
Abstract
Background:
Young people with a mental disorder often perform poorly at school and can fail to complete high school. This study aims to compare scholastic performance and high school completion of young people hospitalised with a mental disorder compared to young people not hospitalised for a mental disorder health condition by gender.
Method:
A population-based matched case-comparison cohort study of young people aged ⩽18 years hospitalised for a mental disorder during 2005–2018 in New South Wales, Australia using linked birth, health, education and mortality records. The comparison cohort was matched on age, gender and residential postcode. Generalised linear mixed modelling examined risk of school performance below the national minimum standard and generalised linear regression examined risk of not completing high school for young people with a mental disorder compared to matched peers.
Results:
Young males with a mental disorder had over a 1.7 times higher risk of not achieving the national minimum standard for numeracy (adjusted relative risk: 1.71; 95% confidence interval: [1.35, 2.15]) and reading (adjusted relative risk: 1.99; 95% confidence interval: [1.80, 2.20]) compared to matched peers. Young females with a mental disorder had around 1.5 times higher risk of not achieving the national minimum standard for numeracy (adjusted relative risk: 1.50; 95% confidence interval: [1.14, 1.96]) compared to matched peers. Both young males and females with a disorder had around a three times higher risk of not completing high school compared to peers. Young males with multiple disorders had up to a sixfold increased risk and young females with multiple disorders had up to an eightfold increased risk of not completing high school compared to peers.
Conclusion:
Early recognition and support could improve school performance and educational outcomes for young people who were hospitalised with a mental disorder. This support should be provided in conjunction with access to mental health services and school involvement and assistance.
Background
Internationally, mental disorders account for around 16% of the global burden of disease among young people (Kessler et al., 2007). In Australia, around 14% of young people are estimated to experience a mental disorder in 2013–2014 (Lawrence et al., 2016). Mental disorders can have an adverse impact on a young person’s home life, ability to relate to peers, and on their academic performance (Leach and Butterworth, 2012; Suldo et al., 2014). The presence of a mental disorder is usually apparent by age 14 (Kessler et al., 2007); therefore, early recognition, treatment and support are key to improving health and education outcomes.
Poor mental health can be both a cause and effect of academic problems (DeSocio and Hootman, 2004). Inconsistent school attendance can be an early indicator of poor mental health among young people and also the social circumstances contributing to the emergence of a mental disorder (DeSocio and Hootman, 2004). Single or comorbid mental disorders can negatively influence a young person’s educational performance through their effect on a student’s engagement with learning (Breslau et al., 2011; Productivity Commission, 2020). The perception of poor academic competence can in turn result in decreased motivation to engage at school (Breslau et al., 2011). In particular, early-onset depressive disorder in otherwise capable students has been associated with poor performance on school assessments, lower grades and poor peer relationships (Fletcher, 2008).
Some students with a mental disorder struggle to complete high school (Bowman et al., 2017; Leach and Butterworth, 2012; Mental Health Commission, 2021). An estimated one-third of students diagnosed with a mental disorder during adolescence do not enter tertiary college in the United States (Breslau et al., 2008). Poor academic performance can be both a mediator for dropping out of high school (Quiroga et al., 2013) and a predictor of high school dropout (Bowman et al., 2017; Sagatun et al., 2014) for students with a mental disorder.
The consequences of not completing high school can include a lower income, reduced stability in relationships and employment, greater reliance on government financial assistance and poor general health associated with lower socioeconomic status (Breslau et al., 2008, 2011; Kessler et al., 1995; Larson et al., 2017). The likelihood of not completing high school may vary for different types of mental disorders (Breslau et al., 2008) and by gender (Leach and Butterworth, 2012), differences which to date have been underexamined (Deighton et al., 2018). This study aims to compare scholastic performance and high school completion of young people hospitalised for a mental disorder compared to young people not hospitalised for a mental disorder by gender.
Method
A retrospective population-level case-comparison cohort study of young people hospitalised for a mental disorder aged ⩽18 years in New South Wales (NSW), Australia using linked birth, health, education and mortality administrative data collections from 1 January 2005 to 31 December 2018 (Mitchell et al., 2019). Ethical approval and a waiver of consent were obtained from the NSW Population and Health Services Research Ethics Committee (2018HRE0904).
Data sources
Information on hospital service use was obtained from emergency department (ED) visit and hospital admission data collections. ED visits to public hospitals included information on arrival and departure times, visit type and provisional diagnosis. Hospitalisations included admissions to public and private hospitals, and contained demographic information, diagnoses, separation type (i.e. hospital transfers, death) and clinical procedures. The NSW Registry of Births, Deaths and Marriages provided mortality data for the study period and young people who died during the study period were excluded from analyses (Supplementary Figure 1).
Information on the number and type of ambulatory specialist mental health services at public hospitals was obtained from the ambulatory mental health client contacts database from 1 January 2006 to 30 September 2019. This included mental health day programmes, public psychiatric outpatients and outreach services.
School performance and parental demographic information was obtained from annual National Assessment Plan for Literacy and Numeracy (NAPLAN) assessments conducted in May during 2008 to 2018 for government, Catholic and independent schools. Assessments were conducted on young people in primary school grades 3 (7–9 years of age) and 5 (9–11 years of age), and secondary school grades 7 (11–13 years of age) and 9 (13–15 years of age) and included assessments in both numeracy and reading. Within each assessment, scores represent the same level of achievement over time (Australian Curriculum Assessment and Reporting Authority [ACARA], 2019). Each score is translated into proficiency bands that indicate whether performance was above, at or below the national minimum standard (NMS). Inability to achieve the NMS indicates that a young person will have difficulty making progress in school without assistance (ACARA, 2017).
Information on a young person’s attendance, absence, withdrawal (e.g. philosophical objections to testing or religious beliefs) or exemption due to significant disability was obtained (Supplementary Table 1). Young people exempt from sitting an assessment due to severe disability or language difficulties were rated as scoring below the NMS as per technical guidelines (ACARA, 2014).
A young person was identified as having a language background other than English (LBOTE) if either they or their parent or guardians spoke a language other than English at home (ACARA, 2019). Where there were multiple records of the parents’ level of education, the highest level of education of either parent was identified. Information on high school completion at years 10 (15–16 years of age), 11 (17–18 years of age) and 12 (17–18 years of age) were obtained through the Record of School Achievement, and the Higher School Certificate.
The Centre for Health Record Linkage (CHeReL) identified the population comparison group and linked the birth, health and education records using probabilistic record linkage. Upper and lower probability cut-offs for a link were 0.75 and 0.25 and record groups with probabilities between the cut-offs were clerically reviewed.
Case inclusion criteria
Young people with a year of birth ⩾1997 who were aged ⩽18 years at hospital admission with a principal or additional diagnosis of a mental disorder in up to 50 additional diagnosis classifications (International Classification of Diseases, 10th Revision, Australian Modification [ICD-10-AM]) during 1 January 2005 to 31 December 2018 (Supplementary Table 2). Cases were included if the young person completed both the numerical and reading NAPLAN assessments in a school grade. The number of mental disorders experienced by the young person was categorised as 1 or ⩾2 disorders.
Population-comparison group criteria
A population-based comparison group not hospitalised for a mental disorder from 1 July 2001 to 31 December 2018 was randomly selected from NSW birth records matched 1:1 on age, gender and residential postcode to their counterpart. The comparison selection time frame included a 3.5-year wash out period prior to the case selection time frame to avoid the potential selection of comparisons that may have been hospitalised for a mental disorder prior to the case criteria time frame.
Geographical location and socioeconomic status
Geographical location of residence was assigned using the Australian Statistical Geographical Standard (ASGS) and the young person’s residential postcode based on distance to service centres (Australian Bureau of Statistics, 2013). The ASGS categories were classified as urban (i.e. major cities) and rural (i.e. inner and outer regional, remote and very remote). NAPLAN records provided the remoteness area of the school and was categorised as major city, inner regional, outer regional or remote (Australian Bureau of Statistics, 2013). The young person’s postcode of residence was used to partition socioeconomic disadvantage into quintiles from most (i.e. 1) to least disadvantaged (i.e. 5) (Australian Bureau of Statistics, 2011).
Identification of chronic health conditions
Common comorbidities for young people were identified from prevalence studies (Edwards et al., 2012; Miller et al., 2013; Mitchell et al., 2017) and were those that would reasonably be expected to last 12 months or result in the need for ongoing healthcare (Miller et al., 2013). For this study, a chronic health condition was identified using a 3-year lookback period (to 1 January 2002) and diagnosis classifications from ICD-10-AM (Supplementary Table 3).
Data organisation and analysis
Data analysis was conducted using SAS 9.4 (SAS Institute, Cary, NC). All hospital episodes of care related to the same event were linked to form a period of care. Chi-square tests of independence and Wilcoxon Mann–Whitney tests were used to examine characteristics of young people hospitalised for a mental disorder and their counterpart. The number of ED visits, hospital admissions and hospital length of stay (LOS) before and during and also after the index admission were identified for both the young person with a mental disorder and their matched peer for each NAPLAN assessment. The calculation of hospital LOS was cumulative and included transfers between hospitals.
To examine school performance at each grade, Poisson regression models with robust variance estimators (Zou, 2004) using PROC GENMOD were used to assess the difference in proportions of performances below the NMS for each assessment domain for the school grades 3, 5, 7 and 9 for young people hospitalised for a mental disorder and their matched peers. Adjusted relative risks (ARRs) and 95% confidence intervals (CIs) were calculated. For each domain, sequential forward selection was used to sequentially add covariates to the model (Mitchell et al., 2019) and significance was assessed using p-values (p < 0.05) to examine the overall effect in the model. The final models included mental disorder status, gender, comorbidity status (Y/N), socioeconomic status, highest level of education for any parent/guardian (i.e. ⩽Year 12; certificate I-IV, trade or diploma; bachelor or higher degree or other), highest level of any parent/guardian occupation (i.e. senior manager/qualified professional; business manager/associate professional; trades/clerks/skilled office/sales and service; machine operators/hospitality/assistants/labourers; or not in paid work in last 12 months) and a log of hospital LOS. As comparison group members could have nil hospital LOS, a constant value was added to LOS before transformation (Woodward, 2005) (Supplementary Table 4).
Generalised linear mixed modelling (GLMM) was conducted to perform multi-level modelling of school performance below the NMS for the numeracy and reading assessment domains for young people and their counterpart who had completed multiple grades of schooling. For each domain, PROC GLIMMIX was used with a binary distribution, log link function and Kenward and Roger denominator degrees of freedom. The residual option of the random statement was used to model R-side covariance and data were analysed to account for within student correlation in the longitudinal data and repeated measurements using an autoregressive covariance structure. ARRs and 95% CIs were generated. The final models for all persons included mental health status, NAPLAN grade (i.e. 3, 5, 7, 9), gender, comorbidity status (Y/N), LBOTE, socioeconomic status, highest level of education for any parent/guardian (i.e. bachelor or higher degree or other), log of hospital LOS and a school sector (i.e. government, Catholic, independent). Each model was then separately run by gender using the same covariates, excluding gender.
Factors associated with high school completion at either year 10, 11 or 12 for young people hospitalised for a mental disorder compared to their counterparts was examined using generalised linear regression using PROC GENMOD. For each grade, models were fitted using generalised estimating equations (GEEs) with binomial distribution and a log function. ARR and 95% CIs were calculated. The final models for all persons included mental health status, gender, comorbidity status (Y/N), LBOTE, socioeconomic status, highest level of education for any parent/guardian and geographic location of residence. Where sample sizes allowed, modelling was conducted separately by gender for all mental disorders and the number of mental disorders using the same covariates, excluding gender.
Results
During 2015–2018, there were 7069 young people hospitalised with a mental disorder for whom a matched comparison could be identified and who completed the NAPLAN assessments in Grade 3; 6203 in Grade 5; 5009 in Grade 7; and 3374 in Grade 9. There were 8575 young people with a mental disorder hospitalised with a matched peer who could have completed year 10; 7497 year 11; and 6063 year 12 of high school.
Across grades 3 to 9, there was a higher proportion of young females (57.9–63.1%) compared to males, and a higher proportion of young people in urban locations (70.7–73.2%) compared to rural locations hospitalised for a mental disorder. Most young people (⩾83%) were from English-speaking households and almost all (⩾96%) had no other health condition identified. Young people with a mental disorder had a higher proportion of parents completing year 11 high school or equivalent and were not in paid employment in the last 12 months than their matched peers for each grade. Young people hospitalised for a mental disorder had higher mean ED visits, hospital admissions, hospital LOS, and pre- and post-ambulatory mental health service contacts than their matched counterparts in each grade (Table 1).
Demographic and healthcare use characteristics of young people hospitalised for a mental health condition and their matched comparison by school grade, linked health and school performance data NSW, 2005–2018.
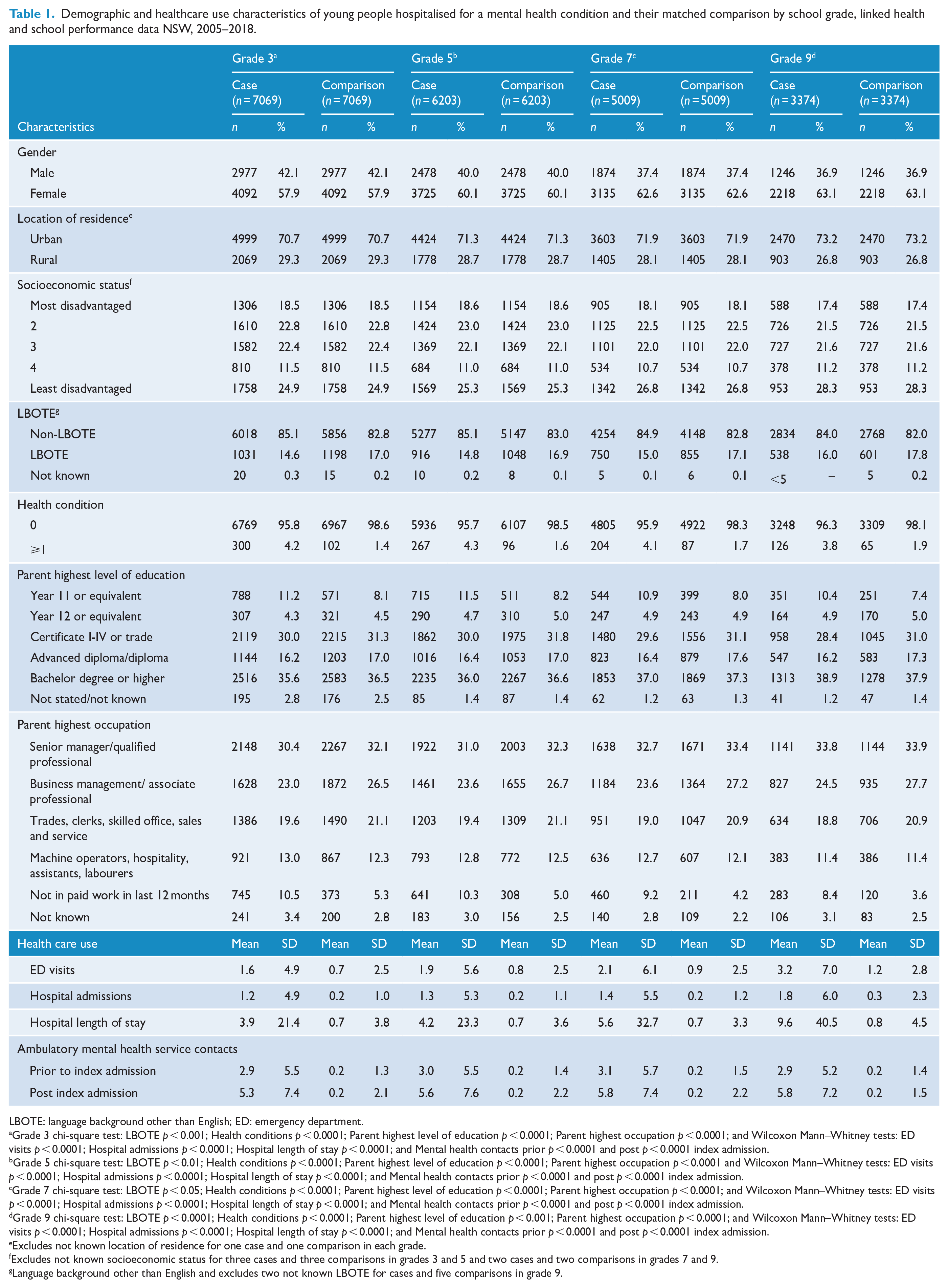
LBOTE: language background other than English; ED: emergency department.
Grade 3 chi-square test: LBOTE p < 0.001; Health conditions p < 0.0001; Parent highest level of education p < 0.0001; Parent highest occupation p < 0.0001; and Wilcoxon Mann–Whitney tests: ED visits p < 0.0001; Hospital admissions p < 0.0001; Hospital length of stay p < 0.0001; and Mental health contacts prior p < 0.0001 and post p < 0.0001 index admission.
Grade 5 chi-square test: LBOTE p < 0.01; Health conditions p < 0.0001; Parent highest level of education p < 0.0001; Parent highest occupation p < 0.0001 and Wilcoxon Mann–Whitney tests: ED visits p < 0.0001; Hospital admissions p < 0.0001; Hospital length of stay p < 0.0001; and Mental health contacts prior p < 0.0001 and post p < 0.0001 index admission.
Grade 7 chi-square test: LBOTE p < 0.05; Health conditions p < 0.0001; Parent highest level of education p < 0.0001; Parent highest occupation p < 0.0001; and Wilcoxon Mann–Whitney tests: ED visits p < 0.0001; Hospital admissions p < 0.0001; Hospital length of stay p < 0.0001; and Mental health contacts prior p < 0.0001 and post p < 0.0001 index admission.
Grade 9 chi-square test: LBOTE p < 0.0001; Health conditions p < 0.0001; Parent highest level of education p < 0.001; Parent highest occupation p < 0.0001; and Wilcoxon Mann–Whitney tests: ED visits p < 0.0001; Hospital admissions p < 0.0001; Hospital length of stay p < 0.0001; and Mental health contacts prior p < 0.0001 and post p < 0.0001 index admission.
Excludes not known location of residence for one case and one comparison in each grade.
Excludes not known socioeconomic status for three cases and three comparisons in grades 3 and 5 and two cases and two comparisons in grades 7 and 9.
Language background other than English and excludes two not known LBOTE for cases and five comparisons in grade 9.
While all young people predominantly attended government schools in major cities, the type of school attended and its geographic location differed for young people with a mental disorder compared to matched peers for each grade. There was a higher proportion of young people with a mental disorder attending government schools and attending schools in major cities compared to matched peers. At least double the proportion of young people hospitalised with a mental disorder did not achieve the NMS for their school assessments across grades 3–9 compared to their matched counterparts (Table 2).
School and NAPLAN assessment characteristics of young people hospitalised for a mental health condition and their matched comparison by school grade, linked health and school performance data NSW, 2005–2018.
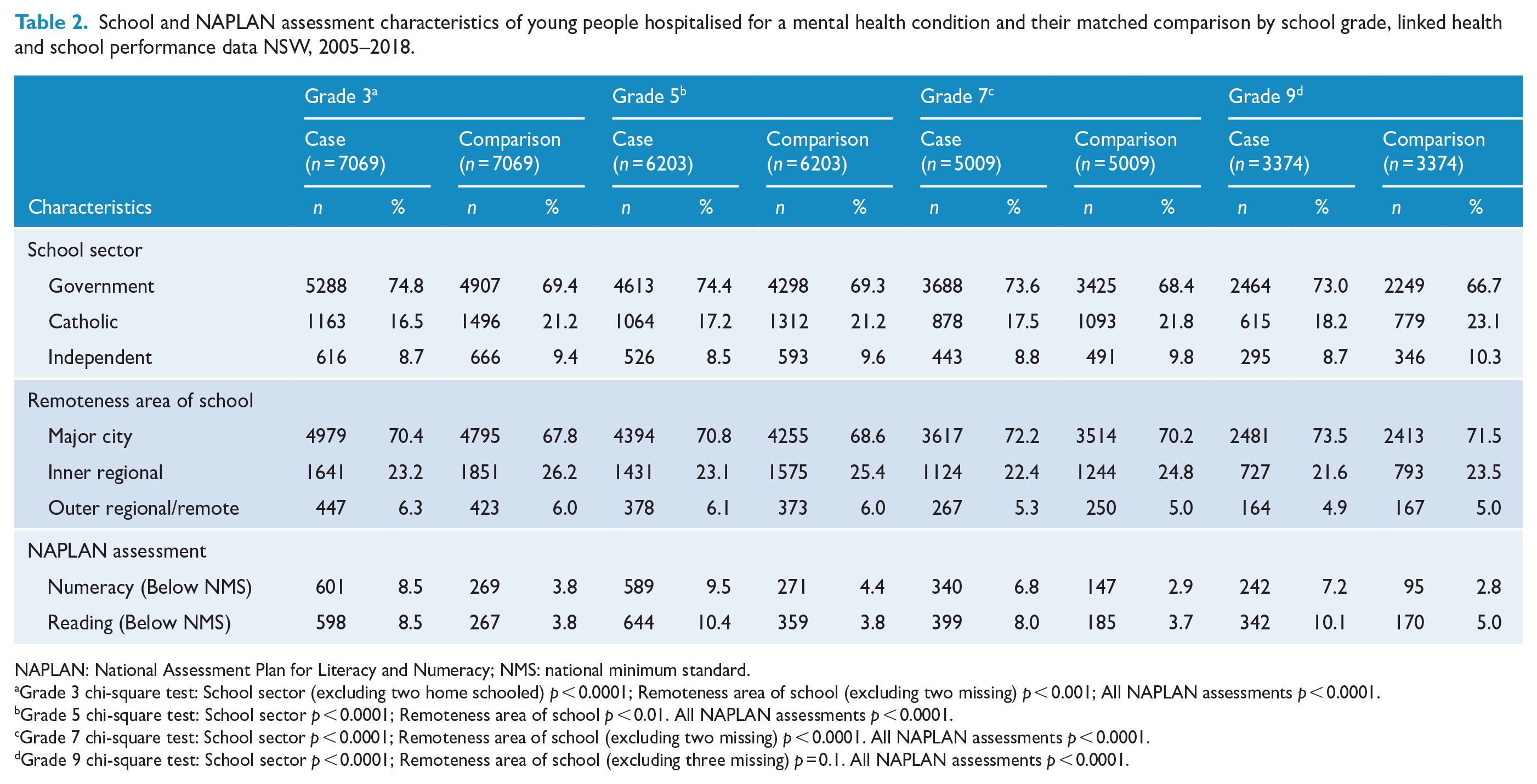
NAPLAN: National Assessment Plan for Literacy and Numeracy; NMS: national minimum standard.
Grade 3 chi-square test: School sector (excluding two home schooled) p < 0.0001; Remoteness area of school (excluding two missing) p < 0.001; All NAPLAN assessments p < 0.0001.
Grade 5 chi-square test: School sector p < 0.0001; Remoteness area of school p < 0.01. All NAPLAN assessments p < 0.0001.
Grade 7 chi-square test: School sector p < 0.0001; Remoteness area of school (excluding two missing) p < 0.0001. All NAPLAN assessments p < 0.0001.
Grade 9 chi-square test: School sector p < 0.0001; Remoteness area of school (excluding three missing) p = 0.1. All NAPLAN assessments p < 0.0001.
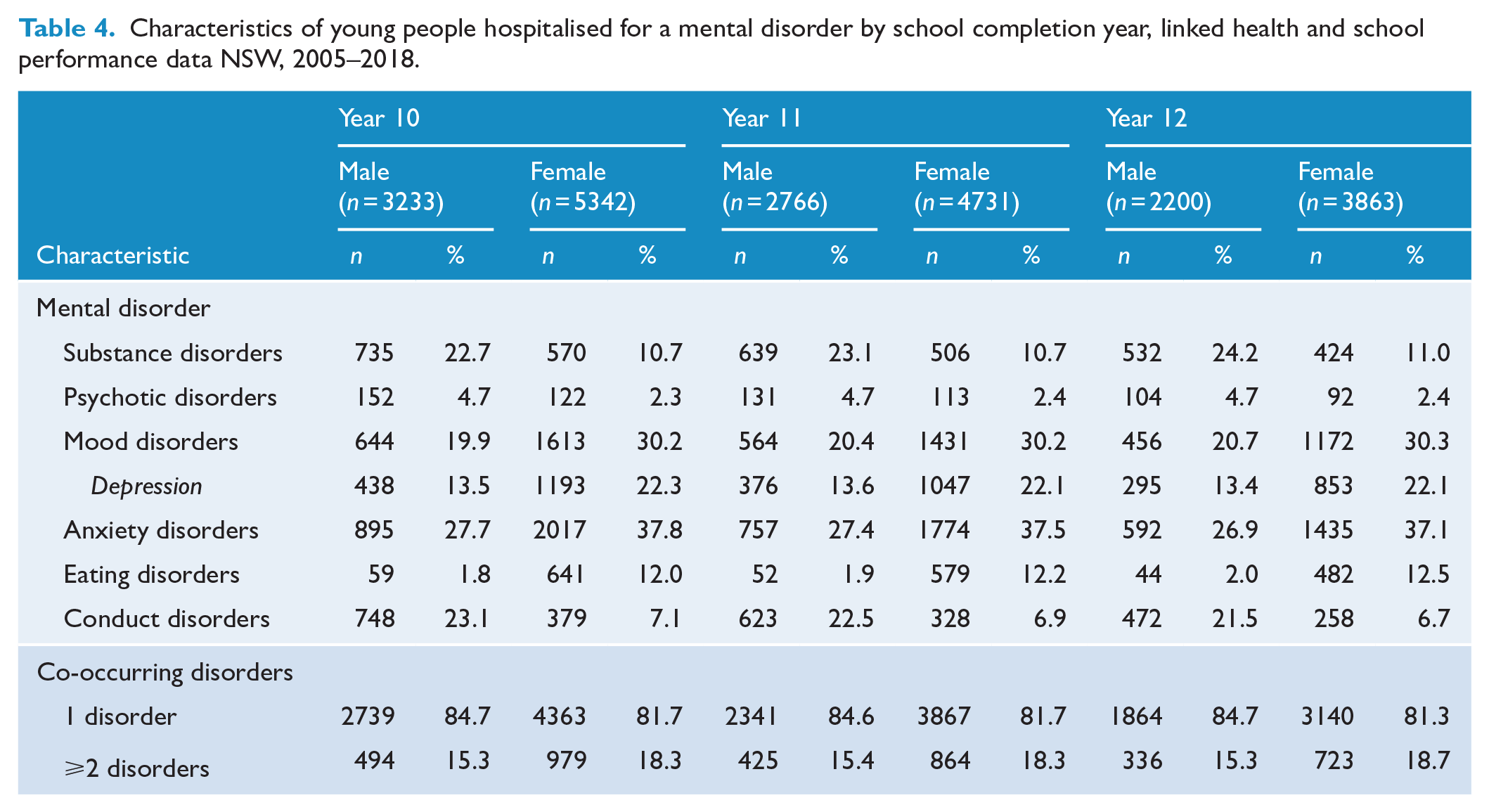
For young people who were hospitalised with a mental disorder and completed school assessments, the most common diagnoses for males between school year 3 to year 9 were conduct (27.8–41.9%) and anxiety (29.3–31.0%) disorders. For females, the most common diagnoses were anxiety (38.2–39.1%) and mood (23.0–27.2%) disorders. Young females (11.8–14.0%) had a higher proportion of eating disorders than young males (2.0–2.3%) in all grades (Table 3). In the comparison of high school completions from year 10 to year 12, anxiety (26.9–27.7%), conduct (21.5–23.1%) and substance (22.7–24.2%) disorders were the most common diagnoses among young males. Anxiety (37.1–37.8%) and mood (30.2–30.3%) disorders were the most common diagnoses for young females in this schooling period (Table 4).
Characteristics of young people hospitalised for a mental disorder by school grade, linked health and school performance data NSW, 2005–2018.
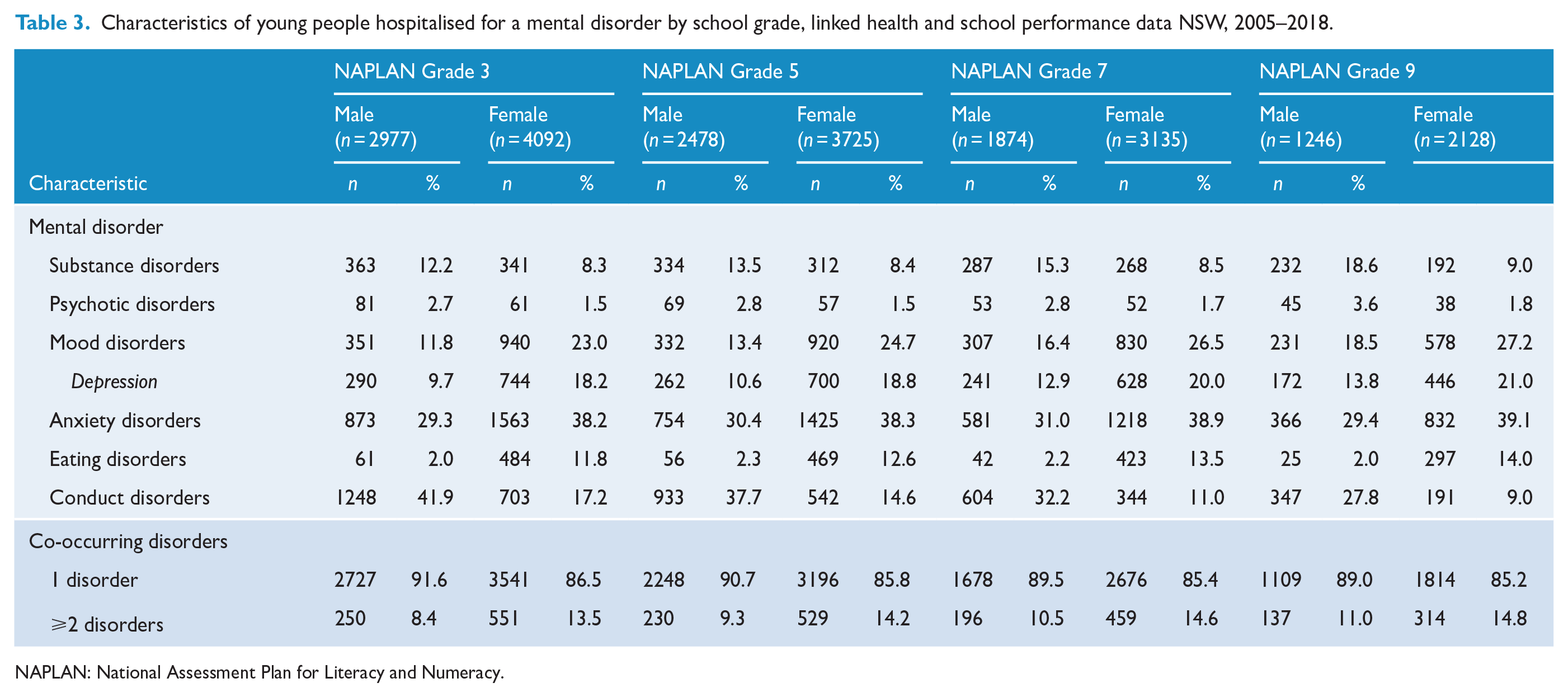
NAPLAN: National Assessment Plan for Literacy and Numeracy.
Characteristics of young people hospitalised for a mental disorder by school completion year, linked health and school performance data NSW, 2005–2018.
Young males hospitalised for a mental disorder had over a 1.7 times higher risk of not achieving the NMS on school assessments for numeracy (ARR: 1.71; 95% CI: [1.35, 2.15]) and reading (ARR: 1.99; 95% CI: [1.80, 2.20]) compared to matched counterparts. For psychotic and conduct disorders, young males had around twice the risk, and for anxiety males had over 1.5 times higher risk of not achieving the NMS in school assessments compared to matched peers. Young females with a mental disorder had around 1.5 times higher risk of not achieving the NMS for numeracy (ARR: 1.50; 95% CI: [1.14, 1.96]) compared to matched peers. For young females, there was around twice the risk of not achieving the NMS for conduct disorders for each assessment compared to matched peers. Both young males and females with depression had around a 1.5 times higher risk of not achieving the NMS for numeracy (ARR: 1.56; 95% CI: [1.22, 1.99]) and reading (ARR: 1.45; 95% CI: [1.04, 2.02]), respectively, compared to matched counterparts. There was no increased risk of not achieving the NMS for mood disorders for males and females or for eating disorders for females compared to matched peers. Both male and female students with ⩾2 disorders had twice the risk of not achieving the NMS for numeracy (ARR: 2.35; 95% CI: [1.28, 4.32] and ARR: 2.39; 95% CI: [1.86, 3.08], respectively) compared to matched peers (Table 5).
Multilevel model of mental disorders associated with a below NMS NAPLAN assessment for young people with an index hospitalisation for during 2005–2018 compared to a matched comparison by gender and assessment type, linked health and school performance data NSW.
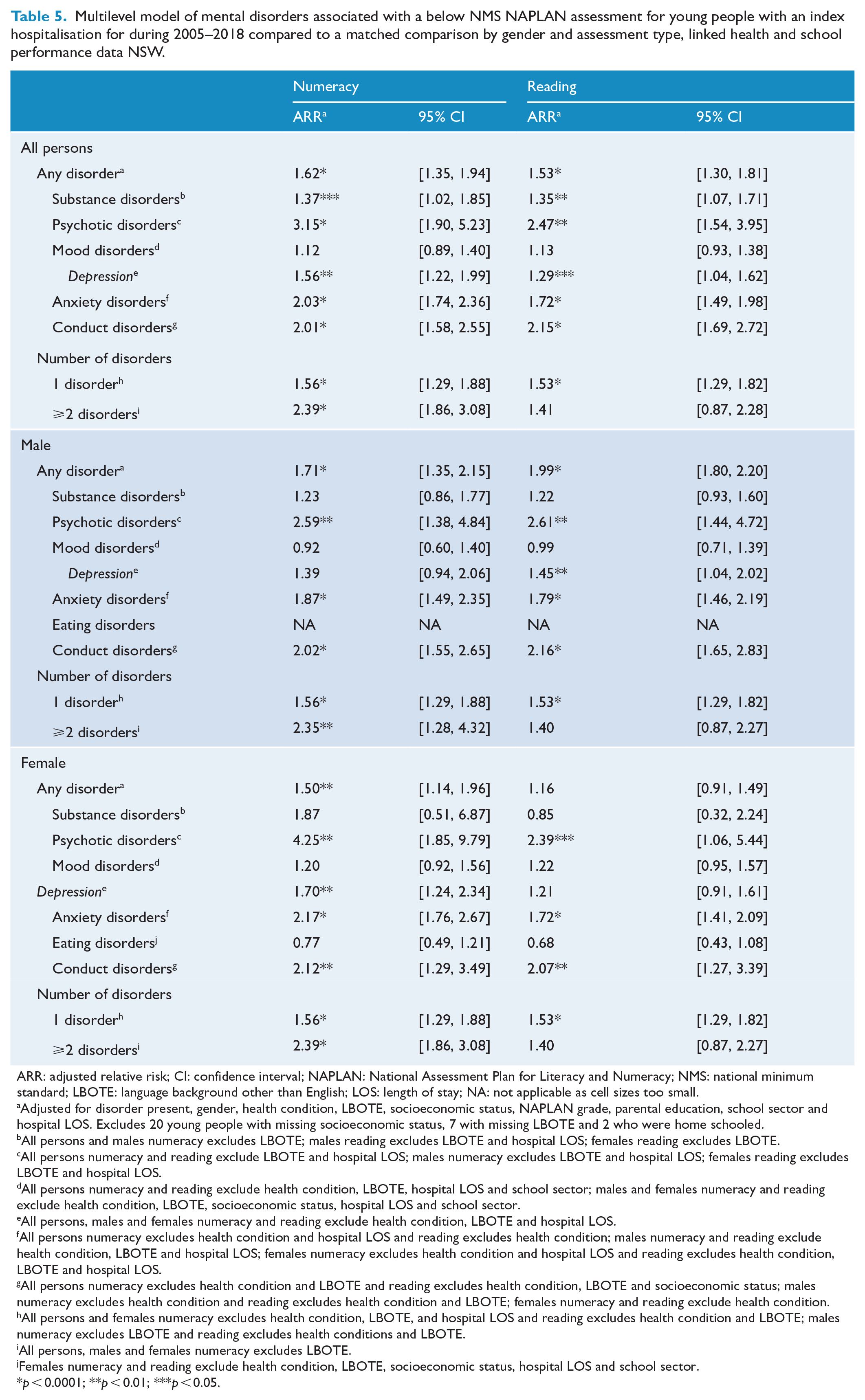
ARR: adjusted relative risk; CI: confidence interval; NAPLAN: National Assessment Plan for Literacy and Numeracy; NMS: national minimum standard; LBOTE: language background other than English; LOS: length of stay; NA: not applicable as cell sizes too small.
Adjusted for disorder present, gender, health condition, LBOTE, socioeconomic status, NAPLAN grade, parental education, school sector and hospital LOS. Excludes 20 young people with missing socioeconomic status, 7 with missing LBOTE and 2 who were home schooled.
All persons and males numeracy excludes LBOTE; males reading excludes LBOTE and hospital LOS; females reading excludes LBOTE.
All persons numeracy and reading exclude LBOTE and hospital LOS; males numeracy excludes LBOTE and hospital LOS; females reading excludes LBOTE and hospital LOS.
All persons numeracy and reading exclude health condition, LBOTE, hospital LOS and school sector; males and females numeracy and reading exclude health condition, LBOTE, socioeconomic status, hospital LOS and school sector.
All persons, males and females numeracy and reading exclude health condition, LBOTE and hospital LOS.
All persons numeracy excludes health condition and hospital LOS and reading excludes health condition; males numeracy and reading exclude health condition, LBOTE and hospital LOS; females numeracy excludes health condition and hospital LOS and reading excludes health condition, LBOTE and hospital LOS.
All persons numeracy excludes health condition and LBOTE and reading excludes health condition, LBOTE and socioeconomic status; males numeracy excludes health condition and reading excludes health condition and LBOTE; females numeracy and reading exclude health condition.
All persons and females numeracy excludes health condition, LBOTE, and hospital LOS and reading excludes health condition and LBOTE; males numeracy excludes LBOTE and reading excludes health conditions and LBOTE.
All persons, males and females numeracy excludes LBOTE.
Females numeracy and reading exclude health condition, LBOTE, socioeconomic status, hospital LOS and school sector.
p < 0.0001; **p < 0.01; ***p < 0.05.
Demographic and healthcare use characteristics of young people hospitalised with a mental health disorder and their matched peers by school completion year are shown in Supplementary Table 5. Both young males and females hospitalised with a mental disorder had around a three times higher risk, and young people hospitalised for substance disorders had four times the risk, of not completing year 10, 11 or 12 of high school than their matched counterparts. Young people with mood, anxiety and conduct disorders had between three to four times higher risk of not completing year 10, 11 or 12 than matched peers. Young people with psychotic disorders had a three and four times higher risk of not completing year 11 or 12, respectively, compared to matched peers. Young females with an eating disorder had around twice the risk of not completing year 11 or 12 compared to matched counterparts. Young people with ⩾2 disorders had between five and seven times higher risk of not completing year 10, 11 or 12 compared to matched peers (Table 6).
Analysis of characteristics associated with not completing high school for young people with an index hospitalisation for a mental disorder compared to a matched comparison by school grade, linked health and school performance data NSW, 2005–2018.
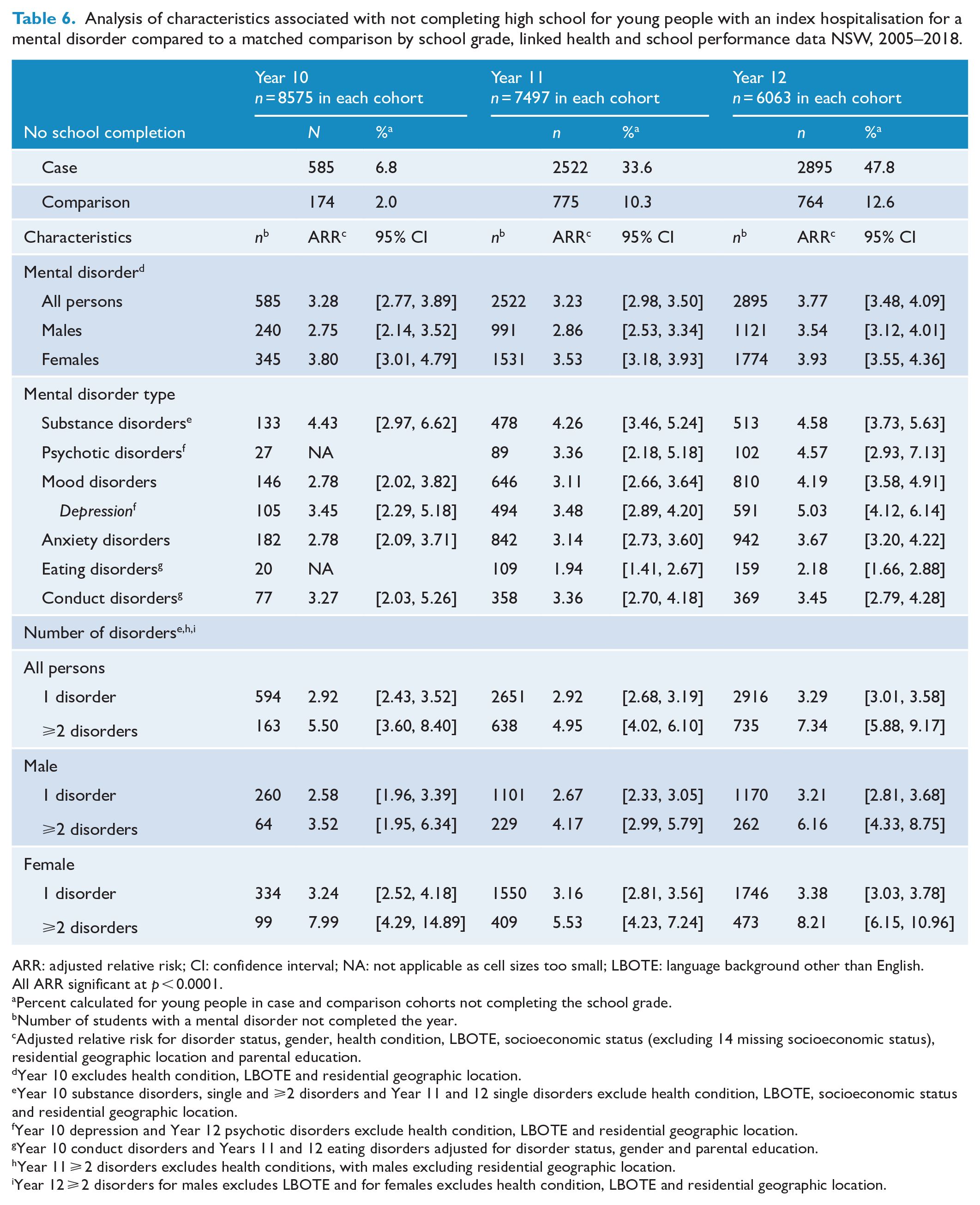
ARR: adjusted relative risk; CI: confidence interval; NA: not applicable as cell sizes too small; LBOTE: language background other than English.
All ARR significant at p < 0.0001.
Percent calculated for young people in case and comparison cohorts not completing the school grade.
Number of students with a mental disorder not completed the year.
Adjusted relative risk for disorder status, gender, health condition, LBOTE, socioeconomic status (excluding 14 missing socioeconomic status), residential geographic location and parental education.
Year 10 excludes health condition, LBOTE and residential geographic location.
Year 10 substance disorders, single and ⩾2 disorders and Year 11 and 12 single disorders exclude health condition, LBOTE, socioeconomic status and residential geographic location.
Year 10 depression and Year 12 psychotic disorders exclude health condition, LBOTE and residential geographic location.
Year 10 conduct disorders and Years 11 and 12 eating disorders adjusted for disorder status, gender and parental education.
Year 11 ⩾ 2 disorders excludes health conditions, with males excluding residential geographic location.
Year 12 ⩾ 2 disorders for males excludes LBOTE and for females excludes health condition, LBOTE and residential geographic location.
Discussion
This study demonstrates the strong association between a young person being admitted to hospital for treatment of a range of mental disorders and a higher risk of not achieving a minimum standard for literacy and numeracy, and of not completing high school, when compared to matched peers. It found that young males with a mental disorder had over a 1.7 times higher risk of not achieving the NMS on numeracy and reading school assessments and that young males with psychotic, conduct and anxiety disorders had around twice the risk of not achieving the NMS compared to matched peers. Young females with a mental disorder had around 1.5 times higher risk of not achieving the NMS for numeracy and that females with psychotic, anxiety or conduct disorders had between 1.5 and 4 times higher risk of not achieving the NMS in assessments compared to matched counterparts. Young males and females with a mental disorder had around a three times higher risk of not completing high school compared to matched peers.
Poor academic performance and a higher risk of not completing high school compared to peers was evident for both young males and females with either internalising (e.g. anxiety, depression) or externalising (e.g. conduct, substance) disorders as has been shown elsewhere (Bowman et al., 2017; Breslau et al., 2008, 2011; Kessler et al., 1995; Leach and Butterworth, 2012; McLeod et al., 2012; Townsend et al., 2007). Psychotic, conduct and anxiety disorders were more strongly associated with poor school performance than depression and substance disorders in the current study. Both anxiety and depression in young people can adversely affect concentration, ability to process information and decision-making, thereby impairing social and cognitive functioning and ability to learn (Quiroga et al., 2013; Wood, 2006), which in turn can lead to school dropout due to perceived poor academic competence (Quiroga et al., 2013).
Young males and females with conduct disorders had twice the risk of not achieving the NMS in school assessments compared to matched peers and a three times higher risk of not completing high school in the current study. Conduct disorders can result in negative behaviour, such as disruptive, aggressive, inattentive behaviour or acting out, and these students can be difficult for teachers to engage in classroom learning. In the United States, students with conduct disorders had twice the likelihood of not completing high school and had a one and a half times higher likelihood of not commencing college (Kessler et al., 1995). However, the effect of conduct disorders on a student’s educational performance can be somewhat attenuated after controlling for attention deficit disorder (Breslau et al., 2008). Disentangling the effects of comorbid disorders, their interrelationship and impact on educational attainment remains an ongoing issue, with the potential of joint effects of different disorders (Breslau et al., 2011). In the current study, from grade 3 to high school between 8.4% and 15.4% of males and 13.5% and 18.7% of females had ⩾2 disorders. However, the sample size was not large enough to investigate potential joint effects of comorbid disorders.
Poor mental health can be a barrier to academic performance and school completion (Leach and Butterworth, 2012). Many young people with a mental disorder experience engagement difficulties in the school environment (Roeser et al., 1998). That some young people with a mental disorder are not achieving minimum standards for numeracy and reading is of concern. The ability to read is a foundational skill required to excel in almost all other academic subjects (Daniel et al., 2006) and poor reading ability is known to be associated with not completing high school (Daniel et al., 2006). Numeracy skills are also fundamental prerequisites in many aspects of day-to-day later life (Geary, 2011).
Young people with multiple mental disorders generally had a higher risk of not achieving the NMS on school assessment tasks and had at least double the risk of not completing high school compared to young people who were diagnosed with a single disorder. Likewise, previous research found that young people with multiple mental disorders attained lower levels of education than those with a single disorder (Breslau et al., 2008; McLeod et al., 2012). Young people with comorbid anxiety and depression often exhibit greater overall severity of symptoms, psychological distress, life interference and can have poorer long-term prognosis than young people with unitary disorders (Breslau et al., 2008).
While high school dropout is likely to be influenced by a number of factors, a young person’s mental health and their academic performance is not unidirectional, but rather they are likely to be reciprocally related (Roeser et al., 1998; Suldo et al., 2014). Initial identification of students with a mental disorder is critical and ongoing support services are vital as generally there is low recognition and diagnosis of mental disorders among the young (Fletcher, 2008). Screening young people who drop out of high school as a potential flag for also experiencing mental health issues could be an option (Breslau et al., 2008), as it is generally 1–4 years before a young person with a disorder will seek mental health services (Bowman et al., 2017). In the United States, it is estimated that between 10% and 46% of attrition from high school can be attributed to the adverse effects of mental disorders (Breslau et al., 2008; Vander Stoep et al., 2003).
Types of support for young people with a mental disorder include symptom management, peer counselling, personal support and social connections, and access to general practitioner and other specialist mental health services (McIntyre et al., 2018; Vander Stoep et al., 2003; Wilson et al., 2008), although access to services in rural and remote areas can be challenging (Bowman et al., 2017). The few targeted nonpharmacological interventions that have shown promise vary by disorder type, but have included interventions based on cognitive behavioural therapy for anxiety disorders and depression (Dray et al., 2017) and parent-group interventions have been found to reduce externalising behaviours (Buchanan-Pascall et al., 2018; Dretzke et al., 2009). There is also potential for school involvement to support a young person experiencing severe mental health concerns through school psychologists, Head Teacher Welfare, and Learning and Support Teams. It is possible that mental health training for educators could assist in improving their knowledge and confidence to promote good mental health among young people (Moon et al., 2017).
Future research could consider which factors may act as either mediators and moderators for a student’s academic performance or high school completion. Whether academic performance at primary school can predict academic difficulties in high school or high school dropout should also be explored, along with the identification of factors predictive of resilience for students with a mental disorder. The potential for reciprocal effects over time could also be investigated, with some parents placing increasing pressure on young people with a mental disorder to perform academically.
This was a large population-based study linking health and educational records over a 13-year period. However, there were some study limitations. The study was not able to separate admissions to child and adolescent units that included school attendance as part of the programme, or admissions to juvenile justice facilities, which also encourage participation in education, or from long admissions that were likely to result in missing a significant part of a school year, for example, to eating disorder units. A small number of residential postcodes were not known to the authors and socioeconomic status for these was not able to be identified. The recency of residential postcode may vary between datasets, which may affect estimates of socioeconomic status. Only comorbid health conditions relevant to a hospital admission are indicated in diagnosis classifications, so it is possible that some comorbidities experienced by young people could be under-enumerated. This is particularly likely for the comparison cohort, where 38.6% had not been admitted to hospital, so there was no opportunity to identify comorbidities, despite the 3-year lookback period.
The study only included young people who had been hospitalised, so did not include young people presenting solely to other health professionals for treatment. In Australia, the threshold for hospitalisation of young people is quite high, as there are comparatively few specialist inpatient beds, and also an uneven distribution of those beds around NSW. The main reasons for inpatient care are primarily concern for the safety of the young person and also identification of the type of disorder for which a consistent inpatient programme is required, for example, a severe eating disorder. Hence, hospitalised young people are likely to be the most seriously affected, regardless of diagnosis and irrespective of the number of days spent in hospital. While the cohort sample size was large, the number of factors able to be adjusted for in analyses was reduced due to low sample sizes for each disorder type by gender. Nor was it possible to determine the direction of any effects of disorders and school performance.
No information was available on the exact age at the onset of the mental disorder and information on ambulatory mental health contacts was only available from 2006. No assessment of data validity was able to be conducted and it is possible that there could be some data misclassification. Visits to private hospital EDs were not able to be accessed. A higher proportion of young people with a mental disorder were absent for NAPLAN assessments compared to their matched counterparts. The current study was not able to take into account school absences or school clustering, nor was it able to identify age at the onset of the mental health disorder from hospitalisation records or examine the proximity of hospital admission to NAPLAN tests or the final year of school for individual subjects. No information was available regarding any special education services, school exclusions (suspension or expulsion) or tutoring received by a young person.
Conclusion
This was a comprehensive investigation of the impact of mental disorders on academic performance and completion by disorder type and gender. Young people hospitalised with a mental disorder are not performing as well as their peers in school-based assessments and they have a higher risk of not completing high school. Disengagement from education may be ameliorated by early recognition and support aimed at enhancing school performance and educational outcomes for young people with a mental disorder. This support should be provided in conjunction with mental health services and school involvement and assistance. Young people should not be disadvantaged in their educational pursuits due to poor mental health as the consequences in terms of employment opportunities, overall health and relationship stability can be lifelong.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211061684 – Supplemental material for Mental disorders and their impact on school performance and high school completion by gender in Australia: A matched population-based cohort study
Supplemental material, sj-docx-1-anp-10.1177_00048674211061684 for Mental disorders and their impact on school performance and high school completion by gender in Australia: A matched population-based cohort study by Rebecca J Mitchell, Anne McMaugh, Carolyn Schniering, Cate M Cameron, Reidar P Lystad, Tim Badgery-Parker and Olav Nielssen in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors wish to thank the NSW Ministry of Health for providing access to the ED visit, hospitalisation and mortality data; NSW Department of Education for providing access to school enrolment and completion information; the NSW Education Standards Authority for providing access to the NAPLAN data; and the Centre for Health Record Linkage for conducting the data linkage.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by a philanthropic donor to Macquarie University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.