
Abstract
Objective:
To describe the prevalence of symptoms of depression and anxiety, and the level of life stress and worry in late pregnancy for Māori and non-Māori women.
Methods:
In late pregnancy, women completed a questionnaire recording their prior history of mood disorders; self-reported current depressive symptoms (⩾13 on the Edinburgh Postnatal Depression Scale), current anxiety symptoms (⩾6 on the anxiety items from the Edinburgh Postnatal Depression Scale), significant life stress (⩾2 items on life stress scale) and dysfunctional worry (>12 on the Brief Measure of Worry Scale).
Results:
Data were obtained from 406 Māori women (mean age = 27.6 years, standard deviation=6.3 years) and 738 non-Māori women (mean age = 31.6 years, standard deviation=5.3 years). Depressive symptoms (22% vs 15%), anxiety symptoms (25% vs 20%), significant life stress (55% vs 30%) and a period of poor mood during the current pregnancy (18% vs 14%) were more prevalent for Māori than non-Maori women. Less than 50% of women who had experienced ⩾2 weeks of poor mood during the current pregnancy had sought help. Being young was an independent risk factor for depressive symptoms, significant life stress and dysfunctional worry. A prior history of depression was also consistently associated with a greater risk of negative affect in pregnancy.
Conclusion:
Antenatal mental health requires at least as much attention and resourcing as mental health in the postpartum period. Services need to specifically target Māori women, young women and women with a prior history of depression.
Keywords
Introduction
It has been robustly demonstrated that depression, anxiety, major life stress and severe and dysfunctional worry in the perinatal period have adverse consequences for maternal, family and child health and well-being both in the short and long term (Dunkel Schetter and Tannner, 2012; Korhonen et al., 2012; Leigh and Milgrom, 2008). Although studied less than postnatal depression and anxiety, pregnancy-specific anxiety and stress have been associated with pre-term birth, while depression, major life stress and chronic stress in pregnancy increase the risk of lower birth weight infants (Dunkel Schetter and Tannner, 2012). Depression, anxiety and major life stress in pregnancy have also all been linked with poorer child health and development outcomes, decrements in cognitive performance in adolescence and poorer mental health as a child, adolescent and adult (Korhonen et al., 2012; Leigh and Milgrom, 2008). For mothers, depression in pregnancy has been associated with reduced self-care which may lead to poor nutrition, drug and alcohol abuse and failure to attend antenatal care (Leigh and Milgrom, 2008). This in turn, may result in a decline in a mother’s physical and mental health and compromise the growth anddevelopment of the foetus. Women who experience depression in pregnancy are also at much higher risk of developing post-natal depression (Milgrom et al., 2008).
Currently in New Zealand, suicide is the leading single cause of maternal death with rates seven times higher than those seen in the United Kingdom (Perinatal and Maternal Mortality Review Committee, 2015). While nationwide surveys conducted in the last decade have not been designed to provide data specifically on perinatal mental health, results show that having a diagnosed mental illness is 1.7 times more likely for women than men (Ministry of Health, 2013). Furthermore, the rates of psychological distress (as measured by the Kessler Psychological Distress Scale) are 1.7 times higher in Māori compared with non-Māori/non-Pacific and 2.5 times higher for those living in more socio-economically deprived areas compared with less deprived areas (Ministry of Health, 2013).
A recent report identified the importance of mental health for the future health and well-being of New Zealand mothers, children and families, but the authors also noted the paucity of information available, particularly on the mental health of Māori mothers (Moewaka Barnes et al., 2013). In New Zealand, there have been a handful of studies investigating the prevalence of postnatal depression (PND) and symptoms of PND. These studies show variable rates of between 7.8% and 16% (Abbott and Maynard, 2006; Irene et al., 2006; McGill et al., 1995; Webster et al., 1994) with differences likely due to the samples studied, timing of assessments and the cut-off scores used. One study has shown Māori women to be at greater risk of PND than non-Māori women (Webster et al., 1994).
Using data collected in a face-to-face interview, the Growing Up in New Zealand (GUiNZ) study found 11.9% of pregnant women reported depressive symptoms in the third trimester (Waldie et al., 2015). In adjusted models, this study also found that women identifying as of Pacific Island, Asian or ‘Other’ ethnicities were at greater risk of depression in pregnancy, as were women who had experienced greater stress in pregnancy and had a diagnosis of anxiety before or during pregnancy. International studies suggest rates of 3.5–12.7% for diagnosed depression (Bunevicius et al., 2009; Gavin et al., 2005), 10–18.4% for depressive symptoms (Gavin et al., 2005; Giardinelli et al., 2012) and 6.6–24.7% for anxiety disorders during the antenatal period (Andersson et al., 2003; Giardinelli et al., 2012).
There is recognition within the New Zealand health sector of the need for effective perinatal mental health services but also acknowledgement that in many areas these services are lacking. In 2012, no District Health Board had all the required services in place (i.e. health promotion, screening and assessment, interventions, access to respite care and inpatient care and consultation and liaison within the health system and with other agencies) (Ministry of Health, 2012). In order to develop the appropriate level of perinatal mental health services and ensure the services target those most in need, information is needed on the prevalence of mood disturbances across the perinatal period and key population risk factors.
Historically, the focus of perinatal mental health research has been on the postpartum period, but emerging knowledge on the critical role of the foetal environment in determining a child’s long-term health and the implications of depression for subsequent maternal health points to a need for more information on mental health in the antenatal period. This study describes help-seeking behaviours of women; the prevalence of symptoms of depression and anxiety, and the occurrence of life stress and worry; and the population risk factors associated with these outcomes in a large sample of Māori and non-Māori women in the third trimester of pregnancy.
Methods
Data for the current study were drawn from a larger study, ‘E Moe, Māmā: Maternal Sleep and Health in Aotearoa/New Zealand’. The overall aim of ‘E Moe, Māmā’ was to investigate changes in sleep across the perinatal period and possible relationships to a range of health outcomes. Inclusion criteria for participation included carrying a single foetus (to reduce complications associated with multiple births), over 16 years of age (for consent purposes) and between 35 and 37 weeks gestation. Kaupapa Māori epidemiological research principles (Simmonds et al., 2008) were employed in the design and conduct of the study. For this study, these principles include Māori participation and control at all stages of the research process; participants self-identifying their ethnicity; and study processes that sought to recruit equal numbers of Māori and non-Māori participants to provide equal explanatory power for both populations (Paine and Gander, 2013). Ethical approval for the study was obtained from the Central Region Health and Disability Ethics Committee (protocol CEN 09/09/070).
Initially, pregnant women were recruited from the District Health Board regions in the lower half of the North Island of New Zealand prior to 37 weeks gestation. Lead Maternity Carers (LMCs) supported the study by informing women of the research and providing them with study information (consent form, information sheet, pregnancy and health questionnaire and pre-paid return envelope). This approach was found to be moderately effective for recruiting non-Māori women but less effective for involving Māori women. Consequently, recruitment was widened to all of New Zealand and a broader range of methods utilised to inform women of the study (Paine et al., 2013).
Measures
Women completed paper-based questionnaires in late pregnancy (35–37 weeks gestation, wave 1), data from which is described and presented here. Additional information was collected from birth records, and surveys conducted between 4 and 6 weeks postpartum and at 12 weeks postpartum.
The ‘Sleep and Health in Pregnancy’ questionnaire was developed and pretested in 2009 with careful attention being paid to the selection of the questions and the language used, as the sample was expected to include people with varying levels of literacy and some for whom English was a second language. The final version (12 pages and 58 items) included the following items that were utilised in this study: date of birth (to determine age); week of gestation (to separate those completing the study requirements between 35 and 37 weeks to those who were outside this timeframe); ethnicity using the 2001 NZ census item (Statistics New Zealand, 2005) (categorised as Māori [anyone who identified as Māori either alone or in combination with another ethnic group/s] or non-Māori [all others]), home address (to assign an NZDep 2006 decile (Salmond et al., 2007) [reduced to quintiles], which is a validated small-area index of socio-economic deprivation based on responses to nine items from the national census); and parity (a single item asking about number of previous births, alive or not, after 20 weeks pregnancy, subsequently categorised as nulliparous or multiparous).
A past history of mood disorders and diagnosed depression was acquired using questions based on items from the Pregnancy Risk Questionnaire (Austin et al., 2005) and Antenatal Risk Questionnaire (Austin et al., 2013). Women were asked: if they had been ‘miserable or depressed’ for a period of two or more weeks prior to the current pregnancy, and during the current pregnancy (hereafter referred to as a period of poor mood); if that had interfered with their functioning or their relationships (on a scale from 0, not at all to 5, very much); and if they had sought professional help. They were also asked if they had ever been told by a health professional they were depressed or needed antidepressants (hereafter referred to as diagnosed with depression). The 10-item Edinburgh Postnatal Depression Scale (EPDS) was used to assess current symptoms of depression and anxiety over the previous 7 days (Cox et al., 1987). Women indicated severity of symptoms on a 4-point scale. In this study, a cut-off of 13 or above was used to define high levels of depressive symptoms (Gorman et al., 2004), which has been shown to be sensitive to major forms of depression (Murray and Carothers, 1990). The EPDS has been shown to be valid and sensitive for use in pregnancy (Gibson et al., 2009) and has been used in other samples of New Zealand women (Ekeroma et al., 2012; Webster et al., 1994). Three of the EPDS items have been identified as reflecting anxiety and a cut-off of six or above shown to accurately identify women with an anxiety disorder (Matthey, 2008). The Life Stress scale from the Pregnancy Risk Assessment Monitoring System (Centers for Disease Control and Prevention, 2009), which is a 13-item measure asking about events in the last 12 months, was included to address the occurrence of recent stressful experiences. Women indicating two or more items on this scale were compared with those scoring less than two. The Brief Measure of Worry Scale is an 8-item self-report questionnaire that assesses the severity of worry and its impact on function using a 4-point response scale (Gladstone et al., 2005). Scores above 12 are considered to indicate dysfunctional worry (Austin et al., 2007).
Data analysis
All questionnaire data were double-entered using Epi Info (v3.5.1), cross-checked using the COMPARE procedure in SAS v9.2 (SAS Institute, Inc. Cary, NC) and discrepancies corrected using the original questionnaire. Data are described using percentages and 95% confidence intervals. Differences in prevalence between groups were investigated using Chi-square tests. To determine whether there were differences by ethnicity, age, parity, deprivation quintile and prior history of depression in the likelihood of reporting depressive or anxiety symptoms, dysfunctional worry or life stress, logistic regression analyses were calculated. All analyses were completed in SAS v9.2 (SAS Institute, Inc. Cary, NC) and are reported using the complete data set.
Results
Figure 1 provides detail on the number of study packs distributed across New Zealand and the final number known to be provided to interested women (from tracking records kept by recruitment sites or research team). Across a 2-year period (October 2009–November 2011), 1199 women completed a study enrolment form and a total of 1144 women completed comprehensive paper-based questionnaires in late pregnancy (Māori women mean age = 27.6 years, standard deviation [SD]=6.3 years; non-Māori women mean age = 31.6 years, SD=5.3 years). Of those, 93% of Māori women and 97% of non-Māori women completed questionnaires between 35 and 37 weeks gestation.
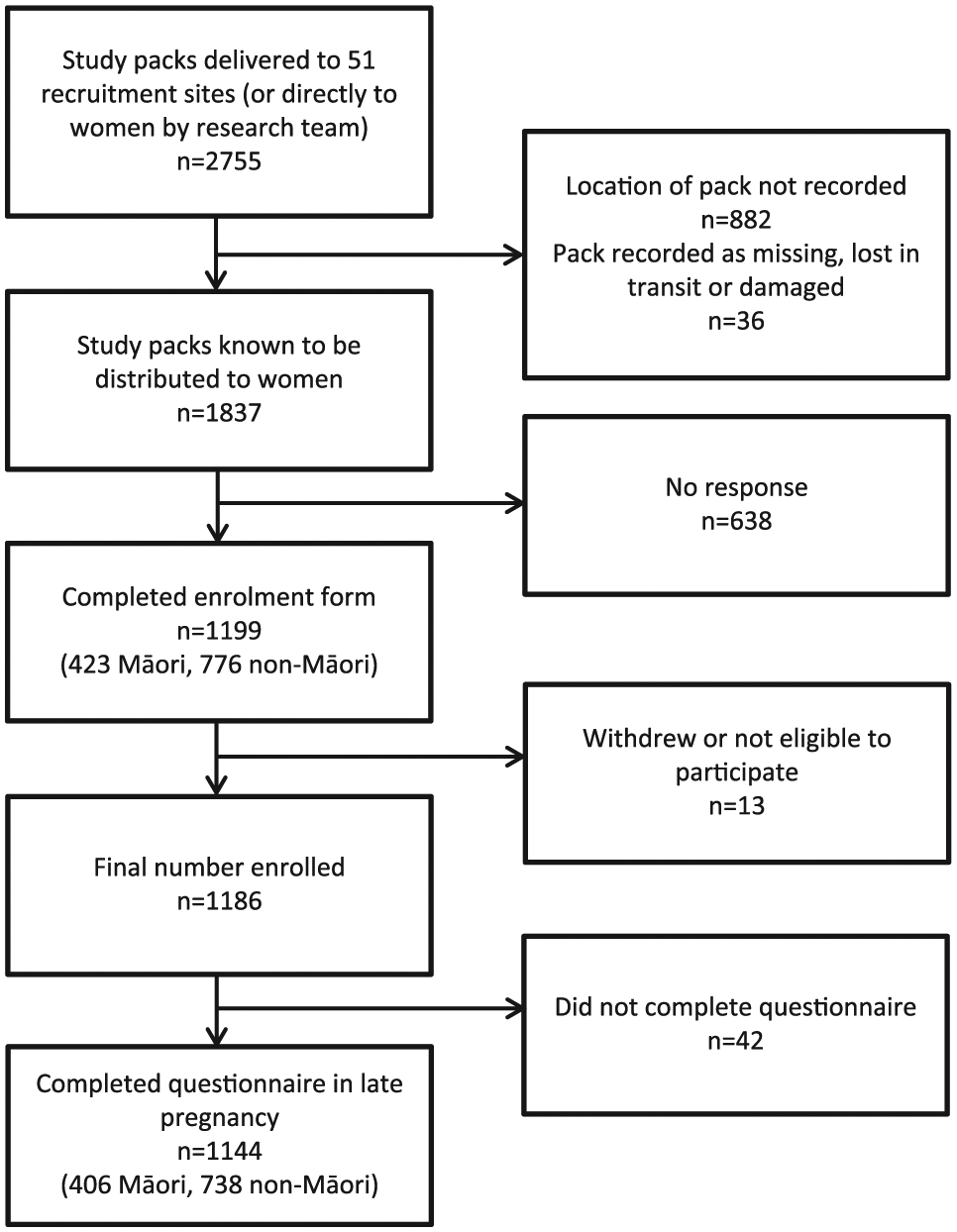
Flow diagram of pack distribution and response rates.
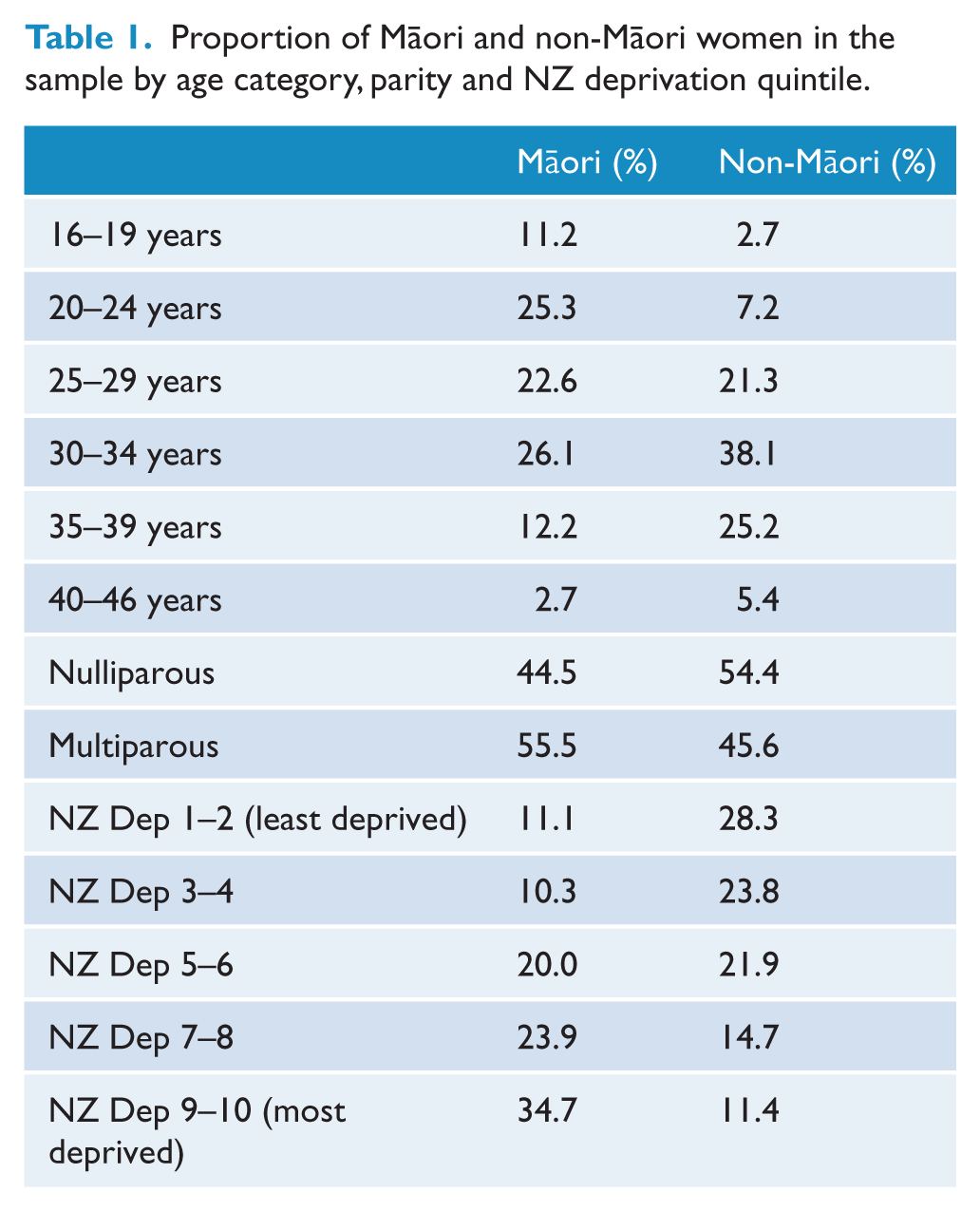
Table 1 indicates the distribution of age categories, parity and NZ deprivation quintiles by ethnicity. Māori women were more likely to be younger (χ2 = 132.96, p < 0.001), have previously had a child (χ2 = 9.94, p = 0.002) and were over-represented in the more deprived deciles compared with non-Māori women (χ2 = 144.74, p < 0.001).
Proportion of Māori and non-Māori women in the sample by age category, parity and NZ deprivation quintile.
Compared with Māori women, a greater proportion of non-Māori women reported experiencing a period of poor mood prior to the current pregnancy (χ2 = 12.83, p < 0.001) and being diagnosed with depression (χ2 = 6.55, p = 0.011). Of those women with previous poor mood, non-Māori women were more likely than Māori women to have sought professional help (χ2 = 7.23, p = 0.007), although there were no differences by ethnicity in the degree to which poor mood interfered with functioning or relationships, t(378) = 0.25, p = 0.803 (see Table 2).
Proportion of Māori and non-Māori women reporting a previous or current period of poor mood, a previous diagnosis of depression, having sought help and the mean level of interference with functioning or relationships.
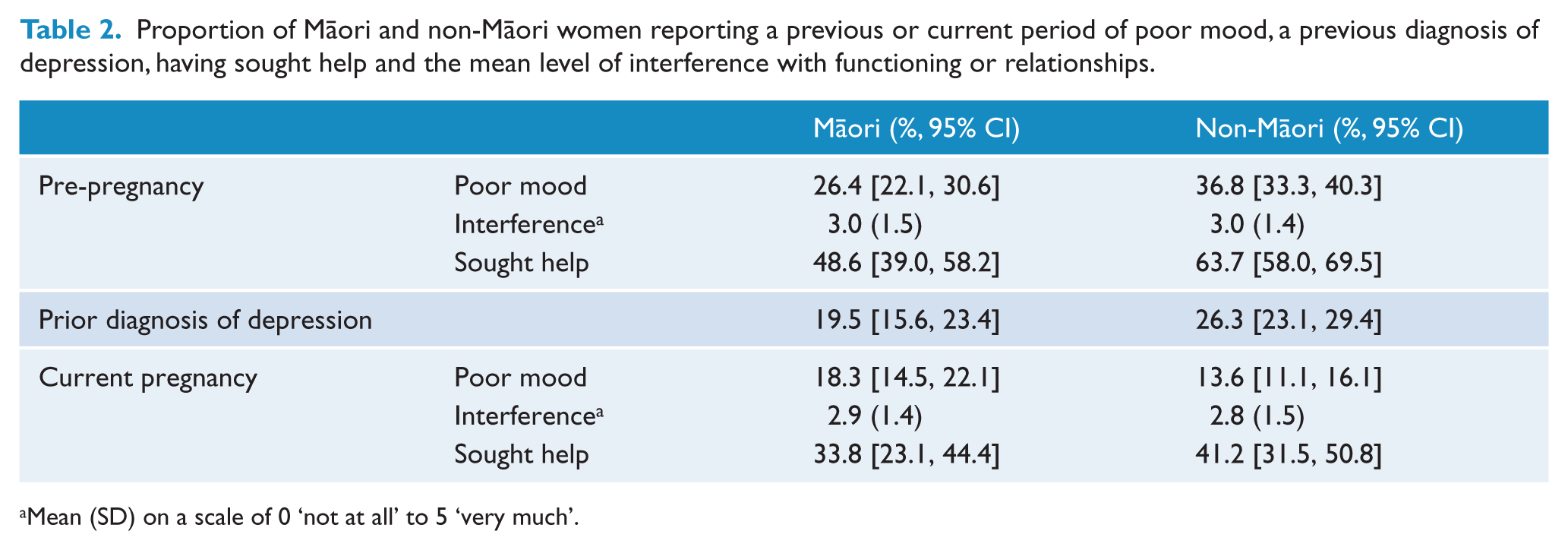
Mean (SD) on a scale of 0 ‘not at all’ to 5 ‘very much’.
When considering the current pregnancy, Māori women were more likely than non-Māori women to report experiencing a two-week or longer period of poor mood (χ2 = 4.51, p = 0.034). There were, however, no differences by ethnicity in the proportion of women who had sought professional help (χ2 = 1.02, p = 0.312) or the level to which poor mood interfered with functioning and relationships, t(178) = −0.29, p = 0.771.
As seen in Table 3, approximately a quarter of pregnant Māori women were above the a-priori cut-off for depressive symptoms and above the cut-off for anxiety symptoms, and over half of Māori women had experienced significant life stress in the last 12 months. Compared with non-Māori women, Māori women were more likely to experience significant depressive (χ2 = 9.02, p = 0.003) and anxiety symptoms (χ2 = 4.03, p = 0.045) and life stress (χ2 = 66.44, p < 0.001), although there was no difference by ethnicity in the proportion of women who were experiencing dysfunctional worry (χ2 = 0.11, p = 0.736).
Proportion of Māori and non-Māori women scoring above recognised cut-offs for depressive symptoms, anxiety, life stress and worry in late pregnancy.
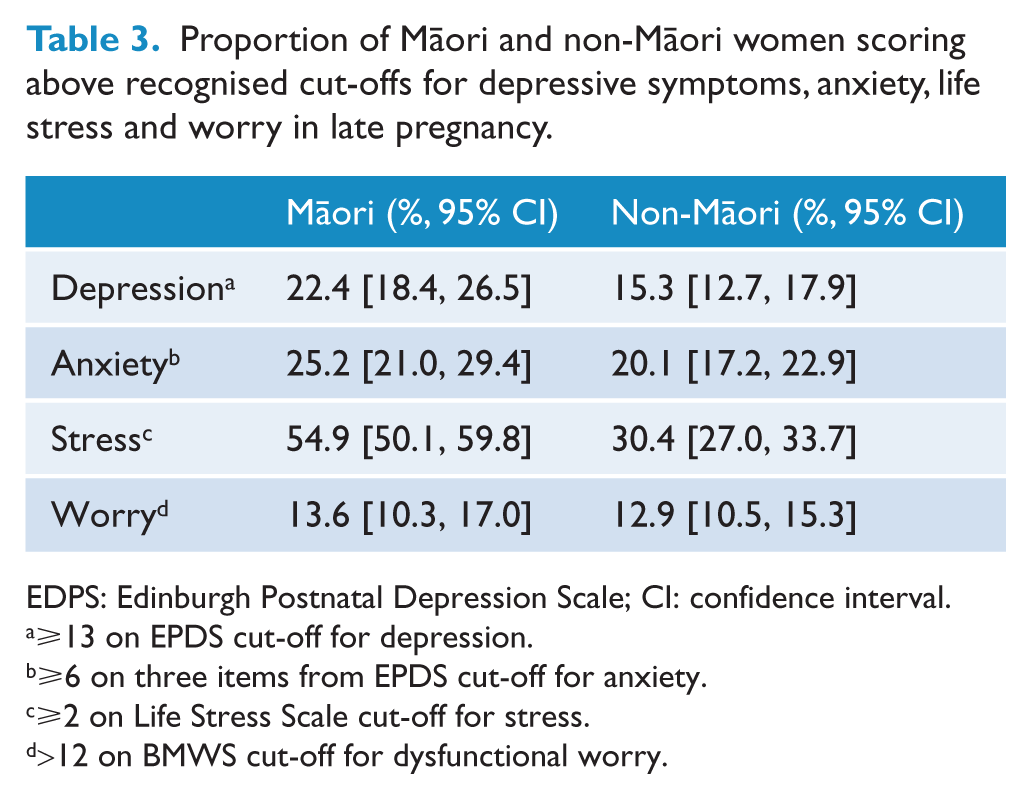
EDPS: Edinburgh Postnatal Depression Scale; CI: confidence interval.
⩾13 on EPDS cut-off for depression.
⩾6 on three items from EPDS cut-off for anxiety.
⩾2 on Life Stress Scale cut-off for stress.
>12 on BMWS cut-off for dysfunctional worry.
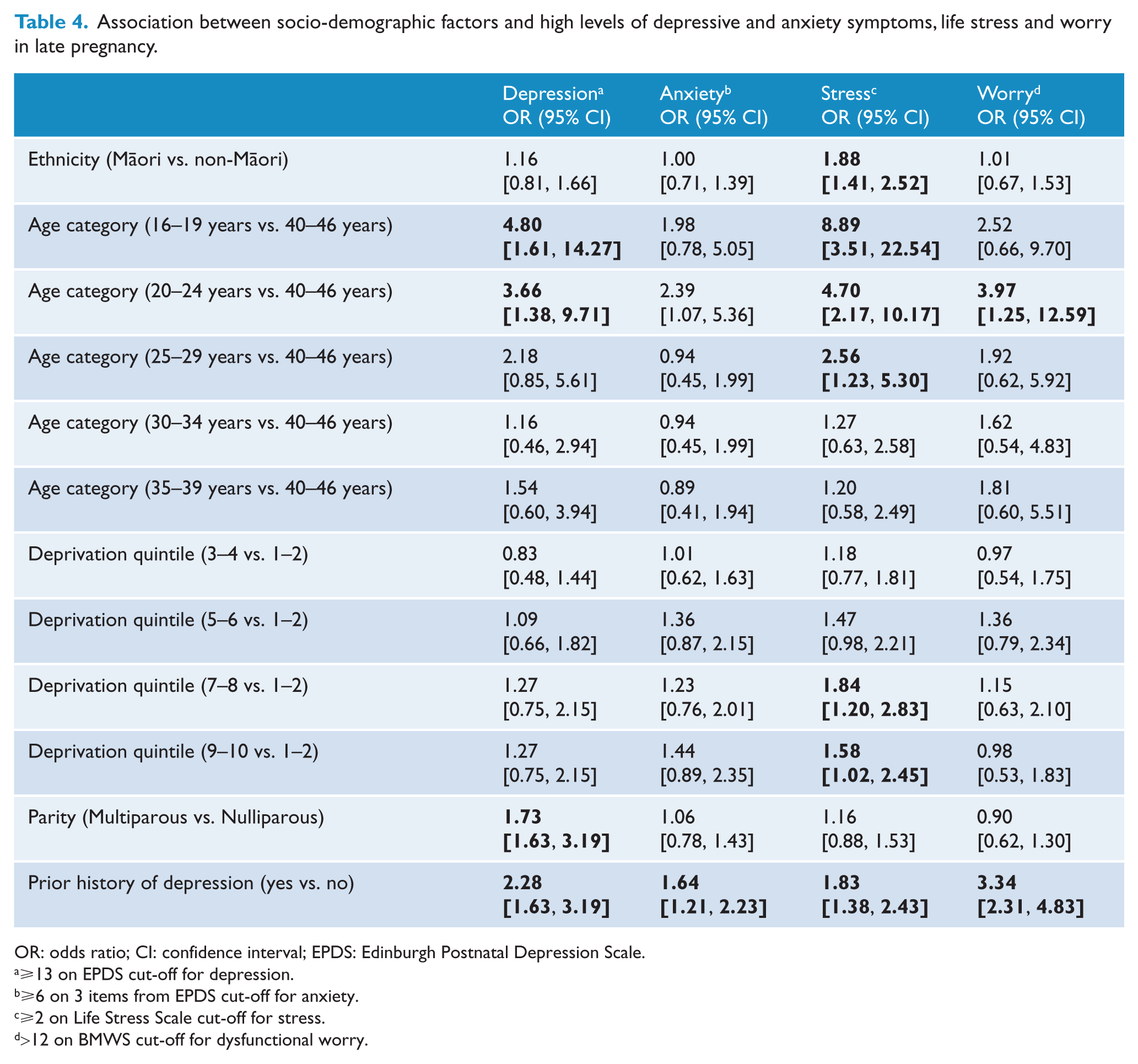
Table 4 provides the odds ratios and 95% confidence intervals for the association between ethnicity, age, deprivation quintile, parity and prior history of depression and symptoms of depression and anxiety, life stress and dysfunctional worry. Findings indicate that women who are under 25 years of age, already have at least one child and have a prior history of depression are at greater risk of experiencing clinically significant levels of depressive symptoms in pregnancy. Results also indicate that ethnicity is independently associated with a greater likelihood of experiencing significant life stress in pregnancy, as is being younger, more socio-economically deprived and having previously been diagnosed with depression. A previous history of depression was independently associated with anxiety and dysfunctional worry as well.
Association between socio-demographic factors and high levels of depressive and anxiety symptoms, life stress and worry in late pregnancy.
OR: odds ratio; CI: confidence interval; EPDS: Edinburgh Postnatal Depression Scale.
⩾13 on EPDS cut-off for depression.
⩾6 on 3 items from EPDS cut-off for anxiety.
⩾2 on Life Stress Scale cut-off for stress.
>12 on BMWS cut-off for dysfunctional worry.
Being between 20 and 24 years of age was independently associated with an increased likelihood of reporting dysfunctional worry in pregnancy. It also appears that with increasing age, the risk of experiencing clinically significant levels of depressive symptoms and significant life stress declines.
Discussion
This study investigated the prevalence of a range of negative affective states in pregnancy including symptoms of depression and anxiety, and the occurrence of life stress and dysfunctional worry in a large sample of pregnant New Zealand women.
Prevalence of negative affective states
Findings demonstrate that Māori women are disproportionately affected by depression, anxiety and life stress in pregnancy. Nearly 20% of Māori women reported a period of ⩾2 weeks of poor mood during their current pregnancy, approximately a quarter reported significant levels of symptoms of depression and anxiety in late pregnancy and over half experienced excessive life stress. The prevalence of these symptoms is at least as high as that seen in international samples (Gavin et al., 2005), and possibly higher. The proportion of non-Māori women reporting depressive symptoms in late pregnancy are lower than those seen for Māori women but are within the range seen internationally (Andersson et al., 2003; Gavin et al., 2005; Giardinelli et al., 2012).
The rates found in this study are slightly higher than those found in a recent study of pregnant New Zealand women (Waldie et al., 2015) (non-Māori 15.3% in this study vs 11% in GUiNZ; Māori 22% in this study vs 17.5% in GUiNZ). The slightly higher rates found in the present sample could be due to the data collection methods and/or sample characteristics. It has been noted that pregnant women may be reluctant to reveal their mental health concerns (Kingston et al., 2014), thus completing the EPDS anonymously and on paper rather than in a face-to-face context may elicit more honest responses. This study was advertised as being about sleep in the perinatal period and consequently women who had concerns about their sleep, which could have been related to mental health issues, may have been more likely to participate.
Despite differences between the two studies, findings from both indicate that antenatal depression and anxiety require at least as much attention and resourcing in New Zealand as postnatal mental health and that services need to be carefully designed to meet the needs of Māori women in order to address inequities.
Factors independently associated with negative affective states
The findings from the multivariable logistic regression models show that inequities in depressive symptoms between Māori and non-Māori are not due to ethnicity per se. Instead being younger, having previously had at least one child and having a prior history of depression are associated with a higher likelihood of experiencing depressive symptoms. Yet, because Māori women are more likely to have children at a younger age and have multiple children, they are disproportionately affected by depressive symptoms.
Being Māori was independently associated with reporting significant life stress even after controlling for other risk factors. It is likely that additional factors, not measured in this study are responsible for this association. Major life stress has previously been associated with both pre-term birth and lower birth weight babies (Dunkel Schetter and Tannner, 2012). Antenatal health services need to consider how best to identify life stress in pregnant women, with simple screening tools such as those used in this study, a possible option, and how women with significant life stress can be supported to minimise the consequences.
Compared with other risk factors investigated in this study, younger women have the greatest odds of reporting clinically significant depressive symptoms and significant life stress in pregnancy. Women between 16 and 19 years are 4.8 times more likely to experience depressive symptoms and are nearly nine times more likely to report significant life stress compared with older pregnant women. This risk appears to decline with increasing age. It is not clear, however, why increasing age is protective, and whether features often associated with older age such as greater life experience, increased emotional and financial stability or more developed support networks could explain this finding. The issue of depression in younger pregnant women is deserving of further investigation.
Although financial security could hypothetically play a role in protecting women from experiencing negative affect in pregnancy, socio-economic status, as measured using the New Zealand deprivation index, was not independently associated with symptoms of depression and anxiety or with dysfunctional worry in this study. The most consistent independent predictor of different states of negative affect was a prior history of depression. This finding has been noted in previous research on risk factors for depression, anxiety and stress in pregnancy (Bunevicius et al., 2009; Fadzil et al., 2013; Lancaster et al., 2010), suggesting that this is a key question pregnant women should be asked by those providing antenatal health care.
Help-seeking behaviour
Importantly, in this study less than 50% of women who had experienced ⩾2 weeks of poor mood during the current pregnancy had sought help. It is unclear why rates of seeking professional help were so low. However, this finding indicates a need to raise awareness among pregnant women about the signs and symptoms of depression, the range of available services and to ensure maternal health providers are sufficiently educated about screening and referral pathways.
Of those women with a period of poor prior mood, non-Māori women were more likely to have sought help than Māori. Non-Māori women were also more likely to have been told they were depressed or required antidepressants. The differences in rates of help-seeking point to potential inequalities between Māori and non-Māori women in access to health services, which in turn may explain the reported differences in diagnosis and medication use.
Implications of study findings
Together these findings provide crucial information as to who should be targeted when providing antenatal mental health services. Such services must reach and be tailored for Māori women. Antenatal mental health services must also be accessible to young women, women with a prior history of depression, women who live in areas of greater socio-economic deprivation and women who already have children. Education of health professionals regarding the existence of ethnic inequalities in maternal mental health outcomes and the higher risk among Māori will be an important part of a multilevel approach to reducing the detrimental impact of maternal anxiety and depression for women and their families (Smedley et al., 2002).
As well as services being available and appropriately targeted, findings regarding the low proportion of women seeking help for poor mood suggests that identifying and referring women to services will be a key part of the success of any service. In New Zealand, most pregnant women will receive antenatal care via an LMC across multiple occasions. If adequately trained and resourced, LMCs are well placed to assist in identifying women who require mental health services and in supporting them to utilise these services.
Strengths of this study include the large number of women sampled and the high proportion of Māori women who participated (35% of the total sample) which has enabled differences between Māori and non-Māori women to be identified. Compared with all women giving birth in 2012, Māori women in the current sample are marginally older than those from the general population (median = 27 years vs 25 years respectively) and more likely to be first time mothers (45% vs 34% respectively). Non-Māori women in this study are also slightly older than women from other ethnic groups in the general population (median = 32 years vs European = 31 years, Asian = 30 years, Pacific = 28 years), but the proportion of first-time mothers is very similar (54% vs 55% respectively) (Ministry of Health, 2015). The pattern of socio-economic deprivation in this sample for Māori and non-Māori women is comparable with that seen in the general population (Salmond and Crampton, 2012). These similarities support the generalisability of the current findings to the wider New Zealand population with any differences potentially leading to a slight underestimation in the risk of depression for New Zealand Māori women, who tend to be younger and already have at least one child (both shown to be independently associated with depression in this study).
This study relied on self-reported data and utilises a screening tool for depressive and anxiety symptoms rather than a clinical interview which would provide a definitive diagnosis. For these reasons, the EPDS cut-off of ⩾13 was used for categorising significant depressive symptoms, rather than ⩾10 as is used in many research settings. This higher cut-off has been shown to be sensitive and specific to serious forms of depression (Murray and Carothers, 1990). It is important, however, that the findings from this study are replicated utilising a structured psychiatric interview and/or alternative measures of depression, anxiety, life stress and worry. The study was advertised as being about sleep in pregnancy and postpartum and the relationship with maternal health. There was no specific mention of mental health, although it is possible that sleep issues are more prevalent among women with poorer mental health and therefore these women may be over-represented in our sample. Given the cross-sectional nature of the data reported here, it is not possible to infer causality between, for example, age and depressive symptoms. However, the dose-response relationship between decreasing age and the increasing odds of reporting depressive symptoms is one of the criteria for causality as defined by Bradford Hill (1965). It also must be considered that variables not measured in this particular study could influence the occurrence of depressive and anxiety symptoms, life stress and worry in pregnancy. However, the focus of this study was on key population risk factors and it was not possible to include all potential risk factors identified in previous research (e.g. Lancaster et al., 2010; Leigh and Milgrom, 2008).
In summary, this study provides crucial information on rates of depressive and anxiety symptoms, worry and life stress in pregnancy for New Zealand women and identifies stark inequities in these rates between Māori and non-Māori. It also indicates that young pregnant women are particularly at risk of experiencing depressive symptoms and significant life stress, and reaffirms the finding that a prior history of poor mental health has a consistent association with negative affect in pregnancy. These findings suggest that the adequacy of antenatal mental health services and the role of LMCs in assisting women to access these services need careful consideration. Identifying and treating women in pregnancy has the potential to reduce the rate of mental health disorders postnatally (Leigh and Milgrom, 2008) and in turn reduce the adverse consequences for both a woman and her family.
Footnotes
Acknowledgements
We gratefully acknowledge the contribution of the women who participated in ‘E Moe, Mama’. We would also like to thank Laura Howe for statistical advice; Alex Smith for assistance with data processing; Meg Thompson and Perrine Boy for their help with data entry; and the study advisory group Dr Michel Sangalli, Dr Kristie Carter, Ms Bridget Robson, Ms Rosie Smith, Dr. Kara Mihaere, and Ms Cheryl Benn for their guidance and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Council of New Zealand grant number 09/255