
Abstract
Objective:
Demoralisation is a state of poor coping characterised by low morale, hopelessness, subjective incompetence, and loss of meaning and purpose in life. While studied extensively in oncology and palliative care, there has been recent exploration in broader medical and mental health settings. The aim was to investigate the prevalence of demoralisation and associated sociodemographic and psychological factors across these clinical settings.
Method:
Six electronic databases were used to locate articles from January 2014 to March 2020. A pre-publication update of non-oncology populations was completed in September 2021. The review has been reported following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Pooled prevalence of demoralisation was determined through % prevalence and mean demoralisation score; this was synthesised through meta-analysis of single means to determine pooled mean prevalence of Demoralisation Scale scores using the ‘R’ statistical software.
Results:
Demoralisation has been examined in 52 studies (n = 11,670) and found to be prevalent in 24–35% of oncology and non-oncology, including mental health, populations. The mean score on the Demoralisation Scale was 24.3 (95% confidence interval, CI = [21.3, 27.3]). There was evidence of divergent validity in addition to significant comorbidity between depression, demoralisation and suicidal ideation. Burdensome physical symptoms, and psychological and demographic factors are strongly correlated with demoralisation.
Conclusion:
There remains a need to recognise demoralisation in various clinical and cultural settings and to strongly consider its inclusion as a ‘specifier’ within formal nosological systems for adjustment and depressive disorders. This is important to initiate targeted interventions and prevent significant morbidity.
Introduction
Demoralisation is a state of poor coping characterised by low morale, hopelessness and loss of meaning and purpose in life (Kissane et al., 2001). The origins of the construct arise from early observations of suffering and the contribution to coping of finding meaning, as expressed by prominent psychiatrist Viktor Frankl (1962). The concept was furthered by Engel’s description of the ‘giving up–given up’ complex, with hopeless cognitions worsening physical health (Engel, 1967). Around the same time, Jerome Frank conceptualised demoralisation as a sense of internalised failure, which then contributes to perceived meaningless in life (Frank, 1974). Subjective incompetence deepens any sense of helplessness and hopelessness (de Figueiredo and Frank, 1982). Demoralisation develops across a spectrum of severity from initial feelings of disheartenment, to a deeper sense of hopelessness and failure, to a severe sense of loss of meaning and purpose (Kissane et al., 2004).
This early literature led to the empirical assessment of demoralisation, with consideration of diagnostic parameters as well as implications for targeted psychotherapeutic interventions, including meaning-based therapy (Robinson et al., 2016a). Validated measures were developed, including the Diagnostic Criteria for Psychosomatic Research/Demoralisation (DCPR/D) (Fava et al., 1995) and the Demoralisation Scale (DS) (Kissane et al., 2004). These two measures are the main primary validated measures of demoralisation utilised in previous literature (Robinson et al., 2016a). The DCPR, first developed in 1995, is a set of diagnostic criteria based on an interview that aims to elicit various psychosomatic syndromes in the medically ill across the clinical domains of stress, personality, illness behaviour and psychological sequelae (Fava et al., 2017). It has demonstrated utility in multiple studies and reviews (Porcelli and Guidi, 2015; Sirri and Fava, 2013) and has undergone further revision in 2017 with fresh emphasis on the expression of hopelessness and helplessness in demoralisation syndrome (Fava et al., 2017). The DS is a 24-item self-report measure rated on a 3-point Likert-type scale, involving five subscales that assess various dimensions of demoralisation including loss of life meaning, disheartenment, helplessness and sense of failure (Kissane et al., 2004). The DS underwent subsequent refinement and revalidation to the DS-II, with re-evaluation as a 16-item scale with strong internal, convergent and divergent validity (Robinson et al., 2016c). In comparing the DS and DS-II, the longer DS has a critical threshold score of >30, compared to >8 in the briefer DS-II (Kissane et al., 2004; Robinson et al., 2016c). In comparing the DS with the DCPR/D, the DCPR/D utilises a longer time frame to evaluate symptoms (1 month compared to 2 weeks in the DS), as well as reduced focus on phenomena such as loss of meaning or dysphoria that are examined in the DS.
The neurobiology of demoralisation involves dopamine circuits, wherein motivational salience, desire and hope are activated in the shell region of the nucleus accumbens, with the values placed on these goals considered in the orbital prefrontal cortex, memory consolidated in the hippocampus, and then motor plans are encoded in the core region of the nucleus accumbens and dorsal striatum (Salgado and Kaplitt, 2015). These frontal-subcortical circuits play a key role in the hope system, with stress and trauma disrupting the dopamine system in the nucleus accumbens (Leach, 2018).
Conceptually and from a phenomenological perspective, demoralisation has been most studied in oncology and palliative care settings, but also with other medical and mental illnesses, among refugees, substance users, the postnatal period and in adjustment to stressors (Bobevski et al., 2014, 2015; Briggs, 2011; De Weert et al., 2017). This has contributed to a broader understanding of the prevalence of demoralisation and the implications for treatment. One key focus has been the differentiation of demoralisation from depression, anxiety, adjustment disorder and grief (de Figueiredo, 2013; Wellen, 2010).
In 2015, three systematic reviews of demoralisation were undertaken in cancer (Tang et al., 2015), palliative care patients (Robinson et al., 2015) and in diffuse clinical settings (Tecuta et al., 2015). Using the DS, a prevalence rate of 13–18% was found among palliative care patients (Robinson et al., 2015). Using the DCPR/D, one third of the medically ill and one half of the mentally ill become demoralised (Tecuta et al., 2015). Additionally, demoralisation and depression were seen to be independent and distinguishable (Tang et al., 2015; Tecuta et al., 2015). Tecuta et al. (2015) identified associations between demoralisation and lower social support, increased stress, the presence of pain and somatisation syndromes, illness behaviour and adverse health outcomes. Robinson et al. (2015) also identified a positive relationship between demoralisation and physical symptoms, depression, anxiety, desire for hastened death and negative quality of life. Tang et al. (2015) emphasised the strong presence of depression in patients with high demoralisation and reported on the increased risk of suicide.
Our objective here was to update these prior reviews by examining recent studies of demoralisation across the past 7 years (2014–2020) in various clinical populations and settings. We aimed to synthesise evidence of the associations between demoralisation and various sociodemographic and psychological factors. This systematic review aimed to answer the following key research questions:
What is the prevalence of demoralisation in studies from 2014 to 2020 inclusively?
What is the relationship between demoralisation and other related clinical syndromes?
What are the findings of recent psychometric analyses of demoralisation syndrome?
What sociodemographic, physical health and psychological factors influence the prevalence of demoralisation in these patient groups?
What impact does demoralisation have on quality of life and risk of suicide?
How might demoralisation be incorporated into the Diagnostic and Statistical Manual of Mental Disorders?
Methods
Six electronic databases were used to locate articles: Medline, Embase, PsychINFO, Cumulative Index to Nursing & Allied Health Literature (CINAHL), The Cochrane Library and PubMed. References of eligible papers were also manually searched for suitable articles for inclusion. The search term (Demorali*) was used across all databases in screening titles, keywords and abstracts. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) methodology was used to guide this review (Liberati et al., 2009; Moher et al., 2009). Two reviewers (L.L.G. and S.G.) independently assessed studies against the inclusion/exclusion criteria, and full texts for eligible articles were reviewed.
Selection criteria
We included peer-reviewed quantitative articles in which demoralisation prevalence was reported and validated measures of demoralisation were used, including the DCPR and DS. Searches were limited to articles published in English between 1 January 2014 and 9 March 2020 (when searches were completed). We excluded conference abstracts, dissertations/theses, studies involving non-clinical or non-medical populations and studies where validated measures were not used. Studies where demoralisation prevalence was not reported or where demoralisation was described primarily as a secondary outcome to validate a novel scale, measure or intervention were also excluded. Additionally, data that were not complete or in process at the time of review were also excluded.
Data extraction
The following data were extracted from the articles by the first author (L.L.G.): study design, sample characteristics including illness and sample size, objective of study, measures used, prevalence results and other key findings. A separate reviewer (S.G.) reviewed and confirmed the extracted data from the studies included in this review.
Data synthesis
The principal summary measure was pooled prevalence of demoralisation by way of overall mean demoralisation score and % prevalence. Results were synthesised through meta-analysis of single means to determine pooled mean prevalence of DS scores. The ‘R’ statistical software (R Development Core Team, 2010) and its ‘Metamean’ package were used to calculate pooled mean prevalence, 95% CI, investigate heterogeneity (I2 and tau squared scores) and generate forest plots of overall pooled mean prevalence using a Random effects model. Sidik-Jonkman estimator was utilised to determine between study variance. Subgroup analysis was performed in oncology and non-oncology studies, and further subgroup analysis was performed in advanced cancer populations.
In studies where demoralisation percentage prevalence was reported, including studies utilising the DCPR/D measure, % prevalence was combined to determine mean % prevalence and range.
Quality appraisal and risk of bias
The quality of included articles was assessed using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields (Kmet et al., 2004). This measure also considers risk of bias in individual studies and contributes to the overall quality score for each article.
Results
Through database searching, we initially identified 1513 articles. After screening for eligibility, we retained 40 articles that measured prevalence of demoralisation, please see Figure 1 for PRISMA study selection flow.
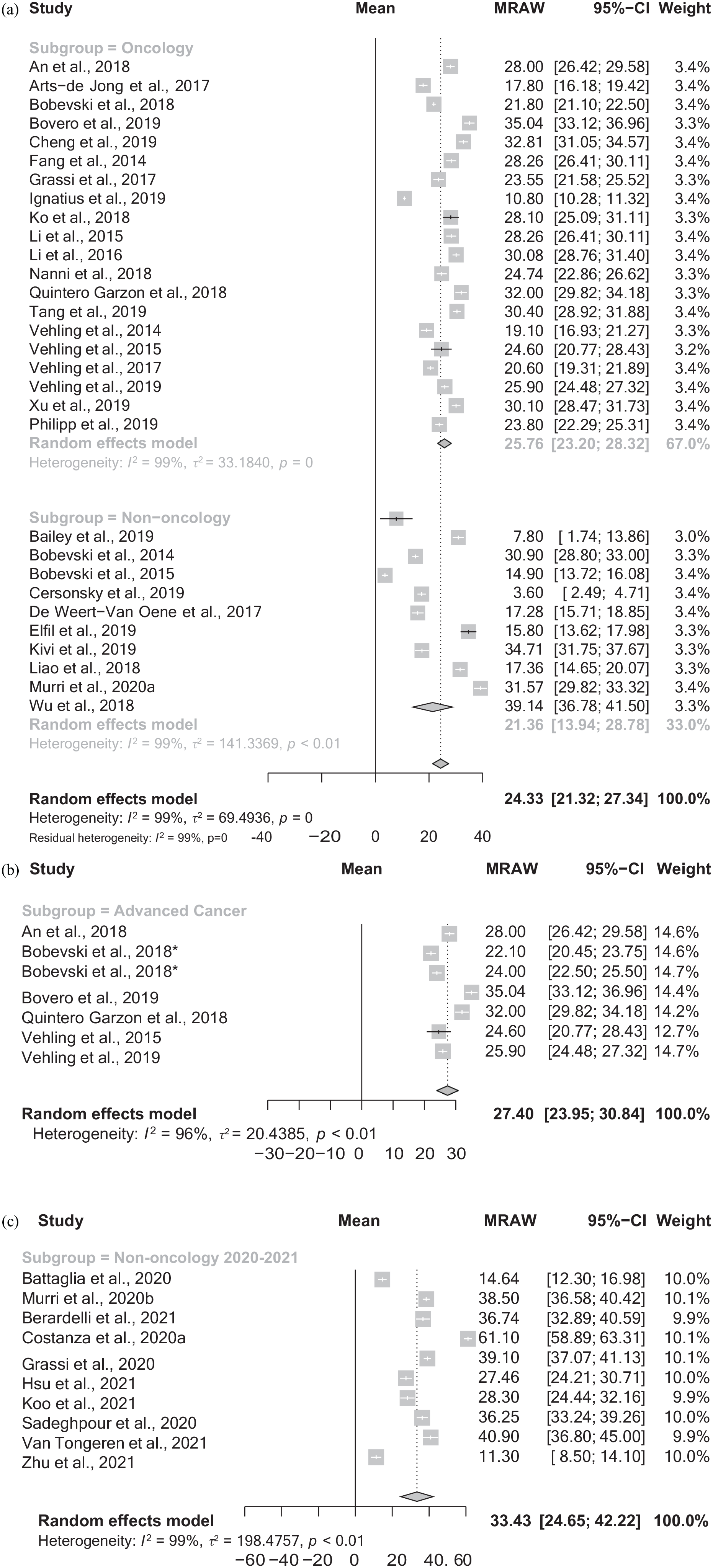
Forest plots. (a). Pooled mean demoralisation score and CI for all studies 2014–2020 reporting mean DS score, divided into oncology and non-oncology subgroups. (b) Pooled mean demoralisation score and CI for studies examining advanced cancer populations 2014–2020. (c) Pooled mean demoralisation score and CI for studies examining non-oncology populations 2020–2021.
The systematic review of studies identified following searches completed in March 2020 represents the experiences of 9920 participants, including 7093 oncology and 2827 non-oncology participants. The range of sample sizes across all included studies was 55–1529 (mean = 248). There were 22 studies examining oncology populations, 17 non-oncology medical populations and 1 with mixed oncology and chronic illness participants. Of the non-oncology studies, four studies investigated demoralisation in cardiovascular disease/cardiac surgery patients, two each for chronic illness, mothers in the postnatal period, psychiatric conditions (one for eating disorders and one for patients with substance use disorders and psychiatric comorbidity), Parkinson’s populations, and one each examined patients with psoriasis, fibromyalgia/rheumatoid arthritis, multiple sclerosis, tremor, primary care populations and those on general medical wards.
In total, 29 studies utilised the DS, 6 studies used the DCPR and 5 studies used both DS/DCPR study measures. Of the included studies, 29 reported results involving mean ± SD, the remaining reported demoralisation as a % prevalence.
There were 34 cross-sectional studies, 5 longitudinal studies and 1 randomised controlled trial included in this review. Two studies (Li et al., 2016, 2017) included in this review reported different relevant analysis findings based on the same study population.
The quality scores of articles ranged between a score of 0.75 and 1 (with 1 being the highest quality score) according to the Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields (Kmet et al., 2004). The main source of bias was recruitment bias through convenience sampling; smaller sample sizes were identified in studies with poorer quality scores.
Please see Table 1 for a summary of characteristics of demoralisation studies meeting eligibility criteria for inclusion in this systematic review. Studies are tabulated according to the study measure used and oncology/non-oncology populations.
Characteristics of demoralisation studies meeting eligibility criteria for systematic review (2014–2020) and using the Demoralisation Scale (DS), Demoralisation Scale-II (DS-II) or Diagnostic Criteria for Psychosomatic Research (DCPR) and an addended update of non-oncological studies (2020–2021).

DS: Demoralisation Scale; DS-II: Demoralisation Scale-II; DCPR: Diagnostic Criteria for Psychosomatic Research; DADDS: Death and Dying Distress Scale; MSAS: Memorial Symptom Assessment Scale; KPS: Karnofsky Performance Status; ECR-M16: modified Experiences in Close Relationships scale; QUAL-EC: Life Completion subscale of the Quality of Life at the End-of-Life – Cancer questionnaire; QOL: Quality of Life Questionnaire; EORTC QLQ-C30: Quality of Life Questionnaire-Core 30; STAI: Spielberger State-Trait Anxiety Inventory; CWS: Cancer Worry Scale; HADS: Hospital Anxiety and Depression Scale; ESAS-r: Edmonton Symptom Assessment System–revised; PHQ-9: Patient Health Questionnaire-9; GAD-7: Generalised Anxiety Disorder-7 questionnaire; DT: NCCN Distress Thermometer; SF-8: Short Form Health Survey; IT: Italian Version; PDI- IT: Patient Dignity Inventory–Italian Version; FACIT-Sp-12: Functional Assessment of Chronic Illness Therapy – Spiritual Well-Being; VAS: Visual Analog Scale for Pain; MQOL: McGill Quality of Life Questionnaire; BHS: Beck Hopelessness Scale; BSI: Brief Symptom Inventory-18; PPS: Palliative Performance Scale; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.); BSS: Beck Scale for Suicidal Ideation; PTGI: Posttraumatic Growth Inventory; QUAL-EC-P: German Quality of Life at the End of Life-Cancer-Psychosocial questionnaire; SF-12V2: 12-item Short Form Health Survey; CLOT-R: Revised Life Orientation Test; ISSS-8: Illness-Specific Social Support Scale Short Version-8; RR: relative risk; CIDI-O: Composite International Diagnostic Interview–Oncology; CI: confidence interval; ECR-16: Experiences in Close Relationships Scale; MSAS-SF: Memorial Symptom Assessment Scale–Short Form; MINI: Mini International Neuropsychiatric Interview; LAP-R: Life Attitude Profile–Revised; CCI: Charlson Comorbidity Index; BaM-13: Being a Mother Scale; DASS-21: Depression Anxiety Stress Scale; EPDS: Edinburgh Postnatal Depression Scale; VPSQ: Vulnerable Personality Style Questionnaire; BPD: Barr Parental Diary; IBM: Intimate Bonds Measure; SIS: Subjective Incompetence Scale; BRS: Brief Resilience Scale; TDQ: Tremor Disability Questionnaire; CIRS: Cumulative Illness Rating Scale; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; GDS: Geriatric Depression Scale; CDR: Clinical Dementia Rating; IADL: Lawton Instrumental Activities of Daily Living Scale; ICU: Intensive Care Unit; MOS SF-12: Medical Outcome Study Short Form; HPLP-II: Health Promoting Lifestyle Profile-II; DCPR-D: Diagnostic Criteria for Psychosomatic Research–Demoralisation Subscale; Mini-MAC/HH: Mini-Mental Adjustment to Cancer Hopelessness–Helplessness subscale; PD: Parkinson disease; SBQ-R: Suicidal Behaviour Questionnaire–revised; BLDS: Brief Lifetime Depression Scale; C-SSRS: Columbia-Suicide Severity Rating Scale; ISI: Insomnia Severity Index; SBQ-17: Suicidal Behaviour Questionnaire-17; nM-EDL: Non-Motor Aspects of Experiences of Daily Living; MDS-UPDRS: Movement Disorders Society–Unified Parkinson’s Disease Rating Scale; QUIP-RS: Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease–Rating Scale; UPDRS-m: Unified Parkinson’s Disease Rating Scale-part III; EQ-5D: EuroQol-5D; PASI: Psoriasis Area and Severity Index; TRIUMPH: Trial Using Motivational Interview, Positive Affect, and Self-affirmation in African Americans with Hypertension; SCID-I: Structured Clinical Interview for DSM-IV; SQ: Kellner’s Symptom Questionnaire; PWB: Psychological Well-Being; TCI: Temperament and Character Inventory; SCID-5: Structured Clinical Interview for DSM-5; PSI: Psychosocial Index; IAS: Illness Attitude Scales; DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.); EAT-40: Eating Attitudes Test-40; BDI-II: Beck Depression Inventory II; SF-36: 36 Item Short Form Health Survey; KTR: kidney transplant recipient; CPC: Canadian Problem Checklist; IS: Insight Scale; ED: emergency department; SI: suicidal ideation; SSI: Scale for Suicide Ideation; CRC: colorectal cancer; PWB-I: Psychological Well-Being Interview; CH: cluster headache; ICHD-3: International Classification of Headache Disorders, 3rd Edition; CH-QOL: Cluster Headache Quality of Life Questionnaire; DLQI: Dermatology Life Quality Index; CID: Clinical Interview for Depression; PDQ-8: Parkinson’s Disease Questionnaire–Short Form; ICD: International Classification of Diseases; HrQoL: health-related quality of life; BRCA: Breast Cancer Gene; DS-MV: Demoralisation Scale- Mandarin Version; HCP: Health Care Provider; ET: Essential Tremor; CHF: Chronic Heart Failure; FM: Fibromyalgia; RA: Rheumatoid Arthritis; CSSRS: Columbia Suicide Severity Rating Scale.
Quality score rating according to the Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields (Kmet et al., 2004).
References
Prevalence of demoralisation syndrome based on mean scores and % prevalence of studies in initial search until March 2020
Pooled average of the mean demoralisation score was 24.3 (95% CI = [21.3, 27.3]) (I2 = 99%) in all studies reporting mean DS score (8802 participants from 30 studies). Subgroup analysis revealed pooled mean score of 25.8 (95% CI = [23.2, 28.3]) in oncology studies (6863 participants from 20 studies) and pooled mean score of 21.4 (95% CI = [13.9, 28.8]) in non-oncology studies (1939 participants from 10 studies) (see Forest plot 1a). Further analysis in advanced cancer populations revealed overall mean of 27.4 (95% CI = [24.0, 30.8]; I2 = 96%, 1751 participants from 6 studies) (see Forest plot 1b).
In all studies reporting % prevalence for clinically significant scores on the DS or DS-II (scores of at least > 8 or ‘severe demoralisation’ based on Robinson et al., 2016c, and Mullane et al., 2009, criteria for clinically significant demoralisation in articles where score cut offs are not reported), pooled prevalence was 34.7% (range, 6–86%; 6350 participants from 27 studies).
In studies examining oncology populations, mean pooled prevalence of participants with scores > 8 or ‘severe demoralisation’ on the DS and DS-II was 35.8% (range, 16–57.6%); 5216 participants from 20 studies). Different studies reported different cut offs for clinically relevant demoralisation according to the DS; those oncology studies that reported percent prevalence of DS scores > 30 (3317 participants from 14 studies) had a mean pooled prevalence of 39.0% (range, 16–57.6).
In studies examining non-oncology populations, for studies reporting clinically relevant demoralisation scores (DS-II ⩾ 8) or ‘severe demoralisation’ (7 studies involving 1134 participants), the pooled mean prevalence % was 31.8% (range, 6–86).
For studies using the DCPR measure, prevalence of demoralisation was 24.3% (range, 15–50%; 1930 participants from 11 studies). Furthermore, among oncology studies, prevalence was 24.4% (389 participants from 2 studies), while in non-oncology studies it was 24.3% (1541 participants from 9 studies).
Pre-publication update on literature of non-oncological studies examining demoralisation (2020–2021)
During the time this manuscript was undergoing review for publication, there were an increasing number of relevant studies of non-oncological populations emerging in the literature. Therefore, an additional search for non-oncological studies was completed on 26 September 2021 using the same methodology and selection criteria. A summary of the results of these studies and their characteristics are summarised in a final section of Table 1.
Of these 12 cross-sectional studies examining a total of 2197 participants, 8 studies examined physical medical illness populations (one each of Parkinson’s disease, Kidney Transplant recipients, Cardiac transplant recipients, General hospital population, patients with positive faecal occult blood test, patients with cluster headache, chronic psoriasis and haemodialysis patients) and 4 studies investigated mental illness populations (one each of acute psychiatric inpatients, patients with suicidal behaviour, non-psychotic psychiatric illness and substance use disorder populations). One study reported new findings from a previously included study in this review Murri et al. (2020a, 2020b).
In all the studies reporting mean DS scores (1765 participants from 10 studies), the pooled average score was 33.4. The mean % prevalence of demoralisation across all studies utilising the DCPR/D (1138 participants from 6 studies) is 24.2%. Pooled mean DS score and forest plot were generated for these additional studies (see Figure 1(c)). Key additional findings have been included in the results and discussion.
Psychometric analysis
Of the studies included in this review examining psychometric properties of the DS and DS-II, high mean scores were identified in the ‘Emotional distress and inability to cope’ subscale (Bailey et al., 2020; Bovero et al., 2019) which examines emotions associated with being in control, irritability, distress, isolation, feeling trapped and regret (Robinson et al., 2016b). High mean scores were also observed in the ‘Disheartenment’ (Grassi et al., 2017; Murri et al., 2020a) and ‘Sense of Failure’ subscales (Liao et al., 2018) of studies assessing the DS. The ‘Disheartenment’ subscale assesses participant accordance with feelings of isolation, discouragement, hopelessness and poor coping. The ‘Sense of Failure’ subscale focuses on identifying self-value, pride in self accomplishment and feeling worthwhile (Kissane et al., 2004). Overall, the DS was found to demonstrate good psychometric properties in settings outside of cancer (Battaglia et al., 2020; Murri et al., 2020a) and when shortened or transformed into culturally or linguistically adapted scales (Cheng et al., 2019; Murri et al., 2020a).
There was also evidence of concordant validity between the DS and DCPR measurements scales; patients who were DCPR/D cases showed significantly higher scores on all DS scales in one study (Grassi et al., 2020).
Relationship between demoralisation and DSM/ICD syndromes
Multiple studies reported a significant portion of patients who were demoralised yet did not show any symptoms of depression (Bobevski et al., 2015; Cersonsky et al., 2019; Grassi et al., 2017; Murri et al., 2020a), with a higher proportion of ‘low depression and high demoralisation’ patients compared to ‘high depression and low demoralisation’ presentations (Ignatius and De La Garza, 2019; Tang et al., 2020). A population was also identified that was found to be demoralised without any evidence of a Diagnostic and Statistical Manual of Mental Disorders (DSM) mood or adjustment disorder as defined by the Composite International Diagnostic Interview–Oncology (CIDI-O) in accordance with DSM-IV criteria (Vehling et al., 2017). Furthermore, a study examining kidney transplant recipients showed a significant proportion of recipients without an International Classification of Diseases (ICD) diagnosis were found to be demoralised, and those with an ICD diagnosis were found to be significantly more demoralised compared to those with no diagnosis (Battaglia et al., 2020).
The distinction between depression and demoralisation has been explored and debated in the literature. A recent network analysis exploring the strength of associations between symptoms reported symptoms of depression (anhedonia, somatic and cognitive symptoms) that fall into a distinct community quite separate from the symptoms of demoralisation. Symptoms of hopelessness and suicidal thoughts were strongly located among the communities of demoralised symptoms and remote from anhedonic depression on the network map (Murri et al., 2020b). In the study by Bobevski et al. (2015), a low proportion of respondents with high demoralisation scores were found to have comorbid moderate to severe depression or anxiety.
Demoralisation was also shown to have significant comorbidity with depression (Arts-de Jong et al., 2018; Bailey et al., 2020; Battaglia et al., 2020; Grassi et al., 2020; Koo et al., 2018; Tang et al., 2020; Vehling et al., 2015; Vehling and Mehnert, 2014; Xu et al., 2019), with a high probability of being highly depressed among highly demoralised patients, and a significant proportion of patients meeting criteria for comorbid Demoralisation and Depression (Belar et al., 2019; Bovero et al., 2019; Elfil et al., 2020; Ignatius and De La Garza, 2019; Juliao et al., 2016; Murri et al., 2020a; Offidani et al., 2017; Tecuta et al., 2019). Increasing scores on the Hospital Anxiety and Depression Scale (HADS)–Depression scale were found to correlate with increasing levels of demoralisation (p < 0.001) (Nanni et al., 2018); higher severity of demoralisation with increasing severity of psychiatric disorders was identified in the study by Grassi et al. (2020). There was also an elevated probability of being highly demoralised among highly depressed patients (Battaglia et al., 2020; Belar et al., 2019; Grassi et al., 2020; Ko et al., 2018; Vehling et al., 2017; Xu et al., 2019) and, in particular, this was noted in the post-operative setting following cardiac surgery (Liao et al., 2018).
In a study of 377 patients with non-psychotic psychiatric disorders, the highest prevalence of demoralisation and mean scores on the DS were in patients with major depressive and personality disorders when compared to adjustment or anxiety disorders (Grassi et al., 2020). A comorbidity between demoralisation and anxiety has also been demonstrated (Bobevski et al., 2018; Vehling et al., 2017; Xu et al., 2019). In examining the relationship between psychiatric disorders and demoralisation, patients with substance dependence experienced higher levels of demoralisation with comorbid anxiety disorders. Conversely, demoralisation levels were observed to be relatively lower in patients with psychotic disorders (De Weert et al., 2017).
Sociodemographic factors
Various medical, psychological and sociodemographic associations are evident in these studies of demoralisation. These have been summarised in Tables 2–4 with associated number (N) of studies and participants, in addition to likelihood of association based on participant size, number of studies sharing common findings and associations that require further exploration.
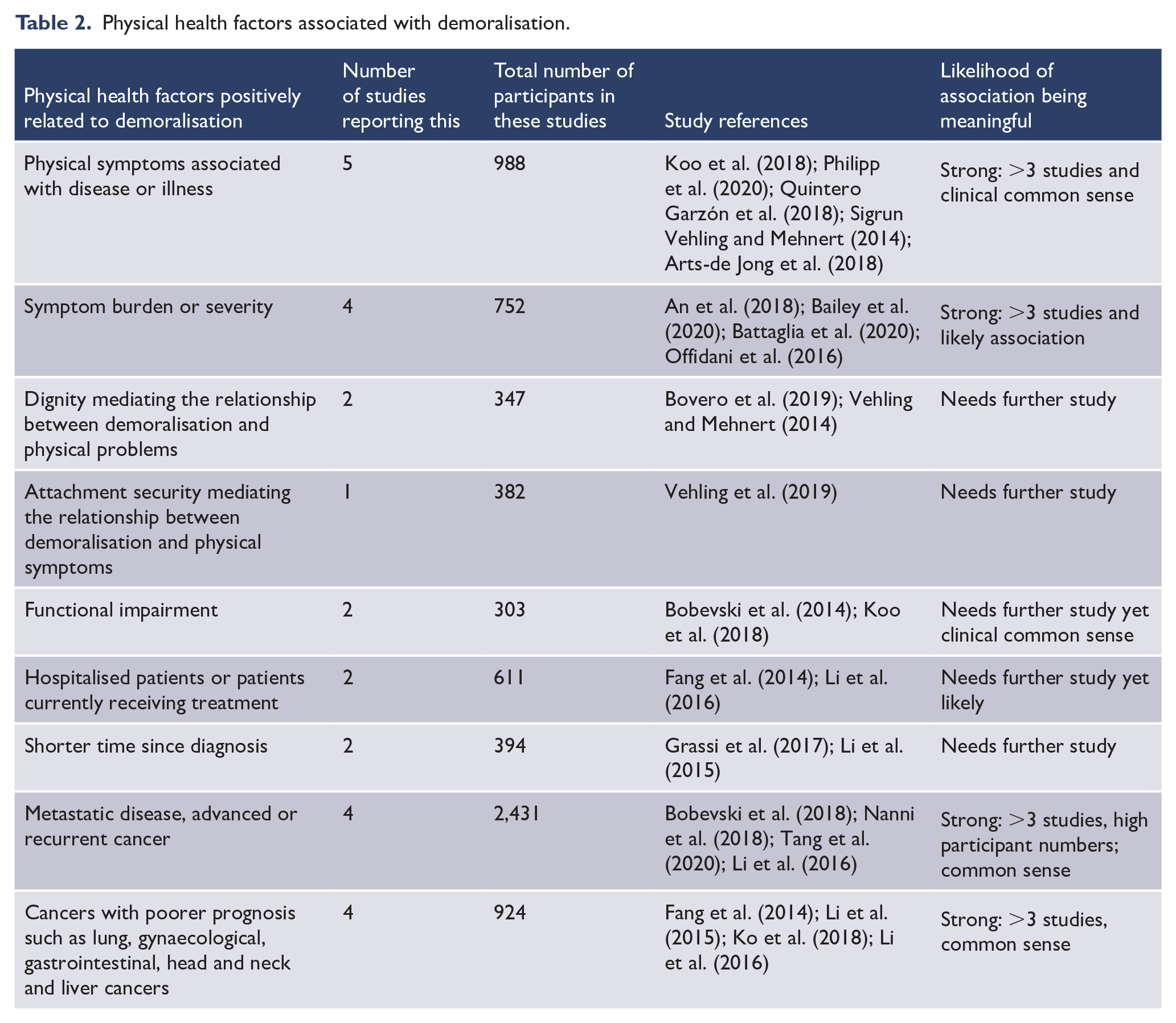
Physical health factors associated with demoralisation.
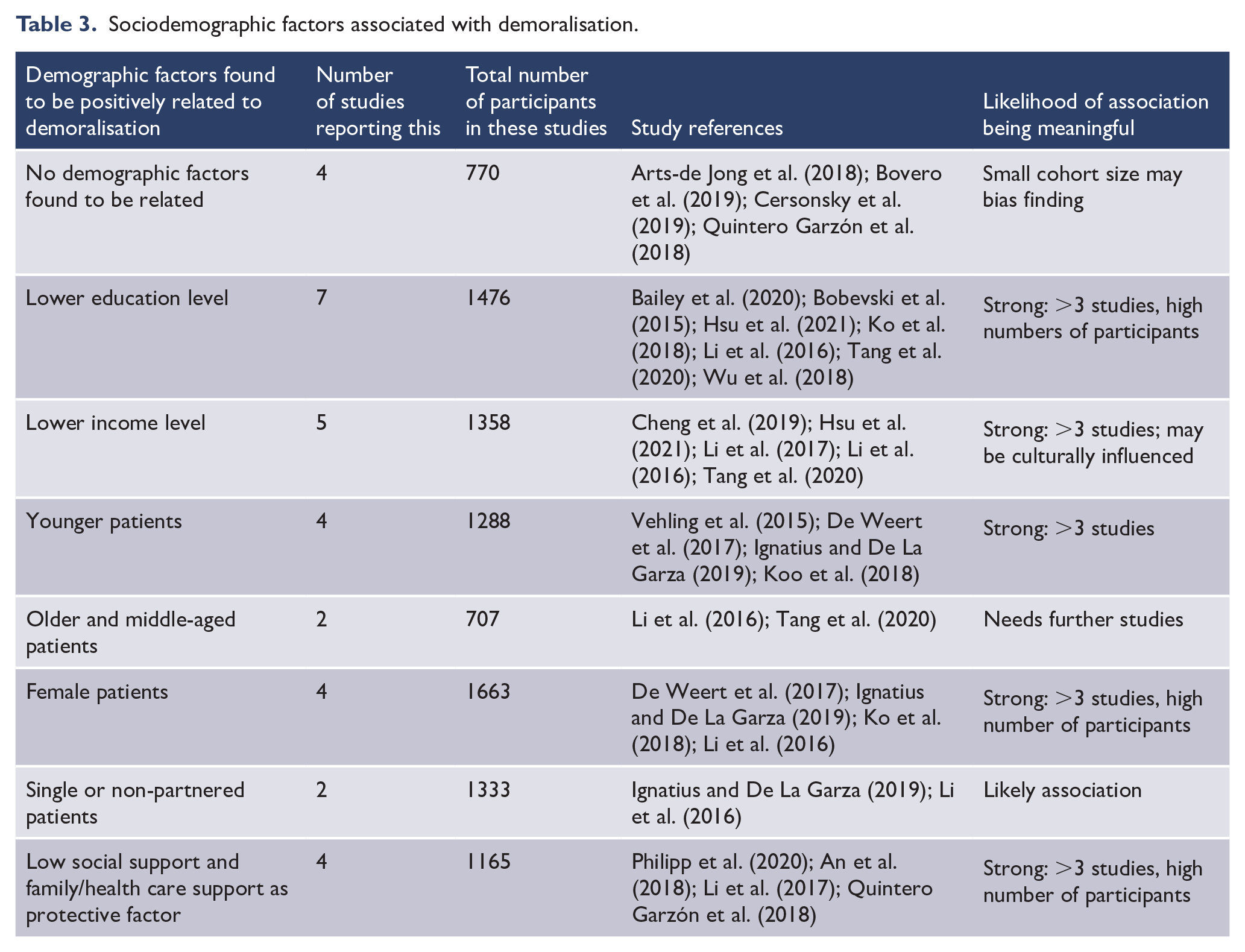
Sociodemographic factors associated with demoralisation.
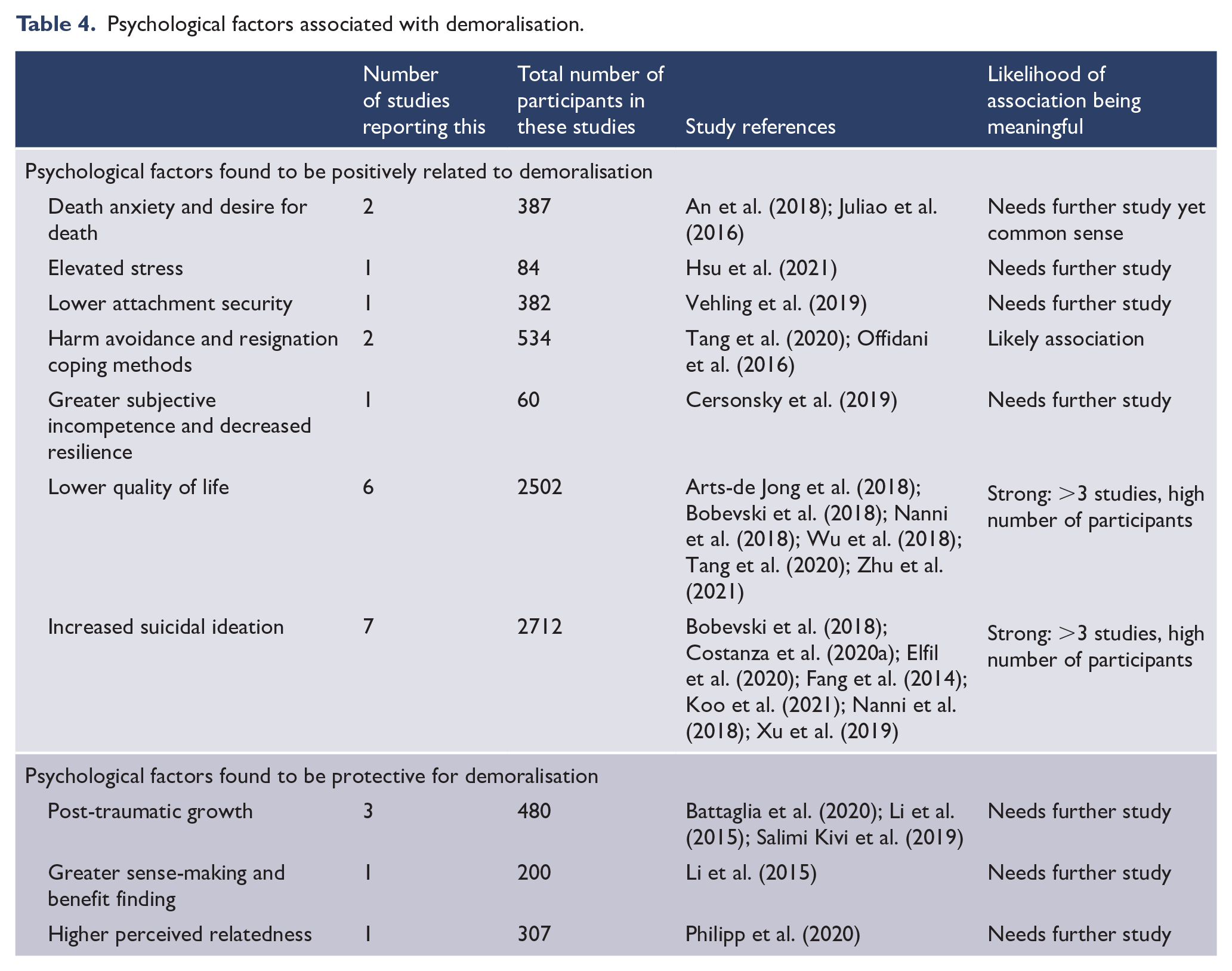
Psychological factors associated with demoralisation.
Physical health burden
Overall, it was found that poor physical health (Arts-de Jong et al., 2018; Koo et al., 2018; Philipp et al., 2020; Quintero Garzón et al., 2018; Vehling and Mehnert, 2014) and burdensome physical symptoms (An et al., 2018; Bailey et al., 2020; Offidani et al., 2017) are strongly correlated with demoralisation. Attachment security (Vehling et al., 2019) and dignity (Bovero et al., 2019; Vehling and Mehnert, 2014) were found to mediate the relationship between demoralisation and physical problems. Additionally, functional impairment (Bobevski et al., 2014; Koo et al., 2018) and treatment-related factors such as treatment stage, advanced disease (Bobevski et al., 2018; Li et al., 2016; Nanni et al., 2018; Tang et al., 2020) and time since diagnosis (Grassi et al., 2017; Li et al., 2015) were found to influence demoralisation.
Demographic factors
Generally, inconsistent associations were identified between demographic and medical factors, as observed in previous systematic reviews. Some studies identified no demographic factors as being predictive of higher levels of demoralisation, although cohort sizes were smaller for some (see Table 3) with potential sample bias resulting (Arts-de Jong et al., 2018; Bovero et al., 2019; Cersonsky et al., 2019; Quintero Garzón et al., 2018). Other studies reported that patients with lower education (Bailey et al., 2020; Bobevski et al., 2015; Hsu et al., 2021; Ko et al., 2018; Li et al., 2016; Tang et al., 2020; Wu et al., 2018), lower income level (Cheng et al., 2019; Hsu et al., 2021; Li et al., 2016, 2017; Tang et al., 2020), female gender (De Weert et al., 2017; Ignatius and De La Garza, 2019; Ko et al., 2018; Li et al., 2016) and younger age (De Weert et al., 2017; Ignatius and De La Garza, 2019; Koo et al., 2018; Vehling et al., 2015) were relatively more demoralised. Additionally, being single/non-partnered (Ignatius and De La Garza, 2019; Li et al., 2016) and having poor social support were found to mediate higher demoralisation (An et al., 2018; Li et al., 2017; Philipp et al., 2020; Quintero Garzón et al., 2018). The demographic factors associated with demoralisation are summarised in Table 3.
Psychological factors
Demoralisation was negatively associated with post-traumatic growth (Battaglia et al., 2020; Li et al., 2015; Salimi Kivi et al., 2019), sense-making and benefit finding (Li et al., 2015). Patients who made more sense of their cancer diagnosis, found greater benefit from, or experienced higher post-traumatic growth after diagnosis experienced less demoralisation (Li et al., 2015).
Other factors such as positive life orientation, avoidance and resignation coping methods (Offidani et al., 2016; Tang et al., 2020), attachment security (Vehling et al., 2019) and death anxiety (An et al., 2018) were also found to be significantly related to demoralisation. There is evidence of higher levels of perceived relatedness (Philipp et al., 2020), greater subjective incompetence and less resilience in those demoralised (Cersonsky et al., 2019).
Quality of life
High demoralisation was associated with a significantly lower quality of life (QOL; Arts-de Jong et al., 2018; Bobevski et al., 2018; Nanni et al., 2018; Tang et al., 2020; Wu et al., 2018; Zhu et al., 2021). Demoralisation was found to affect mental (Nanni et al., 2018; Tang et al., 2020) and physical aspects of QOL (Nanni et al., 2018; Wu et al., 2018); depression was found to mediate the relationship between demoralisation and physical aspects of QOL (Tang et al., 2020).
Risk of suicide
Suicidal ideation was significantly associated with demoralisation in seven studies reporting on 2712 participants (Bobevski et al., 2018; Costanza et al., 2020a; Elfil et al., 2020; Fang et al., 2014; Koo et al., 2021; Nanni et al., 2018; Xu et al., 2019). Additionally, demoralisation was found to have a greater or separate influence on suicidal ideation than depression (Costanza et al., 2020a; Fang et al., 2014; Koo et al., 2021; Vehling et al., 2017) and other psychiatric disorders such as adjustment disorder (Vehling et al., 2017). Patients with depression and demoralisation were also identified to have an increased level of suicidal ideation above the effect of depression alone (Fang et al., 2014).
The psychological factors associated with demoralisation are summarised in Table 4.
Discussion
Overall, among 52 studies comprising 11,670 mostly medically ill participants, demoralisation has been prevalent in 24–35% using a validated self-report measure reporting % prevalence. A higher prevalence (24–36%) was found in oncology compared to non-oncology (24–32%) studies. This is a higher prevalence than reported in a previous systematic review conducted by Robinson et al. (2015). Study heterogeneity explains the variance in findings. Overall demoralisation is prevalent across a range of different clinical sample populations and is a ‘transdiagnostic’ construct that signifies the importance of coping across different medical predicaments (Dalgleish et al., 2020).
The importance of recognising demoralisation
These studies have repeatedly differentiated demoralisation from other mood disorders such as depression, anxiety and adjustment disorder. There was a significant proportion of patients that were demoralised yet did not show any symptoms of depression, which is consistent with previous studies in oncology (Kissane et al., 2004; Mehnert et al., 2011; Mullane et al., 2009; Robinson et al., 2015; Tecuta et al., 2015) and mental illness populations (Grassi et al., 2020). The hallmark of demoralisation has been identified in the prevalence of subjective incompetence and decreased meaning secondary to loss of direction, contributing ultimately to feelings of helplessness and hopelessness. This contrasts with depression being described as a syndrome of anhedonia with predominant loss of consummatory pleasure; where there is general loss of motivation rather than a lack of objective to an individual’s goals and purpose in life (Clarke et al., 2003; de Figueiredo, 2013). Recent studies using network analysis have confirmed that symptoms of depression occupy a separate community to the symptoms of demoralisation (Murri et al., 2020b).
Comorbidity between demoralisation and depression has been consistent, however, throughout these empirical studies and was well exemplified in the latent class analysis by Bobevski et al. (2018). There was a high probability of the demoralisation symptoms being found among the cluster with the most severe psychopathology, as well as the cluster reflecting adjustment disorders. When the symptoms of demoralisation are conceptualised as phenomena associated with poor coping, it is quickly apparent that these are expected with mental illnesses, such as major depressive episodes and anxiety disorders, as well as in settings of maladaptive adjustment. A recent study exploring demoralisation in a psychiatric sample of patients with affective, non-psychotic disorders corroborated the high prevalence of demoralisation (50%) among comorbid anxiety, adjustment or depressive disorders (Grassi et al., 2020).
Significantly, suicidal ideation was strongly associated with demoralisation and demoralisation was identified to mediate suicidal ideation independently of anhedonia.
This has been emphasised in a more recent study (Costanza et al., 2020a). Additionally, hopelessness in relation to demoralisation has both historically and more recently been found to mediate associations with increased levels of suicidal ideation in both refugee and cancer populations (Briggs and Macleod, 2010; Liu et al., 2020). This is consistent with hopelessness being independently associated with a desire for hastened death in terminally ill cancer patients (Breitbart et al., 2000).
Demoralisation presents commonly in patients with schizophrenia and contributes to a greater risk of suicide independent of depression (Berardelli et al., 2019). Overall, this suggests a strong clinical need to identify demoralisation because of its elevated suicidal risk and the need for more urgent institution of management and therapeutic intervention.
The studies in this review that examined mental illness and non-oncological populations demonstrate a similar level of demoralisation to that observed in oncology and palliative settings. The significant burden of illness, irrespective of its mental or physical origins, relates to the development of demoralisation.
Importance of sociodemographic factors associated with demoralisation
Physical health burden was found to be positively correlated with demoralisation. Treatment-related factors were also significant; hospitalised patients, patients currently receiving treatment, a shorter time since diagnosis and more advanced cancer or recurrent disease were associated with higher levels of demoralisation. Previous studies have demonstrated that psychological and social factors related to physical illness rather than the severity of the illness contribute to the incidence of demoralisation (Clarke et al., 2005). Palliative treatment intention is more influential than tumour stage in an oncology population (Vehling et al., 2012).
As reported in prior systematic reviews (Robinson et al., 2015; Tecuta et al., 2015), inconsistent evidence surrounds some demographic factors such as age. Generally, poorer education, lower income, being female and single or lacking social supports were associated with higher demoralisation. Lower socioeconomic status is associated with chronic stress that contributes over time to learned helplessness and powerlessness (Baum et al., 1999); this correlates directly with the core features of hopelessness and loss of purpose inherent to demoralisation. Additionally, social isolation can potentially magnify the threat of existential distress associated with demoralisation. This is reflected in previous studies identifying a positive relationship between poor social and family support on higher demoralisation (Marchesi and Maggini, 2007; Mehnert et al., 2011); the wider literature also corroborates the association between stronger social supports and how this fosters neurobiological changes that contribute to higher levels of resilience, lower emotional distress and increased ability to cope with illness (Kim et al., 2010; Ozbay et al., 2007).
Exploring the need to understand demoralisation as it transcends culture and language
A high prevalence of demoralisation has been observed across cultures. The meaning of life may differ as do Western and Eastern world views. Cultural stigma and perception surrounding suicidal ideation can vary across ethnicities (Xu et al., 2019). Irrespective of this though, the enduring human need for dignity and meaning in life appears to transcend cultures. Significant psychological factors identified here such as sense-making, perceived relatedness and subjective incompetence would do well to be explored in a cultural framework; this will assist the interpretation of demoralisation through various ethnic and cultural nuances. de Figueiredo and Gostoli (2013) have alluded to the importance of understanding ‘idioms’ of distress unique to specific cultures.
Compared to previous reviews (Robinson et al., 2015; Tang et al., 2015; Tecuta et al., 2015), this review provides further evidence of the high prevalence of demoralisation across a range of medical illnesses in addition to its differentiation from and comorbidity with related constructs such as depression and anxiety, the associated risk of suicide and related sociodemographic and psychological factors. This contributes further to the evidence corroborating the significance and diagnostic value of demoralisation syndrome since these previous reviews were completed in 2015.
Clinical significance
Given the past two decades of research exploring demoralisation, its clinical significance and distinction from other syndromes, consideration of its inclusion within DSM and ICD systems continues to be warranted. The incorporation of the mental state of demoralisation as a ‘specifier’ within the DSM nosological system appears to be worthwhile. Specifically, demoralisation can be diagnosed when there is the presence of the core symptoms of ‘hopelessness’, ‘low morale’, ‘poor coping’ and ‘meaninglessness’. There is immediate applicability of this specifier to the diagnoses of mood and adjustment disorders, with particular value in bringing attention to poor coping in depression and increasing targeted therapy towards sustaining purpose and meaning in life. Indeed, a vignette-based study of the utility of this specifier revealed enhanced illness understanding, treatment selection and ease of communication with colleagues (Kissane et al., 2017). The growing body of research identifying demoralisation as a mediator of suicidal ideation serves as a powerful reason to proceed with this development.
Recent studies have generated evidence for the unidimensional nature of adjustment disorder, with proposals for ICD-11 suggesting that adjustment disorder be elevated from a hierarchical classification system to the status of an axis one disorder (Glaesmer et al., 2015). Other critiques have expressed concern about the subjective interpretation of maladaptive coping to generate a diagnosis of adjustment disorder (Strain, 2019). When the phenomenology of low morale and poor coping associated with the development of demoralisation are brought to the fore, as in this review, a richer set of symptoms becomes possible to strengthen the diagnostic criteria for adjustment disorder and allow it to be identified more readily in clinical populations. Historically, there has been a paucity of empirical studies on adjustment disorder (Bachem et al., 2017). There is much still to do and with relative urgency!
Limitations
Limitations of this review include the heterogeneity of the study populations, inconsistent thresholds for clinical significance across these studies and variation in outcome measures. Additionally, the use of convenience sampling and/or a cross-sectional design create a selection bias that hinders generalisability. We examined studies published in the English language. However, there were a variety of countries represented, including but not limited to Canada, The Netherlands, Spain, Germany, Italy, Australia, China, Taiwan and the United States. Also, despite the inclusion criteria extending to medical illnesses beyond cancer, the majority of the studies from the initial search (59%) still represented the experiences of oncology patients. This is a consequence of the early research alignment of demoralisation studies.
Future directions
Demoralisation is currently being examined in patients with epilepsy (Terza et al., 2019), type 2 diabetes (Benasi et al., 2019), refugees (Briggs and Macleod, 2010), veterans (Kelsall et al., 2016) and transgender/gender-diverse populations (Woodrum et al., 2021). Further studies are needed in prison populations where there is already existing evidence of existential distress and loss of life’s meaning (Vanhooren et al., 2015), in addition to psychiatric disease, adolescents and young adults and elderly populations.
This review further cements the need for recognition of demoralisation in various patient settings with the view to initiate targeted intervention and prevent significant morbidity. In addition to cognitively oriented and existential therapies, meaning-centred therapy has been identified as a targeted treatment for demoralisation (Kissane, 2017). The semi-structured intervention, ‘Managing Cancer and Living Meaningfully’ (Nissim et al., 2012), has shown a moderate effect size in ameliorating demoralisation in patients with high baseline death anxiety (Caruso et al., 2020; Rodin et al., 2018). Additionally, logotherapy, a therapy developed based on individuating life and existential meaning, has been demonstrated to be effective in the reduction of demoralisation in breast and gynaecological cancer patients (Sun et al., 2021).
In our global world, the role that the COVID-19 pandemic has played in generating demoralisation is worth further exploration. As COVID-19 presents an existential threat which can evoke helplessness, its important risk of inducing suicide in the context of loss of the meaning of life becomes clear (Costanza et al., 2020b).
Supplemental Material
sj-docx-1-anp-10.1177_00048674211060746 – Supplemental material for Mental state of demoralisation across diverse clinical settings: A systematic review, meta-analysis and proposal for its use as a ‘specifier’ in mental illness
Supplemental material, sj-docx-1-anp-10.1177_00048674211060746 for Mental state of demoralisation across diverse clinical settings: A systematic review, meta-analysis and proposal for its use as a ‘specifier’ in mental illness by Lucy L Gan, Susanna Gong and David W Kissane in Australian & New Zealand Journal of Psychiatry
Footnotes
Authors’ Note
The underlying data from this review can be accessed by contacting the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.