
Abstract
Introduction:
Globally, Indigenous populations have higher rates of suicidal behavior and psychological distress compared to non-Indigenous populations. Indigenous populations also report high rates of exposure to discrimination, which could potentially contribute to poor mental health outcomes. The objectives of this paper were to estimate the prevalence of discrimination among Aboriginal and Torres Strait Islander males in Australia and to examine the role of discrimination in the association between Aboriginal and Torres Strait Islander status and suicidal thoughts and depressive symptoms.
Methods:
We used cross-sectional data on 13,697 males aged 18–55 years from the Australian Longitudinal Study on Male Health. We undertook a Poisson regression with robust standard error analyses to examine Aboriginal and Torres Strait Islander status and self-perceived exposure to discrimination in the past 2 years as correlates of recent suicidal ideation. We used zero-inflated negative binomial regression to assess Aboriginal and Torres Strait Islander status and self-perceived exposure to discrimination as correlates of recent depressive symptoms.
Results:
Aboriginal and Torres Strait Islander males have a twofold higher prevalence of self-perceived discrimination (39.2% vs 19.3%, p < 0.001), suicidal ideation (21.8% vs 9.4%, p < 0.001) and moderate or worse depressive symptoms (24.0% vs 12.2%, p < 0.001) as compared to their non-Indigenous counterparts. After adjusting for sociodemographics and substance use, Aboriginal and Torres Strait Islander status was significantly associated with suicidal thoughts (odds ratio = 1.49, p = 0.019) and depressive symptoms (prevalence rate ratio = 1.19, p = 0.018). About 15.3% and 28.7% of the association between Aboriginal and Torres Strait Islander status and suicidal thoughts and depressive symptoms, respectively, was explained by discrimination.
Conclusion:
Our analyses add to evidence that discrimination is a contributor to mental health disparities between Aboriginal and Torres Strait Islander and non-Indigenous populations in Australia. Reducing discrimination ought to be considered as part of strategies to improve the social and emotional well-being of Aboriginal and Torres Strait Islander people.
Keywords
Introduction
The high rates of suicide among Indigenous populations is a distressing phenomenon observed in several postcolonial countries, including Australia, Canada, the United States and New Zealand. Poor social and emotional well-being among Indigenous peoples is a complex socio-cultural, political, biological and psychological phenomenon that needs to be understood in the context of colonization, loss of land and culture, trans-generational trauma, grief and loss, and racism and discrimination (Elias et al., 2012; Paradies, 2016). Higher levels of marginalization and social disadvantage experienced by Indigenous peoples also increases their exposure to substance misuse and a suite of chronically stressful life events, which are well-documented contributors to poor social and emotional well-being, including symptoms of psychological distress and suicidality.
In Australia, suicide is the second leading cause of mortality for Aboriginal and Torres Strait Islander males (Australian Bureau of Statistics, 2020). The suicide rate for Aboriginal and Torres Strait Islander males was estimated to be 34.5 per 100,000 across 2015–2019, almost twice the rate (19.5 per 100,000) for non-Indigenous males. This disparity in suicide rates is highest in younger age groups, being approximately three times higher among Aboriginal and Torres Strait Islander males aged 15–24 years compared to their non-Indigenous counterparts. Mirroring these inequities in suicide rates, a large general population survey of Australian males observed that Aboriginal and Torres Strait Islander males were twice as likely as non-Indigenous males to report recent suicidal thoughts and more than three times as likely to report a suicide attempt in their lifetime (Armstrong et al., 2017). Other studies of Aboriginal and Torres Strait Islander people have also observed a high and potentially increasing prevalence of suicidal behavior. Additionally, a higher prevalence of symptoms of common mental health problems have been observed among Aboriginal and Torres Strait Islander people compared to non-Indigenous Australians (Black et al., 2015; Jorm et al., 2012).
While there is good evidence establishing the higher rates of suicidality and poor mental health among Aboriginal and Torres Strait Islander people, there is very little research into the social determinants of this disparity despite calls for this through the Aboriginal and Torres Strait Islander Suicide Prevention Evaluation Project (Dudgeon et al., 2016). An important new area of enquiry is the role of discrimination as a contributing factor to poor mental health among Aboriginal and Torres Strait Islander people. Regardless of definition, discrimination is increasingly recognized as an important area of public health research and systematic reviews and meta-analyses consistently highlight associations between discrimination and health inequities (Paradies et al., 2015; Priest et al., 2013), including inequities in psychological well-being (Elias and Paradies, 2016; Schmitt et al., 2014).
Surveys targeted at Aboriginal and Torres Strait Islander people have documented high rates of self-reported discrimination (Cave et al., 2018; Cunningham and Paradies, 2013; Markwick et al., 2019; Temple et al., 2020) and that these experiences of discrimination extend to the healthcare system, which carry detrimental impacts on health-seeking behavior among Aboriginal and Torres Strait Islander people (Waterworth et al., 2015; Wylie and McConkey, 2019). Moreover, survey research has observed that discrimination was associated with worse social and emotional well-being among Aboriginal youth, including depressive and anxiety symptoms and suicidal thoughts (Cave et al., 2019; Priest et al., 2011a, 2011b; Shepherd et al., 2017; Ziersch et al., 2011). However, to our knowledge, no prior research has examined discrimination as a potential mediator of the association between Aboriginal and Torres Strait Islander status and poor mental health outcomes using large general population survey data.
Our paper addresses this gap by analyzing data for males aged 18–55 years that were collected as part of the first wave of The Australian Longitudinal Study on Male Health. The objectives of our analyses were to: (1) estimate the prevalence of perceived discrimination among Aboriginal and Torres Strait Islander males, (2) assess whether discrimination was independently associated with suicidal thoughts and depressive symptoms among Aboriginal and Torres Strait Islander males and (3) assess the potential mediation role of discrimination in the associations between Aboriginal and Torres Strait Islander status and suicidal thoughts and depressive symptoms.
Methods
Data source
The sample consisted of 13,697 adult males aged between 18 and 55 years who participated in the first wave of The Australian Longitudinal Study on Male Health (Ten to Men). This paper presents analysis of data collected in 2013–2014 for the baseline wave only, as discrimination was not measured in subsequent waves of data collection. Details of the study design and data collection methods of the Ten to Men study have been published elsewhere (Currier et al., 2016; Pirkis et al., 2017). In brief, the Ten to Men study used a multistage stratified cluster sampling to recruit Australian males from households in Australian Statistical Geographical Standard (ASGS) major city, inner regional and outer regional areas of Australia. A total of 104,484 households were approached in 2013 and 2014, from which 15,988 Australian males were recruited, resulting in a response fraction of 35% among confirmed eligible males.
Eligible participants were males aged 18–55 years at the time of recruitment, who were Australian citizens or permanent residents and had a sufficient understanding of English to provide informed consent and to complete the self-administered questionnaire. Males aged under 18 years were excluded from our analyses as they were not asked about discrimination.
The Ten to Men study received ethical clearance from the University of Melbourne Human Sciences Human Ethics Sub-Committee (HREC 1237897 and 1237376).
Variables and measurement
Aboriginal and Torres Strait Islander status
Aboriginal and Torres Strait Islander status was determined through participants self-reporting as Aboriginal, Torres Strait Islander or both or neither. Participants were excluded from our analyses if they refused or did not answer the question.
Discrimination
Discrimination was assessed using the question ‘Over the past two years, how often have you experienced discrimination?’ Those who responded ‘very often’, ‘fairly often’ or ‘occasionally’ were grouped into one category and compared against another category that combined ‘rarely’ and ‘never’.
Depressive symptoms and suicidal behavior
Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9) for adults, a nine-item screening tool based on criteria for depressive disorders in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) (Kroenke et al., 2001). The PHQ-9 has well-established criterion, construct and external validity (Kroenke and Spitzer, 2002; Levis et al., 2019). The PHQ-9 asks participants how often they have been bothered with nine symptoms in the past 2 weeks, with response options on a 4-point Likert-type scale: not at all (0), several days (1), more than half the days (HelpAge International Myanmar et al., 2016) and nearly every day (Plantinga et al., 2008). The PHQ-9 yields scores ranging from 0 to 27, with a score of 10 representing the threshold marking the lower limit moderate depressive symptoms.
We used item 9 of the PHQ-9 as a binary measure of suicidal ideation. Item 9 asks participants how often they had been bothered by ‘thoughts you would be better off dead or of hurting yourself in some way’. This measure was dichotomized to compare participants whose response was ‘several days’, ‘more than half the days’ and ‘nearly every day’ with those whose response was ‘not at all’. Endorsement of suicidal ideation on this item has been associated with a 75–185% increase in the risk of suicide in a study of veterans in the United States (Louzon et al., 2016). The lifetime prevalence of suicide attempt(s) was assessed through self-report; participants were asked if they had ever tried to kill themselves. Both measures of suicidality have previously been used in a survey of Aboriginal and Torres Strait Islander youth in Australia (Brown et al., 2013; Luke et al., 2013).
Other variables
Other variables included in our analysis were age, highest educational qualification, combined household income, Socio-Economic Indexes for Areas (SEIFA), employment status, remoteness, alcohol misuse and illicit substance use. SEIFA is a measure developed by the Australian Bureau of Statistics to rank areas by their relative socioeconomic advantage and disadvantage (Australian Bureau of Statistics, 2006).
Statistical analysis
All data analyses were conducted in Stata version 15.0 and accounted for the complex multistage sampling design and unequal probability of selection. Weighted proportions were used to describe the sociodemographic characteristics of the study participants, discrimination, suicidal ideation and depressive symptoms. Prevalence data were disaggregated by Aboriginal and Torres Strait Islander identification, and chi-square tests were used to assess the difference between Aboriginal and Torres Strait Islander males and their non-Indigenous counterparts. We used Poisson regression with robust standard errors (Zou, 2004) (with robust variance estimate) to examine the association between Aboriginal and Torres Strait Islander identification and perceived discrimination. In model 1, we assessed the unadjusted association. In model 2, we adjusted for age, education, household income, SEIFA, employment and remoteness. In model 3, we added alcohol misuse and illicit substance use into the model.
Similarly, we also assessed Aboriginal and Torres Strait Islander status and discrimination as correlates of suicidal ideation using Poisson regression with robust standard errors. As the data for PHQ-9 scores exhibited overdispersion and excess zeros (Tang et al., 2018), zero-inflated negative binomial regression was used to assess Aboriginal and Torres Strait Islander status and discrimination as correlates of depressive symptoms. We used Stata program zinb models for this purpose and inflated parameters for Aboriginal and Torres Strait Islander status and discrimination. Incident rate ratios for the negative binomial portion of zinb models were presented along with their corresponding 95% confidence intervals and p-values.
Using the concept of the additive model (Hafeman, 2009) (i.e. the total effect equals the sum of direct and indirect effect), the proportion of association that could be explained by discrimination was indirectly estimated as a difference between β-coefficients in the regression models with and without discrimination. The proportion of the association between Aboriginal and Torres Strait Islander identification and suicidal ideation and depressive symptoms that can be explained by discrimination was computed as the difference between beta-coefficient (β3) in model 3 and model 4 (β4) divided by the beta-coefficient in model 3 (β3) times 100%; proportion explained = [(β3 − β4)/β3] × 100% (β3 and β4 are beta-coefficients in model 3 and model 4, respectively).
Results
Participant characteristics
A total of 326 (2.4%) males aged 18–55 years identified as being Aboriginal and Torres Strait Islander people, with the remaining 13,371 (97.6%) identifying as non-Indigenous. A detailed description of the weighted prevalence of participant characteristics and how these vary between Aboriginal and Torres Strait Islander and non-Indigenous Australian males is shown in Table 1. The characteristics of the Aboriginal and Torres Strait Islander and non-Indigenous sub-samples differed significantly. A higher proportion of the Aboriginal and Torres Strait Islander sub-sample were younger, never married, in the lower income category, less educated, living in regional rather than urban areas, and engaging in harmful use of alcohol and other substances. The prevalence of discrimination (39.2% vs 19.3%, p < 0.001), suicidal ideation (21.8% vs 9.4%, p < 0.001) and moderate or worse depressive symptoms (23.9% vs 12.2%, p = 0.001) were significantly higher among Aboriginal and Torres Strait Islander males compared to their non-Indigenous counterparts.
Characteristics of the sample population and key outcomes (weighted prevalence and 95% CI).
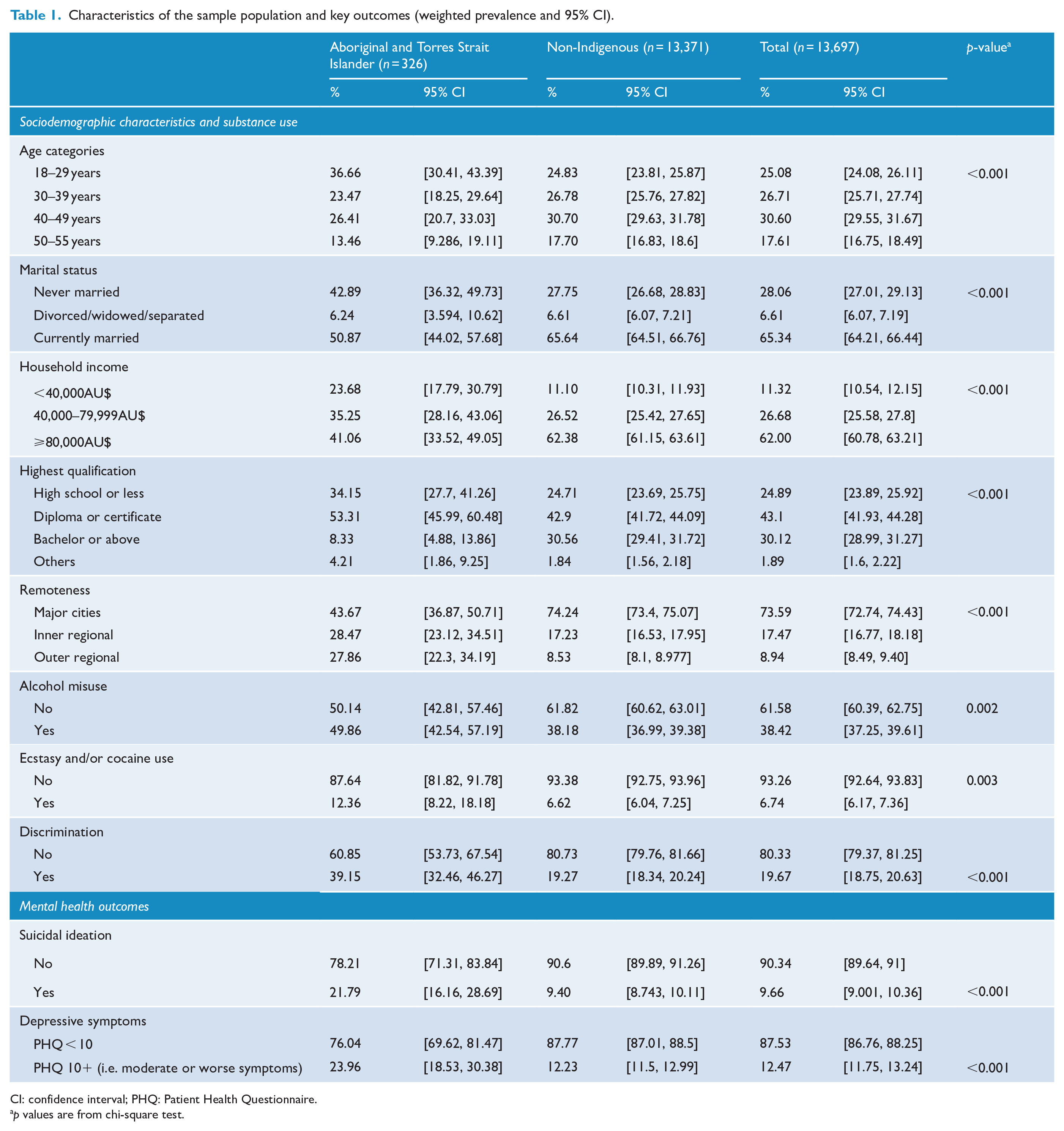
CI: confidence interval; PHQ: Patient Health Questionnaire.
p values are from chi-square test.
Discrimination as a potential mediator of the association between Aboriginal and Torres Strait Islander status and mental health outcomes
Table 2 presents results from Poisson regression with robust standard errors and zero-inflated negative binomial regression models examining the association between Aboriginal and Torres Strait Islander status, discrimination, suicidal ideation and depressive symptoms. We observed that Aboriginal and Torres Strait Islander males had 1.90 (95% confidence interval [CI]: [1.54, 2.33]) times increased risk of experiencing perceived discrimination than non-Indigenous males (p < 0.001) after adjusting for sociodemographic variables (age, education, household income, SEIFA and employment), remoteness, alcohol misuse and illicit substance use.
Associations between Aboriginal and Torres Strait Islander identification, discrimination, suicidal ideation and depressive symptoms.
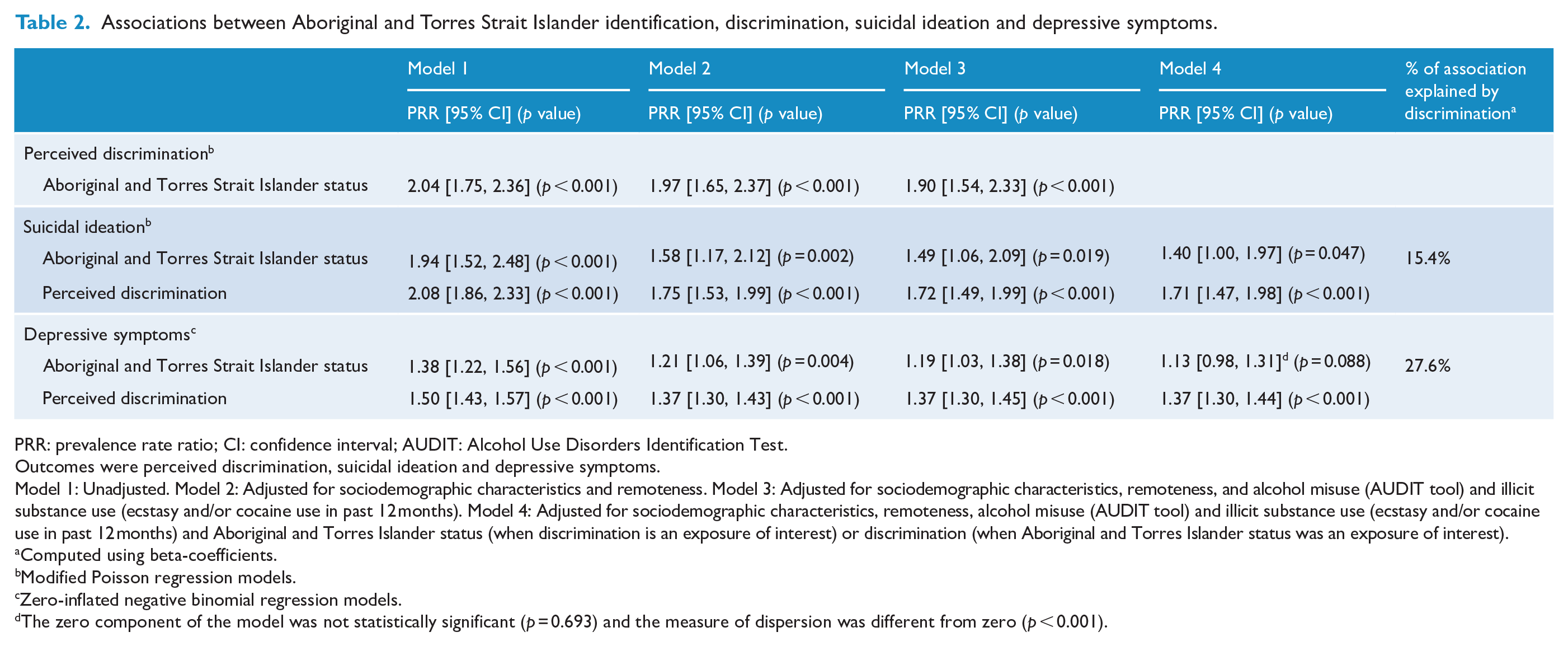
PRR: prevalence rate ratio; CI: confidence interval; AUDIT: Alcohol Use Disorders Identification Test.
Outcomes were perceived discrimination, suicidal ideation and depressive symptoms.
Model 1: Unadjusted. Model 2: Adjusted for sociodemographic characteristics and remoteness. Model 3: Adjusted for sociodemographic characteristics, remoteness, and alcohol misuse (AUDIT tool) and illicit substance use (ecstasy and/or cocaine use in past 12 months). Model 4: Adjusted for sociodemographic characteristics, remoteness, alcohol misuse (AUDIT tool) and illicit substance use (ecstasy and/or cocaine use in past 12 months) and Aboriginal and Torres Islander status (when discrimination is an exposure of interest) or discrimination (when Aboriginal and Torres Islander status was an exposure of interest).
Computed using beta-coefficients.
Modified Poisson regression models.
Zero-inflated negative binomial regression models.
The zero component of the model was not statistically significant (p = 0.693) and the measure of dispersion was different from zero (p < 0.001).
After adjusting for sociodemographic and substance use characteristics, Aboriginal and Torres Strait Islander males had 1.49 (95% CI: [1.06, 2.09]) times higher risk of suicidal thoughts compared to non-Indigenous males (p = 0.019). When perceived discrimination was included in the model, the rate ratio for the association between Aboriginal and Torres Strait Islander status and suicidal ideation decreased to 1.40 (95% CI: [1.00, 1.97]), with analysis of β-coefficients suggesting that discrimination explained 15.3% of the association between Aboriginal and Torres Strait Islander identification and suicidal ideation.
After adjusting for sociodemographic and substance use characteristics, Aboriginal and Torres Strait Islander males had 15% (95% CI: [3%, 29%]) higher depressive symptom scores as compared to non-Indigenous males. The incidence rate ratio for the association between Aboriginal and Torres Strait Islander status and depressive symptoms decreased from 1.19 (95% CI: [1.03, 1.38]) to 1.13 (95% CI: [0.98, 1.31]) when perceived discrimination was included in the model. Analysis of β-coefficients suggested discrimination explained 28.7% of the association between Aboriginal and Torres Strait Islander status and depressive symptoms.
Discussion
Summary of the findings
Our study is the first to use a large general population sample to estimate the prevalence of perceived discrimination experiences among Aboriginal and Torres Strait Islander males and to examine the potential mediation role of discrimination between Aboriginal and Torres Strait Islander status and suicidal ideation and discrimination. We found a statistically significant association between Aboriginal and Torres Strait Islander identification and perceived discrimination (prevalence rate ratio [PRR] = 1.90), suicidal ideation (PRR = 1.49) and depressive symptoms (PRR = 1.19). The estimation of the proportion of the association between Aboriginal and Torres Islander identification and suicidal ideation and depressive symptoms that could be explained by discrimination was small and moderate, respectively.
Our findings are consistent with minority stress theory, which asserts that minority groups experience a high level of discrimination resulting in negative health impacts through various pathways, such as stress, maladaptive behaviors and poor access to health and social services (Dentato et al., 2013; Meyer, 2003). Similarly, social stress models propose that prejudice, discrimination and related social ills place an additional burden on socially disadvantaged populations, which can increase the risk of mental health problems (Schwartz and Meyer, 2010). The findings of this study are also consistent with studies that report the potential mediating role of minority stress factors, including discrimination, on the association between minority status and mental health outcomes. Cross-sectional and longitudinal studies of sexual and other racial minority groups have suggested that minority stress factors, including discrimination, mediate the pathway between minority status and poor mental health outcomes (Baams et al., 2015; Bränström, 2017; Calabrese et al., 2015; Chang et al., 2020). Therefore, reducing discrimination among minority groups may be a promising target for intervention and could potentially provide ‘upstream’ benefits to the prevention of suicidality and psychological distress.
There is a legitimate query as to whether the mood of participants, which was assessed at the same time as discrimination was assessed (albeit with different time parameters), influenced participant perceptions of discrimination experiences. Even though discrimination is a risk factor for suicidal ideation and depressive symptoms, there may be some reverse causality. Mood-as-information research indicates that both positive and negative moods may be influential in affecting perceptions of discrimination; individuals with positive moods may be more likely to minimize discrimination and individuals with negative moods may be more likely to acknowledge greater discrimination in their lives (Sechrist et al., 2003). Nonetheless, the accumulating body of evidence from longitudinal studies has consistently found racial discrimination on the pathway to adverse mental health, with those longitudinal studies that have been undertaken consistently finding adverse mental health effects associated with racial discrimination (Cave et al., 2020).
Implications for prevention and research
Our data indicate that perceived discrimination is a common experience for Aboriginal and Torres Strait Islander men and that this experience may be implicated in contributing to suicidality and depressive symptoms. This has important practical implications for programs seeking to improve social and emotional well-being among Aboriginal and Torres Strait Islander people. Our findings support the broad assertions that discrimination is a determinant of mental health outcomes among Aboriginal and Torres Strait Islander people and that reducing racism and discrimination ought to be considered as part of strategies to reduce suicide and improve the social and emotional well-being of Aboriginal and Torres Strait Islander people. Accordingly, reducing racism and discrimination has been recognized in the 2013 National Aboriginal and Torres Strait Islander Suicide Prevention Strategy (NATSISPS) (Australian Government., 2013) as important to preventing suicide among Aboriginal and Torres Strait Islander people. Ferdinand et al. (2017) advocate that bolstering existing anti-racism policies and programs designed specifically around the histories and experiences of Aboriginal and Torres Strait Islander peoples is necessary to address racism at a community and population level. Future research might examine the potential to reduce suicidal behavior among Aboriginal and Torres Strait Islander people through community-based interventions to reduce discrimination and racism. Further examination of the issue may also take an intersectionality approach, to further examine the multiple intersecting identities that increase vulnerability to discrimination in a range of contexts; for example, Aboriginal and Torres Strait Islander people may experience discrimination from other Aboriginal and Torres Strait Islander people due to their sexual minority status or their mental ill health.
Limitations of the study
Our study had some limitations. First, the use of only one wave of data does not permit rigorous conclusions to be drawn about the temporal sequence of morbidity or the underlying mechanisms of the observed mediated effects of discrimination. A longitudinal study further investigating the nature of this relationship in an Aboriginal and Torres Strait Islander cohort is warranted (Calabrese et al., 2015; Hou et al., 2015; Priest et al., 2017). Second, discrimination was measured using a question that assessed ‘perceived discrimination’, with the inherent weakness of relying on participants to judge whether or not they had experienced discrimination. We were not able to present data on the scope and number of experiences of discrimination, nor the context, which may have further illuminated underlying social mechanisms that could inform improved targeting of anti-discrimination strategies. Indeed, some discrimination experiences may have been the result of interactions with other Aboriginal and Torres Strait Islander people. Nonetheless, there is utility in a broad assessment that does not limit the scope, locations or contexts in which discrimination is perceived to have occurred. Third, the low response rate of 35% could affect the representativeness and limits the ability to produce reliable prevalence estimates at a national level (Pirkis et al., 2016). Furthermore, the Ten to Men study has a relatively low age cut-off of 55 years which excludes older men at increased risk of suicide. Similarly, participants in the Ten to Men study were sampled from major cities, and inner and outer regional areas; the study did not include people from remote areas and so our findings cannot be generalized to those settings. This is an important limitation given that many remote communities have significant proportions of Aboriginal or Torres Strait Islander people. Nonetheless, there was reasonable representation of people from key groups, based on observable characteristics. For instance, the proportion of Aboriginal and Torres Strait Islander males (2.7%) is roughly equivalent to the proportion in the general population (3.0%). Finally, we used the zero-inflated negative binomial regression models as it is appropriate for the PHQ-9 score distribution. The negative binomial portion of the model can be interpreted as the total symptoms (Vyas et al., 2020). However, the inflated portion is not clinically interpretable. Thus, we focused on the negative binomial portion as it is clinically interpretable as severity of total symptoms.
Conclusion
We observed a high prevalence of perceived discrimination among Aboriginal and Torres Strait Islander males. Poor mental health outcomes for Aboriginal and Torres Strait Islander males were strongly associated with exposure to experiences of discrimination, suggesting that discrimination may be a contributor to mental health disparities between Aboriginal and Torres Strait Islander and non-Indigenous populations in Australia. Our findings suggest that reducing discrimination ought to be a critical part of strategies to reduce suicide and improve the social and emotional well-being of Aboriginal and Torres Strait Islander people.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research on which this paper is based was conducted as part of the Australian Longitudinal Study on Male Health (Ten to Men). We are grateful to the Australian Government Department of Health for funding and to the boys and men who provided the survey data. Ten to Men is managed by the Australian Institute of Family Studies. Ten to Men research data is the intellectual property of the Commonwealth. Additionally, G.A. is funded by an Early Career Fellowship from the National Health and Medical Research Council (GNT1138096). J.T.Y. receives salary and research support from a National Health and Medical Research Council Investigator Grant (NTG1178027).