
Abstract
The study of hallucinations across multiple senses in psychosis has garnered renewed interest. Recent studies have adopted the term multimodal hallucinations to describe these experiences, yet some appear to be investigating a different, but related, phenomenon. In the current paper, we suggest use of the terms multimodal hallucinations and multisensory hallucinations to categorise distinct events that involve unusual sensory experiences across multiple domains. We propose that the constructs of temporality and relatedness are critical to delineating these experiences, where multimodal hallucinations refer to hallucinations in two or more sensory modes occurring concurrently in time and/or with significant thematic overlaps. Multisensory hallucinations conversely denote similar multisensory experiences, but with no temporal or relatedness constraints. This is accompanied by a decision-making framework for identifying whether a set of unusual perceptual experiences constitutes multimodal hallucinations or otherwise. We conclude by suggesting several priorities for future research, including empirical validation of our proposed model, further investigation of phenomenology, developing appropriate assessment tools and investigating underlying cognitive and other aetiological mechanisms.
Introduction
Across psychiatric research and clinical practice, there is consensus on what constitutes hallucinations – perceptions that occur in the absence of corresponding external stimuli. Early theorists debated the nature of pseudo versus true hallucinations, but subsequent agreement has permitted our knowledge base to flourish, particularly in relation to auditory hallucinations. It has since been established that voices are prevalent in schizophrenia spectrum and related disorders, though hallucinations in other senses are not uncommon (e.g. McCarthy-Jones et al., 2017). An early study reported that up to 75% of their psychosis cohort experienced lifetime hallucinations across more than one sensory domain (Goodwin et al., 1971). This is notable as the high prevalence does not accord with the successive lack of scientific attention and progress in the area. Over the past decades, the study of auditory hallucinations has dominated psychiatry, whereas hallucinations in the visual and other senses have largely been relegated to the neurological sphere. However, there is now general acceptance that these experiences vary on a continuum of typical misperception applicable to most individuals, to frank clinical disorder, with significant variation in between. To this end, hallucinations affecting multiple senses have been noted in other psychiatric disorders (e.g. bipolar disorder; Baethge et al., 2005), organic brain disease and other medical conditions (e.g. Parkinson’s disease; Llorca et al., 2016), and within the general population (Laroi et al., 2019). As this phenomenon has re-surfaced onto the research agenda in psychosis, three key considerations must be addressed, namely: (1) nomenclature, (2) clear-cut definitions of the events under study and (3) priorities for future research.
Nomenclature
The term multimodal hallucinations (MMH) was first coined by Chesterman and Boast (1994) and operationalised as ‘hallucinations in different sensory modalities occurring simultaneously and appearing to be emanating from a single source’ (p. 279). This nomenclature has since been adopted (e.g. Lim et al., 2016), though many were referencing a somewhat distinct, but related, phenomenon. Specifically, most studies were describing experiences involving multiple sensory modes, but not necessarily synchronous or related in any way. To address this, we would like to advocate for separate terminology describing hallucinatory experiences that occur in more than one sensory domain, but are not congruent in time and/or content (or whose temporality or basis has not been explicitly assessed); these should be termed multisensory hallucinations (MSH). Put simply, MSH refers to hallucinations in two or more sensory modes occurring at discrete time points and/or with negligible overlap in content. There are benefits for delineating these phenomena. This difference is important from a theoretical perspective, especially in view of advancing our understanding of these complex experiences traversing multiple sensory domains. From a research perspective, it is important to gather inclusive descriptions of MMH versus MSH, which could perhaps offer clues relating to unique clinical or neurobiological correlates, or yield utility in terms of differential diagnoses and related treatment implications. We also support use of the MMH terminology, but with refinement to its operationalisation for improved clarity and research utility (see section ‘Pertinent updates to the existing MMH definition’). Retention of this term is desirable, as it appears intuitively expressive of the key underlying concept (rather than less helpful or outmoded labels, such as dissociative hallucinations).
Challenges in operationalising MMH versus MSH
We propose a decision-making framework to guide determinations of whether a set of unusual perceptual experiences constitutes MMH, or fit more appropriately within the umbrella of MSH. There are two aspects to be addressed: (1) electing which sensory modalities to be included and (2) refining the definition of MMH with respect to its temporal source of origin and other aspects; this would facilitate concomitant operationalisation of MSH.
Sensory modalities under consideration
It is vital to decide which sensory modalities should be included. According to Blom (2010), up to 14 types of sensory modes exist, each with its own corresponding type of hallucination. Beyond the five basic senses (i.e. auditory, visual, somatic-tactile, olfactory, gustatory), there seems to be an overwhelming number of further modalities to contemplate. On inspection, we can offer some simplifications. Blom (2010) distinguished the somatic and tactile modes; somatic hallucinations are experienced inside the body, whereas tactile hallucinations typically relate to touch experienced on the outside of the body. We see little need for this division. These two types of experiences often overlap, and detailed phenomenological descriptions will allow separation between the two modes (if desired). Similarly, algesic, sexual and thermal hallucinations typically occur in the somatic-tactile realm. Proprioceptive, kinesthetic, vestibular and cenesthetic hallucinations all involve peculiar visceral or bodily sensations, whereas temporal hallucinations stand unique. Little is known about these latter modalities, which have been rarely studied in clinical or non-clinical populations. Given the infancy of MMH and MSH studies in psychosis, we advocate for inclusion of the five major sensory domains at present (see Figure 1).
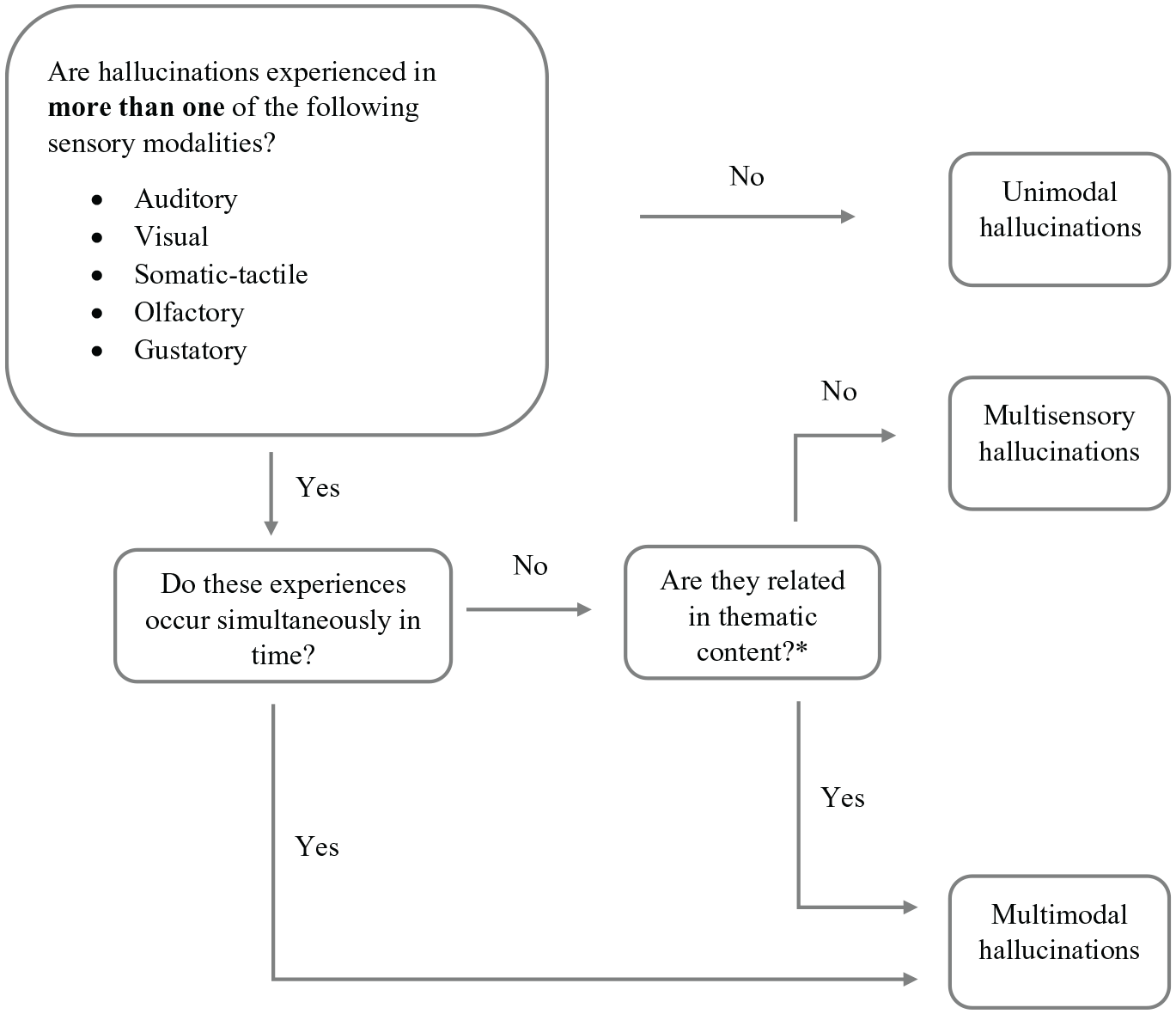
Decision framework for distinguishing multimodal versus multisensory hallucinations.
Pertinent updates to the existing MMH definition
The early MMH definition offered by Chesterman and Boast (1994) was recently adopted by Montagnese et al. (2020), with several updates. First, they extended the temporal component to include simultaneous versus serial MMH. Second, they recommended considering the source aspect from a dimensional perspective in terms of relatedness (i.e. same entity, meaningfully related entities, completely unrelated entities). Third, they introduced an added congruence feature, described as coherence with reality. We will now put forward an inclusive definition of MMH by leveraging off and refining their theoretical perspective.
Temporality
Expanding the temporal component of MMH is logical, as we concur that hallucinations across multiple sensory domains do not need to be synchronous to qualify as MMH. Yet an important concern for serial MMH is the time frame under study. Recommending any temporal cut-off will likely be arbitrary, and consideration within an acute psychotic episode has its own challenges (e.g. some hallucinations are enduring). To counter this, we propose adding the criterion of relatedness, such that serial hallucinations across two or more sensory modalities would only constitute MMH, if they also displayed a high degree of relatedness. Conversely, thematically unrelated hallucinations occurring at distinct points in time would be classed as MSH.
Relatedness
A dimensional perspective spanning a spectrum of relatedness is welcome. We would, however, suggest removing the condition that the experiences need to be attributed to the same source or entity, in favour of examining relatedness of thematic content. For example, if one perceived a vision of angels and the voice of God (whether simultaneously or in serial), we argue this would constitute MMH, even though these experiences may not be ascribed to the same entity. What is key should be level of integration within the MMH experience as well as interactions across multiple sensory domains; thematic consistencies should take precedence over a narrow focus on origin. In deciding relatedness, it is noted that personal relevance should be a determining factor. This will depend on whether an individual believes their multisensory experiences to be meaningfully related.
Congruence
In contrast, we contend that introduction of the congruence feature is somewhat unnecessary. By virtue of their nature, hallucinations are incongruent with reality. Within a clinical episode, these hallucinations are not shared by most others, and their veracity (other than to the affected individual) is highly questionable. What Montagnese et al. (2020) are describing seems to be more aptly encompassed by degree of bizarreness, which is a phenomenological dimension worthy of further study, but likely not essential in delineating MMH.
An illustration of our framework for decision-making
We will illustrate how this works with an example (refer to Figure 1). Hallucinatory experiences are labelled unimodal if only one core sensory modality is implicated. Conversely, experiences across two or more senses will either be termed MMH or MSH. To highlight this distinction, we refer to the case of an individual reporting hallucinations in the form of hearing their brother’s voice and smelling cigarette smoke. Should these experiences occur concurrently in time, this would be classed as MMH. Alternatively, they may occur serially (e.g. daytime vs night-time). Under these circumstances, relatedness of thematic content becomes key. If the individual can identify a clear, personally significant element of relatedness in content, for instance, their brother was a heavy smoker, and the scent of cigarettes was strongly associated with him, this is also termed MMH. Yet if to the individual, cigarette smoke was completely unrelated to their brother, this would be classed as MSH. The element of personal significance is essential for identifying relatedness of hallucinatory experiences because distinct sensory experiences can be seemingly unrelated from an objective viewpoint.
Priorities for future research
Revived interest in hallucinations beyond voices was spearheaded by investigations into non-auditory modalities (i.e. auditory, visual, somatic-tactile, olfactory, gustatory). Yet the majority of this research did not consider the central tenets of temporality and relatedness we have outlined as vital to the definition of MMH; they were, in essence, studies of MSH (Clark et al., 2017; Lim et al., 2016; Llorca et al., 2016; McCarthy-Jones et al., 2017). The fact that some studies utilised the MMH term while actually describing investigations of MSH provides further indication of the pressing need for a consistent set of terminology and definitions for use across the field. Some studies were also biased towards a specific modality (e.g. Chouinard et al., 2019; Langdon et al., 2011) or comprised a subset of the primary sensory domains (e.g. Hoffman and Varanko, 2006). Focusing on MSH, these were found to be twice (53%) as prevalent as hallucinations in a single modality (27%) over the lifetime (Lim et al., 2016). The general consensus was that combined auditory and visual hallucinations were most common in schizophrenia spectrum disorders (Llorca et al., 2016; McCarthy-Jones et al., 2017) and associated with increased psychopathology and less favourable outcomes in first-episode psychosis (Clark et al., 2017). Having auditory hallucinations increased the likelihood of experiences in other modalities by a factor of 2.31, but notably, endorsing visual hallucinations amplified this by a staggering factor of 11.32. Related to this, it was observed that auditory hallucinations were highly prevalent in those with lifetime visual hallucinations (83–97%), but the converse was less true, in that a much smaller proportion of those with lifetime auditory hallucinations also had visual hallucinations (30–37%; McCarthy-Jones et al., 2017). Furthermore, visual hallucinations tended to cluster with those in the somatic-tactile and olfactory domains (David et al., 2011).
To date, there are only three known studies of MMH which fit our definition. Each of these has made a small yet valuable contribution to the scant literature. Oorschot et al. (2012) reported that auditory and visual hallucinations co-occurring in time accounted for 40% of hallucinatory experiences in their cohort. This was associated with heightened negative affect and delusionality, only the latter of which preceded onset of hallucinations. In contrasting MMH and MSH (though they did not explicitly use the latter term), Dudley et al. (2018) noted that the auditory-visual-tactile combination was most common in MMH, whereas the auditory-visual combination was most common in MSH. The latter accords with existing findings (Clark et al., 2017; Llorca et al., 2016; McCarthy-Jones et al., 2017). Dudley et al. (2018) speculated that these hallucinatory experiences were associated with greater levels of conviction and distress (but could not offer empirical corroboration). Other limitations related to small participant numbers and a bias towards psychosis patients with primary visual hallucinations. Employing a sizable transdiagnostic sample, Toh et al. (2019) cited percentages of visual (52.8%), tactile (46.2%), olfactory (35.7%) and gustatory (18.1%) hallucinations comorbid with auditory hallucinations in MSH. Accounting for temporality, more MMH were serial (58.6%) than simultaneous (17.1%) in nature; a proportion (21.1%) was unrelated in time (it was unclear if the latter constituted MMH as relatedness was not assessed). This study was also limited by a bias towards the auditory mode and involved re-analysis of a pre-collected dataset where measures were not explicitly targeted towards an MMH versus MSH framework. To address existing gaps in knowledge, we suggest four priorities for future research: (1) empirical validation of our proposed model, (2) phenomenological investigations, (3) appropriate assessment tools and (4) associated cognitive and other underlying mechanisms.
Empirical validation of our proposed model
Our proposed framework needs to undergo stringent empirical validation. Such attempts may find that other classification models hold greater scientific merit. For instance, we have suggested two mutually exclusive categories – MMH versus MSH, primarily as a straightforward and systematic way to demarcate these unspecified phenomena within an emerging field. However, other theoretical models are possible and could include more than two categorisations (e.g. delineation of MMH subtypes based on overlaps in temporality and/or relatedness), or ones that are not mutually exclusive (e.g. MMH could exist as a subtype of MSH). Our initial preposition rests on the best available (but scant) scientific evidence and is open to further scientific debate and empirical testing.
There are several ways this can be achieved. From a clinical perspective, we advocate for an open dialogue and knowledge-sharing among clinicians, researchers and lived experience consumers. To this end, MMH and MSH could evoke distinct phenomenological experiences (see section ‘Phenomenology of MMH versus MSH’). At a minimum, the former seemingly implicates broader neurocognitive involvement and could invoke greater distress and/or functional impairment. From a statistical perspective, advanced methods involving cluster analysis or discriminant function analysis and the like could elucidate which phenomenological elements of these experiences meaningfully band together or are set apart. This can be informed by further empirical investigations encompassing cognitive and other aetiological correlates (see section ‘Cognitive mechanisms and other underlying aetiological factors’).
Phenomenology of MMH versus MSH
The most pervasive barrier to advancing MMH and MSH research at present is the lack of consensus regarding their definitions. We have proposed a preliminary framework as the first step towards overcoming this, but acknowledge it may need further input and refinement. The next step will be to further elucidate the specific characteristics of MMH versus MSH, including shared phenomenological similarities and differences. This symptom-based approach, coupled with appropriate transdiagnostic comparisons (e.g. unimodal vs MSH vs MMH), will help build up a critical body of literature. Importantly, we will need to gain a deeper understanding of what exactly these phenomena are before we can meaningfully delve into their clinical, genetic and neurobiological correlates. This working model should ideally encompass underlying mechanisms spanning the range of sensory modalities under consideration.
There will be novel considerations, for example, those specific to MMH will likely relate to temporality and relatedness. For serial experiences, the temporal ordering of which sensory modalities typically precede others remains unknown. Whether this is significant is questionable, but could offer vital clues relating to the possible activation of underlying neurobiological networks. The other pertinent question relates to whether specific sensory modalities cluster together and implications therein. This could point towards distinct phenotypes of hallucinatory experiences, possibly with discrete liable mechanisms, therapeutic implications and prognosis.
Appropriate assessment tools
To facilitate further enquiry of these experiences in psychosis, appropriate assessment tools must be developed. An analysis of this issue has been covered by other authors (Montagnese et al., 2020), so we aim to succinctly touch on key points. The majority of validated measures are focused on auditory hallucinations, and those that extend to multiple sensory domains primarily gauge MSH, and lack phenomenological detail. To date, only the Questionnaire for Psychotic Experiences (QPE; Rossell et al., 2019) comes close, but even then, it contains a single MMH question and offers little phenomenological information beyond the auditory and visual modes. For the purpose of assessments, we offer two caveats. First, the complexity of these constructs would necessitate face-to-face interviews with trained researchers to facilitate accurate information gathering. Self-report questionnaires can offer valuable initial insights, but may ultimately face validity issues, especially for MMH. Related to this, assessment of the personal significance of individual experiences will likely involve semi-structured questions, anchored to address specific criteria, but incorporating qualitative descriptors as well. Second, owing to extensive intra- and inter-individual differences, critical decisions need to be made regarding the frame of reference – will assessments be based on predominant, lifetime or current experiences? This will largely depend on the specific research questions under study, but longitudinal examinations will be imperative in understanding the true nature and fluctuations of these complex experiences.
Cognitive mechanisms and other underlying aetiological factors
The study of cognition has been central to unravelling key aetiological mechanisms underlying hallucinatory experiences. A range of cognitive factors liable for auditory hallucinations has been highlighted (e.g. Waters et al., 2012), but their specificity and overreliance on language processes has at times hindered applicability to hallucinations in different sensory modes (Toh et al., 2019). High prevalence rates of MMH and MSH documented thus far (e.g. Goodwin et al., 1971) underscore the inadequacy of existing models that focus on modality-specific cognitive mechanisms.
Given inherent complexities of MMH and MSH, it is likely that multiple aetiological factors are at play. Beyond cognition, nascent research has pointed towards to the importance of trauma, especially in childhood. Positive associations were uncovered between the total number of childhood adversities and involvement of multiple sensory modalities in hallucinations in adulthood (Longden et al., 2016; Medjkane et al., 2020). Yet the following questions remain unanswered: (1) Are MMH or MSH in persons who have experienced trauma phenomenologically distinct from those who have no trauma history? (2) Is it the severity, ongoing nature or type of traumatic event that is most liable? (3) Which sensory modalities tend to be implicated, and what are their dimensions of temporality and relatedness? Further research is required to address these queries.
Conclusion
The current paper introduced the term MSH, delineating its key distinctions with MMH, and offering clarification regarding operationalisation of the latter, involving specific aspects of temporality and relatedness. We put forward a framework for decision-making and illustrated the process of determining how a set of unusual perceptual experiences would be classified as MMH or MSH. Finally, we highlighted priorities for future research, including empirical validation of our proposed model, phenomenological investigations, the development of assessment tools to aid this endeavour and also examination of key cognitive and other aetiological mechanisms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: W.L.T. is supported by a National Health and Medical Research Council (NHMRC) New Investigator project grant (GNT1161609), and S.L.R. is supported by a NHMRC Fellowship (GNT1154651). The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the funding body.