
Abstract
Objective:
Anxiety and depression are the most common mental health disorders experienced by Australians. These disorders are commonly found in people who use methamphetamine; however, much of this research has involved participants recruited from treatment settings who inject methamphetamine. We therefore explored (1) the prevalence of moderate to severe anxiety and depression in a community-recruited cohort who smoked methamphetamine and (2) examined potential factors associated with moderate to severe anxiety or depression in this cohort.
Method:
Data were derived from baseline surveys of 725 participants of the prospective ‘VMAX’ study, recruited from metropolitan and non-metropolitan areas of Victoria, Australia, via snowball and respondent-driven sampling. Anxiety and depression were measured using the Generalized Anxiety Disorder-7 and the Patient Health Questionnaire-9 instruments. Independent associations between moderate to severe scores on these measures and demographic, socio-economic, substance use and other health and social characteristics were examined using multivariable logistic regression.
Results:
More than half (60%) of the participants were classified as experiencing moderate to severe anxiety and/or depression. In the multivariable models, having poor/very poor self-rated health, methamphetamine dependence and being unemployed were associated with higher odds of experiencing both moderate to severe depression and moderate to severe anxiety. Living in a large rural town, identifying as Aboriginal and Torres Strait Islander and smoking methamphetamine were associated with lower odds of experiencing moderate to severe depression. Being female was associated with higher odds of experiencing moderate to severe anxiety.
Conclusion:
The high rates of anxiety and/or depression found in the VMAX cohort were associated with demographic, socio-economic, substance use and other health and social factors. The prevalence of moderate to severe anxiety is a novel finding that warrants further study. Further work is needed to determine how anxiety and depression change over time among people who smoke methamphetamine, to help identify key intervention points.
Introduction
Anxiety and depression are highly prevalent mental health disorders; in Australia, in any given year, an estimated 13.1% of the population suffer from anxiety and 10.4% from depression (Australian Bureau of Statistics (ABS), 2018). There is considerable overlap between anxiety and depression; they are often concomitant, clinical treatment is similar for both conditions in terms of psychotherapy and pharmacotherapy, and having one of these disorders can be a risk factor for developing the other (Groen et al., 2020). Substance use disorders, the third most prevalent mental health disorder in Australia, commonly co-occur with anxiety and depression (Slade et al., 2009). People who use methamphetamine experience disorders such as anxiety and depression at a much higher rate than the general population (Australian Institute of Health & Welfare (AIHW), 2020). Results from the 2019 Australian National Drug Strategy Household Survey show that approximately 30.7% of the participants who had used methamphetamine in the past 12 months prior to the survey had been diagnosed or treated for a mental health disorder, such as anxiety or depression.
A recent systematic review of meth/amphetamine use and mental health outcomes by McKetin et al. (2019) highlighted that studies of the prevalence of anxiety and depression and their relation to methamphetamine use have primarily been undertaken in the United States. Findings indicated that those who use methamphetamine have higher odds of experiencing depression, psychosis and suicidality than those who do not; however, evidence of an association between methamphetamine use and anxiety was not found. Most of the included studies were limited to samples recruited from treatment or criminal justice settings.
Using methamphetamine in addition to having a mental health disorder can result in poorer health outcomes compared to using methamphetamine without mental ill-health (Darke et al., 2008). Importantly, among people who use methamphetamine, a number of potential risk factors for mental health disorders, such as anxiety and depression, have been identified across demographic, socio-economic, substance use, and other social and health domains. Demographic factors associated with mental health disorders in those who use methamphetamine include being male (Akindipe et al., 2014), single (Patterson et al., 2015), aged under 25 (Akindipe et al., 2014), living in a non-metropolitan location (Wallace et al., 2009) and identifying as Aboriginal and Torres Strait Islander (AIHW, 2020). Socio-economic factors include being unemployed (Lee et al., 2012), having lower levels of education (Chang et al., 2018), experiencing homelessness (Chang et al., 2018) and having low levels of social support (Zhang et al., 2020). Substance use factors include intravenous methamphetamine use (Chang et al., 2018), polydrug use in the past month (Su et al., 2017), greater number of years using methamphetamine (Ma et al., 2018) and high levels of dependence (Chang et al., 2018). Other social and health risk factors include having been a victim of violence (Khalkhali et al., 2016) and poorer self-reported health status (Greenwell and Brecht, 2003).
Co-occurring methamphetamine use and anxiety or depression is more challenging to treat than one of these conditions alone (Akindipe et al., 2014), and the risk factors for these three conditions are often shared (McKetin et al., 2019). For those who use methamphetamine and have anxiety and/or depression, successfully engaging with professional support can be difficult (Glasner et al., 2010; Hellem et al., 2015). Impediments include difficulty accessing services, and adhering to treatment (Booth et al., 2010), which can be compounded by the challenges clinicians experience when working with this population (Najt et al., 2011). Treatment outcomes for those with co-occurring substance use and mental health disorders may be enhanced through early consideration of risk factors associated with more severe disability and timely provision of appropriate interventions and support (Najt et al., 2011).
While the mental illness sequelae of methamphetamine use are well-documented (McKetin et al., 2019; Zhang et al., 2020), studies have primarily focused on participants who inject methamphetamine recruited from criminal justice or treatment settings (McKetin et al., 2019). However, smoking methamphetamine is the most common route of administration in Australia (AIHW, 2020). Furthermore, only half of those who primarily smoke methamphetamine seek out or utilised professional support (Quinn et al., 2020). Therefore, it is important to better understand the experience of anxiety and depression in those recruited from community-based settings who smoke methamphetamine.
The aims of this study were to: (1) determine the prevalence rates of moderate to severe anxiety and depression in a cohort of methamphetamine users that smoke methamphetamine, and are community recruited; and (2) examine whether the experience of moderate to severe anxiety and moderate to severe depression was associated with specific demographic, socio-economic, substance use and/or other social and health factors
Method
Design
This is a cross-sectional analysis of 743 VMAX study participants. VMAX, a prospective cohort study, seeks to understand the natural trajectory of people recruited in Victoria, Australia, who smoke methamphetamine in relation to methamphetamine use patterns and other health and lifestyle factors (Quinn et al., 2020). Eighteen participants were excluded for having incomplete data, which allowed individual-level analysis of the remaining 725 participants from the baseline dataset. Although a detailed description of the VMAX study methods has been published (Quinn et al., 2020), a brief description of the recruitment and data collection methods follows. Respondent-driven sampling (RDS) and snowball sampling approaches were used in conjunction with targeted sampling through online advertising and posters, to recruit participants from metropolitan Melbourne and three rural areas in the state of Victoria. Participants were eligible if they were aged 18 years or over, used any form of methamphetamine at least monthly during the past 6 months and primarily used methamphetamine via non-injecting routes of administration (e.g. smoking, snorting). Due to a slower period of recruitment, the latter criterion was relaxed in order to reach an acceptable sample number, and RDS was heavily relied upon (Quinn et al., 2020). Face-to-face baseline interviews, which took up to 60 minutes, were conducted in mutually agreed locations. A structured survey using REDCap (Harris et al., 2009) that canvassed a range of demographic, socio-economic, substance use, and social and health-related variables was interviewer-administered. Participants were reimbursed AUD40 for their time and out-of-pocket expenses. Participants were also reimbursed AUD20 per peer (up to a maximum of three) referred to the study as per the RDS protocol.
Measures
Outcome variables
Symptoms of anxiety were assessed using the 7-item Generalized Anxiety Disorder (GAD-7) scale (Rutter and Brown, 2017), and symptoms of depression were assessed using the 9-item Patient Health Questionnaire (PHQ-9) (Beard et al., 2016). Both scales have been found to be valid and reliable measures (Kroenke et al., 2016). For both scales, participants rated their experience of symptoms in the last fortnight using a 4-point Likert-type scale ranging from ‘not at all’ (0) to ‘nearly every day’ (3). Those scoring 10 or above in either scale were classed as having moderate to severe anxiety or depression (Kroenke et al., 2016).
Independent variables
Variables were selected for analysis on the basis of the literature as outlined in the Introduction above. Factors included gender (male or female), age (number of years), residential location, Aboriginal and Torres Strait Islander status (yes or no), relationship status (in a relationship or single), employment (yes or no), education (⩾Year 11 or ⩽Year 10), homelessness in the past 12 months (no or yes), social support, the most common route of administration in the past month (injecting, smoking or other), polysubstance use, dependence, years of methamphetamine use (number of years), being a victim of violence in the past 6 months and self-rated health status (good health or poor health).
Residential location was classified using five categories of the Modified Monash Model (MMM) (Australian Government Department of Health, 2020): metropolitan areas or major cities (MMM 1), regional centres (MMM 2), large rural towns (MMM 3), medium rural towns (MMM 4) and small rural towns (MMM 5). Due to the small number of participants in MMM 4 and MMM 5 locations, these two categories were combined.
To measure degree of access to self-perceived social support, the ENRICHD Social Support Instrument (ESSI) 7-item scale was utilised (Vaglio et al., 2004). Participants were asked to indicate the response that most closely matched their current situation using a 5-point Likert-type scale ranging from ‘none of the time (1)’ to ‘all of the time (5)’. A total score of ⩽18 was categorised as low social support while scores of 19–34 were classified as medium to high social support (Vaglio et al., 2004).
Polydrug use was calculated by the number of drugs used within the past month (Karjalainen et al., 2017). Scores ranged from 0 to 13, with 0 indicating no polydrug use. Substances included pharmaceutical stimulants (e.g. methylphenidate, dexamphetamine), ecstasy/3,4-methylen edioxymethamphetamine (MDMA), cocaine, gamma hydroxybutyrate (GHB), ketamine, illicit benzodiazepines (e.g. Valium, Xanax, Oxazepam), illicit pharmacotherapy, heroin, other illicit opiates (e.g. morphine, oxycodone), amyl nitrate, other inhalants (e.g. nitrous, paint, petrol), hallucinogens (e.g. lysergic acid diethylamide (LSD), psilocybin), alcohol, tobacco and cannabis.
Dependence for methamphetamine was measured using the Severity of Dependence Scale (SDS). The SDS measures psychological aspects of dependence related to concerns about impaired control over, and preoccupation and anxieties about, drug use (Gossop et al., 1995). Participants who recorded an SDS score of ⩾4 were classified as methamphetamine-dependent (Topp and Mattick, 1997).
Statistical analysis
Contingency table analyses were undertaken to provide prevalence of moderate to severe depression and moderate to severe anxiety across each independent variable. Bivariable logistic regression was used to examine associations between each outcome and the independent variables. Analyses were conducted using SPSS software (version 26.0.0) with a significance level of p < 0.05. Odds ratios (ORs), adjusted odds ratios (aORs), 95% confidence intervals (CIs) and p-values are reported. A complete case approach was used to treat missing data on covariates. Variance inflation factor (VIF) analyses were used to test for collinearity between independent variables; all VIFs were below 10, indicating no problematic collinearity.
Ethics
The study was approved by the Alfred Hospital (Project number: 171/16) and Monash University Human Research Ethics Committees (Project number: 2938). Written informed consent was obtained from each participant prior to enrolment in the study.
Results
Sample characteristics
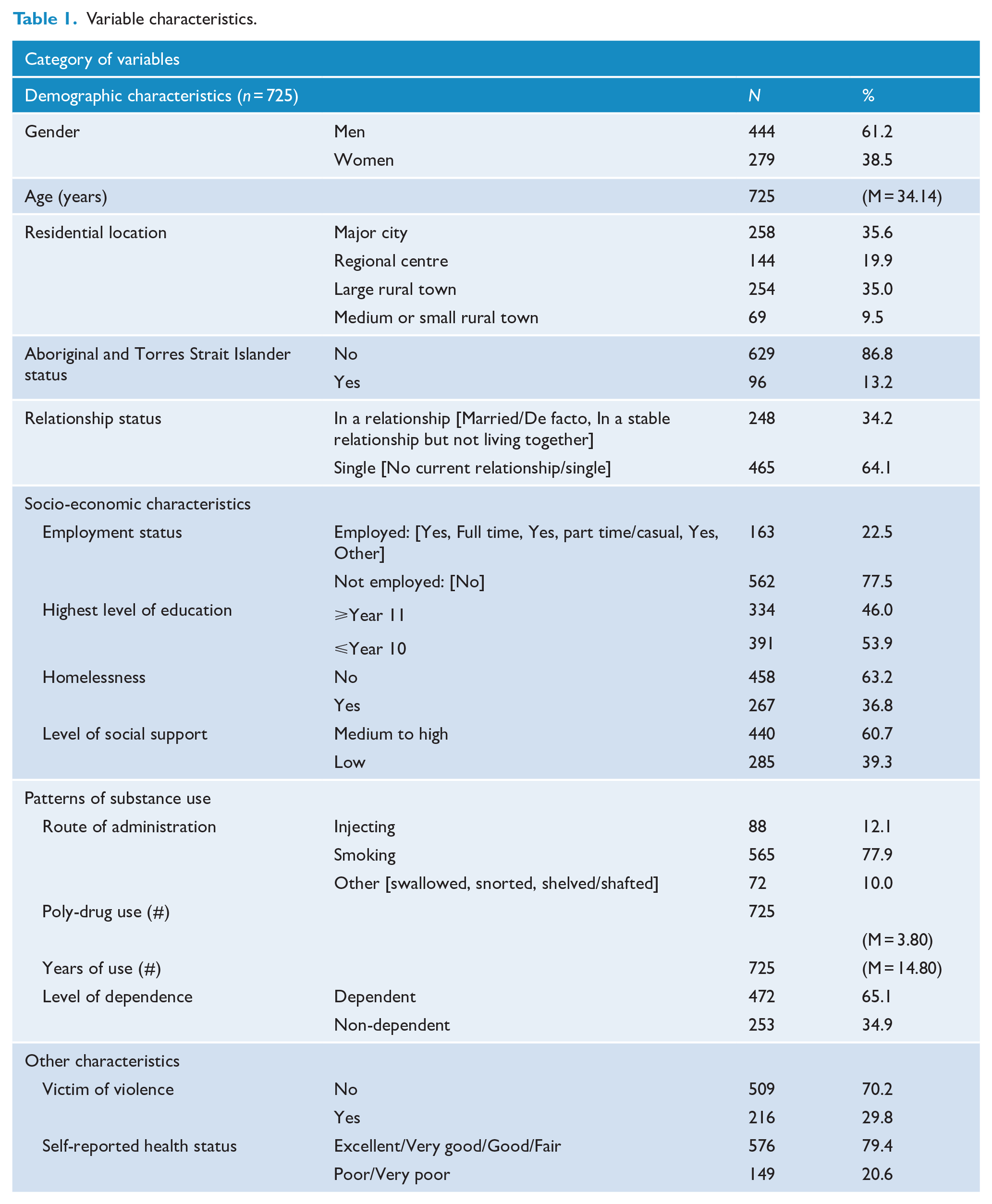
Characteristics of the 755 participants are detailed in Table 1. Ages ranged from 18 to 68 years (mean = 34 years). Almost two thirds (61.2%) of participants identified as male and 13.2% identified as Aboriginal and/or Torres Strait Islander. A little over a third (35.6%) of participants resided in a metropolitan area or major city, a fifth (19.9%) in a large regional centre, just over a third (35.0%) in a large rural town and the remainder (9.5%) in a medium to small town. The majority (77.5%) of participants were unemployed, over half (53.9%) had not completed school beyond year 11 and over a third (36.8%) had experienced homelessness in the past 12 months.
Variable characteristics.
As shown in Table 2, 60% of participants scored in the moderate to severe range for anxiety only (8%), depression only (13%) or both (38%). While approximately half (51%) of the participants scored in the moderate to severe range for depression, slightly less than half (46%) scored in the moderate to severe range for anxiety. There was a moderate positive correlation between anxiety and depression scores, r = 0.70, n = 725, p < 0.001 (R2 = 0.49).
Percentage distribution of PHQ-9 (depression) and GAD-7 (anxiety) scores, n = 725.
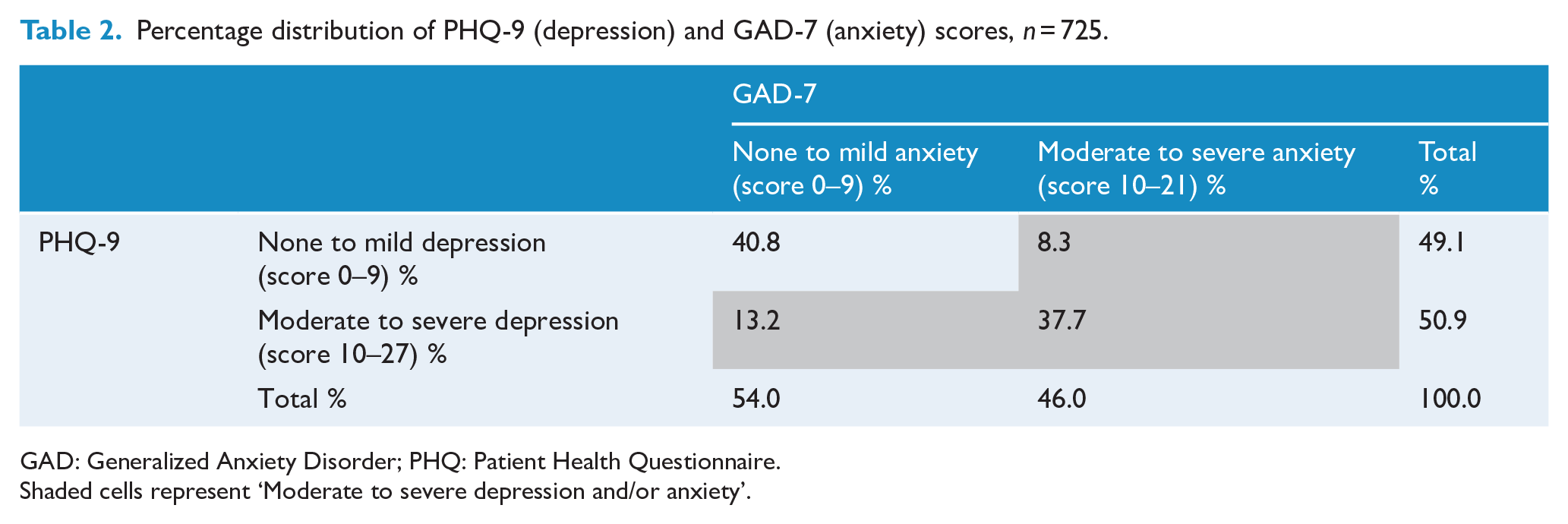
GAD: Generalized Anxiety Disorder; PHQ: Patient Health Questionnaire.
Shaded cells represent ‘Moderate to severe depression and/or anxiety’.
Independent correlates of depression or anxiety
Bivariable analyses found gender, residential location, employment, social support, methamphetamine dependence, victim of violence and self-reported health status were associated with moderate to anxiety (see Table 3) and moderate to severe depression (see Table 4). Homelessness was also associated with moderate to severe anxiety. After adjustment for all of the variables included in the models, three of the independent variables remained statistically significant for both moderate to severe anxiety (Table 3) and for moderate to severe depression (Table 4): self-reported health, methamphetamine dependence and employment status.
Bivariable and multivariable logistic regression showing associations with moderate to severe anxiety: unadjusted, adjusted odds ratios (aORs), 95% confidence intervals (95% CIs) and probability values (p-values).
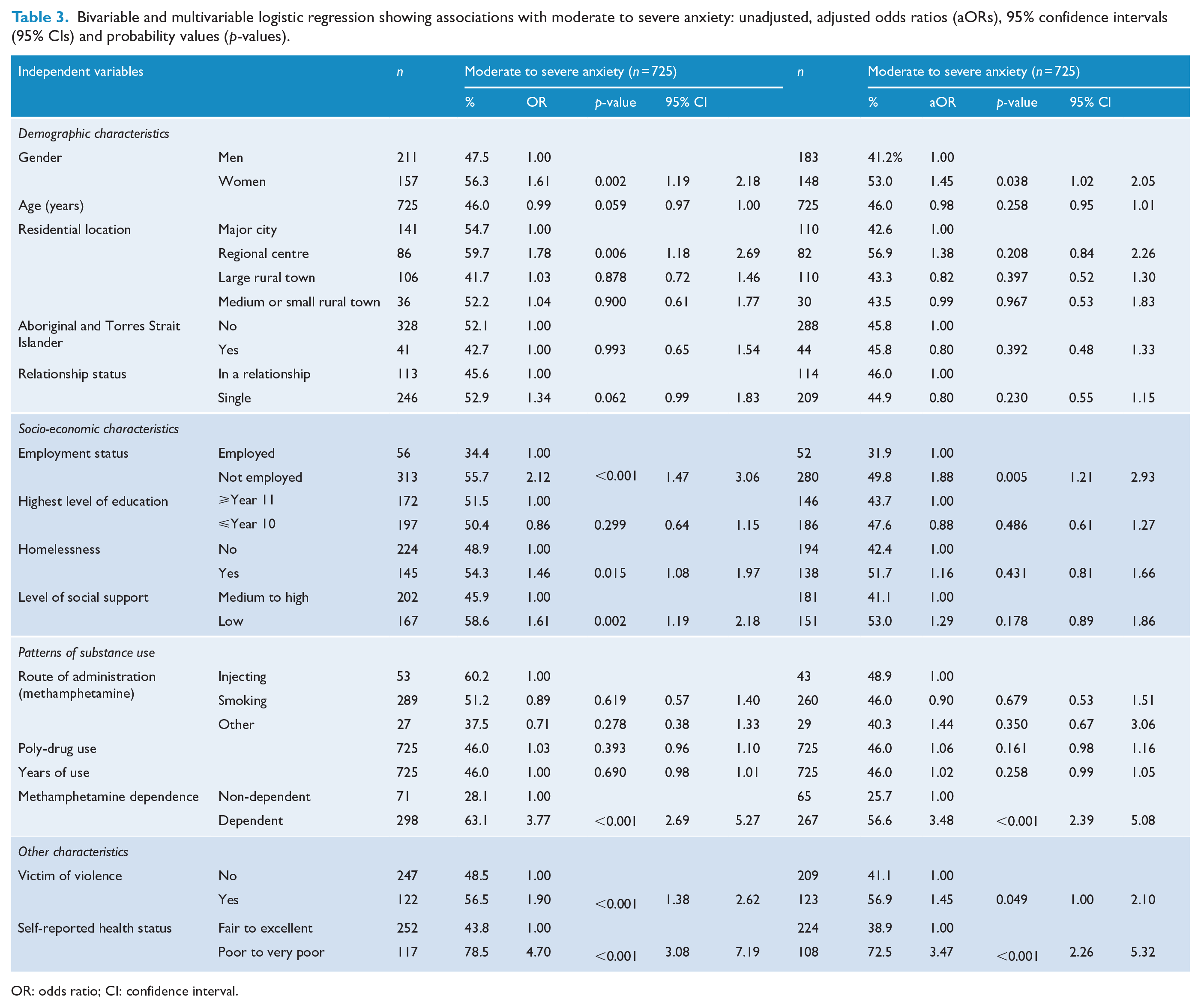
OR: odds ratio; CI: confidence interval.
Bivariable and multivariable logistic regression showing associations with moderate to severe depression: unadjusted, adjusted odds ratios (aORs), 95% confidence intervals (95% CIs) and probability values (p-values).
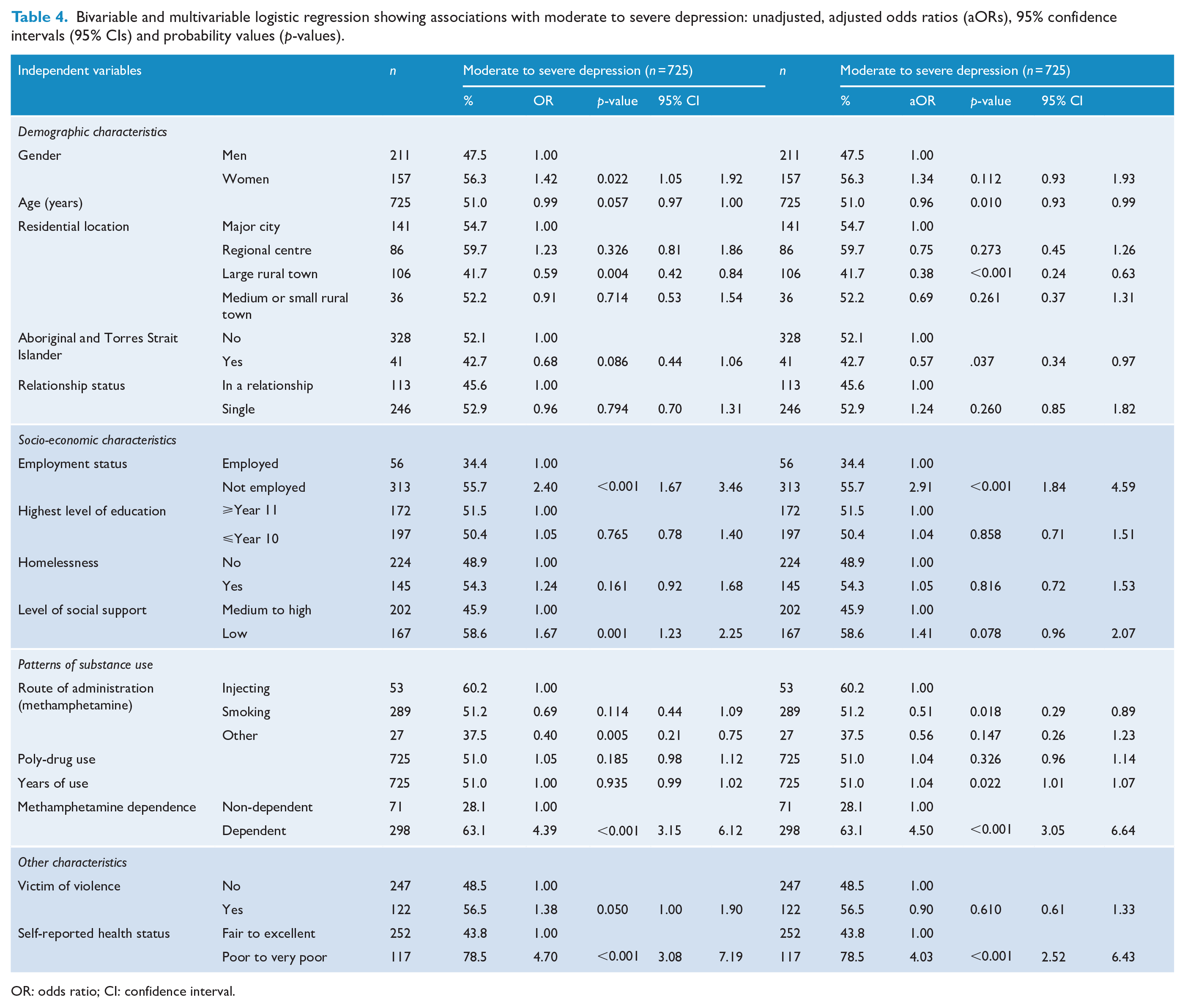
OR: odds ratio; CI: confidence interval.
As reported in Table 3, participants had greater odds of reporting moderate to severe anxiety if they were a woman (p = 0.038, aOR = 1.45, 95% CI = [1.02, 2.05]), believed they were of poor or very poor health (p < 0.001, aOR = 3.48, 95% CI = [2.27, 5.33]), were methamphetamine dependent (p < 0.001, aOR = 3.37, 95% CI = [2.31, 4.89]) or if they were experiencing unemployment (p < 0.005, aOR = 1.92, 95% CI = [1.23, 2.98]).
Table 4 illustrates that participants had greater odds of reporting moderate to severe depression if they believed they were of poor or very poor health (p < 0.001, aOR = 4.02, 95% CI = [2.52, 6.42]), were methamphetamine dependent (p < 0.001, aOR = 4.38, 95% CI = [2.98, 6.43]) or were unemployed (p < 0.001, aOR = 2.95, 95% CI = [1.87, 4.66]). Living in a large rural town (p < 0.001, aOR = 0.38, 95% CI = [0.24, 0.63]), identifying as Aboriginal and Torres Strait Islander (p = 0.037, aOR = 0.57, 95% CI = [0.34, 0.97]) and smoking methamphetamine (p < 0.018, aOR = 0.51, 95% CI = [0.29, 0.89]) were associated with lower odds of experiencing moderate to severe depression.
The Hosmer–Lemeshow goodness-of-fit test indicated the models fitted the data well, Depression: χ2 (8) = 8.8, p = 0.358; Anxiety: χ2 (8) = 10.3, p = 0.257.
Discussion
Over half (60%) of our sample of people who used methamphetamine scored in the moderate to severe range for anxiety and/or depression. The proportion of participants experiencing moderate to severe anxiety (46%) and depression (51%) was higher than Australians in the general population who had an anxiety-related condition (13%) or had depression (10%) (ABS, 2018). Our findings accord with prior research examining the prevalence of depressive symptoms in those who use methamphetamine (McKetin et al., 2019), but the results in respect to anxiety and concurrent depression and anxiety are more novel.
Methamphetamine use is associated with a range of health concerns, such as cardiovascular disease, cerebrovascular disease (Darke et al., 2008), renal conditions and dental problems (McKetin et al., 2008a). Poor physical health is known to be a significant cause of psychological stress (Phillips and Murrell, 1994). Our finding that self-rated poor health was positively associated with moderate to severe anxiety and moderate to severe depression is therefore unsurprising. We also found that unemployment and methamphetamine dependence were associated with experiencing moderate to severe depression and anxiety. While this finding supports previous research findings that have suggested that dependence and unemployment are significant risk factors for psychiatric morbidity in people that use methamphetamine (Chang et al., 2018), the inter-relationships between common mental health issues and dependence and/or unemployment are not well understood. Indeed, these factors can be indicators of social disadvantage, poverty or isolation, which are known to influence the development of or worsen the symptoms of both depression and anxiety (Stansfeld et al., 2011).
Another finding of the present study was that the female participants were more likely to have higher odds of experiencing moderate to severe anxiety compared to their male peers, but there was no gender difference between males and females for moderate to severe depression. This is consistent with findings from the National Health Survey (ABS, 2018). Given the paucity of gender-specific research on anxiety and/or depression in people that use methamphetamine, this finding suggests that further research in this area is warranted.
These findings highlight that drug and alcohol, mental health and primary health services are likely to frequently encounter high levels of anxiety and depression among people who use methamphetamine, irrespective of route of administration. In Australia, primary health care services play an important role in the management and/or referral for the treatment of mental illness (Cross and Hickie, 2017). Consumers who use methamphetamine report primary care services as their most common point of contact with the health care system (McKetin et al., 2018; Quinn et al., 2020), yet some primary care providers report they do not see and/or are reluctant to provide care to this population (Ward et al., 2021). Diagnoses of anxiety and/or depression may provide a segue into an integrated model of care whereby common comorbidities (e.g. depression/anxiety and methamphetamine use disorder) can be treated. Integrated models of care are associated with increased time for practitioners (Yu et al., 2018) to address underlying social disadvantage of health that are known to influence the development of or worsen the symptoms of both anxiety and depression (Stansfeld et al., 2011). Importantly, integrated models of care allow for a ‘no wrong door’ approach which allow increased opportunities for individuals who use methamphetamine to seek professional support for their mental health (Deady et al., 2014).
An important contribution that this study makes to the literature is the findings relating to anxiety. While comorbid anxiety is commonly associated with other types of substance use disorder (Pasche, 2012), the association between methamphetamine use and anxiety has received scant attention (McKetin et al., 2019). Importantly, our study also highlights the association between anxiety and depression, in those who smoke methamphetamine, a previously neglected area of research in Australia. The findings of our study are consistent with the high prevalence of anxiety and depression found in people who inject methamphetamine (Lee et al., 2012). While the odds for experiencing moderate to severe depression were lower for smokers in this study, the prevalence of anxiety and depression in this cohort is elevated relative to the general population. It is important that further research regarding methamphetamine smokers investigates the concurrent relationship of anxiety and depression, as well as anxiety independently.
A limitation was the cross-sectional nature of the study, so we cannot determine the causal direction of the associations observed. There is a need for more longitudinal research that highlights and examines the relationship between methamphetamine use and both depression or anxiety (McKetin et al., 2019). Longitudinal data of the VMAX study cohort will become available in the near future to examine the temporality of anxiety, depression and mental health service utilisation in this cohort. Additional limitations to be considered include social desirability bias, due to the sensitive nature of the questions of the survey, and the risk of recall bias due to the study relying on a self-report survey. Finally, the recruitment issues from Quinn et al. (2020) mean that the sample cannot be considered representative of all methamphetamine smokers.
This study has established that potentially a significant portion of community-based people who use methamphetamine may experience moderate to severe symptoms of anxiety or depression. Factors such as poor self-reported health, dependence and unemployment were related to higher odds of experiencing anxiety or depression. As services are likely to frequently encounter high levels of anxiety and depression among people who use methamphetamine, it is important that interventions and services are responsive to clients’ needs related to anxiety and/or depression, as well as their methamphetamine use.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The VMAX study was established with a grant from the Colonial Foundation and is now funded by the National Health and Medical Research Council (NHMRC, 1148170). P.D. is supported by an NHMRC Senior Research Fellowship. B.Q. was supported by a Postdoctoral Fulbright Scholarship during the 2016/2017 financial year. P.D. has received investigator-driven funding from Gilead Sciences and Indivior for work unrelated to this study.