
Abstract
Objective:
Research designed to increase knowledge about Māori with bipolar disorder is required to understand how health services support wellbeing and respond to identified levels of community need. This paper synthesises the expert critique of Māori patients with bipolar disorder and their whānau regarding the nuances of cultural competence and safety in clinical encounters with the health system.
Methods:
A qualitative Kaupapa Māori Research methodology was used. A total of 24 semi-structured interviews were completed with Māori patients with bipolar disorder and members of their whānau. Structural, descriptive and pattern coding was completed using an adapted cultural competence framework to organise and analyse the data.
Results:
Three themes were evident from participants’ critique of clinical components of the health system. Theme 1 established that the efficacy of clinical care for bipolar disorder was dependent on Māori patients and whānau having clear pathways through care, and being able to access timely, consistent care from clinically and culturally competent staff. Theme 2 identified the influence of clinical culture in bipolar disorder services, embedded into care settings, expressed by staff, affecting the safety of clinical care for Māori. Theme 3 focused on the need for bipolar disorder services to prioritise clinical work with whānau, equip staff with skills to facilitate engagement and tailor care with resources to enhance whānau as well as patient wellbeing.
Conclusion:
The standard of clinical care for Māori with bipolar disorder in New Zealand does not align with practice guidelines, Māori models of health or clinical frameworks designed to inform treatment and address systemic barriers to equity. Research also needs to explore the role of structural and organisational features of the health system on Māori patient and whānau experiences of care.
Introduction
Research suggests Māori (New Zealand Indigenous peoples) and other Indigenous peoples experience greater bipolar disorder (BD) community prevalence not explained by differences in sociodemographic variables alone (Baxter et al., 2006; Blanco et al., 2017; Grant et al., 2005; Waitoki et al., 2014). Limited research has been designed to increase knowledge about Māori with BD despite international health authorities ostensibly prioritising quality mental health research with Indigenous peoples (Anderson et al., 2016; Black et al., 2017; Haitana et al., 2020b; United Nations, 2016; World Health Organization, 2013).
Indigenous peoples are affected by pervasive health inequities through the ongoing effects of colonisation, in which health and other social systems privilege non-Indigenous ethnic groups (Anderson et al., 2016; Reid et al., 2019; United Nations, 2016). BD research is needed in communities with higher prevalence, because it is a chronic condition that has significant impacts and requires high health system resource (Angst, 2004; Cunningham et al., 2020a, 2020b; Merikangas et al., 2011; Rowland and Marwaha, 2018). BD research with Māori has the potential to inform knowledge about many other serious and chronic mental health conditions affecting Indigenous peoples (United Nations, 2016; World Health Organization, 2013).
Clinician beliefs and behaviours contribute to health inequities, with cultural competence skills and cultural safety interventions required to support clinicians to work effectively with Indigenous and minoritised ethnic groups (Anderson et al., 2016; Betancourt et al., 2003, 2014; Medical Council of New Zealand, 2019; Palmer et al., 2019; Reid et al., 2019; Skelly et al., 2013). Culturally competent and safe clinical practice encompasses reflective practice measures to capture bias and minimise discriminatory care practices, clinican knowledge about socio-cultural differences and cross-cultural communication skills (Betancourt et al., 2003, 2014; Palmer et al., 2019; Reid et al., 2019). Although the importance of cultural competence and safety to achieve health equity is widely reported, few studies describe the nuances of these from the perspective of Indigenous peoples receiving clinical care (Haitana et al., 2020a, 2020b; Palmer et al., 2019).
This paper synthesises the expert critique of Māori patients with BD and their whānau (family/support networks) regarding the nuances of cultural competence and safety in clinical encounters with health services.
Methods
Research approach and paradigm
An Indigenous methodology, Kaupapa Māori Research (KMR) was used to inform this qualitative study and is described in detail elsewhere (Haitana et al., 2020a). Methods chosen aligned with KMR principles to achieve the study aim and identify how systemic factors perpetuated inequitable health outcomes for Māori participants.
Sample and context
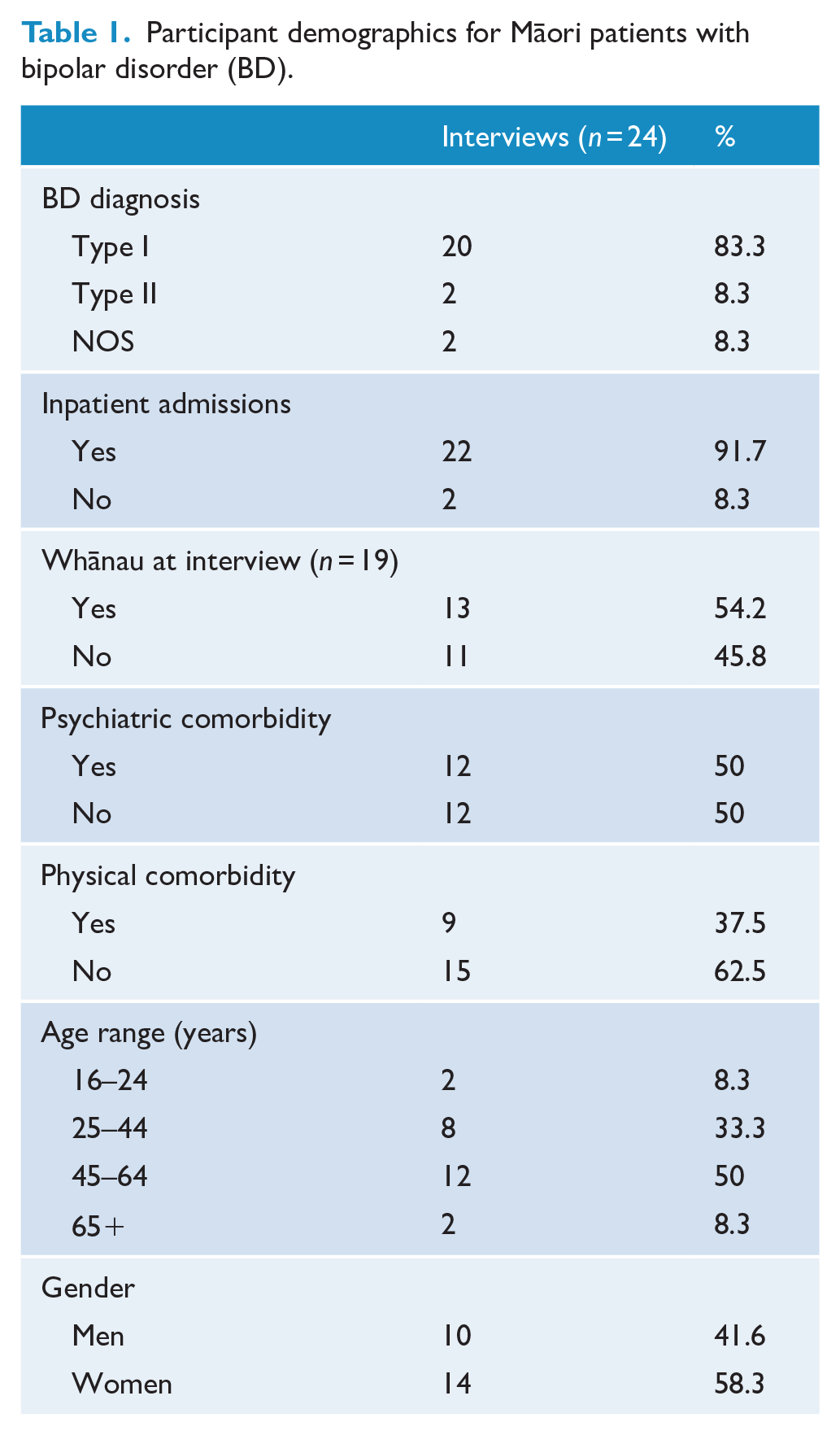
A total of 24 semi-structured interviews were completed across three New Zealand sites selected for their range of mental health services, rural and urban loci. Table 1 summarises self-reported demographic information for Māori patients with BD (n = 24) who participated. Over half of interviews included the perspectives of patients together with one or more whānau (n = 19). All patients had a BD diagnosis with a stable mood at interview. Mental health staff gave study information to eligible patients, and interested participants were then recruited by the research team. No exclusions were made for co-morbidities. A purposive sampling frame recruited men and women of differing ages across sites. Participants provided informed consent in writing before interviews.
Participant demographics for Māori patients with bipolar disorder (BD).
Ethics
Ethical approval was received from the Health and Disability Ethics Committee of New Zealand (ID:16/STH/137). The CONSolIDated critERia for strengthening research involving Indigenous peoples (CONSIDER statement) was utilised to align the study with Indigenous research guidelines and priorities (Haitana et al., 2020a; Huria et al., 2019).
Procedure
Interviews were conducted in-person by two of the research team between December 2017 and August 2019. Venues included participants’ homes, health services or a research unit. The interview schedule was informed by a systematic literature review (Haitana et al., 2020b), and adaptation of a cultural competence framework (Betancourt et al., 2003). Questions explored the impact of clinical interactions on participants’ hauora (wellbeing).
Data collection and processing
Interviews were recorded, transcribed and analysed by the research team. Transcripts were anonymised assigning a number to each interview (1–24) with a corresponding number given to participants (P1–P24) and their whānau (W1–W24). Where multiple whānau were present at one interview, an interview number and letter was assigned to whānau members (W1a, W1b, W1c). NVivo12 data management software was used to display transcripts, code data and refine codes, categories and themes and monitor saturation across themes and sub-themes.
Data analysis
Two cycles of coding were completed (Saldaña, 2016). The first cycle involved two phases. Phase 1 used structural coding. This involved applying a cultural competence framework adapted to the New Zealand context to group data according to whether it involved participants’ critique of clinical, structural and/or organisational components of the health system (Betancourt et al., 2003). The Betancourt framework defined the ‘clinical’ component of health systems as interactions between health care providers, patients and their families (Betancourt et al., 2003). Based on the coding process, the criteria for inclusion widened to incorporate interactions between Māori patients/whānau and specific staff/health services/providers; barriers or enablers to hauora related to/arising from these clinical interactions; and specific clinical interventions and their contribution to hauora. For this paper, only findings from the ‘clinical’ component of analysis will be presented. Phase 2 employed descriptive coding to highlight topics identified within the clinical code.
Coding cycle 2 used a method called pattern coding where related codes and categories from the first cycle were grouped. Groupings provided breadth and depth to understand the phenomenon being explored forming a theme. This process was repeated until theoretical sufficiency was met, measured by the depth of commentary across all interviews, and the point at which no further codes, categories or themes were identified.
Data display
Findings will be presented by defining each theme, then describing the nuances of related sub-themes including the barriers and enablers to hauora through clinical care. Quotes will be included to elucidate each sub-theme.
Results
Three themes reflected participants’ critique of cultural competency and safety of clinical components of health care services provided to Māori with BD and their whānau. Themes centred on clinical care, clinical culture and clinical work with whānau. Figure 1 illustrates these.
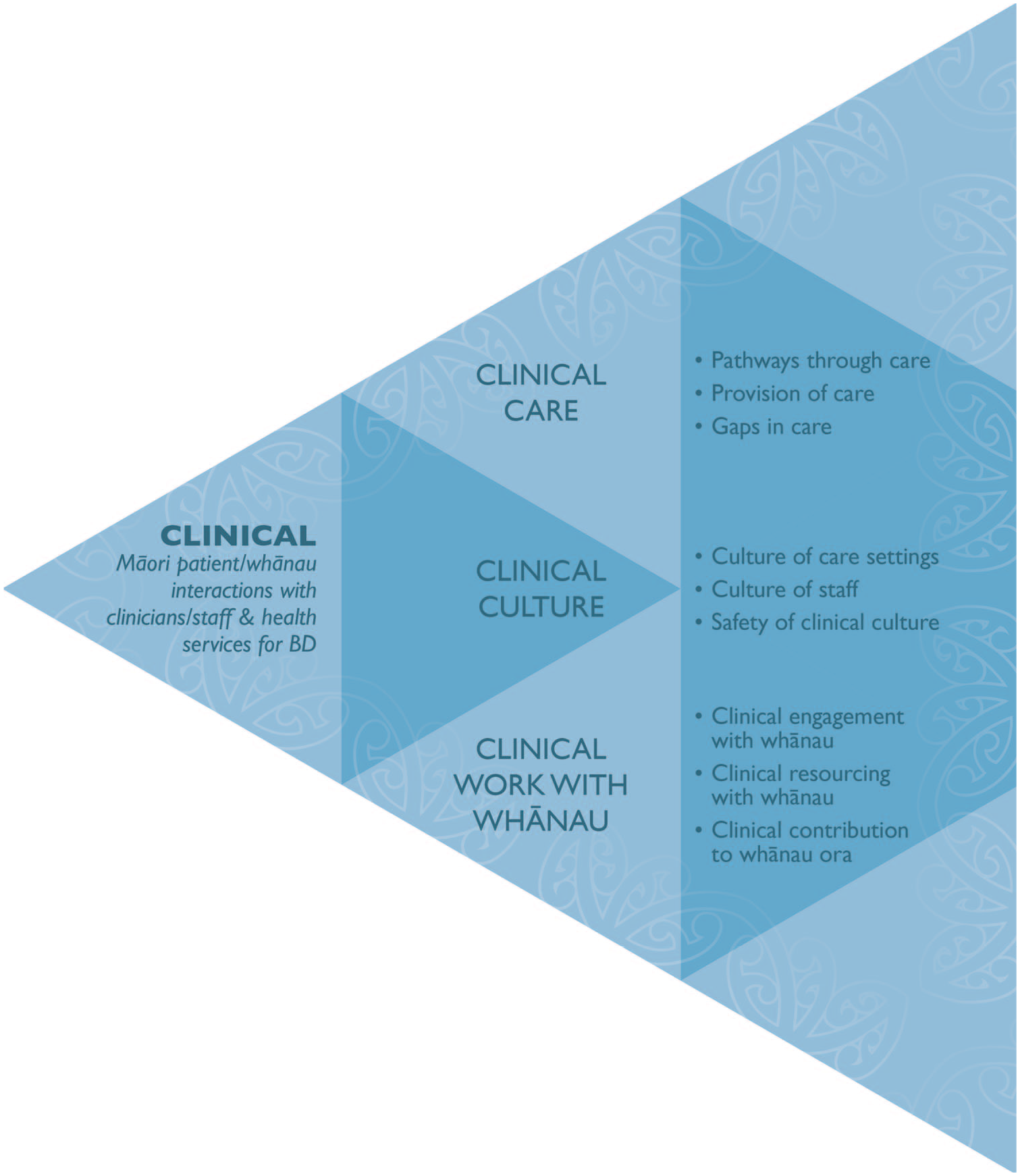
Themes and sub-themes from critique of clinical components of the health system.
Clinical care
This theme included critique about the range, benefits and limits to care provided to Māori patients with BD and whānau by health services. Three sub-themes were involved: pathways through care; provision of care; and gaps in care.
Pathways through care
This sub-theme captured participants’ critique of the number of complex pathways Māori patients and whānau have to learn and navigate to receive clinical care for BD in New Zealand. Participants wanted information about BD to facilitate pathways through care. This required clinicians to increase patient and whānau health literacy about the chronicity and course of BD, explain the types of services and clinicians available to Māori and their role in care, and outline how service contact might vary in response to changing BD symptomatology. Failure to equip participants with information compounded distress and maintained a power imbalance as pathways through care became dependant on the availability and willingness of staff to listen and act on concerns raised.
Pathways through care were obstructed when staff with specialist skills, like psychiatrists, psychologists and hauora Māori (Māori health) practitioners, were absent or unavailable. Participants emphasised the importance of consistently available general practitioners (GPs) for BD, as alternative GP practice models hampered pathways through care contributing to potentially preventable inpatient admissions. Although inpatient care for BD was required infrequently, pathways could be improved if the process or purpose of an admission was clear, whānau were listened to and involved, and all staff were culturally competent and safe minimising the use of violence, restraint and seclusion on Māori in inpatient settings:
By the time we knew what was wrong, she was well and truly unwell, and had to go to a mental health unit. The crisis team weren’t around. We didn’t know what to do. I got my local doctor, who we trusted. But he, like a lot of the professionals didn’t know what to do, and didn’t help. So I learned what to look for. I found it happens really fast, extremely fast. That was the hardest thing to communicate to the professionals. That I knew she was unwell, but they’d wait until she was really bad. (W1)
Provision of care
This sub-theme explored the quality and efficacy of clinical care provided to Māori patients with BD and their whānau. All participants reported having contact with mental health services, some for years, before BD was formally diagnosed. Provision of care for BD therefore necessitated comprehensive assessments, incorporating patient and whānau perspectives, and longitudinal information over more than one interview. Care was considered to be more efficacious when clinicians developed a partnership arriving at a holistic understanding of BD and shared intervention plan. Staff who integrated knowledge about BD, te ao Māori (the Māori world) and their individual Māori patients and whānau were deemed to provide the greatest standard of care.
Medication was described as the mainstay of clinical care in the treatment of BD. While participants generally accepted the role of medications for Māori with BD, effective care required time to review and discuss medications, removal of prohibitive prescription costs and active side effect management. Participants also noted the need for clinical care cognisant of the lifecourse persistence of BD, requiring a tailored approach for Māori men and women with age. This included the need for clinicians to consider that Māori with BD have important roles and responsibilities within their whānau, and that effective care needed to encompass these:
I’m one of those fortunate people I’ve had a lot of help, I’ve had a lot of people who have spent time. When I see tangata whaiora now, and I look at them, they seem so medicated, they’ve had their wairua taken off them. I’ve had the opposite. I’ve had people come in, always at a level which is to support and not to be a nuisance. I’ve had some really good psychiatrists that have given information, they’re kind of an open book. The psychiatrists that sit there with their questions and judgements, they are useless, but the others that are holistic, they are good. (P1)
Gaps in care
The final sub-theme from clinical care identified gaps in health services for BD, and the impact of those on Māori patient and whānau wellbeing. Gaps in care arose when clinicians with relevant skills, like talking therapies, hauora Māori expertise or psychopharmacology, were under resourced, absent or on rotating rosters. Inconsistent care limited the ability of staff to provide timely interventions to influence the course of BD, by altering medication dosage or providing support to mitigate stressors or risk factors. Inconsistency also prevented the development of effective working relationships built on trust, a shared formulation and management plan, affecting decision making for a chronic condition like BD.
Gaps in care also adversely affected hauora when indicators of comorbidity were undetected, physical and mental health conditions were untreated or care was limited to symptom alleviation. This meant that the impact of the social determinants of health were rarely a focus of clinical care for BD, not explored by clinicians or highlighted as important when transitioning Māori patients and whānau to other services. Gaps in care narrowed the focus to Māori patients without considering their roles and relationships with whānau, as clinicians lacked sufficient time, knowledge or skills to work with whānau collaboratively. Gaps caused delays in essential communication at key points of care, and left little scope to incorporate the expertise of Māori patients, whānau and hauora Māori practitioners alongside Westernised psychiatric frameworks:
Over time I think they needed to include my family more. Children need information. I was in the unit and had to plead with the psychiatrist to help my children understand what was going on. They weren’t going to at first. They had the attitude, ‘Oh, children are resilient’. But it’s how people treat them that creates that resilience. You know – because they understand, they can cope with mum’s illness and be supportive. But if they don’t, and you’re mentally ill at the same time and you’re trying to explain it to them it adds pressure. (P2)
Clinical culture
This theme identified the culture embedded within clinical services and expressed by staff and other patients in care settings for Māori with BD and their whānau. This theme encompassed three sub-themes: culture of care settings; culture of staff; and safety of the clinical culture.
Culture of care settings
This sub-theme synthesised critique of established cultural practices and norms in clinical settings, and their influence on care for Māori patients with BD and whānau. The culture of care settings was influenced by clinical and non-clinical staff, features of the care setting and other patients. Culture influenced whether participants felt comfortable, welcome and safe to be Māori and receive health services for BD in that setting. Care settings were valued when Māori tikanga (customs/protocols), kaupapa (focal issues/matters), values and practices were embedded in service culture, and employed flexibly to meet the diverse needs of Māori patients and whānau.
Participants were critical of care settings where the culture was dominated by Westernised approaches, or Māori tikanga, kaupapa, values and practices were applied tokenistically rather than being a core consideration throughout. A critical tenet of an effective culture of care for Māori with BD was defined by the commitment of services and staff to respect and uphold the mana (authority/dignity) of all Māori patients at all stages of their illness. Valuing the importance of Māori spaces within clinical settings, such as providing access to marae (meeting house) or whānau-friendly facilities, also featured strongly as an indicator of a culture of care.
Some participants critiqued culture-blindness in care settings, encountered when services failed to attend to dynamics between Māori patients, whānau and staff with shared whakapapa (geneaological ties) or social networks. Care settings where whakapapa or social connections were not thoughtfully addressed were seen as unsafe by Māori participants and avoided when possible. Where care within unsafe settings was compelled by court order, this was highly aversive to participants, ineffective and harmful. Participants identified that clinical services needed to establish a culture in care settings to support the wellbeing and retention of Māori staff, patients and whānau. This required reflection and discussions about the impact of potential conflicts of interest unique to Māori, and a clinical management approach encompassing clinical and cultural priorities when staff, patients and whānau shared connections:
I’ve had a consistent Māori health worker, she’s been the best. The only consistent person. She would come to anything even if it wasn’t at her service. I went to my outpatient visit with my psychiatrist and Māori health worker and was told: ‘If you don’t walk over to the inpatient service right now you are under the Mental Health Act’. He was forcing me to be admitted without having to put me under the Act and I think it is manipulative to have someone come to an outpatient appointment and not give them a choice, but use language that sounds like they do. It was a complete waste of time. It didn’t work. The services can’t be so separated with one person in between. (P3)
Culture of staff
This sub-theme synthesised critique about the cultural norms sometimes implicitly held and expressed by clinicians and staff, and the impact on care provided to Māori patients and whānau. Participants valued the contribution of cultural diversity among clinicians and staff employed in health services for BD and the choice to work with Māori and non-Māori. However, participants were clear in stating that all staff, regardless of role or ethnicity, needed to be culturally competent to provide effective care in clinical settings.
Key attributes of staff culture contributing to positive experiences for Māori in BD services were also identified. These included effective communication skills, listening, hearing, understanding and relaying key information, often at times of distress, of relevance to Māori patients with BD and whānau. When there were few culturally competent staff, participants noted resistance from teams and additional pressure on those staff to advocate for equity-focused care for Māori. A healthy staff culture, valuing learning, growth and different perspectives, was noted by participants as an antidote to the dominance of Westernised approaches to health care, and an essential component in equity for Māori. This included embracing professional development opportunities to nurture culturally competent and safe practice as it normalised the need for continuous evaluation and service improvements:
It doesn’t matter which service – whether Māori or mainstream, there are always good people in either who go above and beyond what they are called to do. In mental health services what is most important is that staff genuinely care and have empathy. And many of those people aren’t supported by their co-workers or the organisation, they don’t get the credit for the work that they do. The system can be quite brutal to the workers. And I know the system has gone more that way over the years. (P4)
Safety of clinical culture
Safety of clinical culture was the final sub-theme involving critique about the degree of alignment between Māori tikanga, kaupapa, values and practices and the approaches taken to delivering health services for Māori patients with BD and whānau. The safety of clinical culture was measured by how participants felt in services, when with clinicians in that service, or when receiving care. A safe clinical culture supported staff to be conscious and attentive to power imbalances and biases, with flexibility to consider how their approach could mitigate or exacerbate health inequities disadvantaging Māori.
Participants considered a safe clinical culture was measured by the degree to which clinical and cultural competencies were recognised, utilised, valued and integrated into services and expressed in the delivery of care by staff. The provision of equitable health care was also described by participants as an indicator of safety within the clinical culture of services, with participants noting how different approaches could enhance or inhibit the efficacy of care for Māori receiving services for BD. A safe clinical culture required a whole service commitment to quality care for Māori patients and whānau, expressed through the actions of all staff rather than being the sole delegation of Māori:
They welcomed me and my parents, it was always a Māori kaupapa, and a lot of tikanga. They used to have a marae setting which we liked because that made me feel at home. I think that’s what I was missing. But there have been a lot of changes during the years to that service, they’ve been cutting back tikanga which I’ve missed. (P5)
Clinical work with whānau
This theme critiqued the approach taken when working with the whānau of Māori patients seeking care for BD. While just over half of interviews included whānau, this theme was evident in most interviews. Three related sub-themes were identified: clinical engagement with whānau; clinical resourcing with whānau; and clinical contribution to whānau ora (family/support network wellbeing).
Clinical engagement with whānau
This sub-theme synthesised critique of the barriers and enablers to effective clinical engagement with whānau, and the impact on hauora for Māori patients with BD. Participants considered effective clinical engagement with whānau improved health outcomes for Māori with BD and facilitated service contact. Valued roles fulfilled by whānau included assistance to navigate pathways through care for BD, scheduling and transport to and from appointments, and in-person support.
Whānau were also recognised by participants as holding expert knowledge relevant to the assessment and treatment of BD, which could not be utilised without clinical engagement. Effective engagement with whānau allowed changes to patient symptomatology, early warning signs and notable risk factors to be managed proactively to prevent relapse. Engagement also enhanced the efficacy of interventions, as clinically informed whānau were equipped with knowledge to reinforce the importance of medications or encourage uptake of other clinical advice. In addition, services that engaged whānau could reinforce the value of everyday support, structure, stability and aroha (care/empathy/compassion) to prevent relapse after discharge.
Participants were critical of services when staff did not prioritise or recognise the need for clinical engagement with whānau. Lack of clinical engagement was a barrier to hauora and placed a burden of responsibility on Māori patients and whānau to educate staff about their unmet needs. Participants experienced tension when considering whether to provide feedback about ineffective clinical engagement with whānau, and reported occasions when whānau input was viewed pejoratively from a Westernised individualised perspective of health:
We weren’t even encouraged to attend appointments initially. So we just let him go to the appointments by himself. Then at a new service they said ‘it’s lovely to see you, it’s lovely that you are here, it’s great and it makes a difference’. Whereas before, it had been very much behind closed doors. The other thing was there was no real support for us as whānau about how we could best support him, what was best to do, or what bipolar disorder was. I mean, other staff wrote that I was an interfering mother basically. (W2)
Clinical resourcing with whānau
This sub-theme explored whether whānau were recognised as a finite resource fundamental to hauora, and if clinical resources for BD were aligned with (rather than imposed on) available whānau supports. Participants described the need for clinicians to recognise and respect the diverse realities of Māori whānau, and to tailor their clinical resourcing with whānau according to need. This included the need for health care providers to assist whānau to obtain knowledge and skills to support them to enhance clinical outcomes, by building on their existing roles. This critique highlighted the need to assess whānau strengths and resources, to inform a care plan that would not over-burden available whānau.
Participants were clear that clinical resourcing with whānau also equipped them with essential knowledge about BD and resources they could adapt to the changing needs of their loved one over time. This was viewed by participants as an efficient way of maximising a limited clinical resource, by empowering whānau whose relationships with patients extend beyond the clinical encounter. Where whānau support was absent or unavailable, greater resourcing was required from clinical services. In particular, services needed to provide clinical resources when whānau were unavailable, and work collaboratively with established supports:
There should be an investment made in educating the whānau and the consumer. Because you’re not always in the right state of mind when that information is being passed on, so there needs to be an intervention with the whānau as well. Because once you’re discharged from the service you go into the care of whānau. So if the service offered that support to whānau in a more meaningful way, in a faster way, and not just once it would improve the environment for the consumer and their whānau. (P6)
Clinical contribution to whānau ora
The final sub-theme synthesised critique of health care providers’ capacity to recognise and respond to whānau needs to improve hauora for Māori with BD. Participants were clear that clinicians needed to understand that patient and whānau wellbeing is interconnected for Māori to meaningfully contribute to whānau ora. When this was recognised, participants described an improved alignment between services and whānau to enhance hauora and reduce the risk of relapse on discharge. This required clinicians to have an understanding of the ongoing impacts of colonisation on whānau ora, and to assess and tailor care for Māori patients and whānau based on this.
Unfortunately, participants described a tendency for health staff to fail to acknowledge or enquire about the cumulative impact on whānau of caring for a loved one with a chronic condition like BD. Many participants expressed frustration when providers focused care exclusively on Māori patients, without considering the impact or process of treatment on that person’s whānau. To address this, participants recognised the need for a duty of care extending beyond the individual Māori patient, including a broader view of confidentiality and clinical scope, and greater resourcing to facilitate multi-service collaboration:
Services need to focus on educating our people. There needs to be wānanga with whānau to make a difference. Nice and early, manaaki the whānau and explain what’s going on. Then their children understand, know what triggers might be, and as they improve, how to work together so we can all support, and be part of the whole solution. Alongside that clinical model, wellness across the board. (W3)
Discussion
This research identifies barriers and enablers to high quality, culturally safe and equitable clinical care from the expert perspectives of Māori receiving services for BD in New Zealand. Three themes were evident from participants’ critique of clinical components of the health system. Theme 1 established that the efficacy of clinical care for BD was dependent on Māori patients and whānau having clear pathways through care, and being able to access timely, consistent care from clinically and culturally competent staff. Theme 2 identified the influence of clinical culture in BD services, embedded into care settings, expressed by staff, affecting the safety of clinical care for Māori. Theme 3 focused on the need for BD services to prioritise clinical work with whānau, equip staff with skills to facilitate engagement and tailor care with resources to enhance whānau as well as patient wellbeing.
These findings reinforce the utility of Māori models of health, Māori clinical practice frameworks and clinical guidelines for BD, but identify gaps in the standard of clinical care in New Zealand (Durie, 2011; Malhi et al., 2021; Pitama et al., 2017). Gaps were most evident in primary and community care, with few resources beyond medications, and an absence of psychological or social support risking relapse and harmful acute readmissions (McLeod et al., 2017; Malhi et al., 2021). This synthesis extends beyond broad systemic recommendations from other qualitative studies, by detailing changes required to clinical care, clinical culture and clinical work with whānau to improve hauora for Māori with BD in New Zealand (New Zealand Government, 2018; Waitoki et al., 2014). While the ability to access ‘by Māori for Māori’ BD services remains important, we found that this alone was insufficient to meet the health needs of Māori or address the contribution of clinician beliefs and behaviours to health inequity (Harris et al., 2006; Medical Council of New Zealand, 2019; Reid et al., 2019).
Findings also align with provider perspectives’ research investigating health care for Indigenous peoples with cancer, kidney disease, diabetes, mental health conditions and BD (Crowshoe et al., 2018; Johnstone and Read, 2000; New Zealand Government, 2018; Newman et al., 2013; Rix et al., 2013; Staps et al., 2019). Recommendations included the need for systemic changes to reposition responsibility with providers to deliver culturally safe, competent and equitable health care rather than blaming Indigenous patients and their families (Crowshoe et al., 2018; Johnstone and Read, 2000; New Zealand Government, 2018; Newman et al., 2013; Rix et al., 2013; Staps et al., 2019). Similar to our participants, providers also recognised they needed specialised training, knowledge and skills and greater resourcing to tailor care to their context, Indigenous patients and families, to address the determinants, barriers and enablers to health equity. Normalising reflective practice and service evaluation was also essential in provider research to reduce racism and discrimination in care affecting Indigenous peoples’ health outcomes (Crowshoe et al., 2018; Johnstone and Read, 2000; Newman et al., 2013; Rix et al., 2013).
The strengths of this study include the KMR design in an under researched area, adaptation of a method to privilege the expertise of Māori and identification of barriers and enablers to culturally competent, safe and effective clinical care for BD. This study also has limitations. First, recruiting Māori patients and whānau through health care providers may have limited participation to people with positive service experiences, however, this did not appear to be reflected in interview data. In addition, if time had allowed, separate interviews with patients and whānau may have highlighted different critique between groups, however, the benefits of one interview were considered and aligned well with KMR principles (Haitana et al., 2020a).
This study demonstrates that the standard of clinical care for Māori with BD in New Zealand does not align with practice guidelines, Māori models of health or clinical frameworks designed to inform treatment and address systemic barriers to equity (Durie, 2011; Malhi et al., 2021; Pitama et al., 2017). Barriers to equity and harmful approaches to care will continue unless clinicians and services are sufficiently equipped with training, knowledge and resources to meet pre-existing practice standards (Durie, 2011; Harris et al., 2006; Malhi et al., 2021; Pitama et al., 2017). This will require a commitment to evaluation and training, supporting all staff to deliver safe, effective, consistent care to Māori, and community-level resources to maintain hauora over time. While improving clinical care standards and implementing previously recommended health service changes are important (McLeod et al., 2017), we acknowledge the upstream drivers of inequity, and the need for research to identify necessary structural and organisational changes to our health system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Health Research Council (HRC) of New Zealand, Rangahau Hauora Māori Grant [HRC 16/338] and published with the support of a Ngā Pae o te Māramatanga Publication Support Grant.