
Abstract

That another Royal Commission (RC) or Board of Inquiry has eventuated is sadly unremarkable, given the breadth and depth of dysfunction in Australia’s aged care system. The key is whether there will be any effective action, as the accretion of problems through decades of manifest neglect will be very difficult to remediate. Substantial reform of the Australia’s Aged Care system has been proposed and is welcomed (Commonwealth of Australia, 2021). There is a great deal that could be achieved with concerted effort. However, in common with the recent Productivity Commission Report on Mental Health, there are concerns about the recommendations directly affecting clinical healthcare (Looi et al., 2021). Therefore, we focus on the specific recommendations that are of most direct relevance to the provision of psychiatric care for older Australians, discussing the proposals and their ramifications.
The metaphor of putting the cart before the horse is apt. The substantive redesign of the aged care system, especially in relation to improved and coordinated clinical governance, provision of funding, infrastructure and, crucially, workforce capacity, is essential before the implementation of recommendations directly impacting clinical care.
Australia clearly needs better availability and improved quality of mental health care in the aged care sector. However, clinically relevant recommendations appear to lack a practical understanding of the real-world context of provision of psychiatric care in Australia’s aged care system and systemic issues, especially in residential aged care facilities (RACFs) (Looi and Macfarlane, 2014). The key concerns relate to the practicalities of implementation of wide-ranging multi-level inter-governmental funding and policy in relation to specialist psychiatric care; the lack of consideration of the workforce planning, training, retention and recruitment necessary to provide specialist psychiatric care; and potential unexpected consequences of the restrictions on pharmacological and non-pharmacological treatment that are proposed in advance of essentially addressing the two former matters. In particular, There is burgeoning evidence for the efficacy of nonpharmacological psychosocial and nursing strategies, and these should be the basis of mental health care in RACFs. However, the staffing levels in RACFs and mental health skills of most carers (nursing assistants, enrolled nurses, personal carers) may be inadequate to implement such strategies. (Looi and Macfarlane, 2014)
The recommendation numbers from the report are referenced below (Commonwealth of Australia, 2021).
58: access to specialists via multidisciplinary outreach and 59: increased access to OPMHS
Although these are welcome suggestions and should be supported, there is a lack of operational detail on how the proposed local-hospital-network-led multidisciplinary outreach services will be developed. The only suggestions are that it should form part of the National Health Reform Agreement and will require both infrastructure and a skilled workforce, including psychiatrists, for which planning, training, recruitment and retention are necessary.
There are corresponding concerns in relation to the recommendation for increased access to older persons mental health services (OPMHS). In the case of both recommendations, the existing divide between Federal and State/Territory governmental planning and funding will hamper progress.
61: short-term changes to MBS to improve access to medical and allied health services
This is a welcome extension of the general practitioner (GP) mental health treatment plans, including referral to Better Access. The caveat is again a sufficient workforce of GPs, psychiatrists and allied health to deliver care in RACFs.
63: access to specialist telehealth services
Again welcomed, this recommendation will need foundational significant investment in telehealth and digital health facilities for RACF, as in recommendation 68. There will also need to be corresponding governmental support, via the Medicare Benefits Schedule (MBS) of appropriate consultation items for psychiatrists to provide telepsychiatry, including team-based case-conference support of GPs and RACF staff. While review of RACF residents will be best via video-telepsychiatry, telephone-telepsychiatry may be needed when preferred by residents or due to shortfalls in telecommunications network.
65: restricted prescription of antipsychotics by geriatricians and psychiatrists for residents in aged care and 17: regulation of restraints
These related recommendations seek to address the thorny challenge of behavioural and psychological symptoms of dementia (BPSD), in residents of RACFs, that may present a risk to the residents, staff and others. Such BPSD are indeed challenging, and the RC is correct that they are best addressed by non-pharmacological strategies (Looi et al., 2014). However, this must be a systemic approach involving substantive training, credentialling, and recruitment and retention of skilled nursing and allied health staff to implement comprehensive, person-centred dementia care that includes management of BPSD (Looi et al., 2014). Any approach should build on existing arrangements for collaborative care between GPs, nursing and allied health staff. Recommendations that residents with severe BPSD or psychosis should be seen by a geriatricians or psychiatrist need to consider whether there are sufficient levels of staffing, particularly of old-age psychiatrists and geriatricians. Therefore, the proposal to restrict antipsychotic prescribing in RACFs by November 2021 only focuses on one part of wider systemic issues, which requires a more comprehensive approach with careful evaluation of the outcomes (Looi and Macfarlane, 2014).
The RC incorrectly asserts that the purpose for which antipsychotic medication has been used is to sedate. In fact, the guidelines for antipsychotic usage in BPSD are primarily for dementia-related psychotic symptoms that represent a risk of physical aggression (Guideline Adaptation Committee, 2016) Accordingly, all prescribers can follow these guidelines which, in summary, recommend prescribing for targeted indications such as psychosis, agitation and aggression; evaluating the safety and efficacy; and regularly reviewing the need for continued treatment – see Table 1 (Guideline Adaptation Committee, 2016). It is within the expertise of GPs, especially those who visit to continue care of their patients in RACFs, to appropriately prescribe antipsychotic medication for specific indications, as is the case in care of all patients across the lifespan. Indeed, the specific restriction of prescribing for RACFs may have the unintended consequence of de-skilling GPs in use of these medications in such settings and reducing the continuity of care from the residents’ regular GP.
Guidelines for antipsychotic use for people with behavioural and psychological symptoms of dementia.
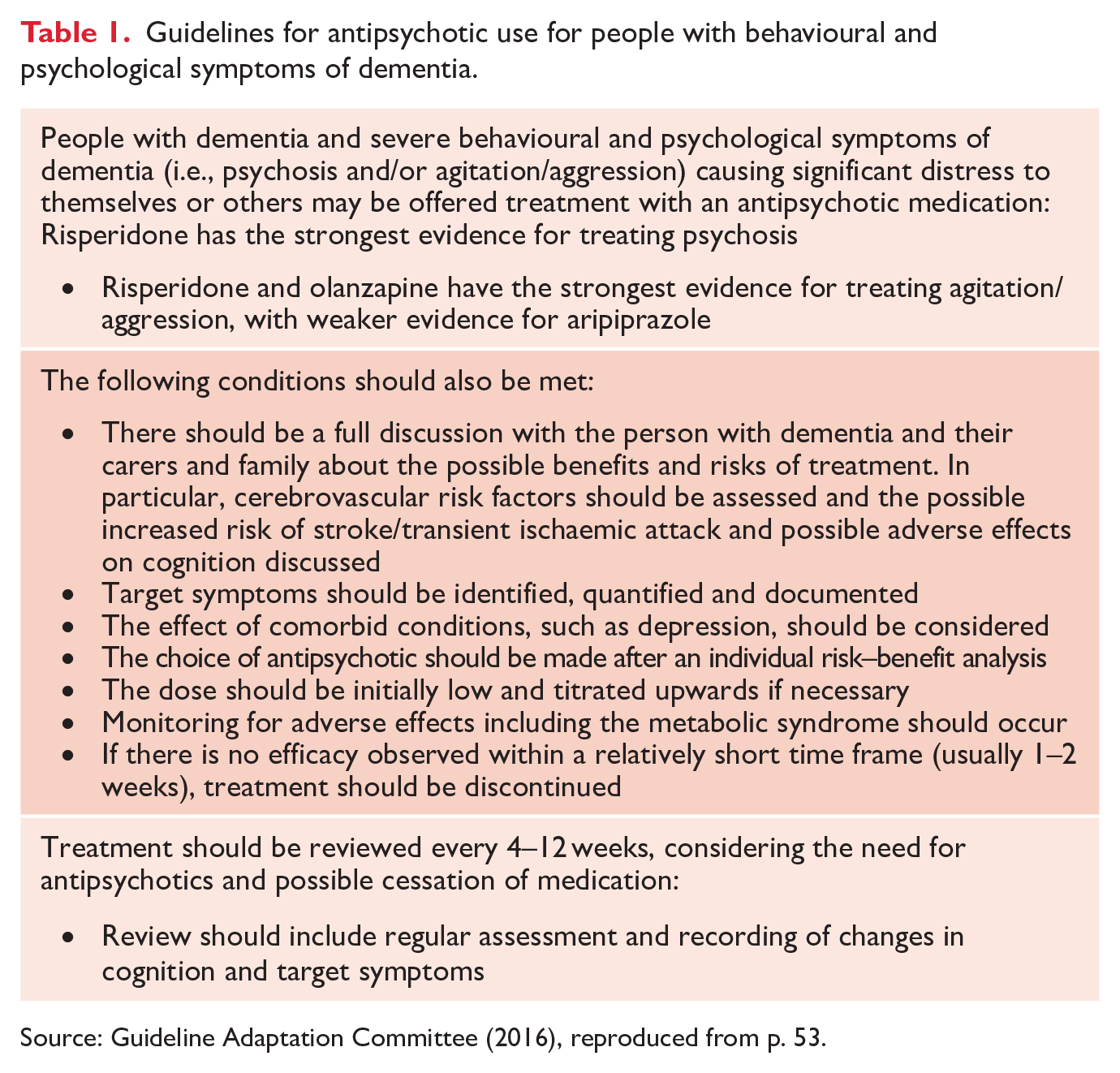
Source: Guideline Adaptation Committee (2016), reproduced from p. 53.
Skilled staffing levels must be sufficient for provision of non-restrictive care (Looi and Macfarlane, 2014); otherwise, there remains the risk of injury to residents and staff from BPSD-related aggressive or similar behaviour that warrants consideration of restrictive measures.
Conclusion
To avoid putting the cart before the horse, reform of Australia’s ailing aged care system is necessary, and especially so in relation to governance, funding, infrastructure and workforce, before the implementation of the RC recommendations pertaining to direct psychiatric care. Analogous to the Productivity Commission Report on Mental Health (Looi et al., 2021), frontline clinicians, such as GPs, Specialists, Allied Health and RACF staff, and specifically psychiatrists, must be integral to the considered implementation of recommendations relating to psychiatric care. To fail in this risks further the health of older Australians, and while very much respecting community expectations may inadvertently render the RC clinical healthcare recommendations: .. a tale … full of sound and fury, Signifying nothing. (Macbeth – William Shakespeare)
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.