
Abstract
Objective:
Post-traumatic stress disorder following injuries unrelated to mass casualty events has received little research attention in New Zealand. Internationally, most studies investigating predictors of post-injury post-traumatic stress disorder focus on hospitalised patients although most survivors are not hospitalised. We compared the prevalence and predictors of symptoms suggestive of post-traumatic stress disorder 12 months following injury among hospitalised and non-hospitalised entitlement claimants in New Zealand’s Accident Compensation Corporation. This government-funded universal no-fault insurance scheme replaced tort-based compensation for injuries in 1974 since when civil litigation (which can bias post-traumatic stress disorder estimates) has been rare.
Methods:
A total of 2220 Accident Compensation Corporation claimants aged 18–64 years recruited to the Prospective Outcomes of Injury Study were interviewed at 12 months post-injury to identify symptoms suggestive of post-traumatic stress disorder using the Impact of Events Scale. Multivariable models examined the extent to which baseline sociodemographic, injury, health status and service interaction factors predicted the risk of post-traumatic stress disorder symptoms among hospitalised and non-hospitalised groups.
Results:
Symptoms suggestive of post-traumatic stress disorder were reported by 17% of hospitalised and 12% of non-hospitalised participants. Perceived threat to life at the time of the injury doubled this risk among hospitalised (adjusted relative risk: 2.0; 95% confidence interval: 1.2–3.2) and non-hospitalised (relative risk: 1.8; 95% confidence interval: 1.2–2.8) participants. Among hospitalised participants, other predictors included female gender, Pacific and ‘other’ minority ethnic groups, pre-injury depressive symptoms, financial insecurity and perceived inadequacies in healthcare interactions, specifically information and time to discuss problems. Among non-hospitalised survivors, predictors included smoking, hazardous drinking, assault and poor expectations of recovery.
Conclusion:
One in six hospitalised and one in eight non-hospitalised people reported post-traumatic stress disorder symptoms 12 months following injury. Perceived threat to life was a strong predictor of this risk in both groups. Identifying early predictors of post-traumatic stress disorder, regardless of whether the injury required hospitalisation, could help target tailored interventions that can reduce longer-term psychosocial morbidity.
Keywords
Introduction
Age-standardised rates for serious injuries in New Zealand have increased in the past decade, largely due to a rise in non-fatal injuries. The rate of 233 serious non-fatal injuries per 100,000 people in 2019 was the highest since the current serious injury statistical definition was adopted in 2000 (Statistics New Zealand, 2020). As suggested by these data, advances in emergency and surgical care are accompanied by significant increases in survival from life-threatening injuries in many high-income countries. However, identifying and addressing longer-term psychological consequences in this high-risk population lacks robust attention even in jurisdictions with well-established trauma systems (deRoon-Cassini et al., 2019; Shalev et al., 2019; Zatzick et al., 2008). This need is challenged by the lack of systematic screening and follow-up of injury survivors, more subtle and subjective indicators of psychological distress (compared with acute and often catastrophic physical hallmarks of injury), complex recovery trajectories influenced by comorbid conditions and social determinants of health and inequitable access to post-acute healthcare, rehabilitation and support services. The limited attention to longer-term psychosocial outcomes of non-fatal injuries risks overlooking remediable factors that impose significant distress and high costs to individuals and society.
Post-traumatic stress disorder (PTSD) is among the strongest correlates of poor quality of life following injury (deRoon-Cassini et al., 2019; Zatzick et al., 2008) but the risk of PTSD following injuries unrelated to mass casualty events has received little attention in New Zealand. A study of 65 major trauma survivors admitted to Waikato Hospital found that 45% interviewed during the following year experienced symptoms suggestive of PTSD, but this estimate may reflect a degree of selection bias given the 40% response rate (Spijker et al., 2018). While most injury survivors are not hospitalised, most studies on PTSD focus on hospitalised patients (Brewin et al., 2000; Davydow et al., 2009; Russo et al., 2013; Skogstad et al., 2014). Among the rare comparative studies, a series from the Netherlands found higher risks of PTSD among hospitalised compared with non-hospitalised injury survivors early in the course but the difference attenuated beyond 12 months (Haagsma et al., 2011, 2012, 2013). The relative lack of information on the prevalence and predictors of PTSD among non-hospitalised people (who account for most injury survivors) can increase inequities in identifying and addressing post-injury PTSD at a population level.
To address these gaps in research evidence, we analysed data on self-reported symptoms suggestive of PTSD collected in a large prospective cohort study of injury survivors in New Zealand, a setting where litigation is uncommon and perverse incentives are unlikely to be a major source of bias. Elsewhere, researchers have raised concerns regarding ‘concept creep’ and secondary gain and misclassification of the diagnosis in jurisdictions where civil litigation is common (Alarcon et al., 2012; Elbers et al., 2013; Mezey and Robbins, 2001). An Australian study found that patients with compensable compared with non-compensable motor vehicle injuries had a significantly higher risk of PTSD at 24 months follow-up, after analyses controlled for differences between the groups in demographic and injury characteristics, pre-injury health, psychological conditions and quality of life (O’Donnell et al., 2010). In Saskatchewan, Canada, changing from a tort-based compensation system to a no-fault system that eliminated compensation for pain and suffering following traffic injuries led to a 28% reduction in the reported incidence of whiplash injury (Cassidy et al., 2000), a condition with litigation challenges similar to PTSD.
In 1974, the Accident Compensation Corporation (ACC) of New Zealand replaced tort-based compensation for all injuries with a government-funded universal ‘no-fault’ injury insurance scheme. Civil litigation has been exceptionally rare since (Bismark and Paterson, 2006). We investigated the risk of symptoms suggestive of PTSD 12 months following injury in a cohort of ACC entitlement claimants. Putative predictors of this risk examined in hospitalised and non-hospitalised injury survivors included demographic, pre-injury health risks; features relating to the injury and early post-injury factors including healthcare interactions.
Methods
This analysis draws on data from the Prospective Outcomes of Injury Study (POIS), a cohort study of 2856 injured people aged 18 to 64 years resident in five regions who were recruited from the ACC entitlement claims database between December 2007 and August 2009. Accredited health professionals refer injured people to ACC who then place injured people on this database if they are deemed by ACC to have injuries requiring support beyond medical only support, e.g. psychological, social or rehabilitative services or income compensation for lost income. People whose injury related to self-harm or sexual assault were excluded from POIS. Hospitalisations within 7 days of an injury (defined as the ‘hospitalised’ group) were determined by probabilistic linkage to New Zealand’s National Minimum Dataset of hospital discharges.
Comprehensive information regarding the study protocol (Derrett et al., 2009), relationship to principles in the Treaty of Waitangi (cession document signed between Māori and British Crown representatives in 1840) (Wyeth et al., 2010), recruitment (Derrett et al., 2011) and follow-up procedures (Langley et al., 2013), flow charts and factors relating to participation (Langley et al., 2013) have been published previously. The study was approved by the New Zealand Health and Disability Multi-region Ethics Committee (MEC/07/07/093) and all participants provided written informed consent.
Interviewer-administered questionnaires collected pre-injury and early post-injury data at the first (baseline) interview approximately 3 months following the injury event (median: 3.2 months; interquartile range: 2.5–4.2 months) and follow-up data at 12 months (median: 12.3 months; interquartile range: 12.0–13.0 months).
Measures
Symptoms suggestive of PTSD
The risk of self-reported symptoms suggestive of PTSD was assessed at the 12-month follow-up interview using the 15-item Impact of Event Scale (IES) (Brewin, 2005; Sundin and Horowitz, 2002) with a positive screen defined as a score of 27 or greater (Coffey et al., 2006). This widely used instrument in the research literature has established validity and reliability as a self-reported screening measure of PTSD (Sundin and Horowitz, 2002). However, it predates the introduction of PTSD into the Diagnostic and Statistical Manual of Mental Disorders classification, elicits symptoms relating to intrusion and avoidance but not hyperarousal. As the IES was designed as a screening measure rather than a diagnostic tool for PTSD (Sundin and Horowitz, 2002), our outcome measure is used to determine the proportion of injury survivors who report symptoms suggestive of PTSD.
Pre-injury demographic, health and personal characteristics
Age, sex, ethnicity and educational level data based on the Census (Statistics New Zealand, 2006) were gathered. As per the New Zealand Census question, participants could self-identify one or more ethnic groups. For descriptive purposes (Table 1) four binary variables were used to report this: ‘Māori’, ‘Pacific’, ‘Other’ and ‘Sole New Zealand European’.
Prevalence of symptoms suggestive of PTSD at 12 months by baseline demographic and health risk factors.
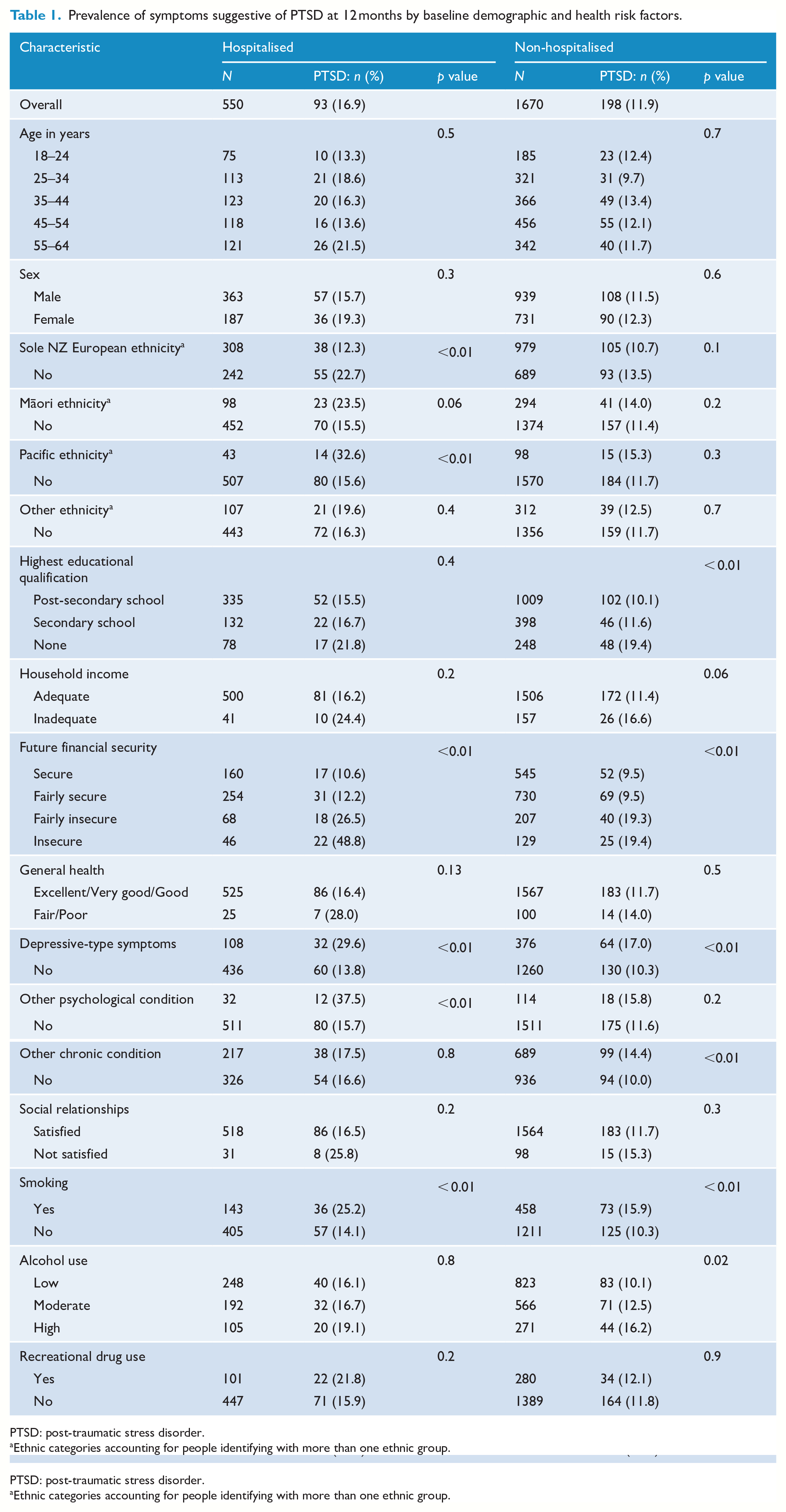
PTSD: post-traumatic stress disorder.
Ethnic categories accounting for people identifying with more than one ethnic group.
The ‘adequacy of pre-injury household income to meet every day needs’ was assessed using a question based on New Zealand’s Living Standards Survey (Ministry of Social Development, 2000), with responses categorised as adequate (‘just enough’, ‘enough’, ‘more than enough’) or inadequate (‘not enough’). Participants were also asked how financially secure they felt with regard to the 10 years ahead. Satisfaction with social relationships, tobacco smoking and recreational drug use were determined as described previously (Derrett et al., 2011). Alcohol use was determined using the AUDIT-C (Alcohol Use Disorders Identification Test – Consumption) (Bradley et al., 2007).
We asked participants about their overall pre-injury general health (dichotomised as ‘excellent’/‘very good’/‘good’ and ‘fair’/‘poor’). Participants were also asked whether they had any of a list of 21 medically diagnosed conditions expected to last for 6 months or more, e.g. asthma, cancer, diabetes, bipolar disorder, schizophrenia, anxiety, depression (Ministry of Health, 2008). An affirmative response to ‘depression’ in this list or to one of two DSM-III screening questions for depressed mood or loss of interest or pleasure in daily activities consistently for at least a 2-week period in the 12 months before injury (American Psychiatric Association Committee of Nomenclature and Statistics, 1980) was deemed indicative of pre-existing depressive symptoms. Analyses categorised affirmative responses to pre-existing comorbidities as depressive-type symptoms, other psychological conditions (bipolar disorder, schizophrenia, anxiety) and other chronic conditions (remaining comorbidities).
Injury-related characteristics
The mechanism of injury was categorised as unintentional or related to an assault (self-harm events are excluded in this study). At the 3-month (baseline) interview, participants were asked whether, at the time of the event, they felt their injury was a threat to their life. They were also asked whether they anticipated that their injury could result in severe longer-term disability. Injury codes in the ACC database for each participant were mapped to International Classification of Diseases, 10th Revision (ICD-10) codes and converted to a New Injury Severity Score (NISS) (Osler et al., 1997) using an approach previously described (Derrett et al., 2012).
Post-injury health and healthcare experiences
At the 3-month post-injury interview, participants were asked whether they had recovered from their injury, and if not, if or when they expected to get better. Participants were also asked about the degree of pain or discomfort they were experiencing using the related question from the EQ-5D-3L (www.euroqol.org).
Questions about health service satisfaction were developed after reviewing other health service treatment measures such as the FACIT (www.facit.org) and undertaking a pilot study which elicited areas of importance for injured New Zealanders. Based on this work, the 3-month survey explored if participants had ‘trouble getting to or contacting health services’, ‘enough time to discuss any problems’ with health professionals, ‘enough information to make decisions about [their] healthcare’, if they were ‘encouraged to participate in decisions about [their] healthcare’, and if health professionals encouraged their families ‘to be involved in decisions about [their] treatment as much as [they] would like’.
Statistical analyses
To identify important factors associated with the risk of PTSD symptoms in each group of hospitalised and non-hospitalised participants, the relationships with hypothesised explanatory variables were initially explored using chi-square tests. Then, using a two-step process, relative risks (RR) expressing the associations between symptoms suggestive of PTSD and putative predictors were estimated using modified Poisson models with robust standard errors (Zou, 2004). First, a stepwise backward selection procedure was used to build separate models for hospitalised and non-hospitalised participants with explanatory variables retained if they met a p value threshold of ⩽0.10, in addition to covariates deemed essential (age, gender, ethnicity, NISS and time between the injury and the 12-month interview). The final models included all variables retained in either the hospitalised or non-hospitalised participant models to observe the strengths of predictors in these sub-groups. Since some of the participants identified with multiple ethnicities, a set of mutually exclusive ethnicity categories were created and used in the regression models. A modified marginal standardisation (Muller and MacLehose, 2014) was then applied to estimate ethnicity-related RRs from the multivariable models.
Results
Of the 2856 POIS participants, 2282 participated in the 12-month interview (81% and 80% of the hospitalised and non-hospitalised groups, respectively). This analysis was restricted to the 2220 (78%) individuals who completed the IES assessing the risk of symptoms suggestive of PTSD, of whom 550 (25%) were hospitalised for their initial injury. Hospitalised and non-hospitalised groups had similar demographic distributions (between-group differences in categorical levels were 5% or less) except for gender, with males comprising 66% of hospitalised and 56% of non-hospitalised participants. Not surprisingly, hospitalised participants were more likely than the non-hospitalised group to have sustained more severe injuries (NISS 4–6: 55% cf. 46%; NISS >6: 18% cf. 8%). At the 3-month interview, hospitalised participants were more likely to report having perceived their injuries as a threat to life (21% cf. 7%) or a threat to disability (50% cf. 34%), and less likely to report they had fully recovered (13% cf. 26%). Hospitalised participants were also less likely to report having had enough time to discuss problems (78% cf. 86%) but more likely to report family involvement in their care was encouraged (53% cf. 44%).
Overall, 17% of hospitalised and 12% of non-hospitalised injury survivors screened positive for PTSD (p = 0.002). Among hospitalised participants, bivariate analyses (Tables 1 and 2) identified that the risk of symptoms suggestive of PTSD was higher among people reporting higher levels of financial insecurity, smoking tobacco (25% vs 14% in non-smokers), a history of depressive-type symptoms (30% vs 14%) or other psychological conditions (38% vs 16%). Participants who were of Pacific ethnicity were more likely (33% vs 16%) and those of sole New Zealand European ethnicity less likely (12% vs 23%) to report symptoms suggestive of PTSD. Trauma-related factors associated with higher levels of this risk included assault compared with unintentional injury (32% vs 16%), perceived threat to life (35% vs 12%), threat of disability (23% vs 11%), higher levels of pain and poorer expectations of recovery. Healthcare interactions associated with a higher risk of symptoms suggestive of PTSD included insufficient information (28% vs 14%) and inadequate time to discuss problems with service providers (28% vs 14%), and families not being encouraged to be involved in the healthcare process.
Prevalence of symptoms suggestive of PTSD at 12 months by injury- and healthcare experiences.
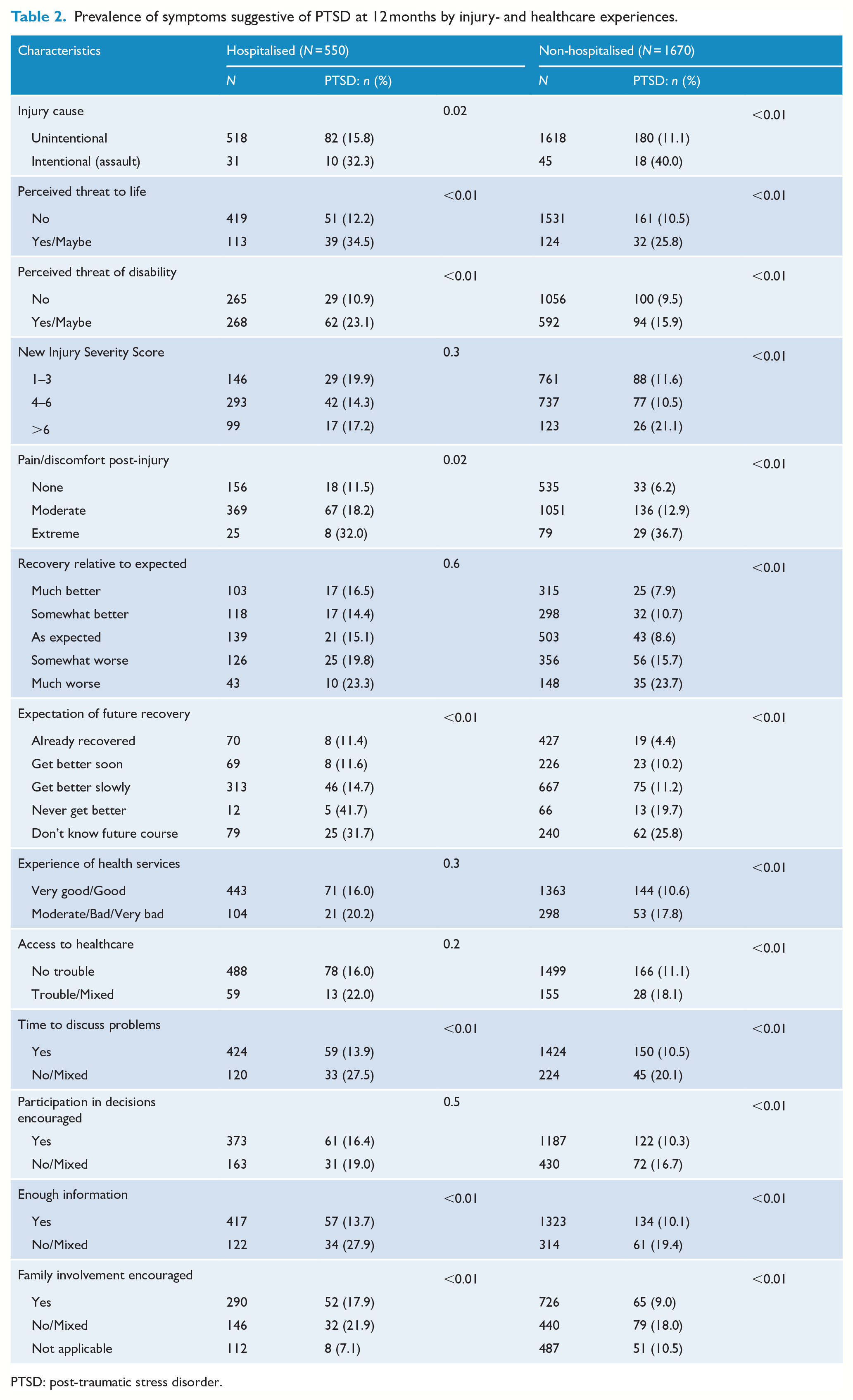
PTSD: post-traumatic stress disorder.
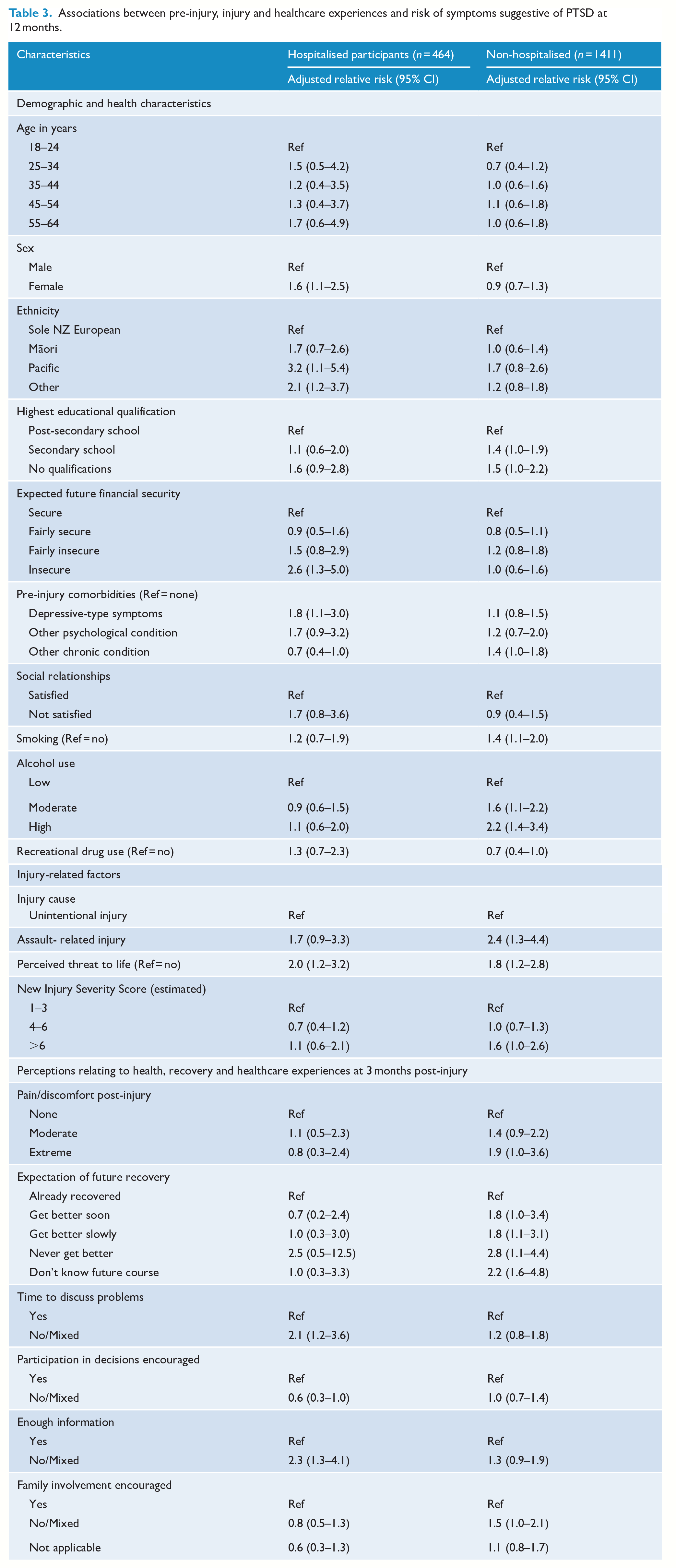
Multivariable models adjusting for covariates (Table 3) identified significantly higher risks of PTSD symptoms among hospitalised survivors who perceived their injury as a threat to life (adjusted RR: 2.0; 95% CI: 1.2–3.2); were female (aRR: 1.6; 1.1–2.5), of Pacific ethnicity (aRR: 3.2; 95% CI: 1.1–5.4) or in the ‘other ethnicity’ category compared with sole NZ Europeans (aRR: 2.1; 95% CI: 1.2–3.7), felt financially insecure (aRR: 2.6; 95% CI: 1.3–5.0) or had a history of depressive symptoms (aRR: 1.8; 95% CI: 1.1–3.0). Patients who felt they had received insufficient information or inadequate time to discuss problems had higher risks of PTSD symptoms but so did those who felt they were encouraged to participate in healthcare decisions.
Associations between pre-injury, injury and healthcare experiences and risk of symptoms suggestive of PTSD at 12 months.
Among non-hospitalised participants, bivariate analyses (Tables 1 and 2) identified a higher risk of symptoms suggestive of PTSD among people who reported chronic conditions (14% vs 10%) or depressive symptoms prior to the injury (17% vs 10%), lower levels of formal education, concerns about their financial security in the future, smoke tobacco or have drinking problems. Even though this group was not hospitalised, a wide range of injury-related risks were associated with PTSD symptoms including the injury being due to assault rather than an unintentional mechanism (40% vs 11%), perceived as a threat to life (26% vs 11%) or disability (16% vs 11%), pain and discomfort at 3 months post-injury, low expectations of recovery and poor healthcare experiences (e.g. limited access, information, time to discuss problems and engagement in decision-making).
After adjusting for covariates (Table 3), the risk of symptoms suggestive of PTSD among non-hospitalised participants was associated with assault compared with unintentional injury (aRR: 2.4; 95% CI: 1.3–4.4), perceived threat to life (aRR: 1.8; 95% CI: 1.2–2.8), tobacco use, hazardous drinking, pain or discomfort and low expectations of recovery. Except for a weakly positive association for the highest injury severity category (NISS >6) in the non-hospitalised group (aRR: 1.6; 95% CI: 1.0–2.6), we found no statistically significant associations between this injury severity measure and the risk of symptoms suggestive of PTSD at 12 months.
Discussion
This study of 2220 injured adults found that one in six who were hospitalised for their injury and one in eight who were not hospitalised experienced symptoms suggestive of PTSD when followed up 12 months following their injury. Peri-traumatic perception of threat to life was an important predictor of PTSD in both groups. Other predictors of PTSD identified in previous research focusing on hospitalised patients such as poor expectations of recovery, tobacco use, heavy drinking and assault (Brewin et al., 2000; Davydow et al., 2009; DiGangi et al., 2013; Gradus, 2017; Ozer et al., 2003; Russo et al., 2013; Santiago et al., 2013) were significantly associated with symptoms suggestive of PTSD among non-hospitalised participants in this study. Collectively, these findings indicate that regardless of whether the initial injury required hospitalisation, PTSD symptoms are relatively common 12 months later, and factors recognisable early in the course may help identify and target interventions that can reduce this risk.
Our findings must be interpreted with caution for several reasons. This study examined the prevalence of symptoms suggestive of PTSD only at the 12-month interview, precluding the ability to consider symptom trajectories earlier or later in the course. Although the IES is widely used in research studies, it is not a diagnostic tool. Furthermore, the original form of the IES used in this study did not capture information on hyper-arousal symptoms incorporated in the IES-Revised version which is considered more sensitive in identifying general traumatic stress in community samples with lower symptom levels (Creamer et al., 2003). Nevertheless, the prevalence estimate of symptoms suggestive of PTSD among hospitalised participants in our study was consistent with several previous studies (Haagsma et al., 2013; Santiago et al., 2013; Schultebraucks et al., 2020; Skogstad et al., 2014).
This study focused on claimants in the national ACC insurance scheme which is theoretically accessible to anyone experiencing an injury in New Zealand, regardless of their income, residency status or fault attribution. Previous studies have documented barriers to accessing ACC among Māori (Jansen et al., 2008) and Asian communities (Sobrun-Maharaj et al., 2010). Such inequities indicate the potential to have underestimated the prevalence of PTSD symptoms in some demographic groups.
While the exposures investigated are not exhaustive, we focused on aspects identifiable early in the post-injury phase using brief measures, and the findings among hospitalised participants are consistent with previous reviews (Brewin et al., 2000; Ozer et al., 2003). However, our study was not designed to assess the presence of acute stress reactions or symptoms suggestive of PTSD soon after the injury which can discriminate, with high levels of precision, individual PTSD risks further along the recovery course in hospitalised trauma survivors (Schultebraucks et al., 2020; Shalev et al., 2019).
The strengths of the study include the insights gained regarding the prevalence and predictors of symptoms suggestive of PTSD among hospitalised and non-hospitalised injury survivors in a country where tort-based compensation is rare, thereby reducing the confounding influences of civil litigation and settlement processes (Alarcon et al., 2012; Elbers et al., 2013; Mezey and Robbins, 2001; O’Donnell et al., 2010). With 80% of eligible participants in this relatively large prospective cohort interviewed at 12 months post-injury, the study achieved a high follow-up rate compared with previous studies involving non-hospitalised patients (Haagsma et al., 2012, 2013). The participants lost to follow-up in our study were more likely to have chronic health problems, experience disability and psychological distress, be younger, male, and of Māori ethnicity (Langley et al., 2013), features likely to under-estimate the prevalence of PTSD. There was no significant difference in loss to follow-up between hospitalised and non-hospitalised participants.
Despite the theoretical advantages of a no-fault government-funded injury insurance scheme, our findings reveal important socio-economic disparities in the risk of symptoms suggestive of PTSD. Individuals in the hospitalised group who anticipated higher degrees of financial insecurity in the 10 years ahead (when interviewed at 3 months post-injury) were at significantly higher risk of PTSD symptoms at 12 months. This may reflect factors not directly measured in this study such as variable access to and quality of compensatory support, and inadequate labour market safety nets for injured people.
Following adjustment for other factors including socio-economic status, we found that hospitalised participants of Pacific ethnicity and those in the ‘other ethnicities’ category were at higher risk of PTSD symptoms. Ethnic differences were not apparent among injured participants who were not hospitalised, a finding consistent with a large community-based survey in New Zealand investigating mental health associated with traumatic events (Kazantzis et al., 2010).
Our findings also draw attention to the relatively neglected domain of healthcare interactions in this field (Gradus, 2017). People who reported having inadequate information or insufficient time to discuss problems with health professionals in the 3-month follow-up survey had elevated risks of PTSD symptoms at 12 months. While reported healthcare experiences may have been associated with participants’ affective states at 3 months post-injury, the associations with PTSD symptoms 9 months later were stronger in the hospitalised group. This may reflect difficulties patients experience when navigating hospital systems or care transitions early in the recovery phase, aspects that require further attention. Although all participants in this study are ACC entitlement claimants, previous studies have identified inequities in the quality of, and satisfaction with, ACC and rehabilitation services (Jansen et al., 2008; Sobrun-Maharaj et al., 2010). While this study was not designed to investigate the nature and delivery of services across the continuum of trauma care, the findings speak to the importance of investigating and addressing potential mechanisms, including inadequate awareness of patient experiences and cross-cultural concepts of mental well-being, institutional racism and other factors that influence provider–patient communication. Unless addressed, the cumulative impact of these factors is also likely to impede the uptake and effectiveness of interventions addressing PTSD.
An overarching implication of the study findings is the need for greater attention to non-hospitalised injury survivors when considering longer-term psychological outcomes. Current ACC guidelines for assessing mental injury ‘generally expects a physical injury to be serious or accompanied by threat of serious injury’ (ACC, 2013). Our findings indicate that even if the physical injury was not considered serious enough to warrant hospitalisation, individuals who perceived their injury event as a threat to life were at significantly higher risk of PTSD symptoms a year later compared with their peers. This finding, which contrasts with the relatively weak association with the anatomical injury severity score used in this study, is consistent with previous research which has demonstrated that ‘subjective, and not objective, injury severity predicted post-traumatic stress symptoms at six weeks and three months following trauma’ (Gabert-Quillen et al., 2011).
At 3 months post-injury, 17% of hospitalised and 19% of non-hospitalised participants reported being uncertain about their future health or feeling they would never get better. A further 58% and 41% in each of these groups, respectively, felt they would get better only slowly. These perceptions strongly predicted PTSD symptoms in non-hospitalised participants suggesting unresolved issues requiring more attention. Other factors associated with the risk of symptoms suggestive of PTSD in non-hospitalised survivors (e.g. assault-related injury, smoking and hazardous drinking) are consistent with vulnerabilities described in hospital-based studies.
There is emerging evidence of the potential utility of predictive algorithms drawing on routinely collected data, brief self-reported clinical assessments and machine-learning approaches, to identify PTSD risk in hospitalised trauma survivors (Schultebraucks et al., 2020; Shalev et al., 2019). In addition to important caveats in this evolving research field noted by others (Vermetten and McFarlane, 2020), more research attention is required to develop approaches relevant to non-hospitalised survivors. The latter account for most ACC claimants in New Zealand and trauma survivors in general, although their stress response trajectories are inadequately captured in standard data collection systems, globally.
Increasing awareness of the impacts of co-occurring predictors and associations with PTSD (e.g. depression, substance use, poor functional recovery and quality of life and difficulty returning to work) has led to a range of promising interventions. Most are designed to be implemented in trauma centres and military health systems and include integrated exposure-based therapy (Mills et al., 2012) and stepped collaborative care interventions (Zatzick et al., 2018). Electronic medical records and decision-support systems, patient-centred portals, interactive record taking and mobile health technology are providing more accessible and scalable opportunities to screen, triage and intervene to reduce the risk of PTSD and other comorbidities (deRoon-Cassini et al., 2019; Hosking et al., 2011; Russo et al., 2013; Zatzick et al., 2018). A systematic review and meta-analysis published in 2018 identified exposure- and cognitive behavioural therapy–based interventions to be the most effective approaches to addressing PTSD and depression post-injury, especially when these are implemented in the first 3 months following injury using a risk-based stepped care strategy (Giummarra et al., 2018).
In summary, our study highlights the need to implement evidence-based screening for early predictors of PTSD in general injury populations in New Zealand, particularly when the event was perceived as a threat to life, and even if the injury did not require hospitalisation. This can help identify those who could benefit from timely, equity-focused interventions that can improve the quality of life and psychological well-being of this high-risk population. These considerations are important in contexts where overtly more pressing clinical demands result in the neglect of harbingers of longer-term psychosocial morbidity.
Footnotes
Acknowledgements
We are most grateful to the study participants for sharing their information with us, and to Dr Amy Richardson for her comments on an earlier draft of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Prospective Outcomes of Injury Study was supported by the Health Research Council of New Zealand (grant number 10/052) and co-funded by the Accident Compensation Corporation, New Zealand. The views and conclusions of this paper are those of the authors and may not reflect those of the funders.