
Abstract
Objective:
Chronic methamphetamine use is commonly associated with the development of psychotic symptoms. The predictors and correlates of methamphetamine-associated psychosis are poorly understood. We sought to systematically review factors associated with psychotic symptoms in adults using illicit amphetamine or methamphetamine.
Methods:
A systematic literature search was performed on MEDLINE (OVID), PsycINFO and EMBASE databases from inception to 8 December 2016. The search strategy combined three concept areas: methamphetamine or amphetamine, psychosis and risk factors. Included studies needed to compare adults using illicit methamphetamine or amphetamine, using a validated measure of psychosis, on a range of risk factors. Of 402 identified articles, we removed 45 duplicates, 320 articles based on abstract/title and 17 ineligible full-text articles, leaving 20 included studies that were conducted in 13 populations. Two co-authors independently extracted the following data from each study: country, setting and design; participant demographic and clinical details; sample size; measure/s used and measures of association between psychosis outcomes and risk factors. Individual study quality was assessed using a modified Newcastle-Ottawa Scale, and strength of evidence was assessed using GRADE criteria.
Results:
Frequency of methamphetamine use and severity of methamphetamine dependence were consistently found to be associated with psychosis, and sociodemographic factors were not. There was inconsistent evidence available for all other risk factors. Individual study quality was low–moderate for the majority of studies. Heterogeneity in study outcomes precluded quantitative synthesis of outcomes across studies.
Conclusion:
The most consistent correlates of psychotic symptoms were increased frequency of methamphetamine use and dependence on methamphetamine. The findings of this review highlight the need for targeted assessment and treatment of methamphetamine use in individuals presenting with psychosis.
Introduction
Amphetamine and methamphetamine (hereafter referred to as MA) are potent and addictive synthetic stimulant drugs that are widely used internationally. Illicit MA use is a growing public health concern globally, in part due to psychological harms such as psychosis (McKetin et al., 2017). Experimental studies have shown that psychosis symptoms triggered by MA correlate with excessive striatal dopamine release (Cruickshank and Dyer, 2009), with some studies supporting a phenomenon of sensitisation arising from increasing vulnerability of dopamine receptors to continuing MA use (Bramness and Rognli, 2016; Curran et al., 2004). Acutely, symptoms of psychosis can be extremely distressing for the individual and affected others and contribute to significant burden on health services (Arunogiri et al., 2015; McKetin et al., 2017).
The term methamphetamine-associated psychosis (or MAP) has been proposed to refer to the spectrum of psychotic symptoms that can occur in MA users (Mathias et al., 2008). This can range from transient intoxication states to longer-lasting substance-induced psychotic disorders or more persistent syndromes that resemble schizophrenia (Bramness and Rognli, 2016). Japanese authors have also described a phenomenon known as ‘flashbacks’ where abstinent ex-MA users experience a recurrence of psychoses in the absence of the drug (Yui et al., 2002). Studies have suggested that the prevalence of MAP in cohorts of illicit MA users varies between 15% and 23% in recreational or community settings to up to 60% in dependent users in treatment settings (Arunogiri et al., 2017; Chen et al., 2003; Ding et al., 2014; Hides et al., 2015; Lapworth et al., 2009; McKetin et al., 2010, 2013). Variability in the prevalence of psychosis symptoms may relate to MA doses and patterns of use, but this does not appear to fully account for the phenomenon – there are subsets of individuals who do not appear to develop psychotic symptoms with frequent MA use, and conversely, some who experience chronic psychosis following limited exposure to the drug (Akiyama et al., 2011; Salo et al., 2013). Taken together, these findings suggest the need to look for potential correlates of psychosis beyond MA use.
The concurrent use of alcohol or other drugs, co-morbid psychiatric disorders and family history have all been examined for associations with psychosis risk (Bramness and Rognli, 2016). However, there remains uncertainty related to these associations due to individual study limitations – such as small or poorly representative samples or inadequate control for confounding factors. Many studies have compared individuals using MA who develop psychosis against healthy controls rather than other MA users. There is great variability in the measurement of psychosis, with some studies reporting diagnoses of psychotic disorders and others measuring symptoms of psychosis. In addition, some studies have not sufficiently accounted for or excluded individuals with primary psychotic disorders. Although there have been three previous narrative reviews focussing on factors associated with MA psychosis (Bramness et al., 2012; Glasner-Edwards and Mooney, 2014; Rognli and Bramness, 2015), these have not utilised systematic methodology and have not attempted to evaluate the quality of studies or potential sources of bias.
As such, we aimed to conduct a systematic review of the existing literature in order to provide higher quality evidence on correlates of MAP. Developing a greater understanding of the factors associated with psychosis in individuals using MA assists in building a profile of high-risk individuals, allowing better targeting of clinical approaches within acute mental health and addiction settings.
Method
A systematic review of studies measuring psychosis symptoms in adults using illicit MA was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Details of the systematic review protocol were registered on PROSPERO International Prospective Register of Systematic Reviews (Registration: 42016052223) prior to data extraction.
Studies were included if they met the following criteria: (1) participants were adult (>17 years) humans with current use (within the last 12 months) of illicit MA or amphetamine (MA); (2) participants using MA with current or lifetime psychosis symptoms (referred to as MAP) were compared with those using MA without psychosis symptoms (MNP), where psychosis was measured using a validated instrument or structured interview and (3) individuals identifying MA as their primary drug were identified and analysed separately from those citing other substances as their primary drug.
Electronic searches were performed on the following databases: MEDLINE (OVID), PsycINFO and EMBASE databases, from the earliest available dates to 8 December 2016. The search strategy combined three concepts: MA or amphetamine, psychosis and risk factors. Search terms for MA included METHAMPHETAMINE, AMPHETAMINE, METHYL-AMPHETAMINE, METHAMPHETAMINE and METHAMFETAMINE; search terms for psychosis included DRUG-INDUCED PSYCHOSIS, SUBSTANCE-INDUCED PSYCHOSIS, PSYCHOSIS, PSYCHOSES, SCHIZOPHRENIA and SCHIZO-AFFECTIVE and search terms for risk factors included RISK FACTORS, VULNERABILITY FACTORS and PREDISPOSING FACTORS (see Appendix 1 for Medline search strategy). In databases where Medical Subject Headings (MeSH) terms were available, they were exploded and combined. No language restrictions were applied to the search.
The reference lists of previous reviews (Bramness et al., 2012; Bramness and Rognli, 2016) and articles identified in the main search were also screened for citations not identified in the main search. As this supplementary search identified five further citations, we elected to perform an additional search using Google Scholar to identify articles that had cited those articles identified in the main search in an effort to avoid missing any potentially relevant articles. The review protocol was updated to reflect this further search. Screening of titles, abstracts and subsequently full texts was performed independently by two authors (S.A. and J.A.F.). Any disagreements regarding study inclusion were resolved by discussion.
Study design and data extraction
Single-case reports, literature reviews and studies in animals were excluded. The following data were extracted from studies: study country, setting and design; participant demographic and clinical details; sample size; measure/s used and measures of association between risk factors and psychosis outcomes. Studies were categorised based on whether psychosis was assessed using a current or lifetime measure. Risk factors were classified according to the following categories: (1) sociodemographic factors (including age, gender, employment, educational status, housing status and socioeconomic status); (2) MA use patterns (including measures of MA use, amount, frequency, duration of use, age of onset of use and route of use); (3) other drug use; (4) psychiatric co-morbidity (including current and previous psychiatric illness and personality disorders); (5) family history (of psychotic or other psychiatric illness) and (6) history of trauma.
An electronic data extraction tool was piloted on one study, refined and subsequently used by two authors (S.A. and J.A.F.) to independently extract data from each included study. Multiple studies conducted on the same population were combined, and data were then extracted together as one study. Where there were uncertainties about the data in studies, or where MA-specific outcomes were not reported, we contacted authors for further clarification and re-analysis of original data.
Quality assessment
As there is no accepted gold standard instrument for assessing quality of observational studies, a modified version of the Newcastle–Ottawa Scale (Wells et al., 2011) was developed specifically for use in this review. The studies were scored on the following domains: (1) representativeness of the cohort (out of 3), (2) assessment of risk factor (out of 3), (3) demonstration that psychosis was not present at the start of the study (out of 2), (4) comparability of the two groups and controls for confounding (out of 2) and (5) assessment of the outcome of psychosis (out of 3), with a final quality score out of 13. S.A. and J.A.F. independently assessed the quality of included studies, with final scores derived by consensus between those two authors. Based on evidence across studies, outcome-level quality for each predictor was assessed by consensus between two authors with reference to the GRADE criteria, considering study design, study quality, consistency and directness for each predictor (Atkins et al., 2004). Inconsistency in evidence was determined by consideration of qualitative study heterogeneity, variation in effect sizes, study populations and outcome definition with reference to the Cochrane guidelines (Schunemann and Santesso, 2011).
Study synthesis
Meta-analysis was planned for correlates reported consistently across three or more studies, where heterogeneity was acceptable. However, lack of consistency in reporting prevented meta-analysis for any correlates, therefore synthesis of results was by narrative review.
Results
Study characteristics
A total of 20 papers met the inclusion criteria, which were based on studies in 13 different sample populations and a total of 5476 individuals (Figure 1). The main reasons for excluding studies were ineligible study design (e.g. case report or literature review), a lack of comparison between MAP and MNP groups and a mixed substance-using population where there was no data available specific to primary MA users.
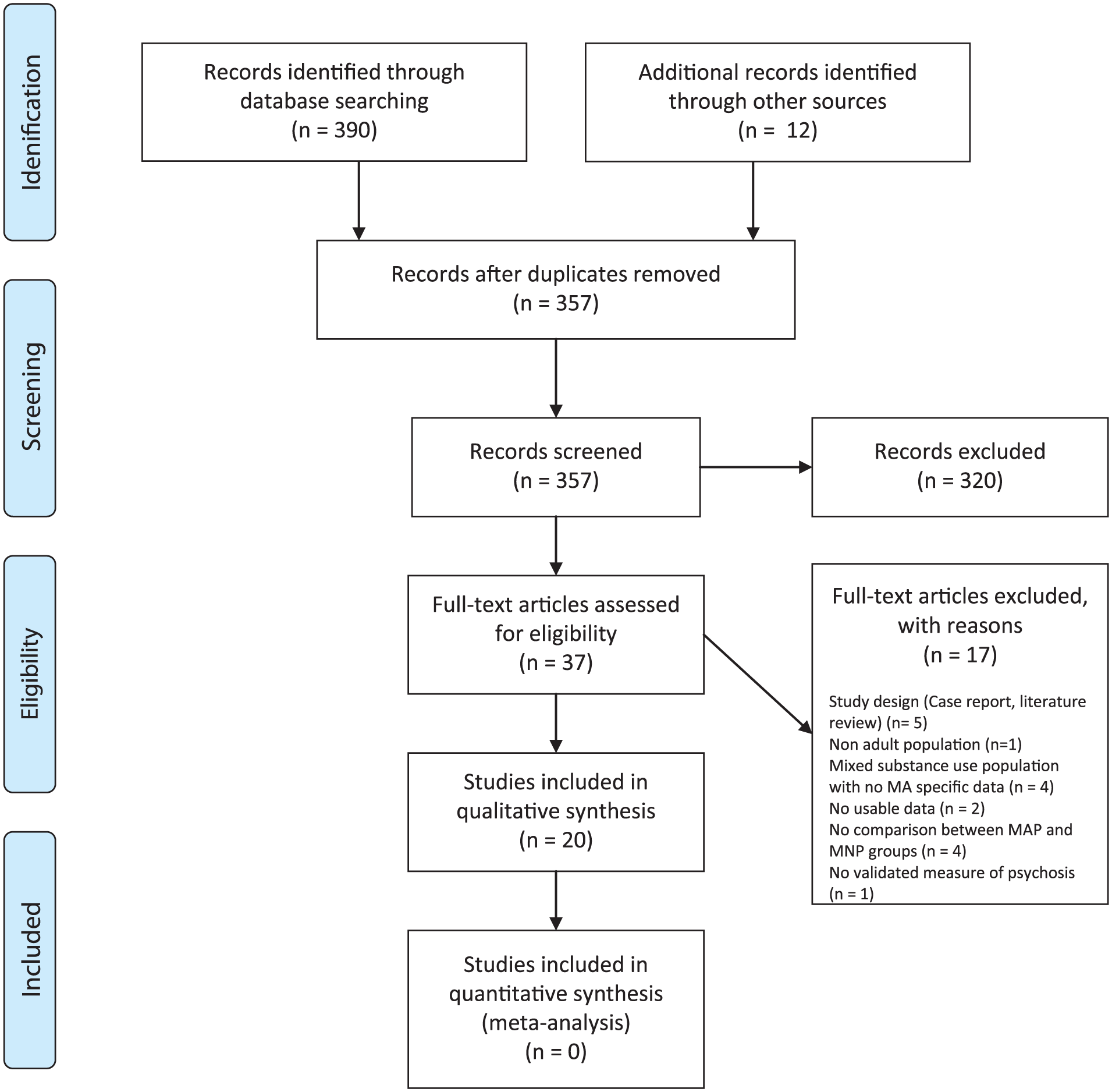
PRISMA flow diagram.
The characteristics of the 13 studies are summarised in Table 1. Four studies were conducted in Asia (China, Taiwan, Thailand and Malaysia), five in Australia, three in the United States and one in Sweden. There was a great deal of variability in the method used to define and assess psychosis. Less than half the studies assessed current symptoms of psychosis (Studies 1–4) or a psychotic disorder (Study 5), compared to a lifetime disorder (Studies 6–10) or symptoms (Studies 11–13).
Characteristics of included studies.
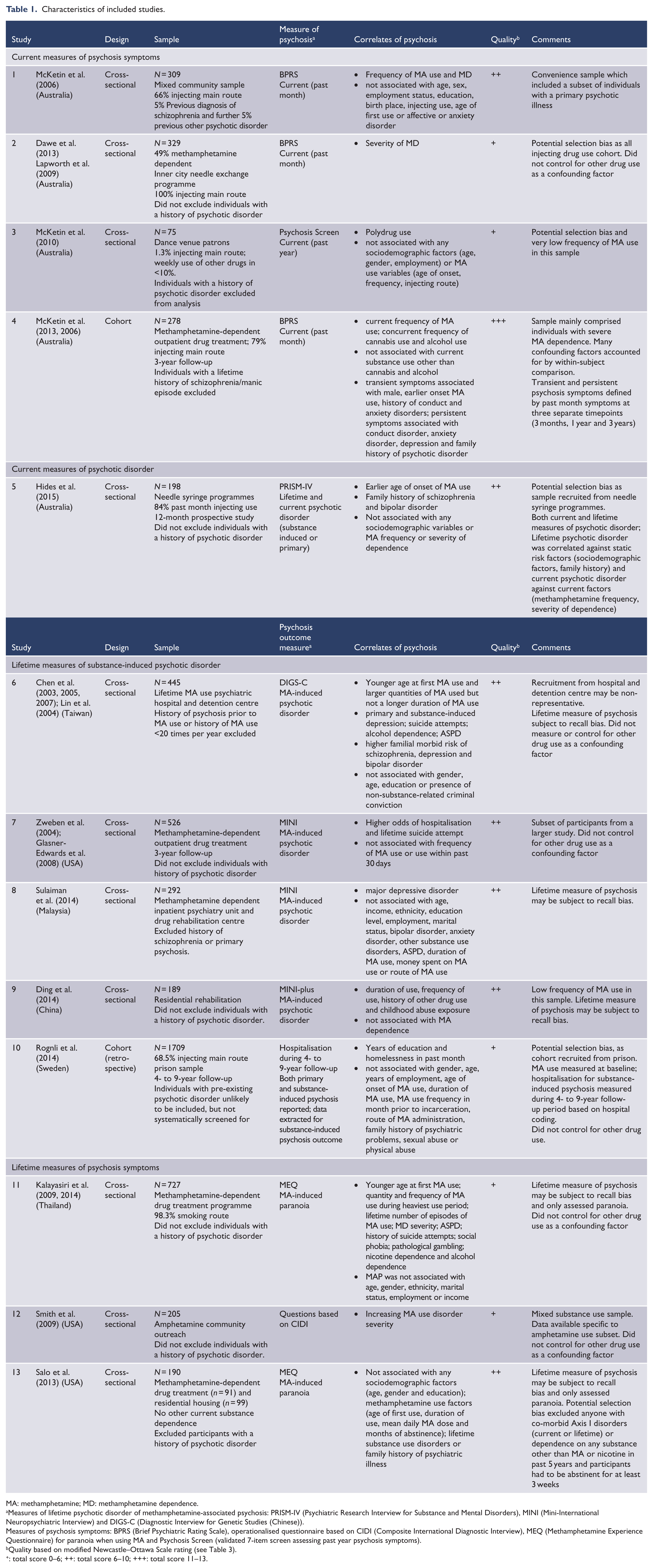
MA: methamphetamine; MD: methamphetamine dependence.
Measures of lifetime psychotic disorder of methamphetamine-associated psychosis: PRISM-IV (Psychiatric Research Interview for Substance and Mental Disorders), MINI (Mini-International Neuropsychiatric Interview) and DIGS-C (Diagnostic Interview for Genetic Studies (Chinese)).
Measures of psychosis symptoms: BPRS (Brief Psychiatric Rating Scale), operationalised questionnaire based on CIDI (Composite International Diagnostic Interview), MEQ (Methamphetamine Experience Questionnaire) for paranoia when using MA and Psychosis Screen (validated 7-item screen assessing past year psychosis symptoms).
Quality based on modified Newcastle–Ottawa Scale rating (see Table 3).
: total score 0–6; ++: total score 6–10; +++: total score 11–13.
Risk of bias within studies
Individual study quality varied considerably with the total quality ratings ranging from 5 to 12 (mean quality score = 7.85, standard deviation [SD] = 2.08; see Table 3 – Online Appendix). The most common reasons for lower quality were the lack of exclusion of a pre-existing psychotic disorder among participants and insufficient control for confounding factors such as other drug use (Figure 2).
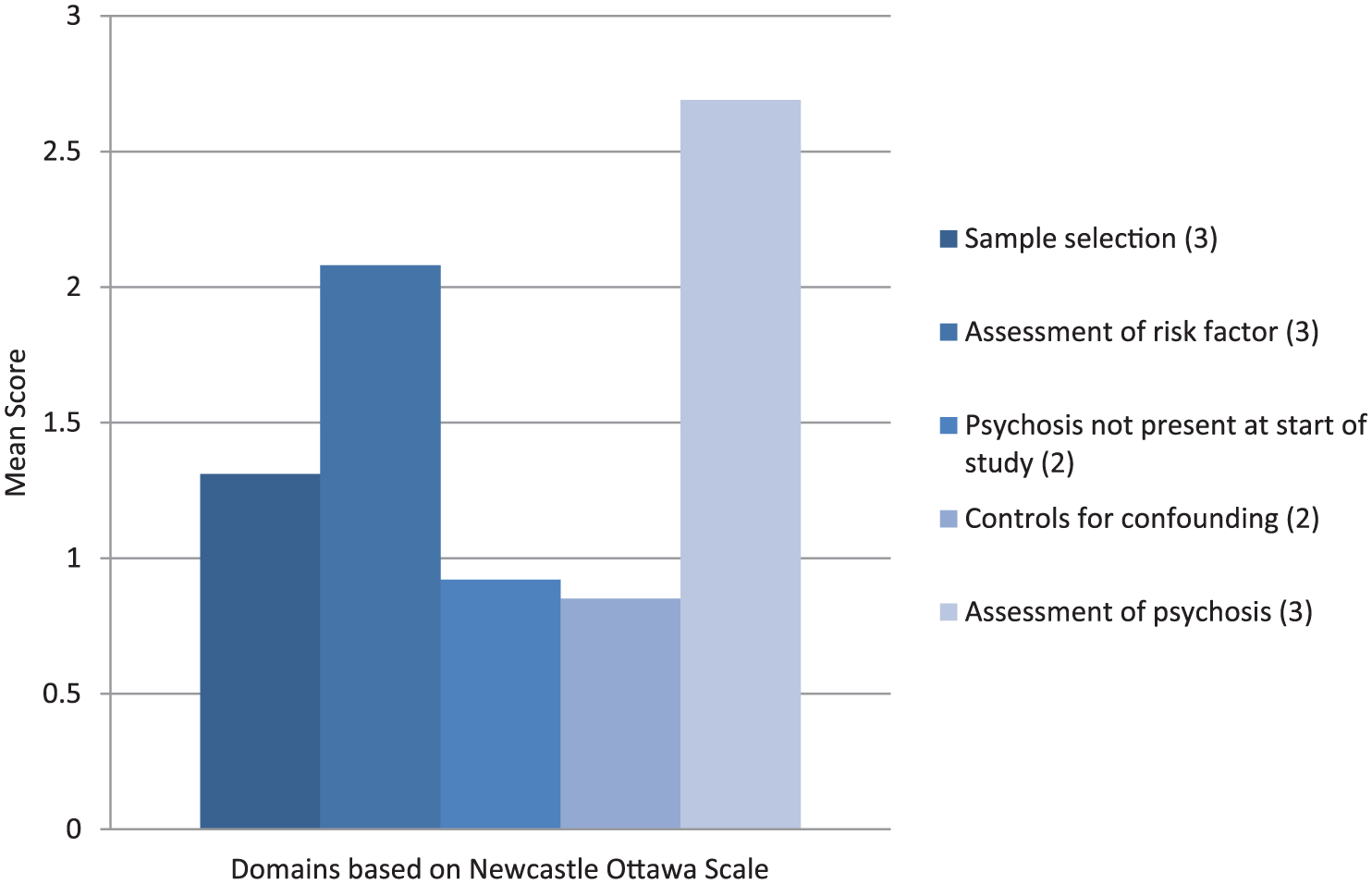
Risk of bias within studies.
Results of individual studies-correlates of MAP
Results of individual studies are presented in Table 2. The included studies compared individuals using MA with and without psychosis on the following factors.
Summary of findings.
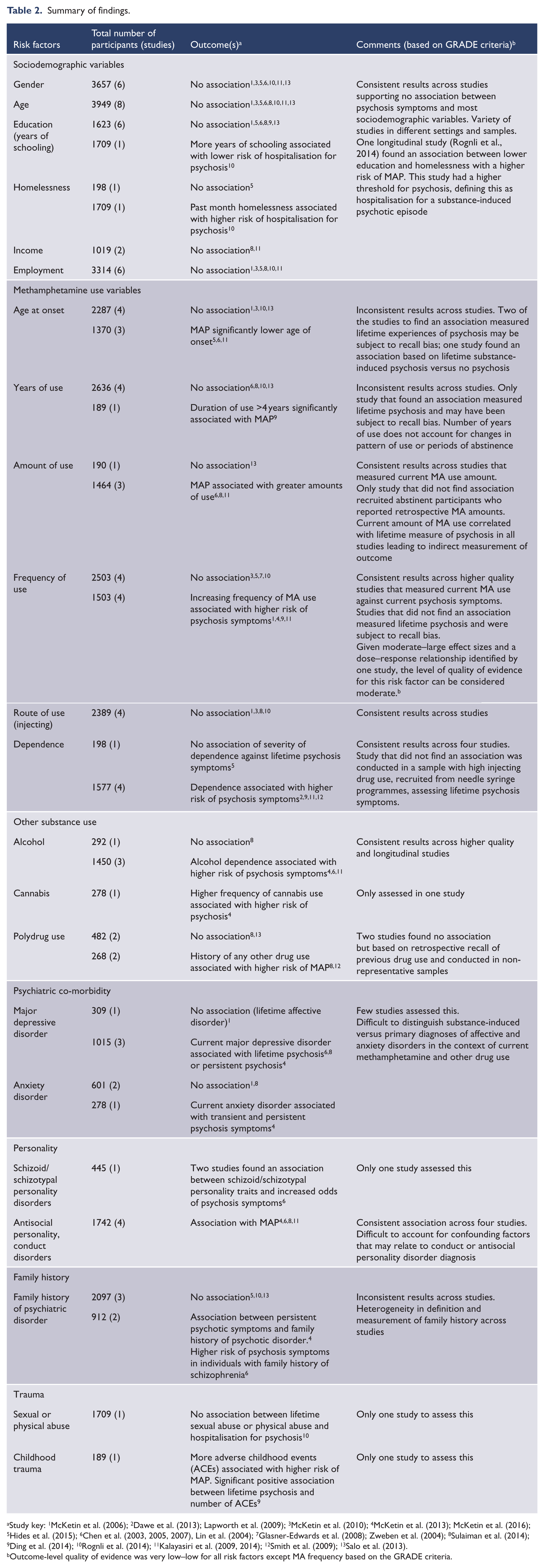
Study key: 1McKetin et al. (2006); 2Dawe et al. (2013); Lapworth et al. (2009); 3McKetin et al. (2010); 4McKetin et al. (2013); McKetin et al. (2016); 5Hides et al. (2015); 6Chen et al. (2003, 2005, 2007), Lin et al. (2004); 7Glasner-Edwards et al. (2008); Zweben et al. (2004); 8Sulaiman et al. (2014); 9Ding et al. (2014); 10Rognli et al. (2014); 11Kalayasiri et al. (2009, 2014); 12Smith et al. (2009); 13Salo et al. (2013).
Outcome-level quality of evidence was very low–low for all risk factors except MA frequency based on the GRADE criteria.
Sociodemographic factors
Age, gender or employment status were not associated with MAP in any study. One study found that fewer years of schooling (OR = 0.8, 95% confidence interval [CI] = [0.7, 1.0]) and homelessness in the past month (OR = 2.5, 95% CI = [1.1, 5.3]) were significant predictors of hospitalisation for substance-induced psychosis (Rognli et al., 2014). Six other studies did not find any association between years of education and psychosis risk (Chen et al., 2003; 2005, 2007; Ding et al., 2014; Hides et al., 2015; Lin et al., 2004; McKetin et al., 2006; Salo et al., 2013; Sulaiman et al., 2014).
Patterns of MA use
Nine studies found associations between MA-related factors (dose – amount or frequency; duration – age of onset or years of use; severity of dependence or route of use) and MAP risk, and the remaining four (Glasner-Edwards et al., 2008; McKetin et al., 2010; Rognli et al., 2014; Salo et al., 2013) reported no association (Table 2).
Three of the studies that did not find an association reported psychosis outcomes based on lifetime symptoms (Salo et al., 2013), substance-induced disorders (Glasner-Edwards and Mooney, 2014) or hospitalisation (Rognli et al., 2014). The fourth study was conducted in a sample with very low frequency of MA use, with only 12% of participants reporting weekly or more frequent use (McKetin et al., 2010). In general, the studies that did not find an association were of lower quality and were vulnerable to selection and recall bias (Tables 1 and 2).
Duration – age of onset or number of years of MA use
There was inconsistent evidence for both age of onset of MA use and number of years of use. The majority of the studies that found an association between these factors and psychosis used lifetime measures of psychotic disorder (Chen et al., 2003; Ding et al., 2014) or symptoms (Kalayasiri et al., 2009). These studies were also mainly conducted in Eastern Asian populations(Chen et al., 2003; Ding et al., 2014; Kalayasiri et al., 2009), suggesting there may be cross-national variation in the association between duration of MA use and risk of psychosis.
Dose-amount and frequency of MA use
More frequent MA use was associated with a higher risk of psychosis in four studies (Ding et al., 2014; Kalayasiri et al., 2009; McKetin et al., 2006, 2013), the majority of which reported an outcome of current or lifetime psychosis symptoms. Conversely, four of the studies did not find this association (Glasner-Edwards et al., 2008; Hides et al., 2015; McKetin et al., 2010; Rognli et al., 2014) and three reported outcomes of lifetime substance–induced psychotic disorder. In general, the studies that found an association between MA frequency and MAP were of higher quality (Table 3 – Online Appendix) (Chen et al., 2003; 2005, 2007; Ding et al., 2014; Kalayasiri et al., 2009, 2014; Lin et al., 2004; McKetin et al., 2006, 2013, 2016; Sulaiman et al., 2014). Based on the results of these four studies, individuals using MA more frequently were estimated to have between 3 and 11 times greater odds of MAP compared to individuals with less frequent use (Ding et al., 2014; Kalayasiri et al., 2009; McKetin et al., 2006, 2013). One longitudinal study comprehensively controlled for a range of confounding factors including other drug use and demonstrated a within-subject dose-related relationship between MA dose (days of use) and concurrent risk of psychotic symptoms (McKetin et al., 2013). In this study, individuals using 16 or more days per month had significantly elevated odds of MAP compared to those using less than 16 days (OR = 11.2, 95% CI = [5.9, 21.1]) (McKetin et al., 2013). In terms of amount of MA use, three of the four studies that examined this predictor found that greater amounts of MA use correlated with a greater likelihood of a lifetime substance-induced psychotic disorder (Chen et al., 2003; Sulaiman et al., 2014) or symptoms (Kalayasiri et al., 2009).
Severity of MA dependence
There was also an association between increasing severity of MA dependence (as defined by Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV] symptom count or by a validated tool such as the severity of dependence scale [SDS] and MAP symptoms across four studies [Ding et al., 2014; Kalayasiri et al., 2009; Lapworth et al., 2009; Smith et al., 2009]). In comparison to non-dependent individuals, MA-dependent individuals were estimated to have between 2 and 3 times greater odds of developing MAP (Ding et al., 2014; Kalayasiri et al., 2009, 2014). One study did not find this association, but this was conducted in a sample recruited from needle syringe programmes with high injecting drug use, which may not have been comparable to other populations (Hides et al., 2015).
Route of MA use
Only four included studies examined the relationship between route of administration and MAP (McKetin et al., 2006, 2010; Rognli et al., 2014; Sulaiman et al., 2014). All of these studies did not find any association between injecting route of use and MAP. One study had a very low rate of injecting use in a recreational drug use sample (McKetin et al., 2010). Two of the studies reported outcomes of current psychotic symptoms (McKetin et al., 2006, 2010), one reported lifetime substance-induced psychotic disorder (Sulaiman et al., 2014) and one reported hospitalisation for substance-induced psychotic disorder (Rognli et al., 2014).
Other drug use
Use of alcohol and other non-stimulant drugs was associated with an increased risk of MAP in five studies (Chen et al., 2003; Kalayasiri et al., 2009; McKetin et al., 2013; Smith et al., 2009; Sulaiman et al., 2014). In particular, co-morbid alcohol and cannabis use or dependence were associated with MAP in three studies (Chen et al., 2003; Kalayasiri et al., 2009; McKetin et al., 2013). One study did not find an association between alcohol dependence and MAP, but had a sample recruited from inpatient psychiatric and rehabilitation settings in a Muslim country, where disclosure of alcohol use may have been less socially acceptable compared to other settings (Sulaiman et al., 2014). There were inconsistent results on the association between a lifetime history of other drug use and MAP.
Psychiatric co-morbidity
Four studies assessed co-morbid affective and anxiety disorders and reported inconsistent results in terms of their association with psychosis (Chen et al., 2003; McKetin et al., 2006, 2016; Sulaiman et al., 2014). These studies did not distinguish between primary or secondary psychiatric co-morbidity in the context of active substance use.
Personality factors
One study suggested a higher incidence of premorbid schizoid or schizotypal personality traits in individuals with MAP (Chen et al., 2003). Four studies supported an association between the prevalence of current diagnoses of antisocial personality disorder or a history of conduct disorder and MAP (Chen et al., 2003; Kalayasiri et al., 2009; McKetin et al., 2016; Sulaiman et al., 2014).
Family history of psychosis or psychiatric illness
Family history was assessed in five studies (Chen et al., 2005; Hides et al., 2015; McKetin et al., 2016; Rognli et al., 2014; Salo et al., 2013). Among these, three found no significant association between family history of psychiatric illness and MAP (Hides et al., 2015; Rognli et al., 2014; Salo et al., 2013). One study that utilised a validated assessment tool, with collateral history from a family member, found that those with a family history of schizophrenia were five times more likely to have a lifetime history of substance-induced psychotic disorder (OR 5.4, 95% CI = [2.0, 14.7], p < 0.001; Chen et al., 2003). One further study suggested an association between persistent (but not transient) current psychosis symptoms and a family history of psychotic illness (McKetin et al., 2016).
Trauma
Only one study examined the predictor of lifetime history of sexual or physical abuse and did not find any association between this and MAP (Rognli et al., 2014). One study examined the prevalence of adverse childhood experiences (ACEs) on the development of MAP and found that individuals with three or more adverse childhood experiences had a significantly higher risk of lifetime MAP (OR = 4.5, 95% CI = [1.6, 12.6]; Ding et al., 2014). This study also found a graded relationship between the number of ACEs and psychosis that remained significant after controlling for sociodemographic variables, duration and frequency of drug use and dependence and other drug use (Ding et al., 2014).
Risk of bias across studies
The quality of the evidence for each predictor as a correlate of MAP was synthesised across studies using the GRADE approach (Atkins et al., 2004; Guyatt et al., 2008) and was found to be low–very low across almost all predictors as a result of an observational study design; unexplained heterogeneity; inconsistency of evidence across studies and multiple sources of bias (Table 2). The only outcome for which there was a moderate level of evidence was frequency of MA use, with evidence of moderate–large effect sizes (Ding et al., 2014; Kalayasiri et al., 2009, 2014; McKetin et al., 2006, 2013) and a dose–response relationship between MA frequency and odds of psychosis symptoms (McKetin et al., 2013).
Discussion
This is the first comprehensive review to examine correlates of psychosis among people who use illicit MA. We found moderate evidence that more frequent MA use was associated with a dose-related increase in the likelihood of psychotic symptoms. There was also consistent evidence that other indices of MA use (quantity of MA use and greater severity of MA dependence) were associated with greater odds of psychotic symptoms. The frequency of use and severity of dependence have been shown to be highly correlated in amphetamine use populations (Gossop et al., 1995), and so, taken together, this adds to the concept that greater use of the drug results in a greater likelihood of psychosis. Polydrug use, particularly alcohol dependence and frequent cannabis use, was also associated with MAP. Sociodemographic factors, such as age, gender and employment status, were not associated with psychosis risk among people who use MA.
Strengths and limitations of this review
This review represents the most comprehensive, rigorous and up-to-date perspective on the evidence for correlates of MAP. The use of a priori criteria, systematic searching (in any language) and independent quality assessments by two co-authors are key strengths of this study, in comparison to previous reviews (Bramness et al., 2012; Bramness and Rognli, 2016). Methodological limitations, however, include the lack of validation of the adapted version of the Newcastle–Ottawa Scale (Wells et al., 2011) used to assess individual study quality and the inability to pool results due to both statistical and qualitative heterogeneity, with outcome-level quality of evidence assessed qualitatively with reference to the GRADE approach.
A key issue with the literature in this area relates to the variability in measurement of psychosis. The search strategy for this review was intentionally broad in order to capture any relevant studies. However, heterogeneity and inconsistency in the measures used to assess the outcome of psychosis prevented any meta-analysis in this review. Less than half of the studies included in this review measured current psychosis symptoms against current MA use (Hides et al., 2015; Lapworth et al., 2009; McKetin et al., 2006, 2010, 2013). In comparison, eight other studies (Chen et al., 2003; Ding et al., 2014; Kalayasiri et al., 2009; Rognli et al., 2014; Salo et al., 2013; Smith et al., 2009; Sulaiman et al., 2014; Zweben et al., 2004) reported lifetime MA–induced psychotic disorders or symptoms as their primary outcome measure and related this to MA use at the time of the study, such that MA use may have occurred at a different time from psychosis outcomes. A further issue arises from the difference in measuring psychotic symptoms versus a disorder and speaks to the inherent difficulties in comparing outcomes based on dimensional, categorical or clinical measures of a syndrome. This is paralleled by a shift in the recent conceptualisation of psychosis, from categorical clinical diagnoses to a more transdiagnostic approach, reflecting a range of symptoms that may relate to different trajectories and disorders (Lappin et al., 2016). In this context, broader definitions of psychoses, such as those used in some of the included studies (Lapworth et al., 2009; McKetin et al., 2006, 2010; 2013), do have the advantage of capturing the full spectrum of psychotic symptoms, even if this does not equate to a clinical diagnosis.
A further limitation of this review relates to its reliance on observational studies, most of which were cross-sectional, and therefore clearly limited in terms of ability to test causal relationships and predictive associations. This is a common problem in dual-diagnosis research, particularly when studying early-onset progressive disorders such as chronic psychotic illness, where it can be difficult to identify whether drug exposure or other risk factors predate the onset of the illness and to account for a range of potential measured and unmeasured confounding (Kendler, 2017). On one hand, there is evidence that MA can trigger psychosis in experimental settings (Angrist and Gershon, 1970; Bell, 1973), and psychosis is a recognised adverse effect of psychostimulant medication for treatment of attention deficit hyperactivity disorder (Ross, 2006). However, this evidence does not translate directly to the use of illicit MA in non-experimental settings, as other factors (for instance, related to the drug, the individual or the environment) may moderate this relationship. A further factor to consider when examining evidence from observational studies is whether the outcome of interest was present in the cohort at baseline – seven of the included studies failed to exclude individuals with primary psychotic disorders from their samples (Dawe et al., 2013; Ding et al., 2014; Kalayasiri et al., 2009, 2014; Lapworth et al., 2009; Rognli et al., 2014; Smith et al., 2009). Thus, while the frequency and amount of MA use and severity of dependence were shown to be consistently associated with psychotic symptoms, the literature presented in this review is insufficient to support a causal association.
Many of the included studies were conducted in mixed substance-using populations. In this review, we chose to include any studies that specifically reported outcomes for individuals citing MA or amphetamine as their primary drug of concern. This definition included populations that were purposively recruited on the basis of MA use, as well as mixed use populations where results were specifically presented for individuals nominating MA as their drug of choice. This is a typical approach in the substance use literature, given that poly-drug use is the norm rather than the exception in most illicit drug use populations, but this does give rise to confounding related to poly-drug use and to the differences in lifestyle and psychosocial circumstances that may accompany poly-drug use patterns. This is particularly salient when studying the phenomenon of psychosis, with clear evidence that a range of other drugs have the potential to precipitate or perpetuate psychosis, such as other stimulants or cannabis (Murray et al., 2013). Only six of the included studies in this review reported adjusted outcomes that controlled for this confounding factor, and this remains a significant limitation of the existing evidence in this area (Ding et al., 2014; McKetin et al., 2006, 2010, 2013, 2016; Sulaiman et al., 2014).
MA-associated psychosis has been proposed by some authors as a potential model for schizophrenia (Bousman et al., 2011; Hermens et al., 2009; Yui et al., 2000); the two disorders have very similar acute clinical syndromes, and studies suggest that up to 30% of individuals with a history of MAP have been found to transition to persistent psychotic illness in longitudinal studies (Niemi-Pynttäri et al., 2013). If this is valid, and MAP is part of the same phenomenon as primary psychotic disorders such as schizophrenia, it is conceivable that established risk factors for schizophrenia can be expected to also raise the risk of psychosis in MA users. However, there is insufficient evidence to support this at present. Putative risk factors for schizophrenia (Tsuang et al., 2001; Van Os et al., 2010) including genes and environmental factors (Tsuang et al., 2001; Van Os et al., 2010) such as maternal nutrition (Brown and Susser, 2002), paternal age (Malaspina et al., 2001), migration (Cantor-Graae and Selten, 2005), urbanicity or childhood adversity and trauma (Matheson et al., 2013) have not yet been shown to be relevant in the aetiology of MAP. Therefore, the extent to which the aetiological pathways of MAP and schizophrenia overlap remains unclear.
Implications for future research
The main limitation of existing research arises from the heterogeneity in study designs, study populations and the measures used for psychosis. Future studies examining this question should aim to exclude individuals with primary psychotic illness at baseline and should involve validated and contemporaneous assessment of MA and other substance use with measures of psychosis, such as the Timeline Followback method (Sobell and Sobell, 1992). Analysis in studies should, at a minimum, seek to measure and control for confounding factors such as other drug use.
In order to strengthen our understanding of the risk factors for psychosis among people who use MA, more data are needed on factors that have only been studied previously a small number of studies, including family history of psychotic disorders or a history of childhood stress or trauma. Similarly, no studies have investigated protective factors in MA psychosis. It is unclear what role familial support or social capital may play in increasing the resilience of an individual using MA.
Existing research has also frequently been based on restricted sample populations such as injecting drug users or in drug rehabilitation or incarceration settings. These settings may not be truly representative of adults who use illicit MAs, and future studies should seek to recruit both individuals from community and treatment seeking settings with a wide range of MA use histories and trajectories. Finally, while we included a number of longitudinal studies in our review, we did not specifically focus on factors related to the transition to chronic psychotic disorders. This is a key question that could potentially be answered by future reviews.
Implications for clinicians
The results of this review suggest that MA-related factors, such as frequency and quantity of use and severity of MA dependence, have the most consistent evidence as correlates of MAP. This highlights the need for clinicians to specifically obtain a detailed history of recent MA use amounts and patterns of use from individuals in both mental health and substance use treatment settings; while this may seem obvious, this point is worth labouring, as accurate assessment may be hampered by some mental health clinicians’ lack of confidence or training in assessing co-existing substance use disorders (De Crespigny et al., 2015). Similarly, harm-reduction messages targeted at this population should emphasise the association between MA use patterns and psychosis and should be aimed at helping non-treatment-seeking individuals minimise their risk of developing this significant adverse effect.
Based on the results of this review, individuals with high dose use of MA should be recognised as a high-risk group for psychosis. The case for an early intervention approach is particularly salient for MA-using individuals, as efforts made to engage them in treatment earlier in their use trajectory may prevent progression to chronic and disabling illness (Lappin et al., 2016). Such individuals presenting either to mental health or alcohol and other drug clinical services may warrant higher intensity, targeted approaches to minimise the risk of psychosis. This has implications for service delivery, necessitating a better resourced, integrated and longer term dual-diagnosis model of care in order to adequately address the needs and risks of this population (Lappin et al., 2016).
Conclusion
Among MA users without a primary psychotic disorder, the most consistent predictors of psychotic symptoms are frequency and quantity of MA use and the presence of dependence features. Further research is required to conclusively determine whether other factors, such as trauma, family history of psychotic illness and other substance use are predictive of MA-associated psychosis. The findings of this review highlight the need for targeted assessment and treatment of MA use in individuals presenting with psychosis.
Footnotes
Declaration of Conflicting Interests
Dan Lubman has provided consultancy advice to Lundbeck and Indivior and has received travel support and speaker honoraria from Astra Zeneca, Bristol Myers Squibb, Janssen, Lundbeck and Servier.
Funding
This research was supported by the Australian National Health and Medical Research Council (NHMRC) postgraduate scholarship (Grant 1093778) which provided a stipend to the primary author during PhD candidature.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.