
Abstract
Objective:
Neurocognitive impairment is considered a core feature of mood disorders. Research has shown that neurocognitive impairment often persists beyond mood symptom resolution and can have significant deleterious effects on interpersonal relationships, academic achievement, occupational functioning and independent living. As such, neurocognitive impairment has become an important target for intervention. In this systematic review, we aimed to examine the extant literature to ascertain whether current standard evidence-based psychotherapies can improve neurocognitive functioning in mood disorders.
Method:
Studies examining changes in neurocognitive functioning following evidence-based psychotherapy were identified using MEDLINE, PsycINFO and Web of Science databases. Given the heterogeneity of study procedures, treatment protocols and patient samples, a narrative rather than meta-analytic review technique was employed.
Results:
Nineteen studies (21 articles) met inclusion criteria. There was preliminary evidence of improved executive functioning following evidence-based psychotherapy for Major Depressive Disorder and Bipolar Disorder. There was also some signal of reduced negative biases in emotional information processing following psychotherapy in depression. Due to methodological variability across studies however, it was difficult to draw clear conclusions.
Conclusion:
Findings from the current review suggest that evidence-based psychotherapies may influence some aspects of neurocognitive functioning in mood disorders. This continues to be an ongoing area of importance and warrants further research.
Introduction
Neurocognitive impairment has become increasingly recognised as a core feature of mood disorders (Porter et al., 2015; Robinson et al., 2006; Rock et al., 2014). Indeed, difficulties with poor concentration, indecisiveness and distractibility are included in the DSM-5 classification of mood disorders (American Psychiatric Publishing, 2013). Evidence suggests that deficits are variable (Burdick et al., 2014; Douglas et al., 2018) and can be widely distributed across cognitive domains, including ‘cold’ neurocognitive functions such as executive function, attention, learning and memory, and psychomotor speed, as well as ‘hot’ neurocognitive functions involving emotional processing (Porter et al., 2015). While mood symptomatology is undoubtedly a contributing factor, a substantial body of research suggests that cognitive deficits persist well into remission (Bora et al., 2013; Robinson et al., 2006; Semkovska et al., 2019). Neurocognitive impairment has been strongly linked to poorer functional outcomes in mood disorders (Depp et al., 2012; Gupta et al., 2013; McIntyre et al., 2013) and there is preliminary evidence that such deficits can predict the likelihood of relapse (Majer et al., 2004; Schmid and Hammar, 2013). As such, neurocognitive impairment has become an important target for intervention.
Data from pharmacological studies suggest that in many cases, there may be a disconnect between resolution of mood episodes and non-emotional or ‘cold’ neurocognitive functions (Shilyansky et al., 2016). In contrast, it has been suggested that changes in emotional processing i.e. ‘hot’ neurocognitive functions, may be necessary for the resolution of mood symptomatology (Godlewska and Harmer, 2020; Harmer et al., 2009). Given the suggested link between changes in emotional processing and recovery from depression, and the link between neurocognitive impairment and functional outcomes in mood disorders, there is increasing interest in elucidating the effectiveness of current treatments in altering both non-emotional and emotional aspects of neurocognitive functioning. Indeed, the effects of pharmacotherapy on these areas have been the subject of several reviews (Keefe et al., 2014; Rosenblat et al., 2016; Wagner et al., 2012). While there is increasing research into cognitive remediation therapies, which are specifically designed to improve neurocognitive functioning, there has not yet been a systematic review examining current standard evidence-based psychological therapies and their effects on neurocognitive function in mood disorders.
Current treatment guidelines recommend several evidence-based psychotherapies (e.g. Cognitive Behavioural Therapy, Interpersonal Therapy) as first line treatment for Major Depressive Disorder (MDD). Within Bipolar Disorder (BD), evidence-based psychotherapies (e.g. Interpersonal Social Rhythms Therapy, Family-Focused Therapy) have also been recommended as adjuncts to pharmacotherapy, with the aim to address bipolar depression, ameliorate residual symptomatology, reduce relapse risk and improve overall quality of life and functioning (Malhi et al., 2021). While these evidence-based psychotherapies are efficacious in improving various aspects of mood symptomatology, and in some cases general functioning, the question remains as to whether they lead to changes in neurocognitive functioning. This has important practical implications. For example, if evidence-based psychotherapies improve neurocognitive function to a greater extent than the pharmacotherapy with which they are often used adjunctively, then this would add to recommendations suggesting that the two forms of therapy should be combined, particularly when there is significant neurocognitive impairment.
Therefore, the aim of this systematic review is to examine the extant literature to ascertain whether evidence-based psychological therapies are associated with improvements in neurocognitive functioning in MDD and BD. There may be some debate regarding which psychotherapies for mood disorder are currently ‘evidence based’; therefore, we used the current accepted treatment guidelines in our countries of practice as a guide (Malhi et al., 2021; Parikh et al., 2016; Yatham et al., 2018). While there is emerging evidence supporting the efficacy of cognitive remediation therapies in mood disorders, they are not yet recommended as ‘evidence based’ in the aforementioned treatment guidelines and are thus, beyond the scope of the current review.
Methods
Protocol and registration
Details of the protocol for this systematic review were registered on Prospero (CRD42020206536) and can be accessed at https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=206536
Search strategy
Up to 1 May 2020, a systematic review of electronic databases was carried out for relevant papers using MEDLINE, PsycINFO and Web of Science. In the initial search, the following search items were used: ‘mood disorders’ or ‘major depression’ or ‘depression’ or ‘bipolar disorder’ and ‘cognitive function*’ or ‘neuropsychological function*’ or ‘executive function*’ or ‘memory’ and ‘psychological treatment’ or ‘psychotherapy’. To ensure inclusion of all available articles, reference lists of all relevant papers were checked for additional pertinent studies. Moreover, citations of relevant articles were followed through Web of Science to enable the inclusion of more recent publications. Due to the extended time-frame between initial search and submission, the search was updated to April 2021 to capture any additional articles. No additional articles were found through this process.
Inclusion criteria
Inclusion criteria were as follows:
Interventional studies where neurocognitive testing was conducted before and after psychological treatment. Only evidence-based psychological therapies were considered for review. We focused on the psychological therapies that have the most robust evidence base and which are currently recommended in treatment guidelines where the authors practice (Malhi et al., 2021; Parikh et al., 2016; Yatham et al., 2018). The following psychological therapies for MDD were considered for review: Cognitive Behavioural Therapy (CBT), Interpersonal Therapy, Mindfulness-based Cognitive Therapy (MBCT), Acceptance and Commitment Therapy, Problem-solving Therapy, Behavioural Activation Therapy, Short term Psychodynamic Therapy and Non-directed Supportive Therapy (Malhi et al., 2021; Parikh et al., 2016). The evidence-based psychological therapies for BD considered for review were the following: CBT, Psychoeducation, Interpersonal Social Rhythms Therapy (IPSRT) and Family-Focused Therapy (Malhi et al., 2021; Yatham et al., 2018).
Adult participants.
Sample including individuals with a diagnosis of MDD or BD (I, II or NOS).
Exclusion criteria
Reasons for exclusion were the following:
Follow-up neurocognitive functioning data not reported after psychological treatment (no studies).
The use of a patient sample with comorbid major medical, neurological or endocrinological conditions (n = 1).
Inclusion of individuals scoring <24 on a Mini Mental Status Exam (no studies).
All studies were limited to English-language publications.
Full study review
The current review was undertaken using the recommended PRISMA guidelines and the PRISMA statement to help guide the search, screening and extraction process (Moher et al., 2009). Titles and abstracts were screened by the primary author, who also examined the full texts of the studies that passed initial screening to determine if they still met inclusion criteria. If inclusion was unclear, a discussion between co-authors resolved this issue. The following data were extracted: (1) characteristics of the sample, including sample size, average age, baseline mood severity; (2) study design; (3) psychological treatment utilised; (4) cognitive tests employed before and after psychotherapy and (5) study outcomes. In each case, the method by which the study controlled for practise effects was also noted.
Assessment of risk of bias
Each randomised controlled trial (RCT) included in the current review was assessed for risk of bias using the Cochrane Collaboration’s tool for assessing risk of bias (Higgins et al., 2019). Risk of bias was assessed by two authors (SG and RP) independently with subsequent discussion where necessary to reach a consensus. The Cochrane risk of bias tool assesses the following domains: Selection Bias, Performance Bias, Detection Bias, Attrition Bias, Reporting Bias and Other Bias. Studies were then assessed as having a low risk of bias, unclear risk of bias or high risk of bias. Non-RCTs were automatically categorised as having a high risk of bias. Due to the limitations of the Cochrane Risk of Bias Tool in assessing risk of bias for studies examining psychotherapies, we also assessed factors that may influence risk of bias which are specific to psychotherapy trials. Such factors include manualisation of therapy, measurement of fidelity and the use of an active control group versus Treatment as Usual (TAU) or waitlist control (Kisely, 2020; see Supplemental Table 1).
Studies examining the effects of evidence-based psychotherapies on neurocognitive function in MDD and BD.
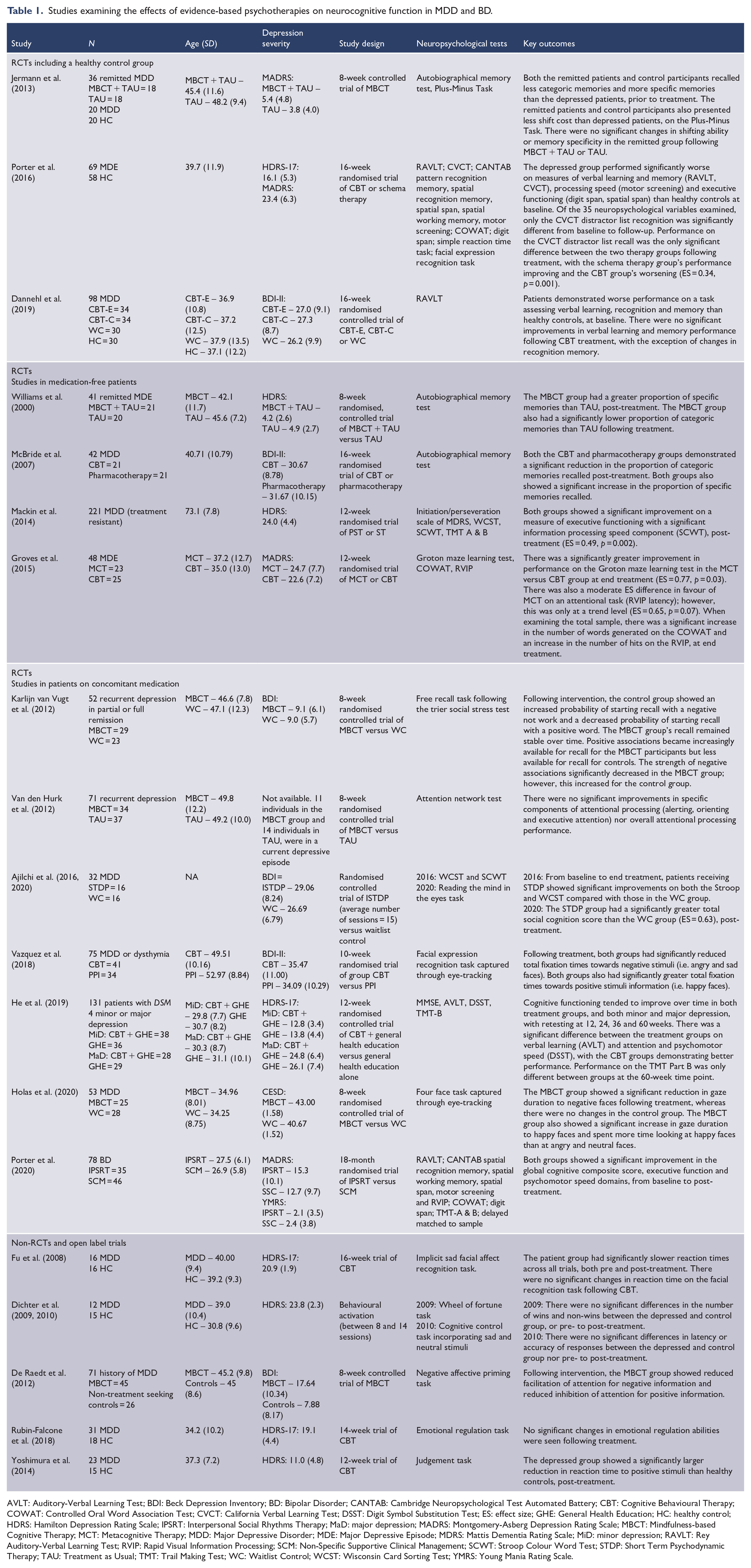
AVLT: Auditory-Verbal Learning Test; BDI: Beck Depression Inventory; BD: Bipolar Disorder; CANTAB: Cambridge Neuropsychological Test Automated Battery; CBT: Cognitive Behavioural Therapy; COWAT: Controlled Oral Word Association Test; CVCT: California Verbal Learning Test; DSST: Digit Symbol Substitution Test; ES: effect size; GHE: General Health Education; HC: healthy control; HDRS: Hamilton Depression Rating Scale; IPSRT: Interpersonal Social Rhythms Therapy; MaD: major depression; MADRS: Montgomery-Asberg Depression Rating Scale; MBCT: Mindfulness-based Cognitive Therapy; MCT: Metacognitive Therapy; MDD: Major Depressive Disorder; MDE: Major Depressive Episode; MDRS: Mattis Dementia Rating Scale; MiD: minor depression; RAVLT: Rey Auditory-Verbal Learning Test; RVIP: Rapid Visual Information Processing; SCM: Non-Specific Supportive Clinical Management; SCWT: Stroop Colour Word Test; STDP: Short Term Psychodynamic Therapy; TAU: Treatment as Usual; TMT: Trail Making Test; WC: Waitlist Control; WCST: Wisconsin Card Sorting Test; YMRS: Young Mania Rating Scale.
Results
Nineteen studies (21 publications) met inclusion criteria (see Figure 1 for PRISMA flow diagram of studies retrieved for review). Of the 19 studies, nine studied CBT, six studied MBCT, one studied Behavioural Activation Therapy, one studied Problem Solving Therapy and Non-directed Supportive Therapy, one studied Short-Term Psychodynamic Therapy and one studied IPSRT (see Table 1). Given the heterogeneity of cognitive tests used, the varying treatment protocols and the differing sample characteristics, it was only possible to use a narrative rather than meta-analytic review technique. However, where possible, we have indicated treatment effect sizes. In the sections that follow, studies will be discussed according to study methodology. Specifically, we will first discuss RCTs that included a healthy control group, followed by RCTs without a healthy control group (studies in medication-free patients, studies in patients on concomitant medication), and last discuss non-RCTs and open label trials. Within each section, findings will be further divided by treatment modality.
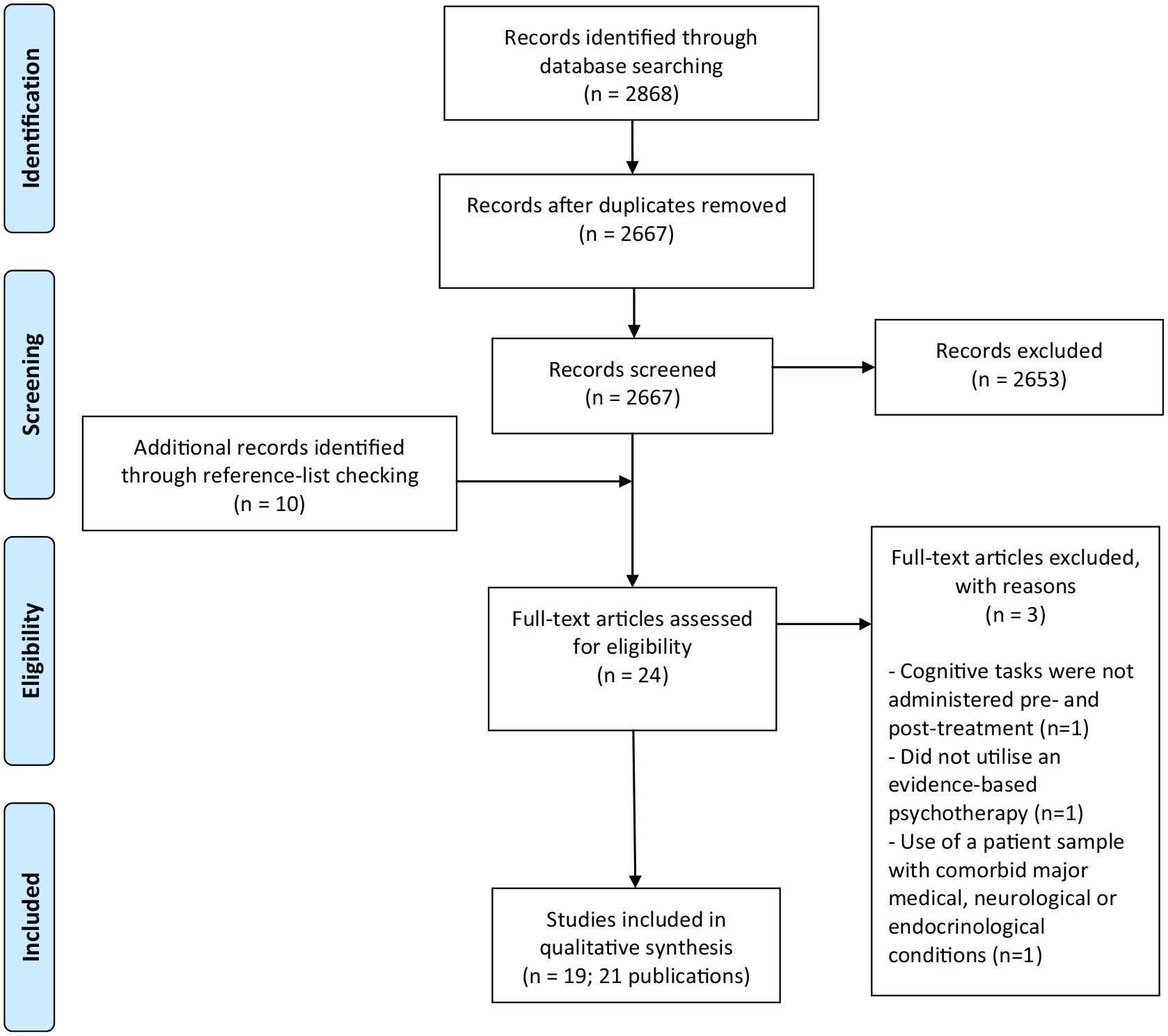
PRISMA flow diagram of article selection process.
Risk of bias
Most RCTs included in the current review were assessed as having ‘unclear’ risk of bias as it is not possible to blind participants in psychotherapy trials. Five RCTs were assessed as high risk of bias due to issues including inadequate allocation concealment, attrition bias and/or selective reporting (see Table 2).
Assessment of risk of bias for RCTs included in review.
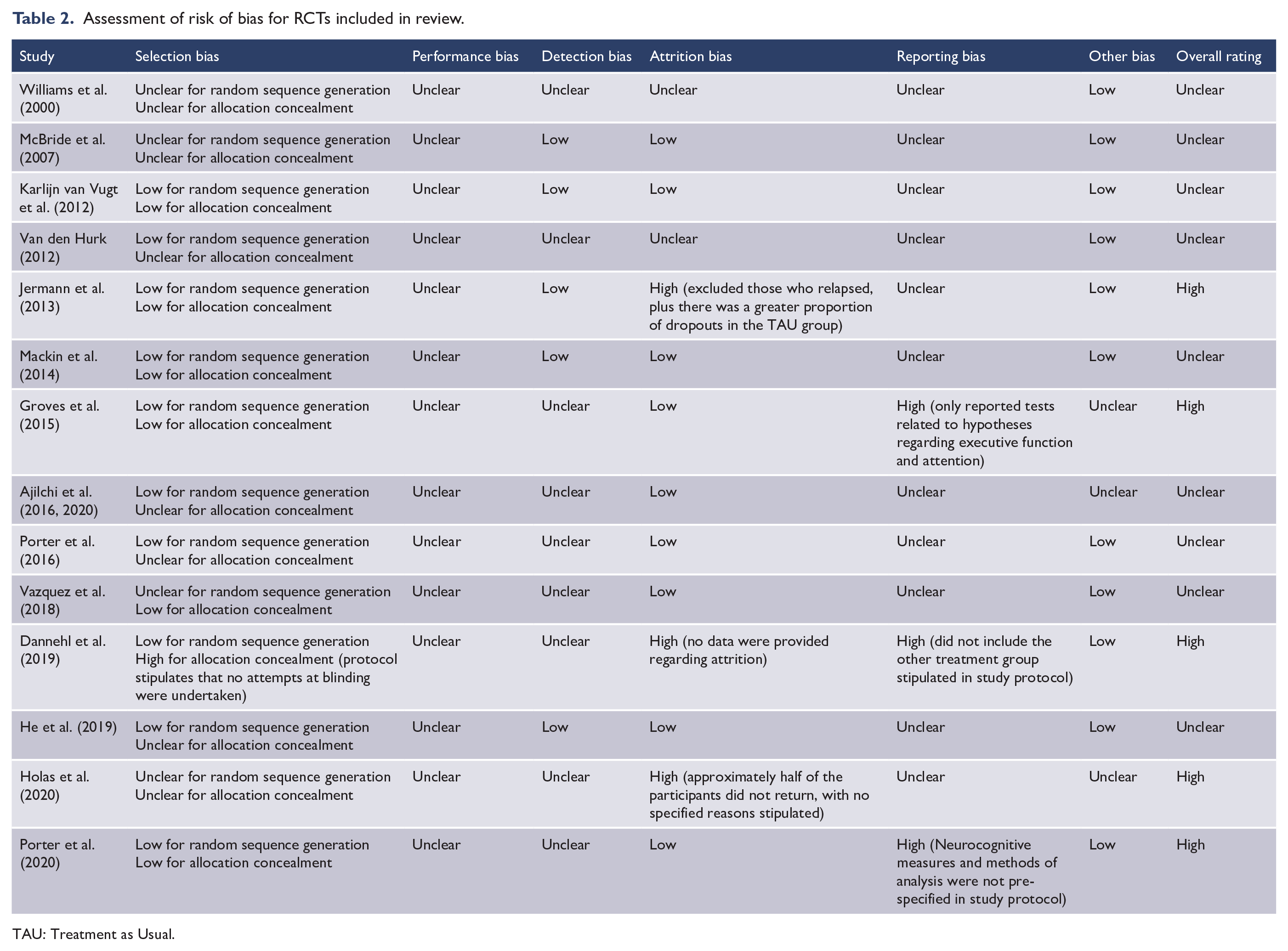
TAU: Treatment as Usual.
Randomised controlled trials including a healthy control group
Three reviewed studies incorporated a healthy control group, with one including healthy controls at baseline and follow-up. Porter et al. (2016) examined the effects of CBT versus Schema Therapy on ‘hot’ and ‘cold’ neurocognitive functions in individuals experiencing a Major Depressive Episode (MDE). The patient sample included 69 medication-free patients with a diagnosis of MDD (93%) or BD-II (7%). Healthy control participants were assessed at baseline and follow-up to help determine the extent of neurocognitive impairment in the patient sample at baseline and to control for familiarity or practise effects. While depressive symptomatology was shown to improve after 16 weeks of psychotherapy, the authors found no convincing evidence of neurocognitive improvement following CBT or Schema Therapy, when compared with healthy controls. Specifically, only one out of 35 neuropsychological variables was shown to improve following psychotherapy (California Verbal Leaning Test distractor list, ES = 0.34, p = 0.001). There were no significant differences between the CBT and Schema Therapy groups, post-treatment.
Dannehl et al. (2019) examined the effects of CBT on verbal learning and memory in 98 patients with MDD. Participants were randomly assigned to CBT with an exercise focus (CBT-E), pleasurable low-energy activities (CBT-C), or passive waitlist control. While the patient group had significantly poorer verbal learning, memory and recognition than healthy control participants at baseline, there were no significant improvements in verbal learning and memory following either form of CBT.
Jermann et al. (2013) examined the effects of MBCT on neurocognitive functioning in individuals remitted from a MDE. Participants were randomised to either 8 weeks of MBCT or TAU; the latter, including unrestricted access to any type of treatment, including medication. The authors found no significant changes in memory specificity (Autobiographical Memory Test) or shifting ability (Plus-Minus task) in the MBCT or TAU groups. It is important to note, however, that there were no significant differences in cognitive performance between the remitted depressed patients and healthy control participants prior to intervention.
Randomised controlled trials
Studies in medication-free patients
Four studies examined the effects of psychotherapy on ‘cold’ neurocognitive processes in medication-free patient samples. In the largest study reviewed, Mackin et al. (2014) conducted a 12-week RCT of Problem Solving Therapy versus Non-directed Supportive Therapy in a sample of older adults with MDD (n = 221) who had significant executive dysfunction; determined by screening performance on the Initiation or Perseveration index of the Mattis Dementia Rating Scale and the Stroop Word Color Test. Both treatment groups showed significant improvements on a measure of executive functioning (Stroop Colour Word Test) following treatment (ES = 0.49, p = 0.002). There were no other significant changes in neurocognitive performance.
Two of the four medication-free studies examined the effects of CBT on neurocognitive functioning. Groves et al. (2015) conducted a 12-week RCT of CBT versus Metacognitive Therapy in a sample of patients experiencing a MDE (n = 48; included MDD, BD-II, BD-NOS). The Metacognitive Therapy group showed a significantly greater reduction in the total number of errors on the Groton Maze Learning Test (a measure of spatial working memory and attention) compared with the CBT group (ES = 0.77, p = 0.03). More specifically, while the Metacognitive Therapy group showed a significant reduction in the total number of errors, the CBT group did not. McBride et al. (2007) examined the effects of CBT versus pharmacotherapy on autobiographical memory in a group of individuals with MDD (n = 41). Following 16 weeks of intervention, the CBT group showed a significant reduction in the proportion of categorical memories recalled and a significant increase in the proportion of specific memories recalled, indicating a significant reduction in the over-generality of memories. However, this reduction was not significantly different from that observed in the pharmacotherapy group.
Williams et al. (2000) examined the effects of MBCT on autobiographical memory, in individuals who had remitted from a MDE (n = 41). Participants were randomly assigned to MBCT and TAU or TAU alone; the latter group remaining under the care of their physician. Following treatment, the MBCT + TAU group recalled a significantly greater proportion of specific memories than those receiving TAU alone. The MBCT group also recalled a significantly lower proportion of categorical memories than TAU pre- to post-treatment, indicating a significant reduction in the over-generality of memories.
Studies in patients on concomitant medication
Seven studies examined the effects of psychotherapy combined with ongoing appropriate pharmacotherapy, on neurocognitive functioning. Two reviewed studies examined the effects of CBT, with one examining changes in ‘cold’ functions and the other examining ‘hot’ neurocognitive processes. He et al. (2019) reported the effects of CBT and General Health Education (GHE) versus GHE alone, on a range of neuro cognitive functions in patients with DSM-IV minor or major depression. Neurocognitive function improved over time in both treatment groups, with retesting completed at 12, 24, 36 and 60 weeks. There was a significant difference between treatment groups on verbal learning (Auditory-Verbal Learning Test) and attention and psychomotor speed (Digit Symbol Substitution Test), with the CBT groups demonstrating better performance at subsequent time points. Performance on Trail Making Part B was only different between groups at the 60-week time point. Analysis of change in cognitive performance from baseline was not conducted.
Vazquez et al. (2018) examined the effects of CBT versus a positive psychology intervention (n = 75) on attentional biases towards emotional information in MDD and dysthymia. Captured through eye-tracking, both groups showed a significant reduction in the total time of fixations towards negative stimuli (i.e. sad and angry faces) and a significant increase in the total time of fixations towards positive stimuli (i.e. happy faces) following 10 weeks of treatment. No significant differences were found between the two groups.
Three studies examined the effects of MBCT on neurocognitive functioning; one examining ‘cold’ neurocognition and the other two examining aspects of ‘hot’ neurocognition. Van den Hurk et al. (2012) compared the effects of 8 weeks of MBCT versus TAU on attentional capacities in 71 individuals experiencing a MDE. Using the Attention Network Test, the authors found no significant improvements in specific components of attentional processing; specifically, alerting, orienting and executive attention, in either group. Moreover, there were no significant changes in overall attentional processing performance following treatment. The remaining two studies examined changes in emotional processing and showed evidence of significantly reduced negative information processing biases following MBCT compared with waitlist control (Holas et al., 2020; Karlijn van Vugt et al., 2012).
One study examined the effects of Short term Psychodynamic Therapy compared with waitlist control, on ‘hot’ and ‘cold’ neurocognitive functions in 32 individuals experiencing a MDE (Ajilchi et al., 2016, 2020). Patients receiving Short term Psychodynamic Therapy showed significant improvements on the Stroop Color Word Test and Wisconsin Card Sorting Test compared with waitlist control, post-treatment (ES ranging from 0.13 to 0.52). The treatment group also showed a significant increase in total social cognition scores, as measured by the Reading the Mind in the Eyes Task, compared with the waitlist control group (ES = 0.63, p = 0.01).
Only one study utilised a sample entirely comprised of individuals diagnosed with BD. Porter et al. (2020) examined the effects of IPSRT versus Non-specific Supportive Clinical Management on neurocognitive function in 78 young people (15–36 years) with BD in various mood states at study entry. Using a broad battery of cognitive tests, the authors found a significant improvement in the global cognitive composite score of the combined patient group, as well as improvements in domains of executive functioning and psychomotor speed, post-treatment. There were no statistical differences in domain scores between the two treatment groups.
Non-randomised and open trials
One reviewed study was a non-RCT, incorporating a non-treatment seeking control group. De Raedt et al. (2012) examined the effects of 8 weeks of MBCT on emotional information processing in a sample of individuals remitted from a MDE (n = 71). Using the Negative Affective Priming Task, the authors found that the facilitation of attention for negative information and the inhibition of attention for positive information were significantly reduced pre- to post-treatment in the MBCT group. In comparison, the inhibition of attention for positive information increased in the control group and there were no significant changes in the processing of negative information.
Four studies examined the effects of evidence-based psychotherapy on neurocognitive functioning in MDD utilising an open trial format. Three of the studies examined the effects of CBT on emotional processing in MDD. Using a self-referential processing task, Yoshimura et al. (2014) found that after 12 weeks of CBT, the depressed group showed a significant reduction in reaction time to positive stimuli, compared with healthy controls. Fu et al. (2008) and Rubin-Falcone et al. (2018) found no significant changes in performance on emotional processing tasks following CBT. Finally, a single study examined the effects of Behavioural Activation (Dichter et al., 2009, 2010) on ‘hot’ and ‘cold’ neurocognitive functions, finding no significant changes following treatment.
Correlation between changes in neurocognitive functioning and mood
Only two studies examined the relationship between changes in neurocognitive functioning and changes in mood symptom severity, pre- to post-treatment. Mackin et al. (2014) found a significant correlation between improved executive function performance and reduced depressive symptom severity, pre- to post-treatment. In contrast, Groves et al. (2015) found no significant correlation between changes in executive functioning and mood symptomatology following CBT and Metacognitive Therapy.
Discussion
Neurocognitive functioning has become increasingly recognised as an important target in the treatment of mood disorders, yet relatively few studies have investigated the effects of evidence-based psychological therapies on non-emotional and emotional aspects of neurocognitive functioning. Moreover, study methodologies and findings are heterogenous and sample sizes are small. In this context, it is difficult to draw clear conclusions from the literature as it stands to date.
Effects of psychotherapy on neurocognitive function
There was preliminary evidence of improved executive functioning following current standard evidence-based psychotherapy for MDD and BD. In the largest psychotherapy trial reviewed, Mackin et al. (2014) found significant improvements on a measure of executive functioning in older adults receiving Problem Solving Therapy or Non-directed Supportive Therapy for depression. It is noteworthy that the patient group was enriched for executive deficit, thereby addressing the issue of dilution of study findings by inclusion of cognitively unimpaired individuals. Indeed, there is evidence that baseline deficit is predictive of cognitive change with treatment (Barczyk et al., 2020; Miskowiak et al., 2016). However, it is also important to note that this was an isolated finding. The fact that only one aspect of neurocognitive functioning changed may mean that psychotherapy had a specific effect on one aspect of executive function, or that this particular aspect was more susceptible to practise effects. Alternatively, the change may have simply been a chance finding in the context of multiple comparisons. Because the study did not incorporate a healthy control group, it is difficult to differentiate therapy-induced change from practise effects.
It is noteworthy that the single study incorporating a healthy control group pre- and post-treatment showed little evidence of cognitive change, including executive functioning, following psychotherapy. Porter et al. (2016) found that only one of 35 neuropsychological variables significantly changed following CBT and Schema Therapy when compared with change in a healthy control group. Interestingly, a follow-up study revealed that only a proportion of the patient sample was cognitively impaired at study intake (Douglas et al., 2018). Therefore, it is possible that small to moderate changes were diluted by inclusion of individuals who were not cognitively impaired at baseline.
In addition to changes in executive functioning, there was some evidence of changes in emotional information processing following psychotherapy for MDE, particularly the attenuation of negative biases in information processing. These findings are in line with the hypothesis that altered emotional processing is key for achieving and maintaining remission (Godlewska and Harmer, 2020; Harmer et al., 2009). However, few studies have examined this area of neurocognitive functioning, with most having small sample sizes and incorporating adjunctive pharmacotherapy. Moreover, none of the studies included a healthy control group, although one can hypothesise that biases in emotional processing are less likely to be influenced by task familiarity and practise effects.
Regarding differential effects of psychotherapies, head-to-head comparisons showed little evidence of superiority in improving aspects of neurocognitive functioning. Only one study found significant differences in neurocognitive function between psychotherapy modalities. Groves et al. (2015) showed a preferential effect of Metacognitive Therapy (which is not yet recommended in current treatment guidelines) on executive functioning when compared with CBT. This effect may relate to the specific attentional practise component of Metacognitive Therapy. There also appeared to be more evidence of MBCT having an effect on emotional processing than other evidence-based psychotherapies. Nevertheless, given the paucity of studies evaluated and the myriad of methodological issues evident in this area, it is difficult to draw conclusions about the differential effects of psychotherapies on neurocognitive functioning in mood disorders.
Methodological issues and considerations
While not an exhaustive list, the following section will discuss the most pertinent limitations associated with the reviewed studies, highlighting key methodological considerations for future research in this area:
Several studies utilised an open trial format and/or lacked a healthy control group. This makes it difficult to determine whether cognitive change was due to psychotherapy or merely a function of task familiarity, practise effects or regression to the mean. While using parallel forms of tasks can help mitigate this issue to some extent, this is still unable to fully partial out such effects from actual cognitive change.
Lack of healthy control groups also precluded the establishment of neurocognitive impairment in the patient samples at baseline. This is a particularly important issue given that cognitive deficits are highly variable in those with mood disorders, with a proportion of patients showing no signs of neurocognitive impairment (Burdick et al., 2014; Douglas et al., 2018). Including individuals who are not cognitively impaired at study entry will undoubtedly dilute study findings.
Studies utilising a greater number of cognitive tests may have been more likely to show significant changes over time, simply as a function of multiple comparisons, unless these were corrected for. One way to mitigate this issue is to create a priori groupings of variables into domains and use composite scores for analyses; however, such an approach may neglect individual aspects of neurocognitive functioning (Pimontel et al., 2012). Moreover, many cognitive tasks require involvement of several cognitive processes, thereby limiting the validity of domain-based analysis.
Statistical power was a limitation for most studies. It is possible that small to moderate changes in neurocognitive function were undetected due to the utilisation of small samples and therefore, some null findings may have been attributable to lack of statistical power rather than lack of cognitive change over time.
Patient samples were often heterogeneous with respect to clinical characteristics such as mood symptom severity, psychiatric comorbidity and medication use. While such samples are more reflective of real-world clinical populations, the presence of such heterogeneity may have influenced the extent of cognitive change in these samples.
Approximately half of the samples were not medication-free or their concurrent medication use was not stipulated. While permitting adjunctive medications may help with generalisability of study findings, it is important to note that psychotropic medications can also have an effect on neurocognitive functioning (Keefe et al., 2014; Rosenblat et al., 2016; Wagner et al., 2012).
In some studies, TAU was unrestricted or not specified. This could have allowed for ‘control’ participants to receive an active treatment; thereby, potentially influencing study outcome. Future studies should specify what TAU entails and should consider the extent to which their TAU arm is truly a control group.
There was a lack of follow-up data in many reviewed studies. Thus, there is limited information regarding the long-term impacts of psychotherapy and the maintenance of neurocognitive change over time.
Limitations
There are several limitations of the current review. First, the review was limited to English-language based publications. This may have resulted in some sources of evidence being missed. Second, given the heterogeneity of patient samples, the variability of treatment protocols, and the differing cognitive tests employed, it was not possible to use a meta-analytic technique and thus, a quantitative result could not be produced. Furthermore, most treatment modalities were examined by only one or two studies, and only one study examined the effects of evidence-based psychotherapy for BD. In this context, it is not possible to make valid comparisons between individual treatments, especially in the absence of head-to-head comparisons. Finally, while risk of bias was formally assessed using the Cochrane Risk of Bias Tool, it is noteworthy that this fails to consider other important sources of bias that are specific to psychotherapy, such as manualisation of therapy and the use of fidelity measures (Kisely, 2020). We have made comment on such sources of bias, however, this was not guided by an established tool. There is an ongoing need for a risk of bias tool that incorporates bias which is pertinent to psychotherapy trials.
Conclusion
As the literature stands, it is difficult to draw clear conclusions regarding the effects of evidence-based psychotherapy on neurocognitive function in mood disorders. This is primarily due to the paucity of studies, utilisation of small samples and the variability of cognitive tests employed. There was preliminary evidence of improved executive functioning following evidence-based psychotherapy for MDD and BD. In addition, there was some signal of reduced negative biases in emotional information processing following evidence-based psychotherapy for MDE. However, such findings should be considered in the context of several significant limitations and thus, must be interpreted cautiously. It is apparent that a greater number of large-scale RCTs involving patients with established neurocognitive impairment are needed to better establish the effects of evidence-based psychotherapies on neurocognitive function in mood disorders. Furthermore, studies should also examine the relationship between changes in neurocognitive function and functional outcome to help ascertain the translatability of cognitive change to real-word functioning. Specific cognitive remediation therapies, which in some cases, combine aspects of evidence-based psychotherapies with more novel cognitive remediation strategies, are beginning to be trialled and show preliminary evidence that such combinations may produce positive results (Bowie et al., 2013, 2017). Given the detrimental effects that enduring neurocognitive impairment can have on clinical and functional outcomes in mood disorders, this continues to be an ongoing area of importance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.M.D., C.R.B., M.M., S.J.G. and R.J.P. use software provided free-of-charge by Scientific Brain Training Pro for cognitive remediation trials. R.J.P. has received support for travel to educational meetings from Servier and Lundbeck. C.R.B. has grant support from Lundbeck, Takeda and Pfizer, and has received consulting fees from Boehringer Ingelheim, Pfizer and Lundbeck.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.M.D. was supported by a Sir Charles Hercus Health Research Fellowship from the Health Research Council of New Zealand during completion of this paper. M.M was supported by a Joseph-Armand Bombardier Doctoral Canada Graduate Scholarship from the Social Sciences and Humanities Research Council, and Ontario Graduate Scholarship, during completion of this paper. S.J.G. was supported by a University of Otago Doctoral Scholarship during the completion of this paper.
Supplemental material
Supplemental material for this article is available online.