
Abstract
The report of the Productivity Commission Inquiry into mental health was released in November 2020, estimating the economic cost of mental illness in Australia at over $200 billion a year. The report makes wide-ranging recommendations for improving the mental health of the population, reforming the mental health treatment system, and in the way mental health is managed in other sectors of society.
Introduction
The Productivity Commission, an agency of the Federal Treasury, is the Australian Government’s independent research and advisory body on economic, social and environmental issues affecting the welfare of Australians. In short, its primary role is to help governments make better policies, in the long-term interest of the Australian community. The scope of the mental health inquiry was to consider the role of mental health in supporting economic participation, enhancing productivity and economic growth. The Commission was asked for recommendations to improve population mental health, so as to realise economic and social participation and productivity benefits over the long term. Between November 2018 and June 2020, the Inquiry held 6 roundtables, 13 days of public hearings, almost 300 individual meetings with stakeholders and received 1244 public submissions (the most for any inquiry held by the Commission). The final report (Productivity Commission, 2020) was delivered on 30 June 2020 and released by the Prime Minister on 16 November 2020.
The economic headline was that mental illness is costing Australia between $200 and $220 billion per year, between $550 million and $600 million per day. This cost is made up of (1) the cost of health and social services, (2) lost productivity, (3) the cost of informal care given by families and friends and (4) the largest cost by far from the monetised impact of diminished health and reduced life expectancy. The total is just over one-tenth of the size of Australia’s entire economic production in 2019. While a large part of this cost is unavertable with our current knowledge, the Commission found there is considerable scope for Australia to do a lot better.
Navigating the report
The report is over 1300 pages, in three volumes, with an additional online set of supporting materials. Volume 1 contains the overview and recommendations, and volumes 2 and 3 contain the chapters (1 to 25). In volume 2, chapters 1 to 4 outline the case for major mental health reform; chapters 5 to 9 address the services for children including in schools, youth economic employment, workplace mental health, social inclusion and stigma reduction and suicide prevention; chapters 10 to 16 cover access to mental healthcare, online treatment, bridging gaps in mental healthcare, crisis services, closing the life expectancy gap, integrating care and the mental health workforce. In volume 3, chapters 17 to 21 cover psychosocial support services, carer and family services, income and employment support, housing and homelessness and justice services; chapters 22 to 25 address the enablers of reform including governance, funding, monitoring, evaluation and research.
Five key reform areas
The report contains recommendations and actions which can be grouped into five main areas. The first area is prevention and early intervention. The Commission was presented with the evidence that social, economic and environmental impacts, for example, interpersonal violence, economic inequality and climate change, increase the risk of mental ill-health. Attempting to address the cause of these impacts fell outside the terms of reference, however the recommendations do target related areas, such as increased support for new parents and developing a mental health system which can respond to the demand for services arising from ‘shocks’ to the population. Other recommendations in this area include making the social and emotional development of school children a national priority, doubling-down on stigma reduction, ensuring follow-up care for people after suicide attempts and empowering Indigenous communities to prevent suicide.
The second area addresses the health sector. The core theme is improving people’s experiences when receiving mental healthcare, with recommendations to enhance skills within the workforce and ensure assessment and referral processes help people find the services that are best for them. Treatment should include identifying, supporting and including families and carers wherever possible. The report supports the expansion of clinically supported online treatment and access to mental healthcare via telehealth. The recommendation on reviewing limits on psychological treatment funded through Medicare was addressed in the recent Federal budget by increasing to 20 the number of sessions subsidised by the MBS each year. In the specialist mental health sector, recommendations include expanding community-based mental healthcare, outreach services, alternatives to emergency departments for crisis care and addressing the significant shortage of non-acute bed-based services. A national target should be set for closing the gap in life expectancy experienced by people with severe mental illness. A summary of the key recommendations relevant to clinical practice is provided in the Table 1.
Key actions impacting on clinical practice.
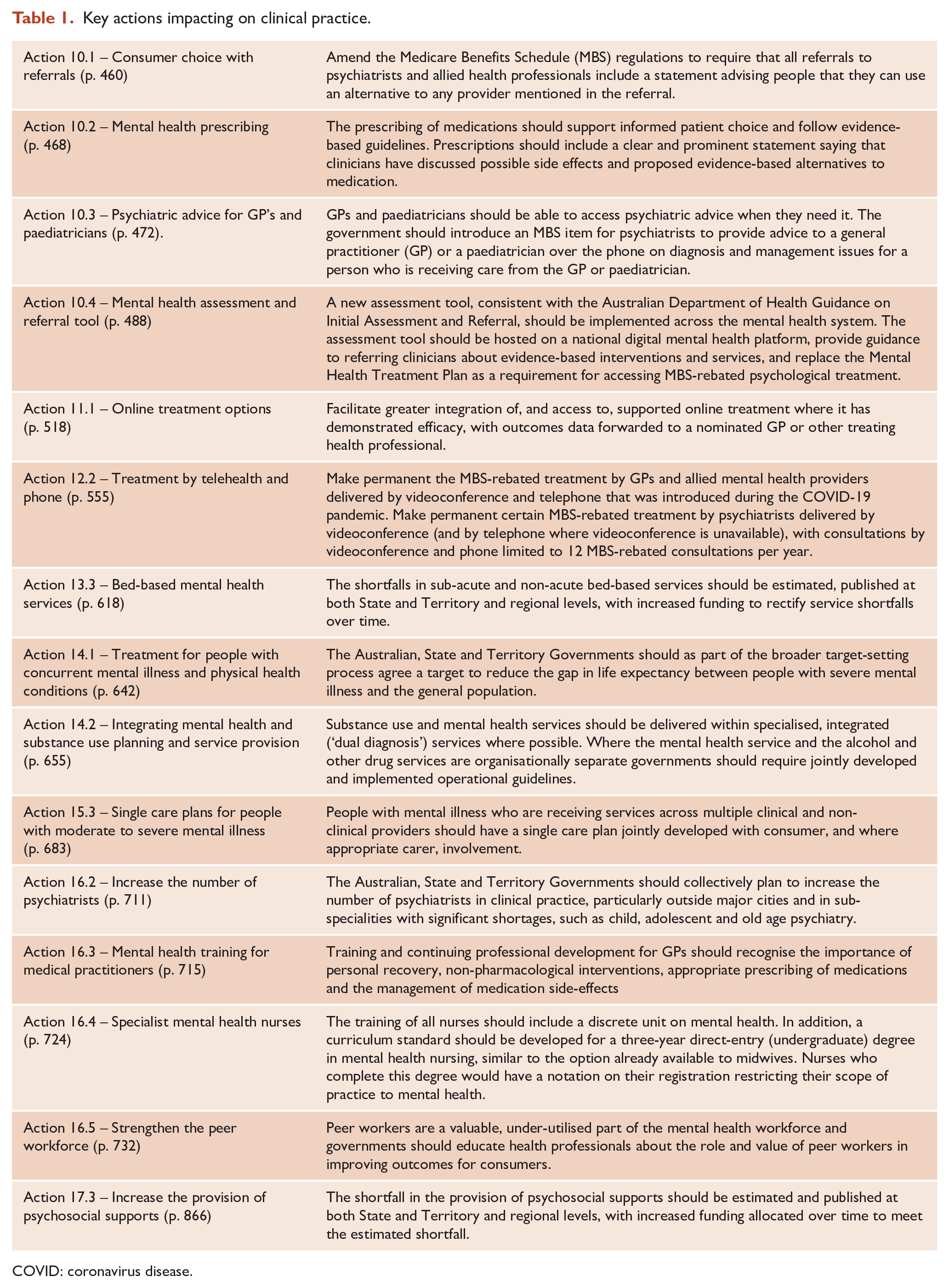
COVID: coronavirus disease.
The third area is to improve people’s experiences with services they need beyond the health system. The Commission found a very significant shortfall in the availability of community support services that are essential in helping people with mental illness recover and live productive lives. In addition, the report recommends a commitment be made to a principle of no discharge from care into homelessness, as well as increased mental health assistance for police responding to mental illness related incidents and legal representation for people facing mental health tribunals.
The fourth area is to elevate the importance of psychological health and safety in workplaces. The Commission recommended clinical treatment be available for mental health related workers compensation claims without waiting for a decision on liability about the cause of a mental illness. Another key recommendation is to expand the individual placement and support programme for people with mental illness to promote vocational recovery.
The final area is to embed incentives and accountability, with recommendations to strengthen an evaluation culture, focusing on outcomes that matter to people. Consumer and carer participation and advocacy across the mental health system is recommended to help drive this. The report strongly supports the planning and integration of services at a regional level, with Primary Health Networks (PHNs) and Local Hospital Networks (LHNs) receiving increased support to jointly determine the mental health service needs of their region and how to allocate the resources to best meet these needs. The report recommends annual comparison of existing clinical and psychosocial support services with a national benchmark of what services are needed (such as provided through the National Mental Health Service Planning Framework, Recommendation 24). A greater role for the Australian Institute for Health and Welfare and a restructured National Mental Health Commission is needed to support these reforms.
Conclusion
What happens now? When launching the report, the Prime Minister committed to only one of the recommendations (Action 23.3), the development of a National Mental Health and Suicide Prevention Agreement between the Australian, State and Territory governments. He mentioned the need for additional funding would be considered in the 2021 Federal budget.
The report has 120 findings and recommendations and there needs to be some prioritisation with sustained reform over the next decade. The workforce implications of the recommendations alone require long term planning. However, there are recommendations that should be started immediately. The Productivity Commission used four criteria to prioritise the reform options, split many of the recommendations into ‘start now, state later’, and found that most of the economic benefit will come from implementing the priority recommendations. The Commission estimated the extent to which each reform is likely to lead to improved health-related quality of life (at the population level) and to result in a net monetary cost or benefit.
The first of the four criteria used to prioritise the reforms is the potential to save or improve lives at the individual and/or community level. Some reforms are expected to improve the quality of life in a substantial way for a small number of people, for example universal aftercare following a suicide attempt (Action 9.1). Other reforms can be expected to improve the quality of life in a smaller way but for a large portion of the population, for example, a national stigma reduction strategy (Action 8.1).
The second criterion is benefits to the economy, and expenditure required, to implement the recommendations. The estimated benefits to the economy are largely from an increase in labour force participation by consumers and carers, and the higher wages through increased productivity of those people who are working. While clinicians will be all too familiar with the life trajectory of a young person shown in Figure 3.3 (page 160), it is Figure 3 in the Overview (page 16) showing the estimated net cost or benefit to the economy from a reform, and the expected improvement in quality of life, that should attract the attention of Treasury. Some reforms actually have a net economic benefit, for example, expanding individual placement and support for people with mental illness entering the workforce, no-liability early treatment for people with mental health related workers compensation claims, expanding supported online clinical treatment and supporting parents in the perinatal period.
The third criterion is ease of implementation. Reforms that require the redeployment of existing resources, involve comparatively little disruption to other parts of the community, and involve just one government or government agency, were considered easier to implement than reforms requiring the redirection of resources from other programmes, or the cooperation of multiple agencies. Examples include expanding digital mental health services and perinatal mental health services. There is also action needed to improve services within their existing budgets and staffing. For example, analysis undertaken by the Commission suggested clinical staff in state and territory community ambulatory services spend less than one-third of their time on consumer-related activities (Figure 12.12), with the recommendation that governments investigate and address the reasons for this (Action 12.4).
The fourth criterion is sequencing. Many reforms need to be implemented in stages with the feasibility of some dependent on the success of earlier actions or reforms. The recommendations to expand community bed-based services and to grow the psychiatry, nursing and peer workforce will take funding and time. Some recommendations, such as the new mental health assessment tool (Action 10.4) and activity-based funding for community mental health services (Action 23.7), require technical development and trialling before they could be implemented on a national scale. Other recommendations, such as measuring and closing the shortfall in psychosocial support services (Action 17.3), will require negotiation and agreement between multiple governments and the non-government sector where most of these services are delivered.
How much of the Commission report will be accepted and implemented by governments remains unclear, with the impact of COVID-19 seen as both a risk and opportunity. On 18 December 2020 David Coleman MP was appointed to a new position, Assistant Minister to the Prime Minister for mental health and suicide prevention, with responsibility for the considering the recommendations in the Productivity Commission report. The Royal Commission into Victoria’s mental health system is expected to provide its final report in early 2021. However, whatever action is taken by governments, the opportunities presented by the Productivity Commission report will also require a concerted, disciplined and sustained effort from the mental health professions, and the sector as a whole (Doggett, 2020).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
Professor Whiteford served as Associate Commissioner on the Productivity Commission Inquiry from November 2018 until August 2020. The views expressed are those of the author and do not necessary reflect the position of the Productivity Commission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.