
Abstract
Background:
Loneliness is known to be associated with both poorer physical and mental health, being associated with increased mortality. Responses throughout the world to the current COVID-19 pandemic all incorporate varying degrees of social distancing and isolation. There is an imperative to provide a timely review and synthesis of the impact of COVID-19 on loneliness in the general population.
Methods:
PubMed was searched using the key terms ‘COVID-19’, ‘coronavirus’, ‘SARS-COV2’ and ‘loneliness’. Fifty-four articles were identified and screened against the inclusion criteria. The inclusion criteria stipulated that the study needed to incorporate a measure of loneliness with participants being drawn from the general adult population. Twenty-four studies met the inclusion criteria.
Results:
The key data extracted from the 24 reviewed studies are presented and summarised with a focus on key demographics of participants, the research designs utilised, the measures of loneliness employed and the other variables assessed in the studies. Overall, the findings indicate that loneliness has been a significant issue during the current COVID-19 pandemic and loneliness is positively associated with mental health symptoms. However, there were inconsistencies in the results evident across studies.
Conclusion:
To our knowledge, this is the first systematic review of research investigating loneliness during the current COVID-19 pandemic in the general adult population. Despite the inconsistencies evident in some of the results across the studies, it is clearly apparent that loneliness is having an impact on the mental health and wellbeing of the general adult population. Furthermore, it is apparent that the current COVID-19 pandemic has had an impact on loneliness in the general adult population and that loneliness is significantly positively associated with mental illness symptomatology. Thus, there is an imperative to address loneliness through public policy and interventions. The limitations of this review are noted and directions given for future research.
Background
COVID-19 was declared a pandemic on 11 March 2020 by the World Health Organization (Ali et al., 2020). COVID-19 is a novel coronavirus that originated in China and rapidly spread worldwide (Ali et al., 2020). As COVID-19 is highly infectious and can be fatal for some individuals, the only known defence for populations worldwide was to adopt strategies to negate and minimise contact between people (Lonergan and Chalmers, 2020). Countries all over the world implemented social distancing policies. Some countries enforced lockdowns where individuals were required to stay in their homes for a period of time to slow the spread of the virus (Lonergan and Chalmers, 2020). Thus, efforts to slow the spread of the virus have resulted in consequences associated with reduced social contact for people all over the world. Accordingly, social isolation and loneliness have become a concern worldwide.
Loneliness and social isolation, despite being inextricably linked, are different concepts. Loneliness is most commonly defined as the subjective negative feeling that an individual’s social network is smaller and lacking in quality to what is desired (Fakoya et al., 2020; Hajek et al., 2020), whereas social isolation can be defined as an objective lack of social interactions or the feeling that one does not fit into society (Fakoya et al., 2020; Hajek et al., 2020). Thus, although COVID-19 has increased social isolation throughout the world, it is possible for an individual to be socially isolated without being lonely. Conversely, it is also possible for an individual to not be socially isolated but experience loneliness as their social network is not of the desired size or quality to meet their social needs and expectations.
Prior to the COVID-19 pandemic, there were increasing public health concerns regarding the challenge of loneliness (Fakoya et al., 2020). Prior to the start of the COVID-19 pandemic, the Government of the United Kingdom had declared a loneliness epidemic (Jeste et al., 2020). Across the world, societies are ageing, with many individuals experiencing loneliness (Fakoya et al., 2020). Loneliness among the elderly is known to be common in developed countries (Leigh-Hunt et al., 2017). However, concerns pertaining to loneliness are not isolated to the elderly, as younger people are also known to be experiencing loneliness at an alarming rate (Leigh-Hunt et al., 2017). The recent Australian Loneliness Report (Australian Psychological Society and Swinburne University of Technology, 2018) found that one in four Australian adults are lonely, with the oldest adults (those over 65 years) reporting lower mean levels of loneliness in comparison with younger Australian adults.
The growing concerns pertaining to increases in loneliness in the community prior to COVID-19 are related to the fact that loneliness is known to be associated with increased mortality and reduced quality of life (Groarke et al., 2020; Hajek et al., 2020). Research has indicated that loneliness contributes to both physical and mental health conditions as well as being associated with decreases in cognitive functioning (Groarke et al., 2020; Hajek et al., 2020; Jeste et al., 2020). Furthermore, the impact of loneliness on an individual’s health has been equated with the impact of other factors that are well known to be detrimental to health, such as smoking, obesity and a lack of physical activity (Fakoya et al., 2020). Therefore in the context of the pre-existing loneliness epidemic (Jeste et al., 2020) and the outcomes that are known to be associated with loneliness, there is an increased need to understand the impact of the current COVID-19 pandemic on loneliness. Recently, other researchers have called for research into loneliness during the current COVID-19 pandemic (Holmes et al., 2020; Smith and Lim, 2020).
Therefore, the primary aim of this rapid review was to perform an updated and timely rapid systematic review to identify, assess and summarise available peer-reviewed research on loneliness during the current COVID-19 pandemic. This rapid review focuses specifically on the impact of the COVID-19 pandemic on loneliness in the general adult population. There is a necessity for such information to inform public policy and support the health of individuals worldwide during the current pandemic and into the recovery. Furthermore, to our knowledge, this is the first review summarising the impact of COVID-19 on loneliness in the adult general population worldwide.
Methods
The protocol for this rapid systematic review was developed in accordance with the majority of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The protocol for this rapid review was not registered with PRISMA due to time constraints; with the current situation of COVID-19 and the rapid proliferation of information, the decision was made to expedite the process. Hence, a rapid review was selected over a more in-depth systematic and/or meta-analytic review. Furthermore, this decision aligns with the overall aims of the review, to provide a rapid systematic review and synthesis of the current research pertaining to loneliness during the current COVID-19 pandemic in the general adult population.
Search strategy
The development of the search strategy incorporated the need to provide a rapid review of the existing evidence and expedite the results. As such, a single database was selected, PubMed, as this database has one of the largest repositories of biomedical and health science literature. As the primary focus of this article is ‘loneliness’ and ‘COVID-19’, these two terms were used. In addition to ‘COVID-19’, ‘SARS-COV-2’ and ‘coronavirus’ were used. Following the notion of the primary focus, the decision was made to limit results to titles that included references to ‘loneliness’ and ‘COVID-19’ (or ‘SARS-COV-2’ and ‘coronavirus’). The search was conducted on 4 November 2020. The search yielded 54 results; the results were assessed against the selection criteria described below. The search strategy and study selection are summarised in Figure 1.
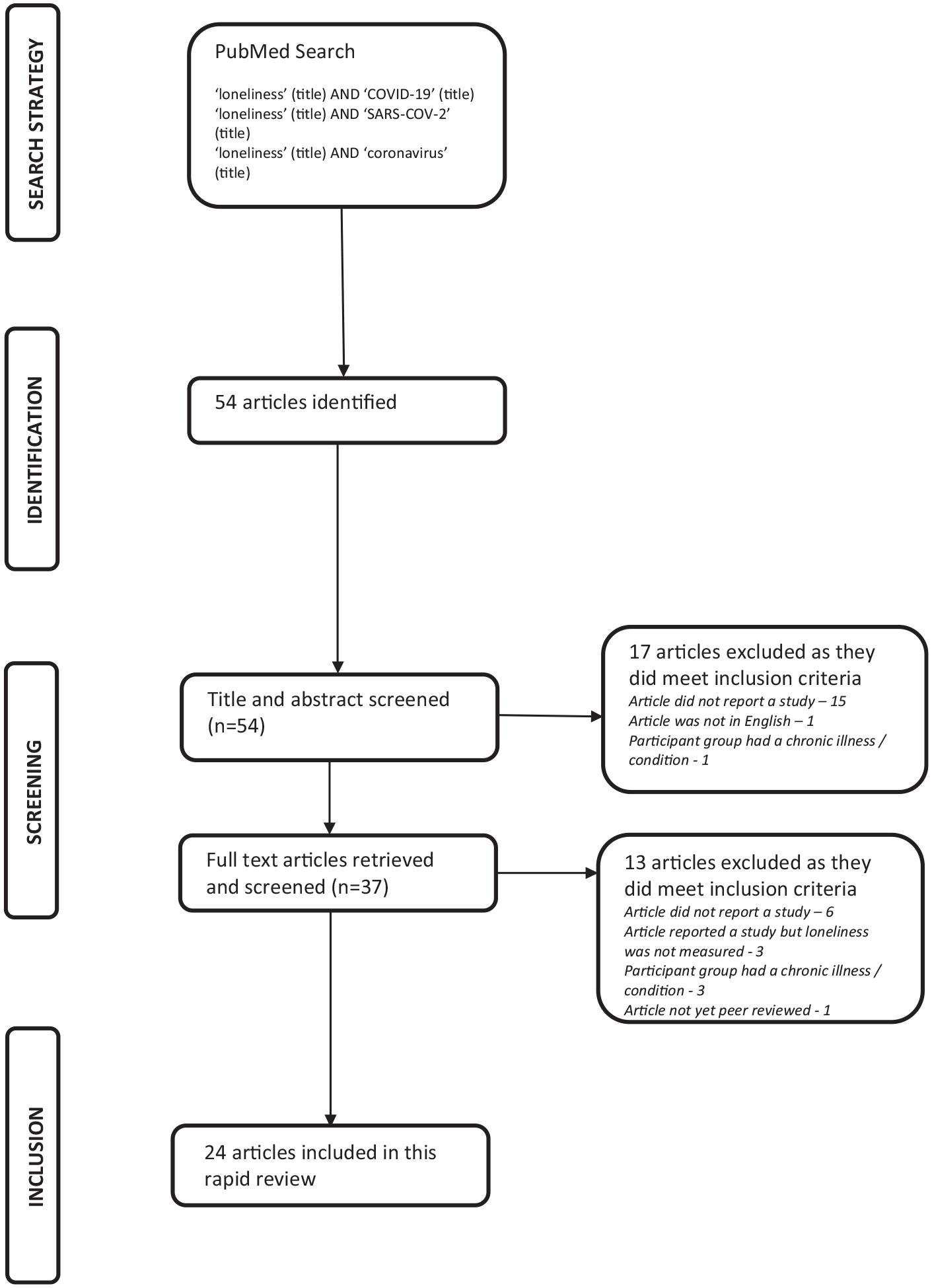
Search strategy and study selection flowchart.
Selection criteria
For articles to be included in this rapid review, they had to report on a study and be published in English and in a peer-reviewed journal (after peer review). All articles needed to contain a measure of loneliness with the study being conducted during the current COVID-19 pandemic. The participants had to be adults (18 years plus) from the general population. The decision was made to exclude articles that reported on subsets of the general population, for example, those with specific medical conditions. The decision was made to forego rigorous quality assessment as due to COVID-19 the studies had been developed and conducted in a shorter time frame than usual. Instead, prior peer review was used as an indicator of the quality of the study and assisted with expediting the findings of this rapid review.
Data extraction
The sample size and characteristics, country the study was conducted in, the aim, the measure of loneliness utilised, other variable measures and the key findings were recorded for each of the 24 included articles in an Excel spreadsheet.
Results
This rapid systematic review reviewed 24 studies investigating loneliness during the COVID-19 pandemic. The 24 studies originated from 13 different countries worldwide. Six studies came from America, four from Israel, three from the United Kingdom and two from Austria. One study originated from each of the following countries: Poland, Switzerland, Spain, Australia, Greece, Italy, Japan, Hong Kong (China) and the Netherlands. The key data extracted from each study during the review process are summarised in Tables 1–3. The studies were separated by research design; Table 1 details the cross-sectional studies, Table 2 the longitudinal studies and Table 3 the intervention-based study.
Data extracted from reviewed studies: cross-sectional research design.
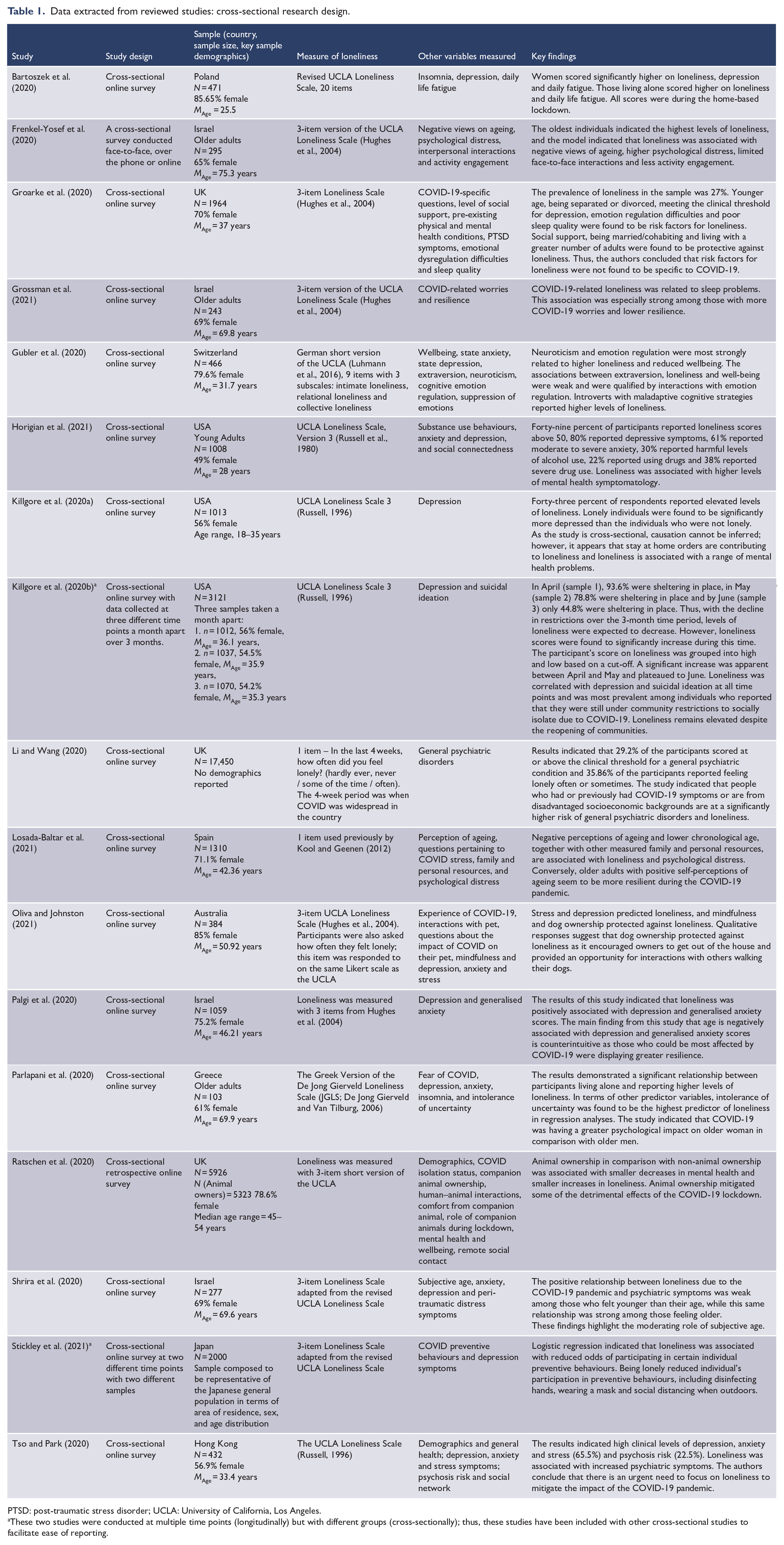
PTSD: post-traumatic stress disorder; UCLA: University of California, Los Angeles.
These two studies were conducted at multiple time points (longitudinally) but with different groups (cross-sectionally); thus, these studies have been included with other cross-sectional studies to facilitate ease of reporting.
Data extracted from reviewed studies: longitudinal research design.
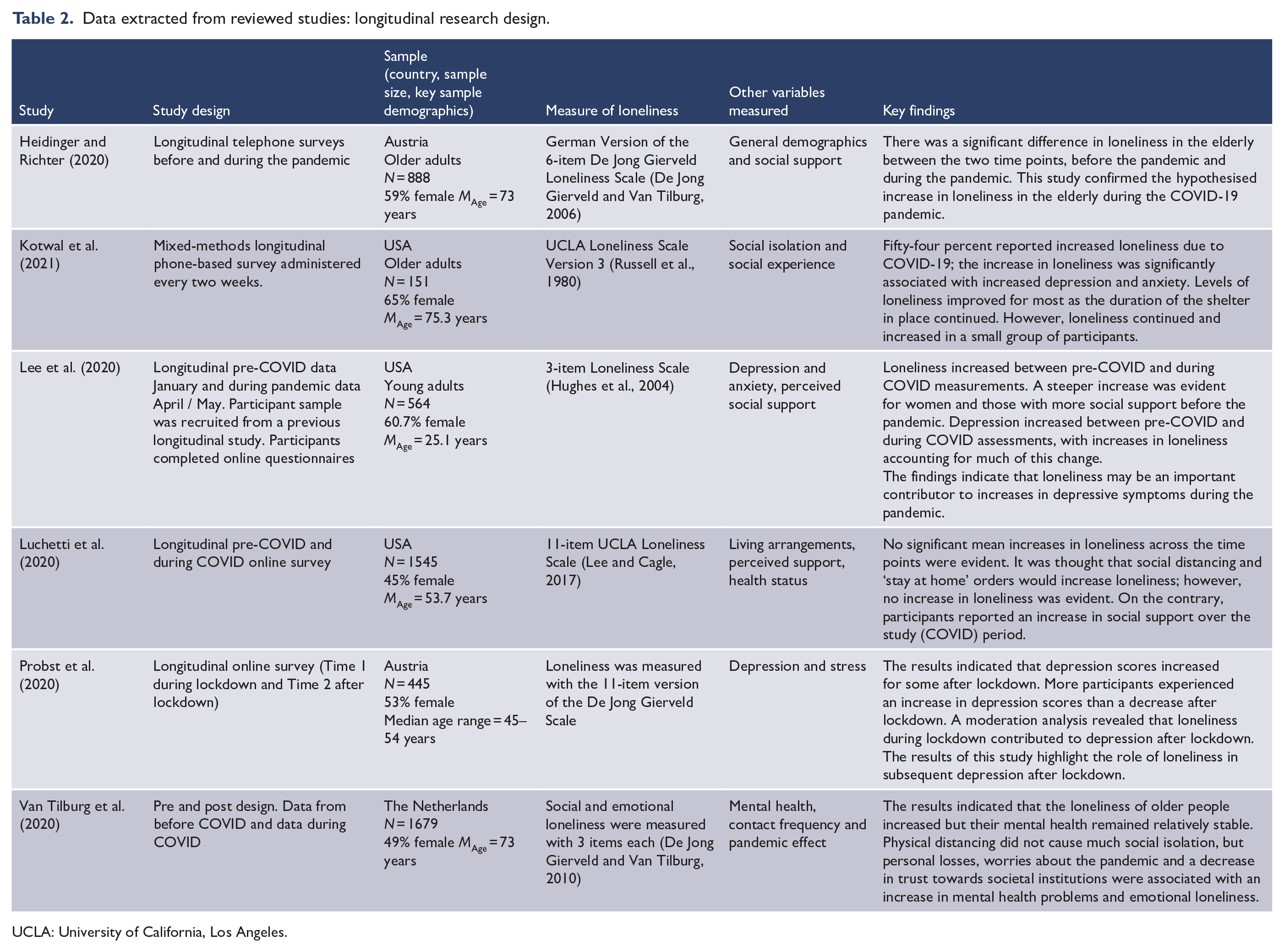
UCLA: University of California, Los Angeles.
Data extracted from reviewed studies: intervention-based research design.
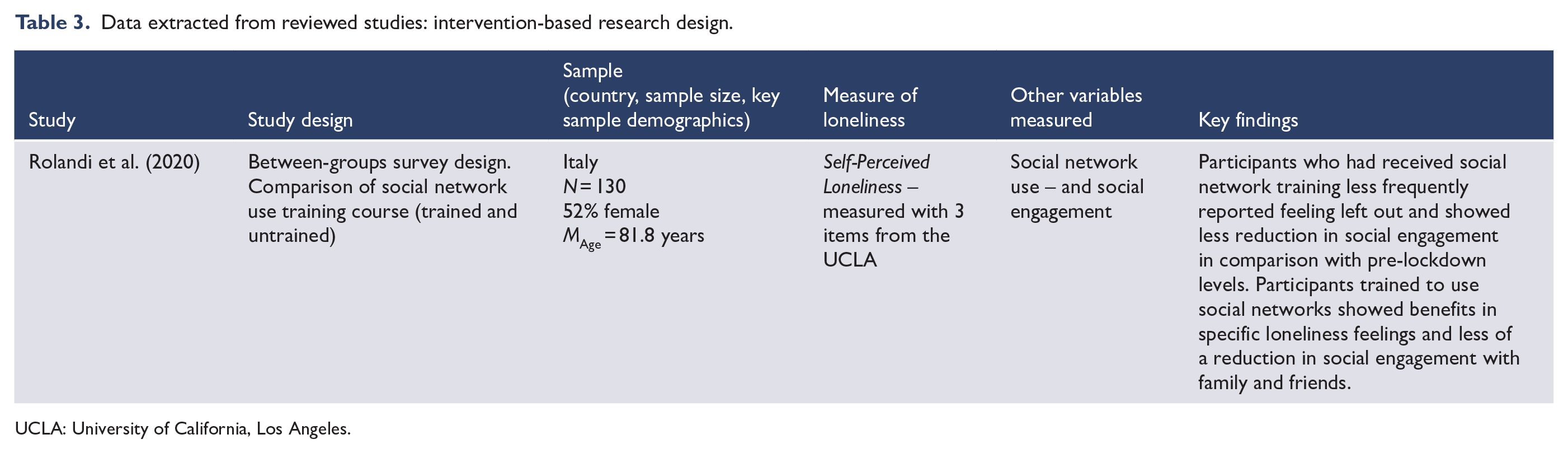
UCLA: University of California, Los Angeles.
Key participant demographics
The majority of participants (>50%) in 20 of 24 studies were women. Two studies did not report participant demographics, while the other two studies had samples with slightly less than 50% female respondents. The studies differed in the mean age of participants; some studies specifically focused on older or younger participants, while some studies included all adult age groups. Furthermore, the specific findings of the studies are difficult to compare as in addition to the demographic differences in the participants sampled, different studies tested how loneliness was associated with different variables. Nonetheless, general demographic trends evident across the studies are summarised below.
Bartoszek et al. (2020) in a study conducted in Poland reported that women scored significantly higher on loneliness and depression in comparison with men. Similarly, Parlapani et al. (2020) investigated the impact of the COVID-19 lockdown in Greece on older adults. It was evident that the lockdown was having a greater psychological impact on older women in comparison with older men. Higher levels of intolerance of uncertainty were found to be associated with greater levels of loneliness.
Thus, Parlapani et al. (2020) found that COVID 19 was having a greater impact on older women. Not all studies commented on the relationship between gender and loneliness; however, none of the studies reviewed reported a greater association between men and loneliness. Therefore it is evident that women in comparison with men tend to be lonelier.
The mean age of participants differed between the studies, as some studies assessed only older adults or younger adults, while other studies were open to all adults to participate. Thus, the mean age of participants differed across the studies. A cross-sectional study conducted by Frenkel-Yosef et al. (2020) with older adults found that the oldest individuals were the loneliest. However, loneliness in this cohort was moderated by negative views of ageing, higher levels of psychological distress and limited face-to-face interactions. Similarly, Gubler et al. (2020) found that younger individuals reported less loneliness, whereas a study conducted by Groarke et al. (2020) with participants between the ages of 18 and 87 years observed that loneliness was the highest in younger individuals. Similarly, Losada-Baltar et al. (2021) found the lower chronological age was associated with increased levels of loneliness. Thus, results regarding the association between age and loneliness are mixed.
In addition to gender and age, some studies assessed other demographic factors such as living arrangements and socioeconomic status. Bartoszek et al. (2020) found that individuals living alone were lonelier than individuals residing with someone else (Bartoszek et al., 2020). Similarly, Gubler et al. (2020) reported that individuals in romantic relationships are less lonely than their single peers. Similarly, Li and Wang (2020) also found that having a partner is a protective factor against loneliness. Furthermore, Li and Wang (2020) found that coming from a disadvantaged socioeconomic background was associated with loneliness. Several studies found a relationship between being in a romantic relationship and/or living with someone as a protective factor against loneliness during COVID.
Research designs
The most common research design employed in the studies reviewed was a cross-sectional design (n = 17; see Table 1), of which the majority utilised online surveys. The other research designs used were longitudinal (n = 6; see Table 2) and a single intervention-based study (n = 1; see Table 3).
Cross-sectional research design
Seventeen of the reviewed studies utilised a cross-sectional research design investigating loneliness in the general adult population during the current COVID-19 pandemic. In addition, the majority of studies included the moderating and mediating effects of other variables such as psychological distress, depression, problems with sleep and even pet ownership. The findings of the majority of studies indicated elevated levels of loneliness during the current pandemic. Furthermore, many studies found a significant association between poor mental health indices and loneliness during COVID-19 (Groarke et al., 2020; Horigian et al., 2021; Killgore et al., 2020a, 2020b; Li and Wang, 2020; Losada-Baltar et al., 2021; Oliva and Johnston, 2021; Palgi et al., 2020; Tso and Park, 2020).
Longitudinal research design
Six of the reviewed studies used a longitudinal research design to assess the impact of the COVID pandemic on levels of loneliness in the general adult population. Overall, the findings were inconclusive with two studies finding no difference in the levels of loneliness before and during the pandemic (Heidinger and Richter, 2020; Luchetti et al., 2020). Conversely, another two studies found that loneliness increased during the pandemic (Lee et al., 2020; Van Tilburg et al., 2020), while Kotwal et al. (2021) found that levels of loneliness decreased during the shelter in place order in the United States. Finally, Probst et al. (2020) found an association between loneliness and stress during lockdown and depression.
Intervention-based research design
Of the 24 articles included in this review, only 1 was an intervention; Rolandi et al. (2020) conducted a between-groups intervention where they trained older adults in the use of social networks prior to the pandemic and compared their levels of loneliness to a demographically similar group of untrained older adults during the COVID-19 lockdown in Italy. Those who were trained in social network use were less lonely than their untrained peers during the extended COVID-19 lockdown in Italy.
Measures of loneliness
The most common measure of loneliness employed in the studies reviewed was the University of California, Los Angeles (UCLA) 3-item version Loneliness Scale (n = 11; Hughes et al., 2004). Oliva and Johnston (2021) utilised the 3-item UCLA Loneliness Scale (Hughes et al., 2004) in a cross-sectional survey of animal owners’ and non-animal owners’ experience of the lockdown in Australia. It was evident that stress and depression contributed to loneliness, while dog ownership and mindfulness were protective against loneliness. Palgi et al. (2020) also utilised the 3-item UCLA Loneliness Scale (Hughes et al., 2004) in a cross-sectional study. The study assessed loneliness, depression and generalised anxiety. The results indicated that loneliness was positively associated with both depression and anxiety; surprisingly, age was negatively associated with both depression and anxiety. Thus, older adults, although more vulnerable to COVID-19, were showing greater resilience and less loneliness.
Other versions of the UCLA Loneliness scales were also utilised (n = 6). Killgore et al. (2020a, 2020b) utilised the UCLA Version 3 Loneliness Scale (Russell, 1996) in cross-sectional online surveys conducted in the United States. The findings indicated that levels of loneliness were high and associated with depression (Killgore et al., 2020a, 2020b) and suicidal ideation (Killgore et al., 2020b). Furthermore, Killgore et al. (2020b) conducted a series of three cross-sectional surveys (April, May and June) and found that loneliness increased between April and May and plateaued in June. It was evident that loneliness remained despite the reopening of communities.
The De Jong Gierveld Loneliness Scale (De Jong Gierveld and Van Tilburg, 2006) was utilised by n = 4 studies. One study used a single item drawn from a previous study and one study used a single author-generated item. Thus, 23 of the 24 studies utilised items from previously published and validated scales measuring loneliness. Probst et al. (2020) conducted a longitudinal online survey during and after lockdown in Austria investigating changes in depression levels between the two time points. Depression was found to increase after lockdown. A moderation analysis indicated that respondents who were lonely during lockdown were more likely to be depressed after lockdown.
Other variables assessed
The most common additional variables assessed in the studies pertained to mental health and mental illness. Nineteen of the 24 studies reviewed included at least one mental illness or mental health measure. The two most common mental health indices assessed were depression and anxiety. Four of the studies that did not assess mental health–related variables all included measures pertaining to social support and resources, while one study assessed resilience.
Tso and Park (2020) investigated psychological distress and loneliness in Hong Kong in response to COVID-19. The authors identified a very high clinical level of depression, anxiety and stress in the respondents. An elevated risk of psychosis was also evident in 22% of respondents. Loneliness was associated with increased psychological distress and symptoms (Tso and Park, 2020). Similarly, Li and Wang (2020) conducted a study assessing general psychiatric disorders and loneliness in the United Kingdom in response to COVID-19. The results indicated that nearly a third of respondents scored above the clinical threshold for at least one general psychiatric condition, while over a third of respondents indicated that they were feeling lonely often or sometimes. The majority of the studies that measured mental health–based indices found an association between poor mental health and loneliness during COVID-19.
Stickley et al. (2021) investigated whether loneliness significantly impacted the odds of performing COVID-19 preventive behaviours in Japan. It was apparent that lonely individuals were less likely to engage in necessary COVID-19 preventive behaviours such as hand washing, wearing a mask and social distancing.
Luchetti et al. (2020) conducted a longitudinal study assessing loneliness, living arrangements, perceived support and health status before and during COVID-19 ‘stay at home orders’ in a study with participants with an average age of 53.7 years. It was thought that loneliness would increase during this period; however, no significant increase in loneliness was evident. Respondents indicated an increase in social support during this period. Conversely, Van Tilburg et al. (2020) conducted a similar longitudinal study in older adults in the Netherlands and found that loneliness did increase but the respondents’ mental health did not change significantly.
Discussion
It is apparent from this rapid systematic review that the current COVID-19 pandemic has had a substantial impact on loneliness in the general adult population (Killgore et al., 2020a, 2020b; Li and Wang, 2020). Furthermore, it was evident that loneliness and mental health symptomatology were significantly positively associated (Horigian et al., 2021; Kotwal et al., 2021; Li and Wang, 2020). Although there were some inconsistencies evident in the results across all 24 studies reviewed, overall levels of loneliness and associated distress (mental health symptoms, sleep problems etc.) in the adult general population are significant during the current COVID-19 pandemic. However, loneliness did not emerge as a result of COVID-19; loneliness was known to be a significant public health issue prior to COVID-19 (Lim et al., 2020).
Thus, has COVID-19 increased the levels of loneliness in the general adult population? Three of the longitudinal studies reviewed investigated the levels of loneliness in the general adult population before and during the COVID-19 pandemic. Heidinger and Richter (2020) as well as Lee et al. (2020) found that loneliness levels have increased since the start of the pandemic. Conversely, Luchetti et al. (2020) found no increase in loneliness levels in American adults in comparison with pre-pandemic levels of loneliness. However, a recent white paper ‘Ending loneliness together in Australia’ highlighted that one in two Australians report being lonelier since the onset of the COVID-19 pandemic (Ending Loneliness Together, 2020). Therefore, it remains unclear whether loneliness has increased in the general adult population as a result of the COVID-19 pandemic.
The research pertaining to loneliness during the current COVID-19 pandemic reviewed in this article originated from 13 countries around the world. Thus, although this provides a relatively good sample geographically regarding loneliness in the general population during COVID-19, a lot of countries contributing to these findings are quite similar, being developed nations. Therefore, there is a need to explore loneliness during this time in less developed and more disadvantaged countries. This is especially crucial as loneliness has been found to be elevated in individuals coming from socioeconomically disadvantaged backgrounds (Li and Wang, 2020; Lim et al., 2020). However, such findings may be relative to the society an individual resides in.
Many of the inconsistencies in the data across the studies pertain to the simple demographic factors of gender and age. For example, some studies reported that women felt lonelier than their male peers (Bartoszek et al., 2020; Parlapani et al., 2020), while numerous other studies did not report any significant gender differences in loneliness (Groarke et al., 2020; Palgi et al., 2020; Tso and Park, 2020). Previous research has highlighted that the elevated levels of loneliness in women in comparison with men may result from how loneliness is measured (Lim et al., 2020), with women being more willing to answer direct questions pertaining to loneliness, while men are more likely to respond to more discrete questions. Furthermore, most of the recognised measures of loneliness have not been validated across different age groups and cultures, which contributes to the inconsistency in results.
Age was another demographic variable with inconsistencies in the data across studies. Some studies reported that loneliness is more of an issue for older adults (Heidinger and Richter, 2020; Van Tilburg et al., 2020), while other studies found that older adults were more resilient (Kotwal et al., 2021) and less lonely during the COVID-19-induced lockdowns in comparison with younger adults (Groarke et al., 2020; Horigian et al., 2021). Interestingly, some studies indicated that it was not age per se that was associated with loneliness, it was the participants’ perception of their age that was a significant contributing factor to loneliness (Losada-Baltar et al., 2021; Shrira et al., 2020), that is, individuals who held more negative views of ageing tended to be lonelier than individuals who held more positive views on ageing (Losada-Baltar et al., 2021; Shrira et al., 2020).
Intuitively it makes sense that loneliness would be more of an issue in an older population; however, Heidinger and Richter (2020) and Van Tilburg et al.’s (2020) studies were limited to only older adults. Kotwal et al. (2021) found that loneliness improved for most of the older adults in their study as the lockdown continued; however, there was a subset for which loneliness did not improve. Furthermore, Groarke et al. (2020) found that loneliness was more evident in younger adults and those with mental health symptomatology. Similarly, Horigian et al. (2021) found that loneliness was associated with mental illness symptoms in a sample of young adults. Thus, it may be that mental illness or health and resilience are the defining risk and protective factors in relation to loneliness during the current pandemic rather than age.
Inconsistencies were also apparent in data pertaining to loneliness throughout the lockdown investigated by cross-sectional and longitudinal studies. Killgore et al. (2020a, 2020b) found that home-based lockdowns contributed to loneliness during the current COVID-19 pandemic across a series of cross-sectional online surveys, whereas Luchetti et al. (2020) found that loneliness did not significantly increase during the lockdown period in a longitudinal study. These inconsistencies could potentially be explained by the difference in research designs, with Killgore et al. (2020a, 2020b) sampling different respondents at each time point and Luchetti et al. (2020) maintaining a repeated-measures approach. The participants in Killgore et al. (2020a, 2020b) could see the research as an opportunity vent, whereas Luchetti et al.’s (2020) respondents had already participated and thus felt like their view and feelings had been heard.
Interestingly, some studies indicated that loneliness and mental illness symptoms did not dissipate when the lockdowns ended; instead, the loneliness continued despite communities reopening (Killgore et al., 2020b). Lee et al. (2020) ascertain that increases in loneliness are the most likely cause of increases in depressive symptoms during the pandemic. More conclusively, Probst et al. (2020) found that loneliness during the lockdown period contributed to depression after the lockdown period. Moreover, it is known that the development of mental illness can further reinforce levels of loneliness (Lim et al., 2020).
Limitations and recommendations for future research
This rapid systematic review is limited by several factors. First, this review was conducted in an expedited time frame to support the delivery of timely results; as such, the review process was shortened. Specifically, only one database was used to conduct the review and no grey literature was searched. Furthermore, the search strategy was limited to keywords (loneliness*, COVID-19, SARS-COV-2, coronavirus) being part of the title. Thus, future reviews could seek to broaden the search strategy and inclusion criteria. Also as more research is published in the area, a meta-analysis may be warranted.
In regard to the research reviewed, many of the studies had similar research designs, with many studies being cross-sectional online surveys. This is not surprising due to the context and nature of the research. Cross-sectional designs are limited as they cannot infer causality, which is important in delineating the relationship between loneliness, mental illness and COVID-19. However, there were also longitudinal and telephone-based survey studies identified and reviewed. More longitudinal research is required to further verify the relationship between loneliness and mental illness. There is also a need to develop research designs that can successfully delineate between loneliness as a consequence of COVID-19 and loneliness caused by other factors. Furthermore, some of the studies were limited by the sample size and the self-selection bias of those choosing to participate in the research. Thus, the results may not be indicative of the general population due to these sampling limitations. Thus, future studies should seek to include larger samples and randomly sample from the population of interest.
A further confounding variable is the severity of the COVID-19 pandemic in the country and specific area the study was undertaken in. Following from this is the level of restrictions the country and associated area where the study was undertaken were subject too at the time of the study. Thus, most studies did not control for or specifically measure these factors. Future studies could attempt to overcome this bias by directly measuring the impact of COVID-19 within the population being assessed. For example, this could be captured through reported indices of testing rates, number of COVID cases and deaths per day. In addition, the personal impact of the pandemic on the individual could also be measured through measures such as the Pandemic Emotional Impact Scale (PEIS; Ballou et al., 2020). The results of studies that measure and control for these factors will provide a clearer understanding of the impact of COVID-19 on loneliness in the general adult population.
Conclusion
To our knowledge, this is the first systematic review of empirical research investigating loneliness during the current COVID-19 pandemic in the general adult population. Thus, this rapid review provides the first synthesis of previous research into loneliness during the current pandemic. Despite the inconsistencies evident in some of the results across the studies, it is clearly apparent that loneliness is having an impact on the mental health and wellbeing of the general adult population worldwide and that this impact has increased since the start of the COVID-19 pandemic. Specific country-based data are required worldwide from rigorous studies that control for significant confounding factors in order to delineate broad population-based interventions. Thus, there is a need to immediately seek to address loneliness as a consequence of the current pandemic through public policy and interventions in order to support the health and wellbeing of individuals’ worldwide and to mitigate the impact of loneliness on mental health indices now and into the recovery phase of the pandemic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.