
Abstract
Objectives:
Whether a country’s level of development is associated with an increased or decreased burden of mental and behavioural problems is an important yet unresolved question. Here, we examined the association between the burden of mental and substance use disorders and self-harm with socio-demographic development along temporal and geographical dimensions.
Methods:
We collected data from the Global Burden of Disease study 2019, which uses robust statistical modelling techniques to calculate disease burden estimates where data are sparse or unavailable. We extracted age-standardized Disability Adjusted Life Year rates as a measure of disease burden for 204 countries and territories, as well as the Socio-Demographic Index, a measure of development reflecting income per capita, fertility rate and level of education. We tested the association between Socio-Demographic Index and Disability Adjusted Life Years for mental and substance use disorders and self-harm, between 1990 and 2019, and across six geographical regions as defined by the World Health Organization.
Results:
The association between Socio-Demographic Index and Disability Adjusted Life Years was heterogeneous across world regions for all mental and behavioural conditions. For substance use disorders and self-harm, these regional variations were further moderated by time period. Our findings were robust to down-weighing outlier observations, as well as controlling for other socio-demographic variables, and the number of data sources available in each country.
Conclusion:
Based on data from the Global Burden of Disease study 2019, we demonstrated that the association between mental and substance use disorders and self-harm with socio-demographic development is dependent on geographical regions and temporal periods. This heterogeneity is likely related to geographical and temporal variations in socio-cultural norms, attitudes towards mental problems, as well as health care and social policies. Better knowledge of this spatial and temporal heterogeneity is crucial to ensure that countries do not develop at the expense of a higher burden of mental and behavioural conditions.
Keywords
Background
Mental and behavioural conditions, which regroup mental disorders, substance use disorders and self-harm, represent one of the leading causes of Years Lived with Disability (YLD) worldwide (Vos et al., 2020). A great challenge to both developed and developing countries is to better understand risk and protective factors driving the burden of these disabilities, and in turn, develop effective health policies.
Taken broadly, the concept of development usually refers to material security and freedom of choice (UNDP, 2010), and as such would be strongly linked to the concept of vulnerability (being unable to cope with harmful or stressful conditions) and that of mental health. Potential mediators of these relationships would encompass a number of social determinants of health, such as security of food and shelter, employment, education, participation in the community, health literacy, health expenditure and so on. A vast amount of studies investigating the social determinants of health have shown that a low level of development is in general related to an increased burden of these conditions (Patel et al., 2018). However, recent observations from the field of psychiatric epidemiology have seemed to uncover an opposite finding: for various mental, but also substance use disorders and self-harm, the burden of disease seems to be paradoxically greater in less vulnerable, more developed nations – which some have referred to as a ‘vulnerability paradox’ (Bromet et al., 2011; Degenhardt et al., 2018; Dückers and Brewin, 2016; Dückers et al., 2016, 2019; Dückers and Olff, 2017; Ruscio et al., 2017). If confirmed, this finding could mark an important milestone, where research could take an interesting turn: investigating the negative effect of development on mental and behavioural disabilities.
Yet, at this point, the discrepancy between this so-called ‘vulnerability paradox’ versus more classical theories relating wealth to the burden of mental and behavioural conditions is far from being resolved and has become a debated topic (Jorm and Mulder, 2021; Mulder et al., 2020). Two important issues limit the validity and generalizability of previous findings testing the association between a country’s level of development and the burden of mental problems. First, associations have been tested using a limited number of high-quality observations, especially with respect to low-income countries. In this context, findings are either prone to data inaccuracy and inconsistency, or are restricted to countries that have trustful datasets – most often developed, Western countries (Adebisi, 2020; Jorm, 2006; Vermetten et al., 2016). Second, there are theoretical grounds to postulate that the relationship between development and mental and behavioural disabilities might vary along geographical and temporal dimensions. Geographical regions regroup individuals with similar genetic and cultural backgrounds, probably based on historical (e.g. colonial history) and geological (e.g. climatic conditions) contexts (Beugelsdijk and Welzel, 2018; Elhaik et al., 2014). These have been shown to influence both a country’s level of socioeconomic development and its relationship to an individual’s emotions, cognitions and behaviours (Enke, 2019; Granato et al., 1996; Jorm and Ryan, 2014). Hence, plausibly, the association of mental and behavioural issues with development could depend on these geographical clusters. Likewise, the burden of mental and behavioural disabilities and its relationship with development could be mitigated by temporal factors, such as the emergence of novel health policies, treatment programmes or socioeconomic conditions.
This study attempts to overcome these issues by using data from the Global Burden of Disease (GBD) study 2019, which provides estimates of morbi-mortality for 204 countries and territories from 1990 to 2019 (Vos et al., 2020). This data source has been described as the most comprehensive health database worldwide, and uses robust statistical modelling techniques to predict disease burden estimates for countries where data are sparse or unavailable. More specifically, our aim was to use the GBD database and expand on previous research (e.g. Degenhardt et al., 2018) to explore the association between the burden of mental and substance use disorders and self-harm with socio-demographic development along regional and temporal dimensions. Regional variation was examined by grouping countries into the six geographical regions as determined by the World Health Organization (WHO). Temporal aspects were investigated by testing whether estimates in 2019 differed from those in 1990.
Methods
Data
Presentation of the GBD study 2019
The GBD study 2019 incorporates 86,249 input sources to estimate the burden of 369 diseases and injuries for 204 countries and territories (often referred to as locations in the GBD terminology) from 1990 to 2019 (Vos et al., 2020). As such, it represents an important tool to inform clinicians, researchers and policy makers to better understand health trends and further achieve quantifiable progress in global health. These input sources include a comprehensive catalogue of health-related data such as surveys, the scientific literature, censuses, registries and other administrative data. To be included in the GBD study, input sources have to comply with guidelines provided by GATHER which are the gold standard for observational studies (Stevens et al., 2016). Following GATHER ensures that adequate information is available to assess the quality of the source data, in particular, that study samples are representative of the general population and have clinical thresholds established by international classifications.
The GBD study includes all member states of the WHO (Vos et al., 2020). In the current study, we further grouped locations within world regions using the WHO regional classification system (WHO, 2021). Briefly, the WHO divides the world into six regions, defined for reporting, analysis and administration purposes: Africa (AFR, n = 47 locations), the Americas (AMR, n = 38), the Eastern Mediterranean region (EMR, n = 22), Europe (EUR, n = 54), South-East Asia (SEAR, n = 11) and the Western Pacific region (WPR, n = 32). The composition of each WHO region is provided in the Supplementary Material (p. 1).
Previous works have reported GBD estimates of the burden of mental and substance use disorders and self-harm (e.g. Charara et al., 2017; Charlson et al., 2015; Dandona et al., 2018; Degenhardt and Hall, 2012; Degenhardt et al., 2018; GBD 2019 Mental Disorders Collaborators, 2021; Griswold et al., 2018; Whiteford et al., 2013). Typically, these studies use a number of primary data sources to inform GBD modelling (e.g. Degenhardt et al., 2011; Rehm et al., 2010, 2013; Vigo et al., 2016; Whiteford et al., 2016). The number of sources available in the GBD database to provide estimates for each condition was as follows: 3235 for mental disorders, 5280 for substance use disorders and 4193 for self-harm (Global Health Data Exchange, 2020). However, these relatively large numbers are mitigated by two caveats. First, the availability of the data sources is unequally distributed across locations and geographical regions, with Europe and the Americas having the greatest number of available sources. Second, available data may be of poor quality, for instance, if it does not use the preferred case definition or an appropriate measurement method. Using a 5 stars classification system, the GBD provides a grading of data quality for each location. In the Supplementary Material, we provide a definition of the higher-level causes, as well as a breakdown of available sources and data quality per WHO regions (pp. 2–3).
To make sense of this large number and a wide variety of input sources, and to adjust disease burden estimates where data sources come from locations with a low-quality grading, the GBD uses a multi-step procedure. First, all available data are standardized, mapped to the GBD cause list, stratified by age and sex, corrected for miscoded causes and redistributed to appropriate causes, aggregated over various sources, and finally pooled into a single database (Vos et al., 2020). Second, to generate cause-specific estimates by age, sex, year and location, data are modelled using standardized tools. A detailed description of the methods used to calculate disease burden estimates for mental and substance use disorders and self-harm and especially those that have changed between the GBD study 2019 and the previous round (GBD study 2017) are provided elsewhere (Afshin et al., 2019; James et al., 2018; Roth et al., 2018; Vos et al., 2020). Of particular importance is the out-of-sample predictive validity of the modelling techniques to calculate estimates for locations where data are unavailable or sparse. Such an out-of-sample predictive validity largely depends on the quality of the modelling techniques and in particular on the use of specific covariates that ‘borrow strength’ across time and geography. Overall, the GBD study made use of more than 700 covariates, which include socioeconomic and demographic data, as well as indicators on health system access, climate and food consumption. Note that the out-of-sample predictive validity of the modelling techniques for mental and substance use disorders and self-harm was overall excellent (Vos et al., 2020).
Outcome measure
Disability Adjusted Life Years (DALYs) was our outcome of interest. Briefly, for a specific year, country and disability, DALYs are a measure of overall disease burden, expressed as the sum of the number of estimated YLD and early death (Years of Life Lost, YLL). YLD is measured according to the formula YLD = Prevalence × Disability Weights. Disability weights are based on population surveys to lay descriptions of sequelae highlighting major functional consequences and symptoms (Vos et al., 2020). Disability weights are held invariant between age and sex groups, as well as locations and over time. Disability Weights are measured on a scale from 0 (full health) to 1 (death). Importantly, in the GBD study, each disability is collectively exhaustive and exclusive of any comorbidity. We specifically extracted age-standardized DALY rates (per 100,000) of the 204 locations included in the GBD study 2019 for mental and substance use disorders and self-harm in 1990 (the earliest time point) and 2019 (the latest) (Global Health Data Exchange, 2020).
Measures of data quality and uncertainty
We extracted two additional measures representative of data quality and uncertainty. First, we collected the number of sources available for each location and each condition from the GBD database (Global Health Data Exchange, 2020). Second, for each location and each condition, we calculated a measure of data uncertainty around standardized DALY rates using their 95% uncertainty intervals (UIs) which are also provided in the GBD study (Global Health Data Exchange, 2020). The 95% UIs are defined by the 25th and 975th value of the ordered 1000 estimate values of the DALYs uncertainty distribution. UIs reflect various sources of uncertainty, such as measurement error due to sampling distributions, sample sizes of data sources, adjustments and corrections of measurement errors applied to data parameter, as well as uncertainty in model estimation, within all-cause and cause-specific mortality models, and uncertainty associated with establishment of disability weights. We computed the coefficient of variation of each standardized DALYs rate based on their 95% UIs and included them as a measure of data uncertainty in our statistical analysis.
The Socio-Demographic Index
The Socio-Demographic Index (SDI) was developed by GBD researchers as a summary measure to quantify the development of locations included in the GBD study (Global Health Data Exchange, 2020). Briefly, the SDI is the geometric mean of indices of total fertility rate under the age of 25, mean education for those aged 15 and older, and lag distributed income per capita. Each component is scaled relative to maximum effect on health outcomes. The SDI range is 0 to 1. A value of zero represents the lowest income per capita, lowest educational attainment and highest total fertility rate observed across all locations from 1980 to 2019. A value of one represents the highest income per capita, highest educational attainment and lowest total fertility rate.
Other socio-demographic measures
We compiled other time-varying location-level variables that might influence the relationship between DALYs and SDI (Barbalat and Franck, 2020; Ribeiro et al., 2017; Wilkinson and Pickett, 2009): income inequalities (defined as the 90/10 ratio: the ratio of the top 10% of incomes to the lowest 10% of incomes and extracted from the World in Data database; n = 173 locations); unemployment rate (extracted from the World Bank database; n = 181 locations); population size (retrieved from the Global Health Data Exchange database; n = 204 locations); and total health expenditure as a percentage of the gross domestic product (GDP) (also retrieved from the Global Health Data Exchange database – note that the earlier and later years where data were available for this measure were years 1995 and 2017; n = 195 locations). URL for these data sources are provided in the Supplementary Material (p. 5).
Analysis
We conducted a series of statistical models corresponding to our study objectives and described below.
Baseline statistical model for each condition (Model 1)
We first tested the effect of development, time and region on standardized DALY rates separately for mental and substance use disorders and self-harm. For each condition, we ran a linear mixed-effects regression model of standardized DALY rates by the SDI, Time (2019 vs 1990) and Region (AFR vs AMR vs EMR vs EUR vs SEAR vs WPR). Countries were entered as a random factor (defining a random intercept model). We also added the coefficients of variation of DALYs as a covariate to take into account data uncertainty. For each model, we removed extreme DALY values from our dataset, which were identified using the 1.5 × IQR rule (Supplementary Material, p. 3).
All main effects and interactions among fixed effects were tested. Note that we used ‘contrast coding’ to examine whether the effects related to each geographical region significantly differed from that of the grand mean of all observations (rather than the mean of a reference region as with ‘dummy coding’). However, as we were primarily interested in the overall Region effect (i.e. in the joint significance of all regional effects), rather than the specific effect of each geographical region, we chose to report results related to regional variability (main effects or interactions) using overall F statistics, which, if significant, were further decomposed using t statistics retrieved from the full models. A detailed report of our full models is provided in the Supplementary Material (pp. 5–8).
Sensitivity analysis (Models 2–5) and assumptions of linear regression
For each mental and behavioural condition, we tested a set of additional statistical models to check that estimates were robust to the following variations from our baseline analysis:
down-weighing outlier observations using robust linear mixed-effects regression: Model 2;
including time-varying within-level socioeconomic covariates (unemployment rate, income inequality, health expenditure and population size): Models 3;
including the number of available sources for each location and each condition as a between-level covariate: Models 4;
analysis of locations with a higher data quality grading: Models 5.
Finally, note that we applied two transformations to the data to ensure that our models complied with the assumptions of linear regression. First, we log-transformed the dependent variable (standardized DALY rates) to ensure that the link function between the dependent and independent variables was of the Gaussian family. Second, we centred the SDI relative to each period (1990 and 2019) to ensure the absence of multi-collinearity between regressors in each model (the Variance Inflation Factor was inferior to 2 for each model). For each baseline model, we report a residuals versus fitted values plot to check that our baseline models generally satisfied assumptions of linearity and homoscedasticity of residuals (Supplementary Material, pp. 3–4).
The results of these additional analyses are briefly discussed in the ‘Results’ section and reported in detail in the Supplementary Material (pp. 6–8).
Results
Table 1 reports the mean, standard deviation and range of DALYs for mental and substance use disorders and self-harm, as well as of the SDI, across the six world regions and both time periods.
Summary Statistics of Disease Burden Estimates and Socio-Demographic Index for Each World Region and Time Period.
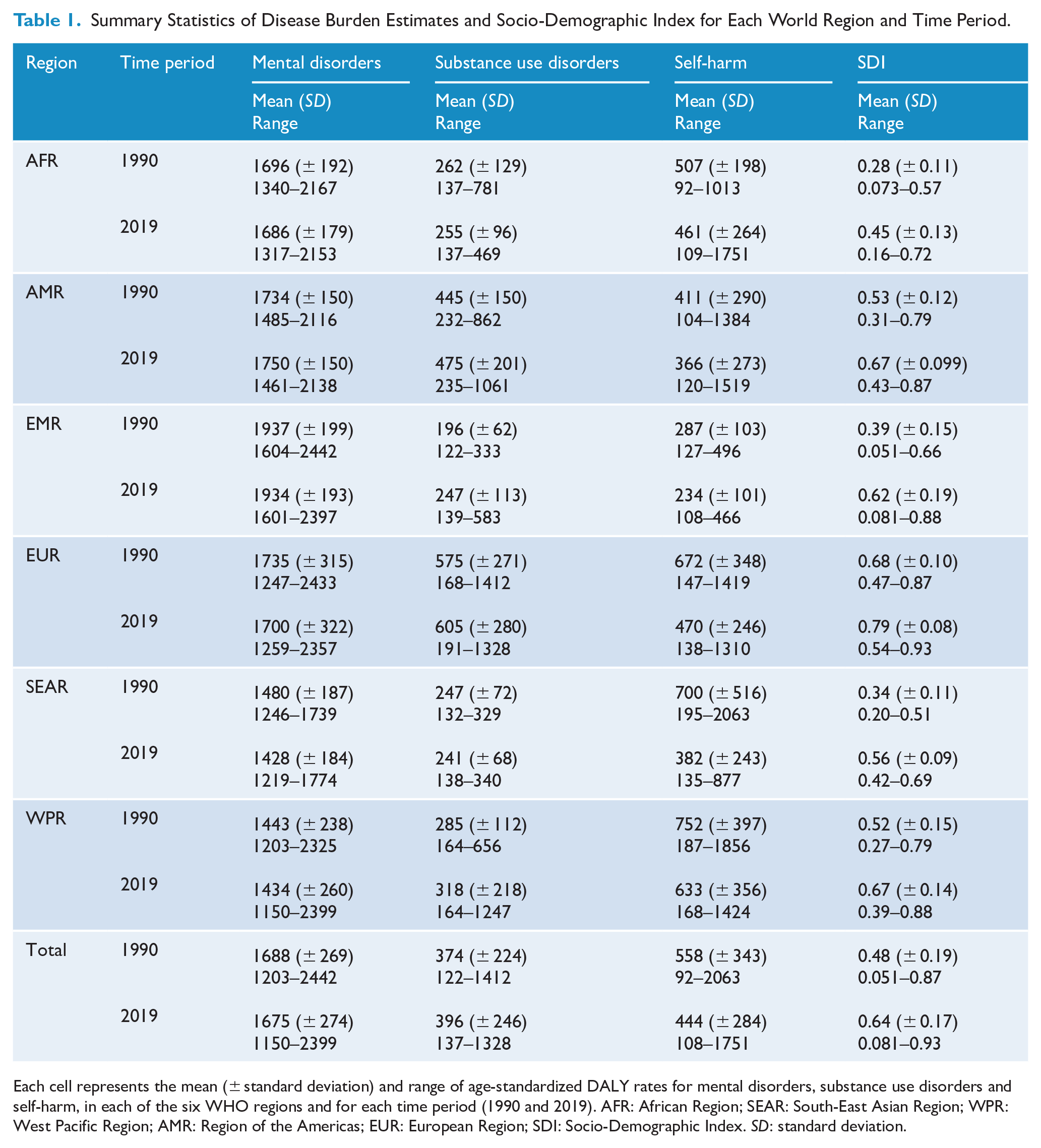
Each cell represents the mean (± standard deviation) and range of age-standardized DALY rates for mental disorders, substance use disorders and self-harm, in each of the six WHO regions and for each time period (1990 and 2019). AFR: African Region; SEAR: South-East Asian Region; WPR: West Pacific Region; AMR: Region of the Americas; EUR: European Region; SDI: Socio-Demographic Index. SD: standard deviation.
Baseline statistical models for each condition (Model 1)
We first aimed at investigating the effect of SDI, as well as heterogeneous effects across regions and time periods, on standardized DALY rates separately for each condition.
For mental disorders (Figure 1), there was no significant relationship between SDI and standardized DALY rates (T = –0.23; p = 0.82). DALYs were lower in 2019 than in 1990 (T = –2.2; p = 0.03) and differed significantly between regions (F = 17.4; p < 0.001 – see Supplementary Material, p. 6, for specific regional effects). Our analysis also showed a significant SDI × Region interaction, reflecting that the effect of SDI on DALYs differed between regions (F = 3.1; p = 0.01). This was driven by a negative association between SDI and DALYs in SEAR (T =−2.3; p = 0.02), and a positive association between SDI and DALYs in EUR (T = 3.5; p < 0.001). The SDI × Time and SDI × Region × Time interactions were non-significant (p > 0.32). Marginal and conditional R2 were of 0.34 and 0.98, respectively.
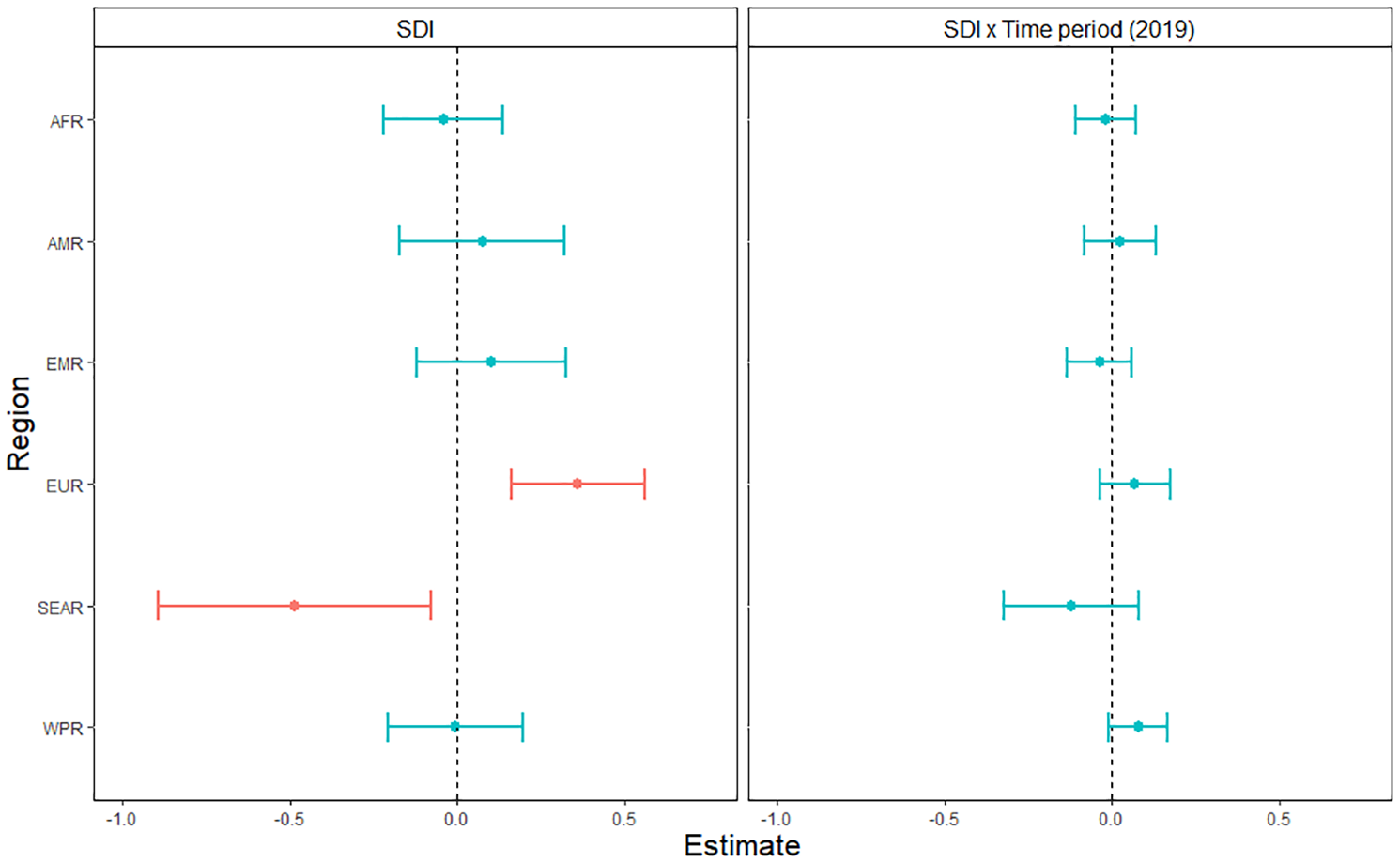
Association between age-standardized DALY rates for mental disorders and the Socio-Demographic Index across six world regions and years 2019 versus 1990.
For substance use disorders (Figure 2), there was a significantly positive relationship between SDI and standardized DALY rates (T = 2.0; p = 0.04). DALYs were significantly higher in 2019 than in 1990 (T = 4.2; p < 0.001). There was an overall main effect of Region (F = 18.0; p < 0.001 – Supplementary Material, p. 7). Our analysis also showed a significant SDI × Region interaction (F = 2.4; p = 0.04), driven by a positive association between DALYs and SDI in AFR (T = 3.2; p = 0.001). In addition, there was a significant Region × Time interaction (F = 4.4; p < 0.001 – Supplementary Material, p. 7). There was no SDI × Time interaction (T = 0.8; p = 0.43). Finally, we observed a three-way SDI × Region × Time interaction (F = 2.5; p = 0.03), where, in AFR, the relationship between SDI and DALYs was negative in 2019 compared to 1990 (T = –2.6; p = 0.009), while in EMR, the relationship was positive in 2019 compared to 1990 (T = 1.9; p = 0.05). Marginal and conditional R2 were of 0.62 and 0.96, respectively.
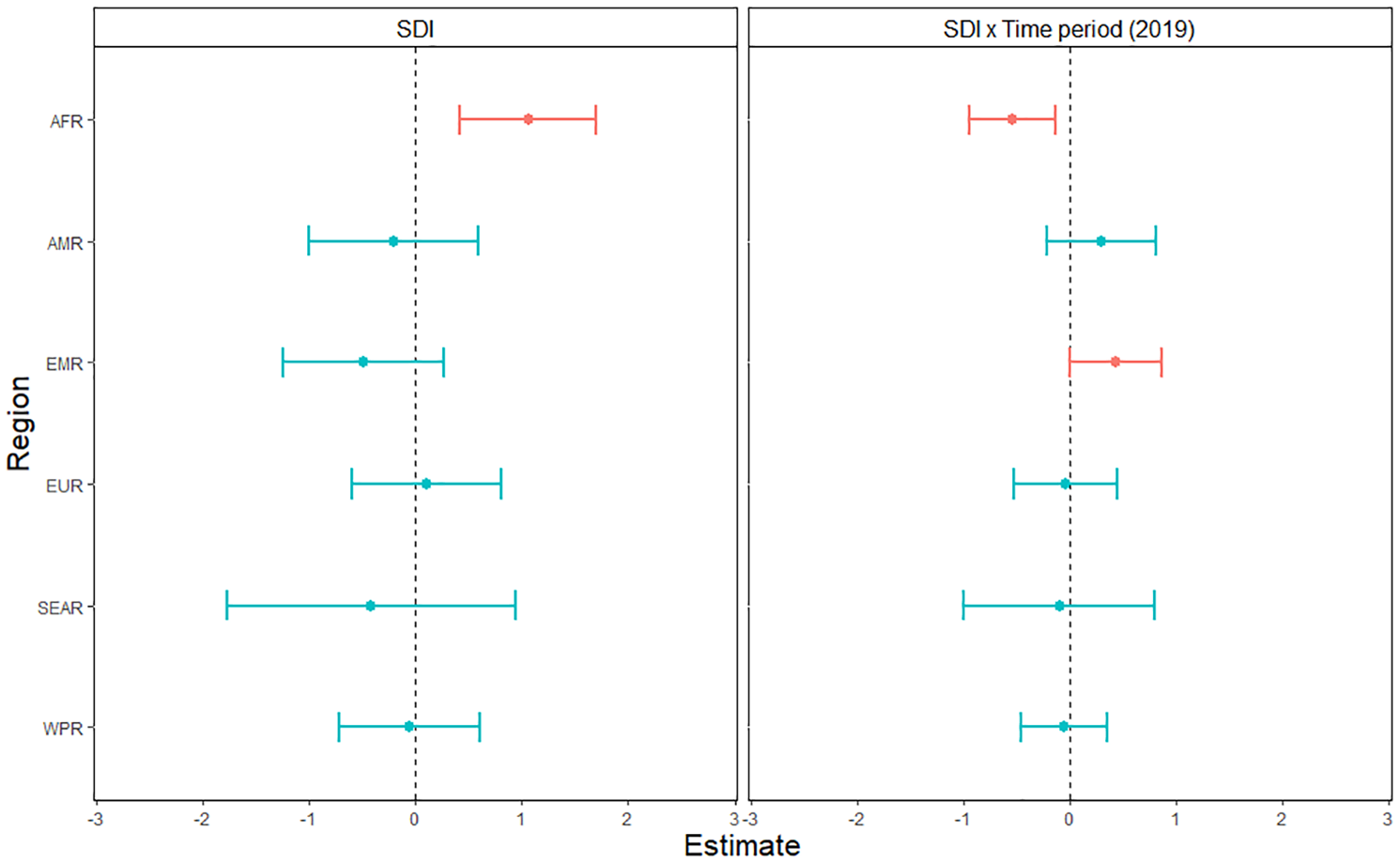
Association between age-standardized DALY rates for substance use disorders and the Socio-Demographic Index across six world regions and years 2019 versus 1990.
For self-harm (Figure 3), there was no significant relationship between SDI and standardized DALY rates (T = –0.85; p = 0.40). DALYs were significantly lower in 2019 than in 1990 (T = –3.5; p < 0.001). There was an overall main effect of Region (F = 11.6; p < 0.001 – Supplementary Material, p. 8). There was also a SDI × Region interaction (F = 2.5; p = 0.03), driven by a negative and marginal association between SDI and DALYs in EMR (T = –1.9; p = 0.06) and WPR (T = –1.7; p = 0.08), and a positive association in EUR (T = 2.5; p = 0.01). In addition, we observed a Time × Region interaction (F = 3.9; p = 0.002 – Supplementary Material, p. 8). While there was no SDI × Time interaction (T = –1.3; p = 0.19), we retrieved a SDI × Region × Time interaction (F = 3.0; p = 0.01), where the association between SDI and DALYs in EUR was negative in 2019 compared to 1990 (T = –3.5; p < 0.001),. Marginal and conditional R2 were of 0.28 and 0.88, respectively.
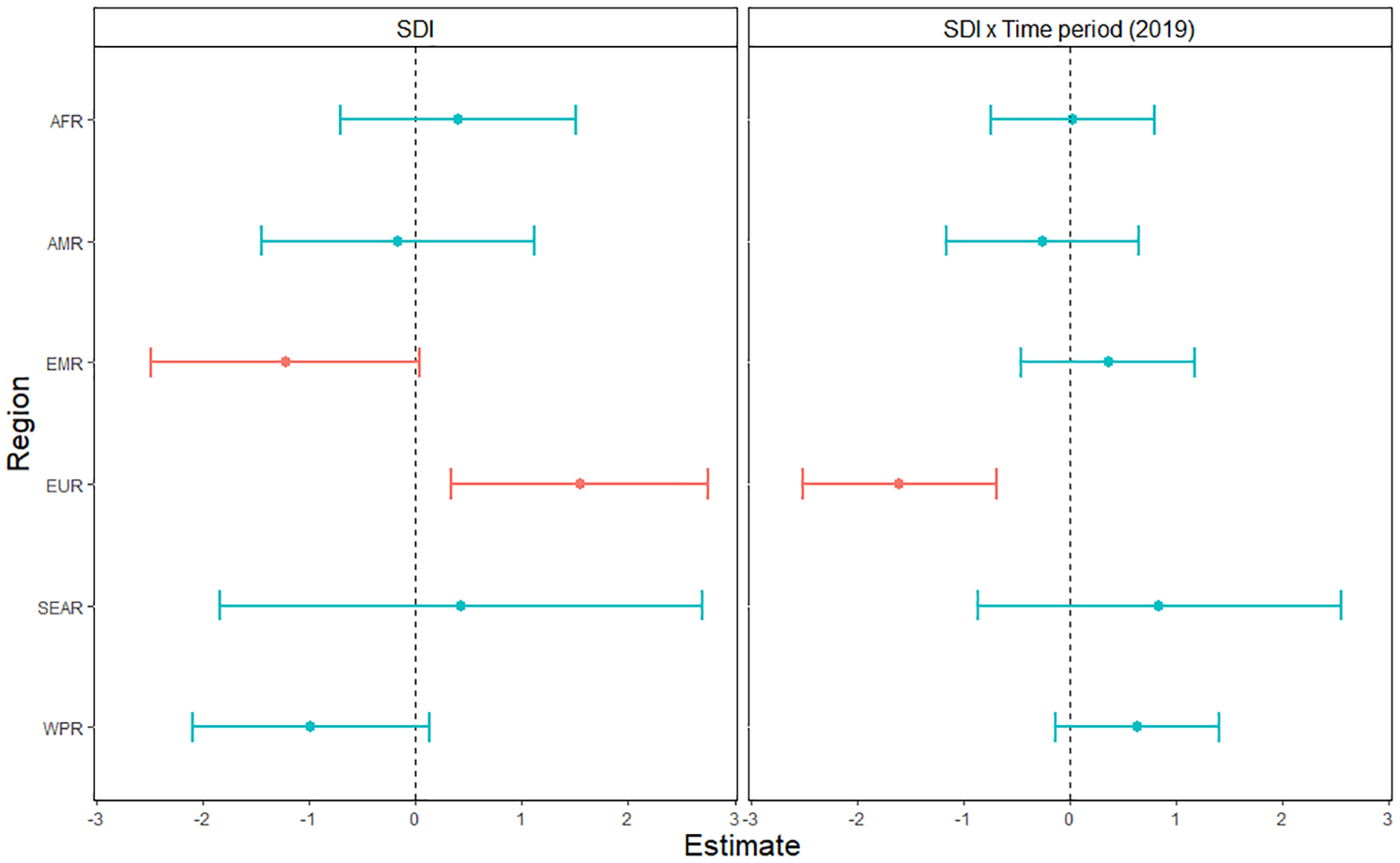
Association between age-standardized DALY rates for self-harm and the Socio-Demographic Index across six world regions and years 2019 versus 1990.
Sensitivity analysis (Models 2–5)
Results were generally not affected by down-weighing outlier observations (Models 2), adding other socio-demographic covariates (income inequality, unemployment rate, population size and health expenditure: Models 3), adding the number of available sources per location and condition as a covariate (Models 4), and running our analysis on those locations with a higher rating of data quality (Models 5) (Supplementary Material, pp. 5–8). Only one major difference was observed: for self-harm, including socio-demographic covariates removed the (marginal) statistical significance of the SDI × WPR coefficient (Model 3). Other significant results remained significant (or marginally significant) despite these adjustments.
Of note, when running our analysis on locations with high-quality observations, mental disorders and self-harm demonstrated a significantly positive relationship with SDI (Model 5), contingent on the fact that SDI was positively associated with DALYs in EUR in the baseline models for both these conditions. In contrast, locations with high-quality observations did not demonstrate a positive relationship with SDI for substance use disorders as SDI was not positively related to DALYs in EUR or AMR (Model 5).
Discussion
In the current study, we tested the association between socio-demographic development and the burden of mental and substance use disorders, and self-harm, across six world regions and between years 1990 and 2019. We designed our study to enlighten the current debate around the relationship between a country’s level of development and the burden of mental and behavioural problems. We used data from the GBD study 2019, which provides the most comprehensive database of morbi-mortality worldwide, as well as a measure of socio-demographic development based on income per capita, fertility rates and level of education (Vos et al., 2020).
Overall, we retrieved a positive association between a country’s level of development and its burden of disease for substance use disorders only. Associations for mental disorders and self-harm were non-significant across world regions and time periods. However, we found that the effects of development are heterogeneous across geographical regions and between time periods. In certain regions of the globe, more developed countries present with a greater burden of mental and behavioural disorders. These relatively worrying regional patterns were predominantly found in Africa for substance use disorders and in Europe for mental disorders and self-harm. Previous studies have reported a similar pattern of results (though they did not differentiate across world regions), and have hypothesized that they could be accounted for by lower levels of social support and greater competition for instant reward in more developed and individualistic societies (Barbalat and Franck, 2020; Dückers et al., 2019).
Other regions demonstrated an opposite, more reassuring pattern, where increased development was associated with decreased disease burden, for example, in South-East Asia for mental disorders or the EMR for self-harm. For instance, economic and social development has undoubtedly contributed to a significant investment in suicide prevention, an uplift of community mental health programmes, and a more enabling legal and policy framework for mental health in many parts of South-East Asia (e.g. the Mental Health Act in India: Firdosi and Ahmad, 2016). Other factors, not studied here, may have affected the relationship between mental and behavioural conditions with socioeconomic factors across geographical regions, factors that may reflect differences in biological and cultural backgrounds (Essau et al., 2011; Schreier et al., 2010).
In addition, we found that these regional patterns are not fixated and can change over time, both positively and negatively. These temporal changes could be the result of socioeconomic shocks, or changes in health and social policies that may affect access to and quality of care. For instance, in Europe, our results point towards a negative relationship between socio-demographic development in 2019 compared to 1990 for self-harm, which somehow mitigates the overall positive association of development with mental disorders and self-harm observed at the regional level. Efforts focusing on patients suffering from mental health crises in Europe are a potential explanatory factor for this reassuring temporal trend (Malone et al., 2009; Shields-Zeeman et al., 2020). Over the past few decades, there have been significant investments and action plans on behalf of WHO Europe as well as from the European Commission to improve access to mental health care in Europe (e.g. European Commission, 2005). This has helped narrow the gaps in parts of Central and Eastern Europe regarding mental health systems development, which might have predominantly impacted mental health emergencies. Our results also depict other temporal fluctuations of regional patterns, such as the strengthening of the association between development and DALYs for substance use disorders in 2019 compared to 1990 in the EMR or the weakening of this association in Africa. Further research is needed to explore this regional and temporal variability and the role of cultural and socioeconomic factors that could explain and limit the burden of mental and behavioural conditions.
Because we showed that the association between development and disease burden could be both positive and negative depending on conditions, world regions and time periods, our results can be seen as compatible with previous studies suggesting both a positive and negative link between a country’s vulnerability and its prevalence of mental and substance use disorders, and suicide (Degenhardt et al., 2018; Dückers and Brewin, 2016; Dückers et al., 2016, 2019; Jorm and Mulder, 2021). Yet, our results suggest that subtle and specific geographical and temporal factors are responsible for cross-national differences in the burden of mental and behavioural problems, rather than, or in addition to, vulnerability or development per se. In other words, if our data confirm the theoretical validity of research studies investigating the effects of socio-demographic development on mental health, they mostly put a strong emphasis on these factors and encourage further research aiming to better understand their link to mental and behavioural conditions.
Our study has several important strengths. First, data from the GBD study allowed the extraction of disease burden estimates for 204 countries and territories across the world, which included data from low-income countries. This represents a serious quantitative improvement compared to previous studies (Dückers and Brewin, 2016; Dückers et al., 2016, 2019; Jorm and Mulder, 2021). Second, this quantitative improvement is also associated with a qualitative uplift. The GBD 2019 study used a large number of sources to estimate disease burden and synthesized these sources to produce consistent estimates across locations with sparse, unavailable or low-quality data. More generally, some countries may have very different understandings of concepts related to mental illness and development. In that sense, our results offer both a more holistic and nuanced view of the relationship between country-level development with mental and behavioural disabilities. Third, this increased number of observations allowed us to test for heterogeneous effects across geographical and temporal dimensions. To our knowledge, this is the first time that temporal and regional sources of variability are examined in an ecological study that seeks to investigate the relationship between development with the burden of mental and substance use disorders and self-harm. Fourth, our study design allowed us to determine the effect of socio-demographic development on DALYs independent of specific geographical and temporal effects, as well as their interaction, since they were included – hence explained away – in our statistical models. Likewise, our results are independent of a country’s age structure as we used age-standardized DALY rates as our outcome variable. Fifth, our sensitivity analyses allowed us to take data quality and uncertainty into account; down-weigh outlier observations; and control for time-varying country-level socio-demographic variables such as unemployment rate, income inequality, health expenditure and population size. In general, these sensitivity analyses confirmed findings from our baseline models, even though the fact that Africa showed a positive association between DALYs and SDI for substance use disorders warrants confirmation with high-quality datasets.
There are, however, a few limitations to our study. First and most importantly, we acknowledge that estimates obtained from the GBD study 2019 may be imprecise. Although the GBD study 2019 used various statistical adjustments and modelling techniques that are substantial improvements from previous GBD rounds, calculating estimates and UIs in locations with sparse, unavailable and low-quality data is necessarily prone to inaccuracies. Therefore, patterns that we were able to identify in the current study warrant confirmation.
Second, in the current study, we were mostly interested in testing the association between development and disease burden for mental and substance use disorders and self-harm, focussing primarily on mental and behavioural conditions as they are generally fragmented in health care services. However, different mental and substance use disorders would inevitably have various relationships with development (Degenhardt et al., 2018). For instance, eating disorders, that some have categorized as full-blown cultural disorders predominant in rich countries, could be more associated with socio-demographic development than, say, autism which is often regarded as highly biological (Lee, 1996; State and Šestan, 2012). Further studies should examine the relationship between development and the burden of disease at a lower level, investigating specific diagnosis rather than higher-level causes or conditions.
Third, the division of countries into regions defined by the WHO is well accepted, and thought to be meaningful in terms of organization and cultural values (Hofstede, 2010; Schwartz, 2006; Stankov et al., 2014). Yet, at the same time, there is arguably an important within-region variability in terms of socio-demographic and cultural characteristics relevant to health and health care. In particular, WHO regions can include both high-income and low-income countries in the same cluster, or countries with different stages of mental health system development. Although our model fits were relatively high, a substantial proportion of the variance was explained by countries random effects. This suggests that variations in the burden of disease for mental and behavioural conditions are also unique to each country. We acknowledge that future studies should examine this within-region variability at a finer level.
Despite these limitations, our study provides evidence that qualifies current theories relating socio-demographic development to the burden of mental and substance use disorders and self-harm. Using data from the GBD study 2019, the most comprehensive source of burden estimates worldwide, we found that the association between development and the burden of these conditions shows significant heterogeneous effects along temporal and geographical dimensions. These are likely related to geographical and temporal variations in health care policies; socio-cultural norms; and attitudes towards illnesses characterized by cognitive, emotional and behavioural disturbances. Better knowledge of this spatial and temporal variability could help understand why certain regions of the globe develop at the cost of an increased burden of mental conditions. This could be crucial in an era where at least one in four suffer from a mental problem (Bebbington and McManus, 2020).
Supplemental Material
sj-pdf-1-anp-10.1177_00048674211066764 – Supplemental material for Socio-demographic development and burden of mental, substance use disorders, and self-harm: An ecological analysis using the Global Burden of Disease study 2019
Supplemental material, sj-pdf-1-anp-10.1177_00048674211066764 for Socio-demographic development and burden of mental, substance use disorders, and self-harm: An ecological analysis using the Global Burden of Disease study 2019 by Guillaume Barbalat and Sze Liu in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.