
Abstract
Objective:
This study sought to assess the extent to which gender attitudes are associated with mental health among Australian men and women.
Methods:
This study used a sample of 26,188 individuals drawn from five waves of the Household, Income and Labour Dynamics in Australia Survey. Gender attitudes were classified into three groups (traditional, moderate-egalitarian and egalitarian), and were constructed from six items. Mental health was measured using the Mental Health Inventory (MHI-5). We calculated the magnitude of associations between gender attitudes and mental health, stratified by gender, and adjusted for potential confounding.
Results:
Compared to men with egalitarian attitudes, poorer mental health was observed among men with moderate-egalitarian (−1.16, 95% confidence interval = [−1.84, −0.49]) and traditional gender attitudes (−2.57, 95% confidence interval = [−3.33, −1.81]). Among women, poorer mental health was observed among those with moderate-egalitarian (−0.78, 95% confidence interval = [−1.34, −0.22]) and traditional attitudes (−1.91, 95% confidence interval = [−2.55, −1.26]) compared to those with egalitarian attitudes.
Conclusions:
For both men and women, egalitarian gender attitudes were associated with better mental health.
Keywords
Introduction
Gender equality imparts benefits to individuals and society across many domains including health, economic security and productivity. Initiatives in Australia, as in other parts of the world, have continued to gain momentum to drive and enact changes in gender equality towards increasing egalitarianism. These changes are represented at all levels of society. At the macro level, education systems, labour markets and political systems in most developed countries have been transformed by the increasing representation of women. At an individual level, changes have translated into dramatic shifts in the roles and opportunities that individuals have in society. Shifts towards gender equality are considered to represent one of the most significant social achievements of modern times. Despite substantial gains, gender gaps remain; the gender pay gap, for example, has remained relatively unchanged in many parts of the world, including Australia, for the past two decades (Workplace Gender Equality Agency [WGEA], 2020).
Epidemiological research has typically drawn on structural and material measures such as education, economic resources, and the intersections between these measures and gender, when assessing health outcomes in relation to gender equality. Few studies however, have considered gender ideology (including norms, attitudes and beliefs) as an exposure, and assessed health outcomes in relation to these. This is an important gap, particularly because at the attitudinal level, there is some evidence that momentum towards gender egalitarianism has slowed, or even stalled (England, 2010).
Gender norms define consensual expectations about what women and men do, and prescribe what should be done (Cislaghi and Heise, 2020). They also embody beliefs about behaviours and attributes considered appropriate and esteemed for males and females (Heise et al., 2019), and the importance of this was the focus of a recent special edition in The Lancet on the relationship between gender norms, gender equality and health (Heise et al., 2019; Rao Gupta et al., 2019). Heise et al. (2019) articulated a conceptual framework for the way the gender system impacts on health across the life course. From birth, individuals are immersed in a gender system that operates across multiple social domains including family, community, institutions such as schools, and structures and policies. These structures embed patriarchy and sexism, and distribute power, resources and status according to gender, and intersect with other systemic forms of discrimination such as ableism, ageism, racism and classism to structure differential health outcomes (Heise et al., 2019).
Gender normative beliefs and expectations are commonly assessed using gender attitudes that tap into beliefs about behaviours and responsibilities that are appropriate and desirable for men and women. According to the gender ideology framework, gender attitudes are typically distributed across a spectrum ranging from traditional to egalitarian (Davis et al., 2007). Gender ideology has effects across many domains in life including fertility and relationships, education, employment and income, relationship quality, the division of household labour and inter-partner violence (Davis and Greenstein, 2010). Shifts in gender ideology towards egalitarianism are observed as individuals age (Fan and Marini, 2000), and with cohort replacement – new generations tend to report more egalitarian attitudes (Brooks and Bolzendahl, 2004).
Only a small number of studies have examined associations between gender attitudes and mental health. Analysis of data collected from 2 years (1991 and 2007) of the British Household Panel Survey showed that more traditional gender attitudes were associated with more psychological distress, particularly for men (Sweeting et al., 2014). Among middle-aged adults in the United Kingdom, traditional gender attitudes were associated with suicidal ideation (Hunt et al., 2006), and in Australia, egalitarian gender attitudes in adolescents were associated with better outcomes on some dimensions of mental health (King et al., 2019).
A body of work has also found that adherence or conformity to masculine norms (Houle et al., 2008; Pirkis et al., 2017) was associated with an increased risk of suicidal behaviours and reduced help-seeking behaviour among males. Among adolescent males, certain masculine norms such as self-reliance have also been associated with greater suicidal ideation (King et al., 2020). Overall however, there has been scant research examining gender attitudes and associations with mental health in population representative samples of adults internationally and in Australia. This represents an important gap in evidence. If there is evidence that egalitarian gender attitudes are associated with improved mental health among both men and women, this opens important avenues for approaching gender equality initiatives.
Using a large population representative sample of Australian adults, we examined associations between gender attitudes and mental health. Based on previous work examining gender attitudes among adolescents, and given known associations between masculine norms and suicidality, it was hypothesised that compared to egalitarian attitudes, traditional gender attitudes would be associated with poorer mental health for both men and women.
Methods
Study design and participants
Data were drawn from a longitudinal, nationally representative study – the Household, Income and Labour Dynamics in Australia (HILDA) Survey (Department of Social Science, Melbourne Institute of Applied Economic and Social Research, 2020). The HILDA Survey commenced in 2001 drawing on a large national probability sample of households occupying private dwellings. The baseline wave of the survey consisted of over 13,000 individuals aged 15 years and over, within more than 7000 households. HILDA collects detailed, annual information on a range of topics, including social, demographic, health and economic conditions, using a combination of face-to-face interviews with trained interviewers and a self-completion questionnaire.
To maintain representativeness of the Australian population, the sample has been supplemented in several ways. First, as individuals within the sample households turn 15 years of age, they have been invited to participate. Second, as baseline respondents change households, their new household members have been invited to participate. Third, in 2011, a top-up sample of 2000 people was added to the cohort to ensure optimal representation of the Australian population (Summerfield et al., 2019). The response rate in Wave 1 was 66% and wave-on-wave retention rates have been over 90% in each study wave thereafter (Summerfield et al., 2019). Over 70% of the new respondents invited into the study have continued to participate (Summerfield et al., 2019).
Our sample selection is shown in Figure 1. A total of 42,747 participants had ever taken part in a wave of the Survey, but 6951 never completed a survey in the waves covered in this analysis. A further 9380 participants had no recorded responses for mental health or gender attitudes and were excluded. The final sample consisted of 26,416 respondents (n = 13,588 women and n = 12,828 men).
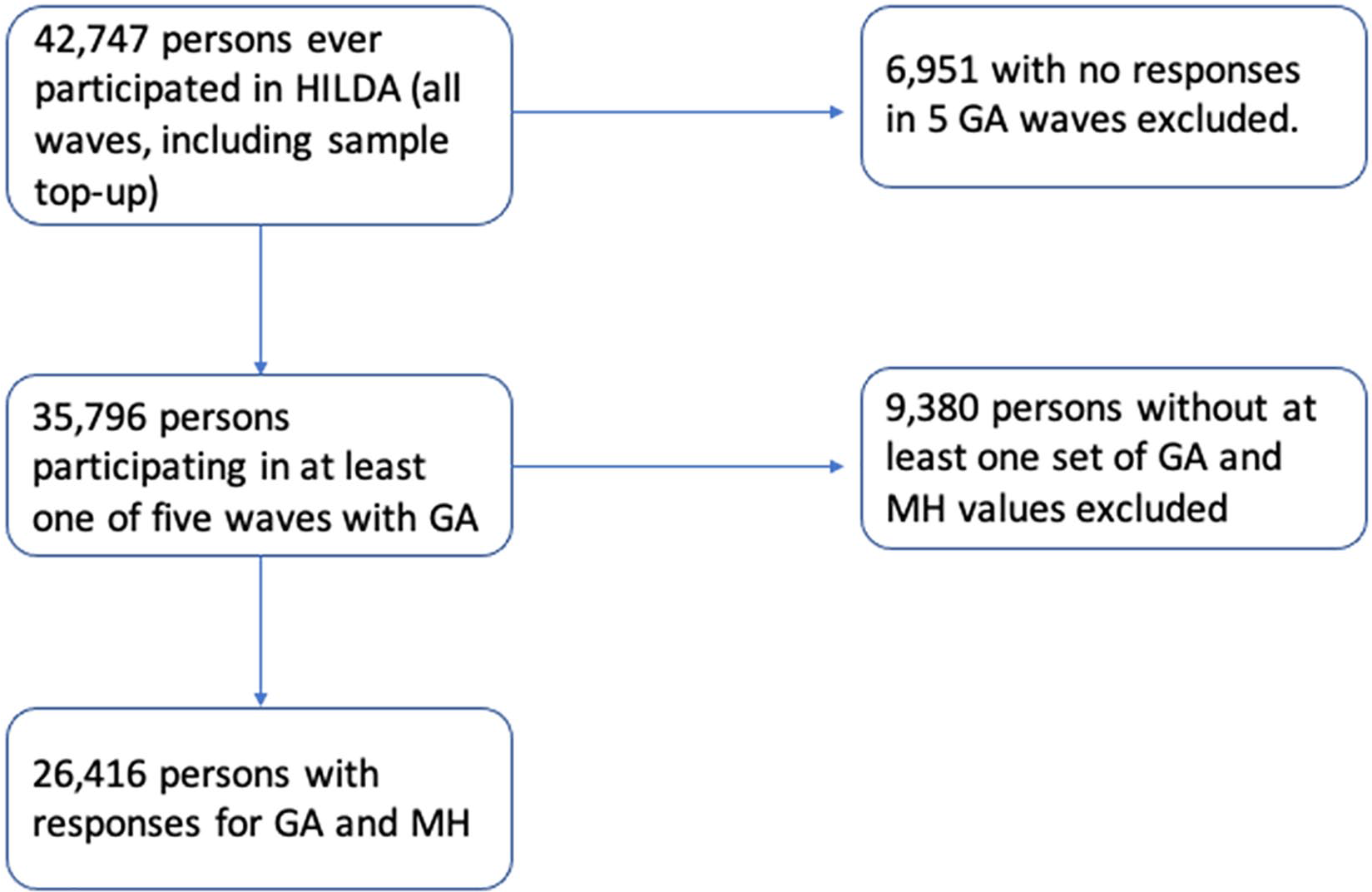
Sample selection.
Exposure variable
A composite measure of gender attitudes was derived from six items that assessed attitudes and beliefs about the appropriate and acceptable roles of men and women. The HILDA Survey contains 16 closely related questions on gender attitudes, collected in Waves 1, 5, 8, 11 and 15. Many of these questions are the obverse of another (replacing mother for father, woman for man) or aim at the same phenomena (multiple questions about the effects on children of having mothers work). Following Perales et al. (2017), we focused upon six conceptually distinct questions:
(a) Many working mothers seem to care more about being successful at work than meeting the needs of their children.
(b) If both partners in a couple work, they should share equally in the housework and care of children.
(c) Whatever career a woman may have, her most important role in life is still that of being a mother.
(d) Mothers who do not really need the money should not work.
(e) Children do just as well if the mother earns the money and the father cares for the home and the children.
(f) A working mother can establish just as good a relationship with her children as a mother who does not work for pay.
Respondents were instructed to indicate their endorsement of these statements on a scale of (1) (‘strongly disagree’) to (7) (‘strongly agree’), with only the two extreme categories labelled. Items b, e and f were reverse coded, so that higher scores indicated more traditional gender attitudes.
Following the precedent of other work in HILDA (Perales et al., 2017), these items were summed, and rescaled to a range of 0–100. This transformation does not alter the statistical properties of the measure, but eases its interpretation. On this scale, the relationship between gender attitudes and mental health was strong and non-linear. Supplementary Figures 1 and 2 show the distribution of attitudes on the 0–100 scale. We created smoothed plots of the relationship between gender role attitudes and mental health using the Lowess method of moving averages. The Lowess approach explicitly enables the examination of non-linear patterns of data (Cleveland, 1979), and by doing this, facilitates the identification of cut-points. Using this method, gender attitudes were categorised using cut-offs identified as the points at which the Lowess curve moved outside the 95% confidence intervals (CIs) of the predicted linear model (Simonoff, 1996). This led to four categories: egalitarian (0–22), moderate-egalitarian (23–44), moderate-traditional (45–74) and traditional (75–100). The traditional category included only 1.4% of respondents and so for the regression analyses, this was combined with moderate-traditional to form a category hitherto referred to as ‘traditional’.
Outcome variable
Mental health was assessed using the 5-item Mental Health Inventory (MHI-5), a subscale from the Short Form-36 (SF-36) general health measure. As part of the MHI-5 respondents are asked to rate their symptoms of depression and anxiety (nervousness and depressed affect) and positive aspects of mental health (feeling calm and happy) in the past 40 weeks. The MHI-5 is widely considered to be an effective screening instrument for mood disorders or severe depressive symptomatology in the general population (Rumpf et al., 2001), and has been validated as a measure for depression (Rumpf et al., 2001). Responses to the five-items are summed to produce a continuous score on a scale of 0–100, with higher scores indicating better mental health. To minimise reverse causation and maximise theorised temporal sequencing between gender attitudes and mental health, the mental health measures were taken from the wave following the collection of gender attitudes (i.e. we utilised Waves 2, 6, 9, 12 and 16 of mental health data).
Covariates
Several variables were identified as plausible common causes of gender attitudes and mental health. Failure to adjust for these variables could lead to the over estimation or under estimation of the measure of association (Rothman and Greenland, 1998) between the exposure (gender attitudes) and the outcome (mental health). Identified covariates were therefore included in the models to control for potential bias due to confounding. These were as follows: country of birth (Australia, other English speaking country and non-English speaking other country), age group (15–24, 25–34, 35–44, 45–54, 55–64, 65 and older), area of residence (major cities, inner regional and outer regional/remote), employment (employed, unemployed and not in labour force), year (continuous), highest education level attained (tertiary, certificate/diploma, high school and did not complete high school) and household income (quintiles) (ABS, 2019).
Imputation
HILDA is internationally distinctive for its high retention rates. Nevertheless, as with many longitudinal surveys, HILDA suffers from some missing data due to loss to follow-up. Assuming the values were missing at random, multiple imputation using chained equations was performed with the ‘mice’ package in R. Given the high frequency of missingness, a total of 50 imputed data sets were created, and the statistical models were fitted to each. Estimates of the parameter values defining the models were generated by the application of Rubin’s rules (Rubin, 1986), which account for the variability of the imputed values.
Statistical analysis
A linear mixed model was used to estimate the effect of gender attitudes on mental health. A random intercept was used to accommodate any within-participant correlation of outcomes due to repeated measures. Linear mixed models allow for unequal time periods between measures (Verbeke and Molenberghs, 2009), including the possibility of missing data, and do not, therefore, require participants to contribute longitudinal data that are identical in structure.
In sensitivity analysis, we also applied a within-groups fixed effects model to check for the existence of shared unmeasured confounding and found the results closely matched those of the random effects model. As noted above, to delineate the causal ordering of key variables, mental health measures were taken from the wave following that in which gender attitudes were surveyed. Thus, at each of the five waves, gender attitudes preceded the mental health measure. All analyses were conducted in R (version 4.0).
Results
Table 1 displays the descriptive characteristics of the sample. Most respondents were born in Australia and lived in urban areas. While most respondents were employed, a larger proportion of women than men were not in the labour force (38.5% compared to 26.1%), and a larger proportion of men were employed than women (67.6% compared to 56.5%). In terms of the highest level of education, certificate/diploma was the most common category for men (39.1%), while for women, the largest proportion had not completed Year 12 (high school, 33.6%). Slightly more women than men reported having a tertiary qualification (20.4% compared to 17.0% of men). The sample was slightly over-represented in the lowest income quintile (26.4%, compared to 13.7% in the highest income quintile).
Baseline characteristics of individuals included in sample from the Household, Income and Labour Dynamics in Australia Survey.
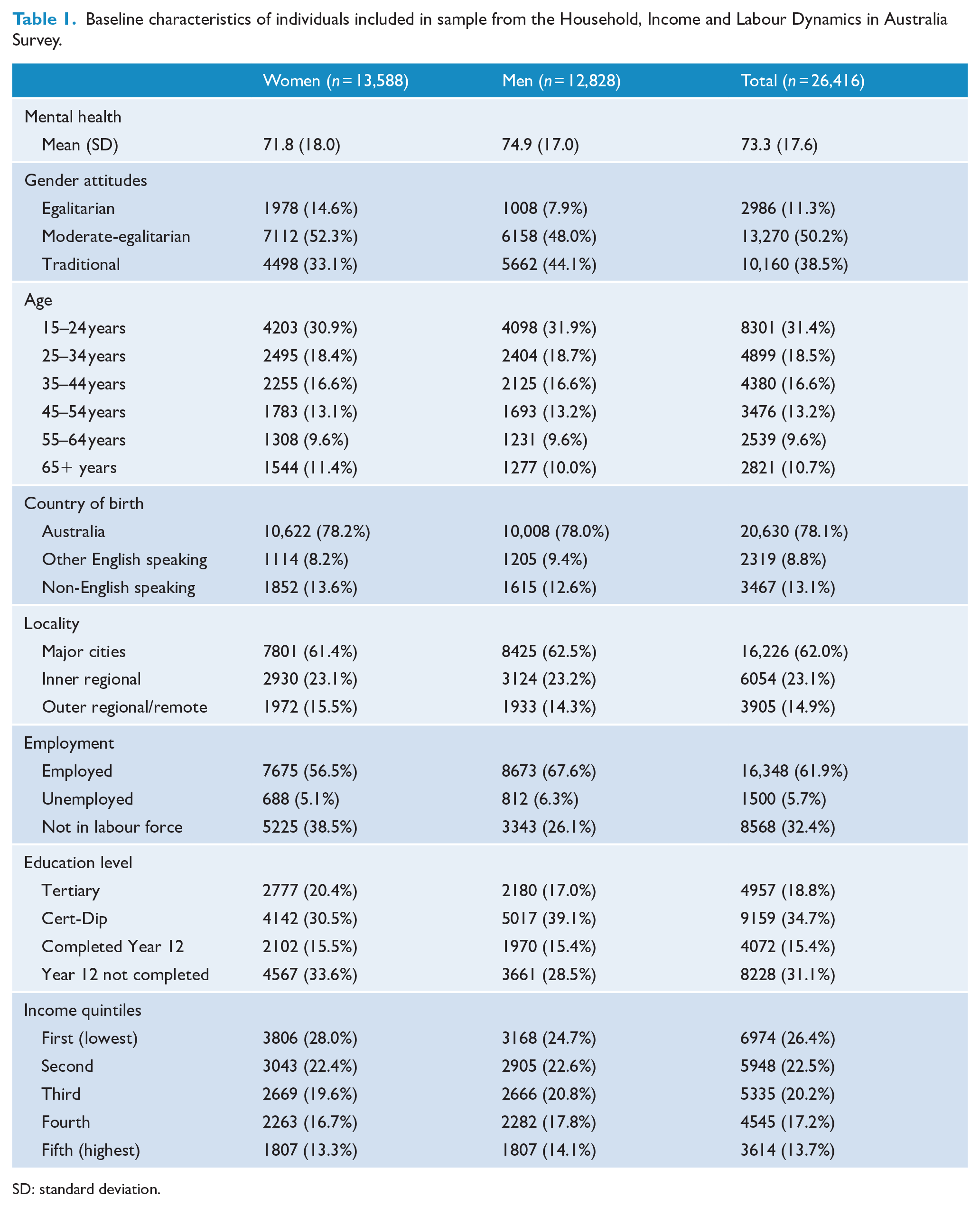
SD: standard deviation.
Mean mental health scores for women were poorer than those for men (71.8 and 74.9, respectively), and a higher proportion of women expressed egalitarian gender attitudes compared to men (14.6% and 7.9%, respectively). Results of the linear mixed model are displayed in Table 2. For both women and men, egalitarian gender attitudes were associated with better mental health. Among women, those with moderate-egalitarian attitudes had poorer mental health compared to those with egalitarian attitudes (estimated mean difference = −0.78, 95% CI = [−1.34, −0.22]). Those with traditional attitudes had the poorest mental health (−1.91, 95% CI = [−2.55, −1.26]). There was also strong evidence of a difference in mental health between moderate-egalitarian and traditional females (−0.814, 95% CI = [−0.32, −1.30]).
Regression results a : associations between gender attitudes mental health and n = 13,588 women and n = 12,828 men across Waves 1, 5, 8, 11 and 15 (years 2001, 2005, 2008, 2011 and 2015) of the Household, Income and Labour Dynamics in Australia Survey.
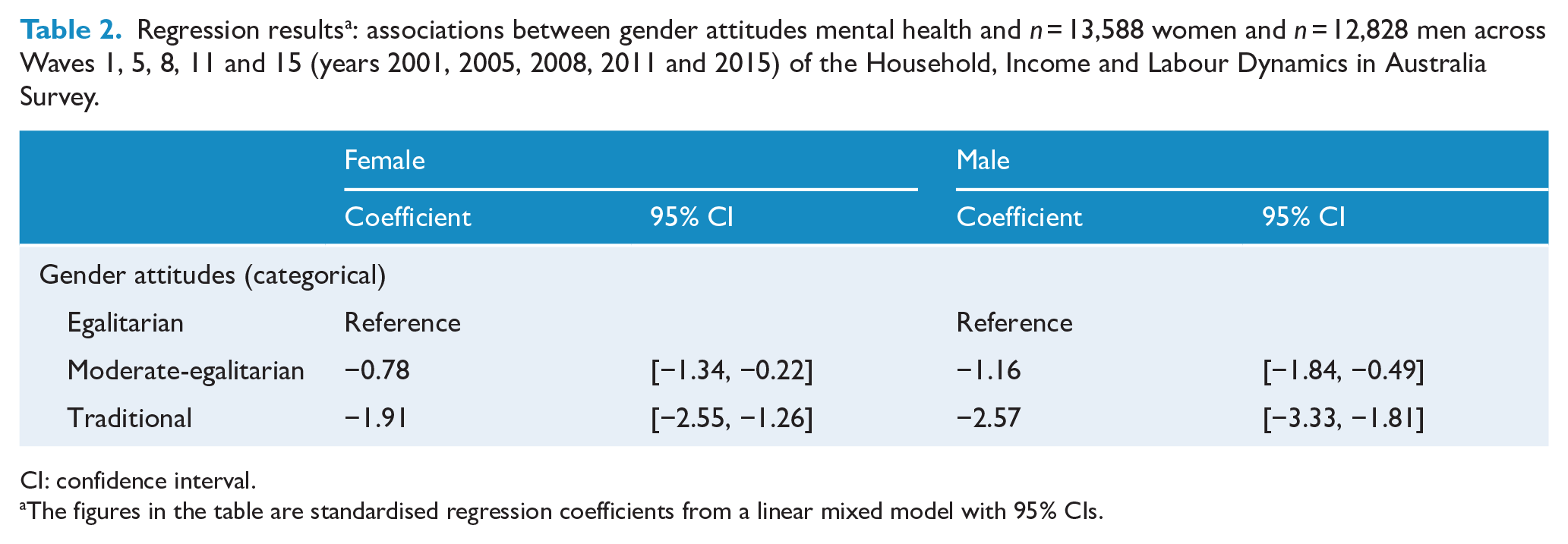
CI: confidence interval.
The figures in the table are standardised regression coefficients from a linear mixed model with 95% CIs.
Among men, increasing traditionalism in gender attitudes was associated with increasingly poor mental health. Those with traditional gender attitudes had the poorest mental health compared to those with egalitarian attitudes (−2.57, 95% CI = [−3.33, −1.81]). Moderate-egalitarian views were also associated with poorer mental health compared to men with egalitarian attitudes (−1.16, 95% CI = [−1.84, −0.49]). For males, the mean difference in mental health scores between those holding moderate-egalitarian vs traditional views was greater than in women (−1.20, 95% CI = [−0.749, −1.64]).
Discussion
Consistent with the stated hypothesis, the results of this analysis indicate that egalitarian gender attitudes are associated with better mental health. For both men and women, a gradient was observed, with the poorest levels of mental health observed for those with traditional attitudes.
These results align with previous research showing that more egalitarian gender attitudes are associated with better mental health among adults (Sweeting et al., 2014) and adolescents (King et al., 2019). More broadly, the results for men are consistent with evidence that some elements of masculinity are associated with mental health (Milner et al., 2018) and suicidal behaviour among men and boys (Houle et al., 2008).
As in many parts of the world, the public health burden of poor mental health in Australia is substantial, and it is estimated that each year about 20% of adults experience a mental health problem (Australian Institute of Health and Welfare [AIHW], 2019). Improving gender attitudes across the population is not the ultimate panacea for improved mental health; however, the results suggest that if part of a broader approach, shifting gender attitudes towards egalitarianism may deliver population-level mental health gains.
The attitudes assessed here tap into normative beliefs about the roles and behaviours appropriate for men and women. Gender norms are recognised to be powerful determinants of health (Rao Gupta et al., 2019). Globally, gender norms etiolate the rights and entitlements of girls and women, and restrict the lives of all (Heise et al., 2019) – men and women and boys and girls. Gender norms are pervasively operationalised through the maintenance and perpetuation of sets of hierarchies that privilege masculinity, and what it is to be male, over what it is to be female (Heise et al., 2019).
We identify a number of potential pathways by which endorsement of egalitarian gender norms and attitudes might impart a positive effect on mental health (and traditional norms exert a detrimental effect on mental health), acknowledging that these may be different for men and women. It is important to note that the items used to measure gender attitudes in this analysis broadly tapped into attitudes regarding the division of paid and unpaid work, and parental and work responsibilities. While the results do not indicate the extent to which these attitudes about gender roles align with behaviours, gender differentiated division of roles may represent important pathways through which traditional gender attitudes lead to poor mental health, particularly for women.
The act of juggling multiple tasks and roles exerts considerable time-pressure and stress for women (Pocock et al., 2013). There is evidence that differential exposure to work and family stressors is a key factor underpinning the fact that women have higher rates of depression than men (Marchand et al., 2016). It is possible that women with more egalitarian attitudes may be able to negotiate and seek family and work arrangements that support their normative position; there is some evidence that egalitarian attitudes are associated with a more equal division of household labour (Aassve et al., 2014).
For men, it is possible that endorsement of traditional gender attitudes reflects broader endorsement of traditional masculine norms which are known to be associated with poorer mental health. Traditional or hegemonic masculinity reifies emotional containment, self-reliance and stoicism, and a repudiation of help-seeking – factors that may be disadvantageous in times of stress or distress. It is also known that men who endorse traditional gender attitudes are less likely to take an active role in caring for children (Scambor et al., 2012). It is theorised that partaking in more caring roles within the home, particularly for small children can deliver health benefits, fostering healthy behaviours and precluding unhealthy behaviours (Månsdotter et al., 2006).
One explanation previously advanced (Hunt et al., 2006), applicable to both men and women, is that as society becomes more explicitly embracing of gender equality, those who hold traditional ideologies may find their views dissonant to broader society. This dissonance may exert a mental health penalty. Hunt and Sweeting also speculate that it is possible that endorsing traditional views may be indicative of an underlying trait associated with inflexibility and resistance or a maladaptive response to social change (Hunt et al., 2006).
It is also important to consider these results in the context of global trends, as well as the Australian political and social context. Advancing gender equality remains a key objective of governments and agencies in many countries, yet there is still considerable work to be done. Even countries at the forefront of gender equality progression such as Iceland and Norway, lauded for their continued and steady commitment to gender equality, sustain overall gender gaps of between 12% and 16% (World Economic Forum, 2020). Australia, ranked 44 on the World Economic Forum’s international ranking, has reduced its overall gender gap to 27% (World Economic Forum, 2020).
As noted, the gender attitudes captured here reflect attitudes to roles and responsibilities of men and women. Gender norms and inequalities are powerful determinants of health and well-being. They shift over time, and are malleable. Given the economic and social importance of participating in the labour market, female labour force participation is considered to be a vital component of gender equality (Mandel, 2009). Initiatives that enable and support female labour force participation, not only by enabling the entry, re-entry and retention of women in the labour force, but also redistributing their unpaid responsibilities, may deliver greatest gains in supporting change in gender attitudes and norms. We also note that COVID-19 strengthens the impetus to consider these associations. COVID-19 may offer the opportunity to catalyse substantial changes to traditional gender roles and responsibilities, potentially reshaping our gender systems to improve gender equality (King et al., 2020). Depending on how we navigate this however, COVID-19 may lead to the entrenchment of existing norms: in previous economic crises, increasing endorsement of traditional gender attitudes has been observed (Kushi and McManus, 2018).
Strengths and limitations
There are some strengths and limitations of this analysis. As a first point, the data were drawn from a large, population representative sample of individuals over the age of 15 years. Statistical precision was maximised by utilising data collected at five time points across 17 years. Using mental health variables in the wave following the collection of gender attitudes, we were able to define the theorised temporal ordering between exposure and outcome.
As a limitation, the measure of mental health used here was self-reported, and thus may be vulnerable to reporting bias. In addition, despite being a well-validated measure, the MHI-5 scores do not have accepted clinical meaning. As with many surveys of this kind, migrants/new Australians, and more economically disadvantaged groups are under-represented in HILDA (Summerfield et al., 2019). Furthermore, the gender attitudinal items assessed here are not part of a validated scale, and do not comprehensively reflect gender attitudes and norms, focusing instead on attitudes to paid and unpaid roles and work and parenting responsibilities. Despite this, the items used here are identical, or very similar, to items used in other surveys around the world, and we applied robust methods (novel in their application) to define the categories here. Finally, we note that the egalitarian group was substantially smaller than the other groups. One potential implication of this is reduced statistical power, which could result in estimate imprecision and type II errors – i.e. a failure to observe a relationship in the sample that exists in the population. Reassuringly, the coefficient on this smaller egalitarian group was consistently statistically significant.
Conclusion
In summary, using a population representative sample, this paper demonstrates that egalitarian attitudes are associated with better mental health for both men and women. These results have clear population health implications. Initiatives that support egalitarian gender attitudes may be beneficial in ways not previously anticipated, with mental health among women as well as men, appearing to be optimised when gender egalitarian attitudes are endorsed.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211031488 – Supplemental material for Traditionalism vs egalitarianism: Is there an association between gender attitudes and mental health?
Supplemental material, sj-docx-1-anp-10.1177_00048674211031488 for Traditionalism vs egalitarianism: Is there an association between gender attitudes and mental health? by Tania King, Francisco Perales, Ankur Singh, Lyle Gurrin and Bradley Crammond in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674211031488 – Supplemental material for Traditionalism vs egalitarianism: Is there an association between gender attitudes and mental health?
Supplemental material, sj-docx-2-anp-10.1177_00048674211031488 for Traditionalism vs egalitarianism: Is there an association between gender attitudes and mental health? by Tania King, Francisco Perales, Ankur Singh, Lyle Gurrin and Bradley Crammond in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Australian Research Council Linkage Project: Gender equality in Australia: impact on social, economic, and health outcomes (LP 180100035). TK is the recipient of an Australian Research Council Discovery Early Career Researcher Award Fellowship (DE200100607).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.