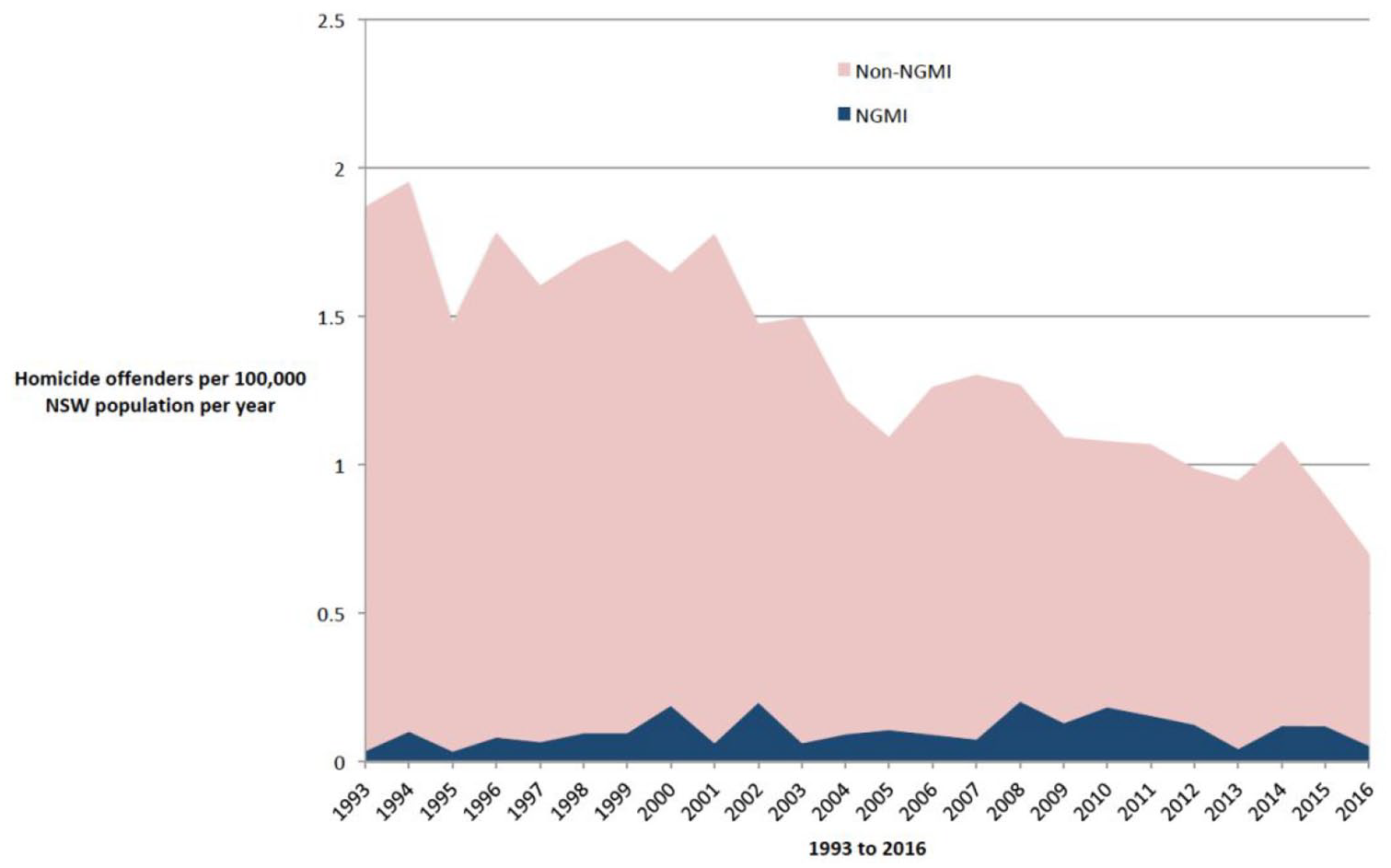
Homicide offenders in NSW 1993 to 2016.
Characteristics of NGMI offenders
The demographic features of the sample are described in Table 1. Almost 9 in 10 offenders were male, just under a third were born overseas, and the mean age at the time of the verdict was in the mid-thirties. Most of the victims were relatives of the offender and fewer than 1 in 10 victims were unknown to the offender until immediately prior to the homicide. To the authors’ knowledge, there were no recidivist homicides in the NGMI group.
Almost 9 in 10 of the NGMI offenders were thought to have a schizophrenia spectrum disorder. Other conditions included dementia and organic mental disorders, including epilepsy. More than half of the offenders had a comorbid substance use disorder, around half had taken a psychoactive substance prior to the offence and almost a third were reported to be affected by a substance at the time of the offence. Other comorbidities included a history of acquired brain injury and intellectual disability. Nearly 1 in 5 were found unfit to be tried at some stage in the proceedings, although data were not available as to how many of those recovered sufficiently to be able to enter a plea at trial.
Linked health data revealed that over 8 in 10 had prior contact with the public mental health system, and almost three quarters had an earlier admission to a psychiatric hospital for any reason. According to the MHRT records, about a quarter of the offenders were judged to be in the first episode of psychosis, although about 4 in 10 NGMI offenders had no record of having been treated with antipsychotic medication prior to the offence. Two thirds of NGMI offenders had some history of deliberate self-harm.
Records held by the MHRT showed that over half of the NGMI offenders had a previous criminal charge, often for a violent offence, and around a fifth had previously been in prison (Table 2).
Characteristics of NGMI homicide offenders 1993–2016.
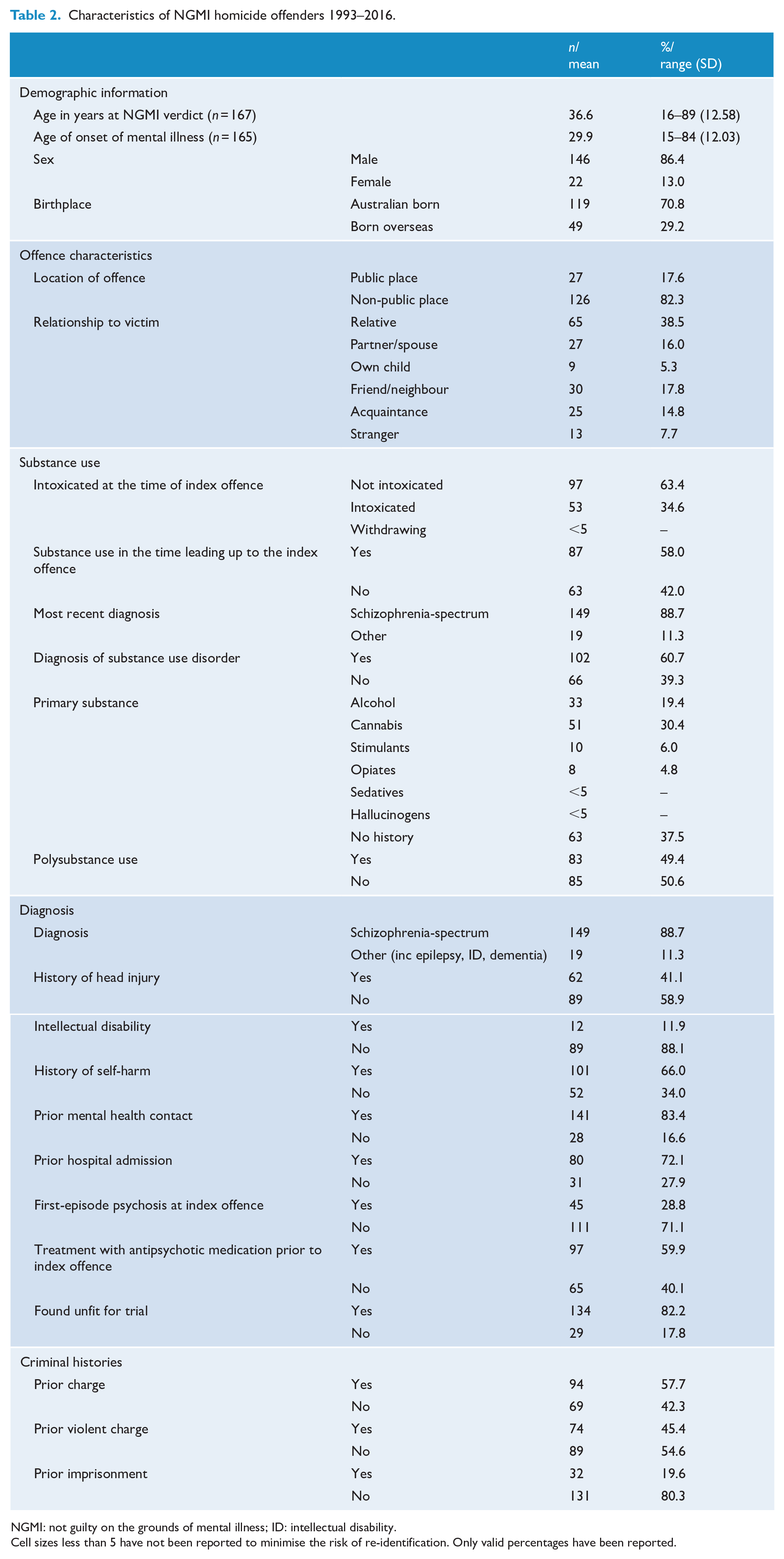
NGMI: not guilty on the grounds of mental illness; ID: intellectual disability.
Cell sizes less than 5 have not been reported to minimise the risk of re-identification. Only valid percentages have been reported.
Discussion
There has been a steady decline in the rate of homicide in NSW over the last quarter of a century to the extent that the rate of homicide in Australia is at an historic low (AIC, 2020), far below the current global homicide rate of about 6 per 100,000 per annum (Global Study of Homicide Report, 2020). The proportion of known homicide offences resulting in a conviction has also increased in the last 25 years (BoCSaR, 2017) meaning that there has been a real and important decline in homicide in NSW. By contrast, there has been no decline in the rate of homicides by the mentally ill, as measured by the number of homicide offenders found NGMI, causing the proportion of all homicide offenders found to be NGMI to double between the first and second halves of the study period.
The finding that NGMI homicides have not fallen with the decline in the overall rate of homicide is disappointing and was contrary to our expectations. We had expected that the factors associated with the decline in non-mentally ill homicide, such as a decline in the availability of firearms (Chapman et al., 2006) and reduced alcohol consumption (Livingston et al., 2018), would have also contributed to a reduction in the rate of homicide by the mentally ill. Furthermore, we had hoped that improvements to the systems of care for patients with emerging psychosis and better continuity of care for known patients would have resulted in a decline in the number of homicides by people with mental illness.
Most of the NGMI offenders supervised by the MHRT were diagnosed with schizophrenia, consistent with earlier studies (Bennett et al., 2011; Nielssen et al., 2007) and research finding an association between schizophrenia and homicide offending (Fazel et al., 2009). However, many NSW NGMI homicide offenders had other criminological risk factors, including comorbid substance use and involvement in criminal activity, as reflected in the number who had prior criminal convictions and imprisonment. Almost all of the NGMI offenders had some previous contact with mental health services and nearly half had been admitted to a psychiatric hospital. A surprisingly high proportion had at least one episode of deliberate self-harm. However, despite almost all of the NGMI offenders having schizophrenia, a significant proportion were recorded as never having been treated with antipsychotic medication, either because the emergence of schizophrenia had not been identified during earlier contact or because the intervention had not been assertive enough to ensure effective treatment (Nielssen et al., 2007, 2011). Barriers to treatment of emerging psychosis was a factor in some cases, and studies have shown that families make between three or four attempts to obtain treatment before they actually receive care (Lieberman and Fenton, 2000). Most of the offenders with established psychosis were not adherent to medication at the time of their offences, as is the case in episodes of serious non-lethal violence in psychosis (Yee et al., 2011) and non-adherence to treatment is a major reason for both hospital re-admission and serious violence by known patients.
If the current trend in NGMI and non-NGMI homicide rates continues in the next decades, a growing proportion of homicide offenders will be regarded as mentally ill, a trend that has also been observed in England and Wales (Flynn et al., 2020) and in Ontario (Penney et al., 2018). A rising proportion of homicides committed by the mentally ill is likely to increase the stigma associated with serious mental illness, even if the number of homicides do not increase in absolute terms. The stigma associated with schizophrenia is arguably a greater problem than the actual acts of violence by people with mental illness (Pescosolido et al., 2019). However, a reduction in the number of highly publicised homicides by people with schizophrenia might help reduce the stigma associated with the illness (Torrey, 2011). Although intensive early intervention for psychosis has not been shown to reduce offending in other jurisdictions (e.g. Stevens et al., 2013), our finding that most of the NGMI offenders had had some contact with mental health services suggests that there might be opportunities to prevent some homicides through earlier and more continuous treatment of psychosis and greater attention to comorbid substance use. Given the very low base rate of these tragic events, attempts to identify and intervene to treat known patients at greater risk of serious violence are unlikely to prevent individual cases. The alternative is to establish a universal standard of care with lower barriers to care, adequate treatment of episodes of illness, provisions for continuity of care, persistent attention to comorbid conditions and the mobilisation of services to improve the social circumstances of patients (Nielssen et al., 2017).
This study has a number of significant limitations. The first is our reliance on legal verdicts rather than diagnoses made by a systematic evaluation of every homicide offender, which has formed the basis of studies conducted elsewhere (e.g. Golenkov et al., 2011). Furthermore, although the legal threshold for NGMI verdicts has not changed in NSW, it is possible that there have been differences in the way the law has been applied over the years. For example, in 1997, a change to the Crimes Act from ‘diminished responsibility’ to ‘substantial impairment by abnormality of mind’ effectively raised the threshold for a manslaughter verdict because of an abnormal state of mind. In 2009, there were significant changes to the Mental Health (Forensic Provisions) Act 1990 to give the MHRT the sole power to make decisions in relation to Forensic Patients, whereas those decisions had previously involved a discretionary decision by the Executive branch of government. This may have made a plea of NGMI more attractive. A second limitation is a lack of detailed or systematically collected information on the mental conditions of the offenders who were found guilty of a homicide offence. The authors are aware of a small number of offenders with psychotic illness, including established schizophrenia, who were convicted of homicide offences, or who appear to have chosen not to raise the mental illness defence. A further study is planned to examine the published court judgements for evidence of psychiatric disorder that might have been present, in order to establish a more accurate rate of homicide by people with schizophrenia. The lack of detailed information about those convicted of homicide offences also meant we were unable to compare the criminological features of convicted offenders to those found NGMI. A third limitation is that neither data set includes information about homicide followed by suicide, potentially excluding a further group of offenders with severe mental illness who might otherwise have been eligible for an NGMI verdict. Another consideration is the effect of comorbid substance use on criminal responsibility. In other parts of Australia and elsewhere a mental illness verdict is not available to homicide offenders who are affected by substances at the time of the offence, recently added to the common law in NSW (R v Fang, 2017), which would have the effect of reducing the proportion of offenders found NGMI, even if the number with severe mental illness was similar.
Conclusion
A growing proportion of homicides in NSW are by people who are subsequently found NGMI, not because the rate has increased, but because of the historic fall in homicides generally. Interventions designed to reduce the incidence of serious violence, including homicide, seem to have contributed to a decline in the overall rate of homicide, but do not appear to have affected the rate of homicide by people with serious mental illness in NSW. The finding that many of the NGMI offenders had prior contact with services suggests there are opportunities for mental health services to intervene to prevent these rare but catastrophic events by reducing barriers to care and greater efforts to ensure continuity of care and treatment of comorbid substance use.
Footnotes
Acknowledgements
The authors thank the staff of MHRT who assisted in compiling the database.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Approval for this study was obtained from the University of New South Wales Human Research Ethics Committee (reference no. HC12505) and the NSW Population and Health Services Research Ethics Committee (AU RED Reference: HREC/18/CIPHS/48; Cancer Institute NSW Reference: 2018HRE1003).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
O.N. has prepared reports for court in many of the matters in this study and holds shares in Intra-Cellular Therapies, Inc. M.L. has prepared opinions for Coroner’s inquests and in professional standards matters.