
Abstract
Objective:
This study aimed to evaluate whether the Therapist-assisted Online Parenting Strategies programme increased parenting behaviours known to be supportive of adolescents experiencing anxiety and/or depression. Secondary parenting outcomes of parental self-efficacy, parental accommodation, carer burden, parent–adolescent attachment, family functioning and parent distress were also examined, along with adolescent outcomes of anxiety and depression symptoms, suicidal ideation and sleep.
Method:
Seventy-one parents (94.4% females) and their adolescents (73.2% females) aged 12–18 years (Mean = 15.02, SD = 1.56) being treated for depression and/or anxiety in Australia were recruited into a single-arm double-baseline open-label trial. Parents received Therapist-assisted Online Parenting Strategies, which comprised up to nine web-based modules each supplemented with coaching sessions via videoconferencing. Outcomes were analysed using latent growth curve modelling to determine if changes to outcomes at post-intervention (4 month post-second baseline) exceeded changes between two baselines measured 1 month apart.
Results:
Sixty-five parents (91.6%) completed at least one module of the online parenting intervention and on average received nine coaching sessions (SD = 2). Parenting behaviours targeted by Therapist-assisted Online Parenting Strategies improved at post-intervention (Cohen’s d = 1.16, 95% confidence interval [0.78, 1.51]). Parent-reported parental self-efficacy and parent−adolescent attachment increased (Cohen’s d = 1.44 [1.05, 1.82] and 0.39 [0.05, 0.74], respectively), while impairments to family functioning and parent distress decreased (Cohen’s d = −0.51 [−0.86, −0.16] and −0.84 [−1.23, −0.44], respectively). Changes to adolescent anxiety, depression and sleep were not significant.
Conclusion:
The Therapist-assisted Online Parenting Strategies intervention improved self-reported parenting behaviours, parental self-efficacy, parent levels of distress, parent–adolescent attachment, and family functioning in parents with adolescents being treated for anxiety and/or depression. However, significant changes in adolescent mental health and sleep outcomes at post-intervention were not observed. The usefulness of a therapist-supported online parenting programme in addressing a service gap for parents seeking professional help is indicated.
Trial Registration:
Australian New Zealand Clinical Trials Registry Number (ACTRN) 12618000290291, prospectively registered on 26 February 2018; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=368031
Keywords
Developmental models (Schleider and Weisz, 2017) and longitudinal empirical research (Yap et al., 2014a) support the protective role of modifiable parenting factors for adolescent depression and anxiety. Defined as cognitive or behavioural factors that are in parents’ capacity to alter either through self-directed or psychological intervention, these include protective factors like parental warmth, autonomy granting and monitoring, and risk factors like inter-parental conflict, over-involvement and aversiveness (Yap et al., 2014a). Parenting programmes have demonstrated efficacy in improving these parenting factors as well as in reducing adolescent internalising symptoms (Nieuwboer et al., 2013; Yap et al., 2016).
Parents face barriers engaging with face-to-face parenting programmes due to logistical challenges such as geographical remoteness and scheduling demands (Finan et al., 2020). Self-guided online parenting programmes have been developed to overcome some of these barriers, and while shown to be efficacious for both parent and child outcomes (Nieuwboer et al., 2013), are faced with challenges such as poor programme adherence or premature termination (Hansen et al., 2019). Blended programmes that provide professional support to enhance programme adherence, while offering the flexibility of accessing online parenting content at the parent’s convenience, offer a bridge between the two models (Yap et al., 2017). Such programmes draw on the ‘Supportive Accountability’ model (Mohr et al., 2011), proposed to improve goal achievement, increase intervention adherence and maintain behaviour changes. Professional-supported online parenting programmes have yielded small-to-medium effect sizes for parenting outcomes (Nieuwboer et al., 2013).
The current study
There are very few online parenting programmes designed for parents of adolescents (Hansen et al., 2019) and none to our knowledge that addresses the needs of parents of adolescents already experiencing internalising problems (MacDonell and Prinz, 2017; Nieuwboer et al., 2013). For these families, a parenting programme may be even more valuable, not only to address the parenting factors that may maintain adolescent internalising problems (Yap et al., 2014a) but also to support parents who carry the substantial burden of caring for an unwell adolescent (Yap et al., 2017). This is especially important if youth mental health services are largely individual-focused and inadvertently exclude parents (Gopalan et al., 2010). The Therapist-assisted Online Parenting Strategies (TOPS) programme was designed to address this gap, providing parents whose adolescents have clinical-level depression or anxiety problems with individually tailored, web-based modules that target the modifiable parenting factors associated with adolescent anxiety and/or depression (Yap et al., 2017), supplemented with telehealth coaching sessions (Fulgoni et al., 2019).
The aim of this study was to examine whether the TOPS programme is associated with improvements in parenting factors associated with adolescent anxiety and/or depression, in parents whose adolescents are concurrently receiving separate treatment for these symptoms, at post-intervention. This study also examined whether TOPS is associated with various secondary outcomes, including improvements in parental self-efficacy, parent–adolescent attachment and family functioning, and reductions in carer burden, parent accommodation, parent distress, adolescent anxiety and depression symptoms, and suicidal ideation. Given the high comorbidity between sleep problems and anxiety and/or depression in adolescents (Johnson et al., 2006), and evidence indicating overlaps in the parenting factors associated with adolescent sleep (Khor et al., 2021), anxiety and depression (Yap et al., 2014a), we also examined sleep outcomes in adolescents.
Method
Trial design
The trial protocol was prospectively registered with the Australian New Zealand Clinical Trials Registry (ACTRN12618000290291). Ethics approval was received from the Monash University Human Research Ethics Committee (Application no. 11095). This study used a single-arm, double-baseline, open-label design to obtain preliminary evidence of the efficacy of the TOPS programme (Figure 1). In single-arm trials, double-baseline designs may help to account for naturalistic changes or regression to the mean that can inflate the trial’s true effect sizes (Barnett et al., 2005). Post-intervention assessments were conducted 4 months after Baseline 2, with a further follow-up (not included in this publication) 8 months post-intervention.
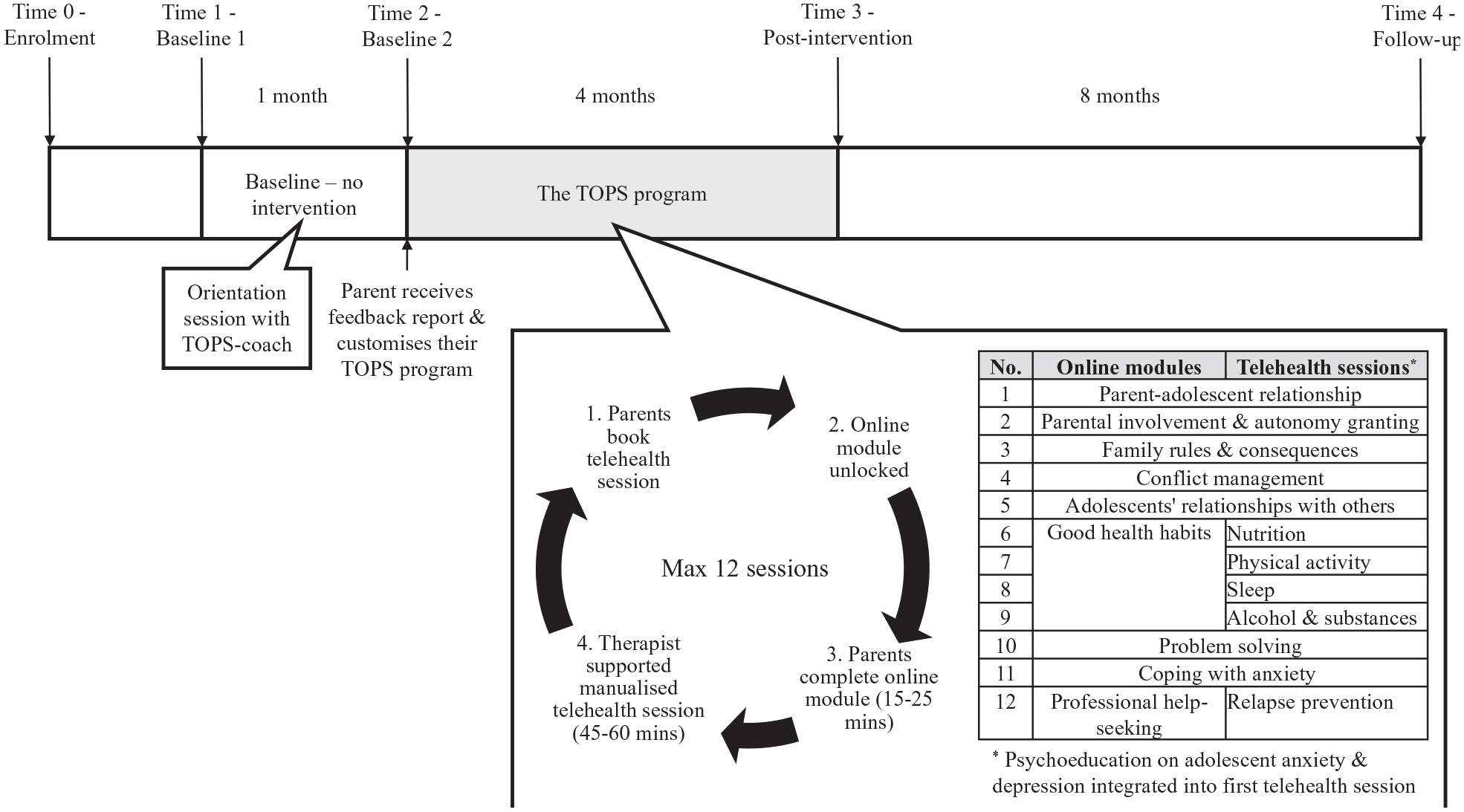
Double-baseline design for evaluating the TOPS programme with inset outlining the content of the intervention.
Participants
Parents and adolescents were recruited across Australia through schools, private psychologists working with adolescents, mental health services, social media (including targeted Facebook advertisements) and word-of-mouth (snowballing). Inclusion criteria are that participants needed to reside in Australia; be proficient in English; and have access to a telephone, Internet and email. Adolescent participants had to be aged 12–18 years and be receiving professional treatment for anxiety and/or depression (to ensure appropriate care and risk management as adolescents participated only in the research assessments, and did not receive direct intervention as part of the trial). For parsimony reasons, no more than one parent–adolescent dyad per family was enrolled.
Data collection procedures
A dedicated website was set up for participant enrolment, data collection and to run the web-based intervention (https://tops.partnersinparenting.net.au/). Additional surveys hosted online through service provider Qualtrics were integrated via links with the primary website.
Parent participants who registered for the study were telephoned by a researcher to confirm eligibility. A parent could participate without their adolescent; however, due to the parent-focussed nature of the intervention, an adolescent was not eligible to register for the study without their parent.
At each timepoint, after obtaining their verbal assent to participate, adolescents were invited by phone to complete an online survey comprising measures of mental health and sleep (30 minutes) and separately, a 1 week timestamped online sleep diary (approximately 5 minutes/day) via SMS reminders. Adolescents (n = 5) unable to complete their sleep diary online were provided with softcopy versions which were returned by email. Adolescents completed surveys during the school term, excluding holidays, and at least 3 weeks after the summer holiday break. Following submission of the adolescent assessment, parents were emailed a link to complete their assessment (60 minutes).
Parent and adolescent participants were separately reimbursed $20 for completing both baseline surveys and a further $15 for completing each post-intervention and follow-up assessments. Maximum reimbursement was $50 per participant.
Intervention
The TOPS intervention (see Figure 1 inset) is composed of two parts: (1) the Partners in Parenting (PiP) web-based intervention (Yap et al., 2018) and (2) therapist-facilitated coaching delivered via teleconference. PiP consists of an individually tailored feedback report highlighting strengths and providing strategies for further improvement in the parent’s parenting behaviours. Each parent is also automatically recommended up to nine weekly-web-based modules targeting the domains of parenting where they were assessed as being non-concordant with evidence-based (Yap et al., 2014a) and expert-consensus-based (Yap et al., 2014b) parenting guidelines (henceforth the Guidelines; Parenting Strategies Programme, 2013). These nine domains are parent–child relationship, parental involvement and autonomy granting, relationship with others, family rules and consequences, conflict management at home, good health habits (regarding nutrition, physical activity, sleep and substance use), problem solving, coping with anxiety and professional help-seeking. Parents could then choose which modules (15–25 minutes each) that they wished to complete by ‘locking in’ their selection on the PiP website.
All parents received psychoeducation about adolescent anxiety and depression in their first telehealth session. They could then have up to 12 telehealth sessions (about 45 minutes each; see Figure 1 inset), one for each PiP module, except for the Good Health Habits module where four sessions are offered, and one for each health habit (nutrition, physical activity, sleep and substance use). The content and structure of each coaching session is detailed elsewhere (Fulgoni et al., 2019).
TOPS-coaches were six provisional psychologists undertaking doctoral-level training in Clinical Psychology at Monash University. TOPS-coaches received 6 hours of direct training on top of completing self-guided training materials including the TOPS-coach manual and coaching materials. They received at least 1 hour per fortnight of clinical supervision from a senior psychologist (Authors 4, 6 or 8) and had weekly peer supervision.
Between baseline assessments, the assigned TOPS-coach facilitated an orientation session to familiarise the parent with videoconferencing technology (Zoom) and provide a general overview of TOPS (without therapeutic content).
Parents were encouraged but not required to have their TOPS-coaching sessions on a weekly basis. Zoom-recorded coaching sessions were guided by content from a standardised manual and a slide set that was annotated during the session and emailed to the parent. Once parents completed their programme, all online modules became unlocked and parents had continued access to the online programme.
Measures
Primary outcome
Parenting behaviours were measured using the Parenting to Reduce Adolescent Depression and Anxiety Scale (PRADAS; Cardamone-Breen et al., 2017), a 79-item criterion-referenced scale that assesses the self-reported frequency or likelihood of parenting behaviours against the Guidelines (Parenting Strategies Program, 2013). The PRADAS has nine subscales (6−12 items each) assessing nine parenting domains identified as modifiable risk or protective factors for adolescent anxiety or depression, which are targeted in PiP. Each item is scored as either concordant (1) or non-concordant (0) with the Guidelines. Higher subscale and total scores indicate parenting practices that are more concordant with the Guidelines. The PRADAS had good reliability in the current sample, with agreement coefficients across timepoints ranging from 0.83 to 0.93.
Secondary outcomes
Parental self-efficacy was self-reported using the Parental Self-Efficacy Scale (Nicolas et al., 2020), which had adequate internal consistency (McDonald’s ω = 0.85−0.88).
Carer burden was measured via parent-report on the Burden Assessment Scale (Reinhard et al., 1994) to assess the objective and subjective consequences of caring for their adolescent, with ω = 0.94–0.96.
Parental accommodation was measured via self-report on the Family Accommodation Scale−Anxiety (Lebowitz et al., 2013) to identify the level of parental behaviour modification used to reduce their child’s distress; ω = 0.92−0.94.
Family functioning was measured via parent and adolescent reports on the McMaster Family Assessment Device−General Functioning subscale (Epstein et al., 1983). Higher scores indicate greater impairments, with scores greater than 2 indicating significantly impaired family functioning. McDonald’s ω were 0.89−0.93 and 0.91−0.92 for parent and adolescent versions, respectively.
Parent−adolescent attachment was measured using parent (McElhaney et al., 2008) and adolescent reports (Gullone and Robinson, 2005) on the Inventory of Parent and Peer Attachment. Attachment was measured as a total scale score across three dimensions: degree of mutual trust, quality of communication, and extent of anger and alienation. McDonald’s ω were 0.90−0.93 and 0.96 for parent and adolescent versions, respectively.
Parent distress was measured using the six-item Kessler Psychological Distress Scale (K6; Kessler et al., 2002) at the beginning of their first and final telehealth session. McDonald’s ω were 0.78 and 0.81, respectively, indicating adequate scale internal consistency.
Adolescent anxiety was measured using total scores of the parent- (Nauta et al., 2004) and adolescent-report versions (Spence, 1998) of the Spence Children’s Anxiety Scale (SCAS). Total scores > 33 were defined as meeting diagnostic cut-off (Olofsdotter et al., 2016). Across timepoints, ω = 0.95−0.97 for both versions.
Adolescent depression was measured using parent and adolescent reports on the Short Mood and Feelings Questionnaire (SMFQ; Messer et al., 1995). Cut-off scores ⩾ 12 for males and ⩾ 13 for females (Thabrew et al., 2018) were indicative of clinical levels of depression. Across timepoints, ω = 0.91−0.94 for both versions.
Suicidal ideation was measured using adolescent-report on the Suicidal Ideation Questionnaire−Junior (SIQ-JR) version (Reynolds and Mazza, 1999); ω = 0.97. Total scores > 30 indicated elevated suicidal ideation (Reynolds, 1988).
Adolescents reported on sleep and waketimes, and sleep onset latency using the Consensus Sleep Diary (CSD; Carney et al., 2012). Derived variables from the CSD used in this study included total sleep time (TST; difference between time-in-bed and total time awake at night), sleep efficiency (ratio of TST and actual time-in-bed in percentage) and social jetlag (free-nights [non-school] minus constrained-nights [school] TST). Only participants who recorded observations from a minimum of three school nights and one non-school night were included in analyses.
Parent- and adolescent-reported Patient-Reported Outcomes Measurement Information System® (PROMIS) for Paediatric Sleep Disturbance (PROMIS-SD) and Paediatric Sleep-Related Impairment (PROMIS-SRI; Forrest et al., 2018) were used to measure subjective quality of night-time sleep and daytime wakefulness, respectively. McDonald’s ω = 0.89−0.92 and 0.92−0.95 for adolescent-report of PROMIS-SD and PROMIS-SRI, respectively, with ω = 0.95−0.96 for parent-report of both PROMIS-SD and PROMIS-SRI.
Adolescents reported on chronotype (optimal time-of-day subjective alertness and functioning preferences) using the Composite Scale of Morningness (Smith et al., 1989). McDonald’s ω = 0.86−0.88.
Participant characteristics
Parents provided demographic data at registration and postcodes were used to impute participants’ state and geographical remoteness locations, as well as their neighbourhood socioeconomic position. Neighbourhood socioeconomic status was derived from the Australian Bureau of Statistics 2016 Socio-Economic Indexes for Areas Index of Relative Socio-Economic Advantage and Disadvantage (SEIFA; Australian Bureau of Statistics, 2018).
Treatment fidelity
Using predetermined checklists, two independent observers rated 50 (11.2%) video-recorded sessions assessing whether the TOPS-coach delivered the key content within each module. One coaching session per parent (excluding Orientation) was selected at random. The average number of items in each checklist was 27, with a range from 17 (Psychoeducation) to 46 (Sleep) items. Items were coded as 0 (no) or 1 (yes) and the percentage of the maximum possible score for the module was calculated. Intraclass-correlation between the two coders was 0.91 (95% confidence interval [CI] [0.81, 0.96]), indicating good to excellent inter-rater reliability.
Programme evaluation
Parents reported on treatment satisfaction and acceptability at post-intervention through five items: (1) ‘Have you used any parenting strategies that were discussed in TOPS in the past 4 months?’ (2) ‘How would you rate your relationships with your TOPS-coach?’ (3) ‘Were you able to work on the goals and topics of your choice with your TOPS coach?’ (4) ‘To what extent did working with your TOPS-coach help you to apply the parenting strategies to your situation?’ and (5) ‘To what extent would you recommend the TOPS program to other parents whose adolescents are experiencing anxiety, depression and related sleep disorders?’ The first question was dichotomised to a ‘yes’ or ‘no’ response; the remaining questions were scored from 1 (low) to 5 (high).
Sample size
A total of 70 participants were estimated to provide sufficient power (.80) at α = 0.05 level assuming an effect size of Cohen’s d = 0.35 and attrition rate of 15% (Faul et al., 2007). The sample size was derived based on the smallest expected effect size across primary outcomes.
Statistical methods
Descriptive statistics and preliminary data analysis using t- and χ2 tests were conducted using Stata 16.0.
Pre- to post-intervention change for the K6 was examined using a repeated-measures t-test using pairwise deletion.
Latent growth curve (LGC) modelling in Mplus 7.2 (Muthén and Muthén, 2012) was used to assess efficacy of all other outcomes. Missing data were handled by full-information maximum likelihood method and application of 10,000 bootstrap draws provided robust estimates examining the change between Baselines 1 and 2 (s1), as well as estimates comparing the slope from Baseline 2 to post-intervention (s2; Preacher et al., 2008). Models were specified with fixed slopes and random intercepts. Statistically significant differences between s1 and s2 indicated that the parenting intervention improved the outcome measured. Supplementary analyses of the nine PRADAS parenting domains were also conducted using LGC modelling. Cohen’s (1992) guidelines were used to categorise effect sizes of outcomes (d = 0.2, 0.5 and 0.8 for small, medium and large, respectively).
Results
Figure 2 presents the CONSORT flow diagram of participants. Of 83 parents who enrolled in the trial between 28 March 2018 and 21 May 2019, 66 completed assessments at Baseline 2 and 65 subsequently received the intervention. Post-intervention surveys were collected between 3 October 2018 and 26 May 2020.
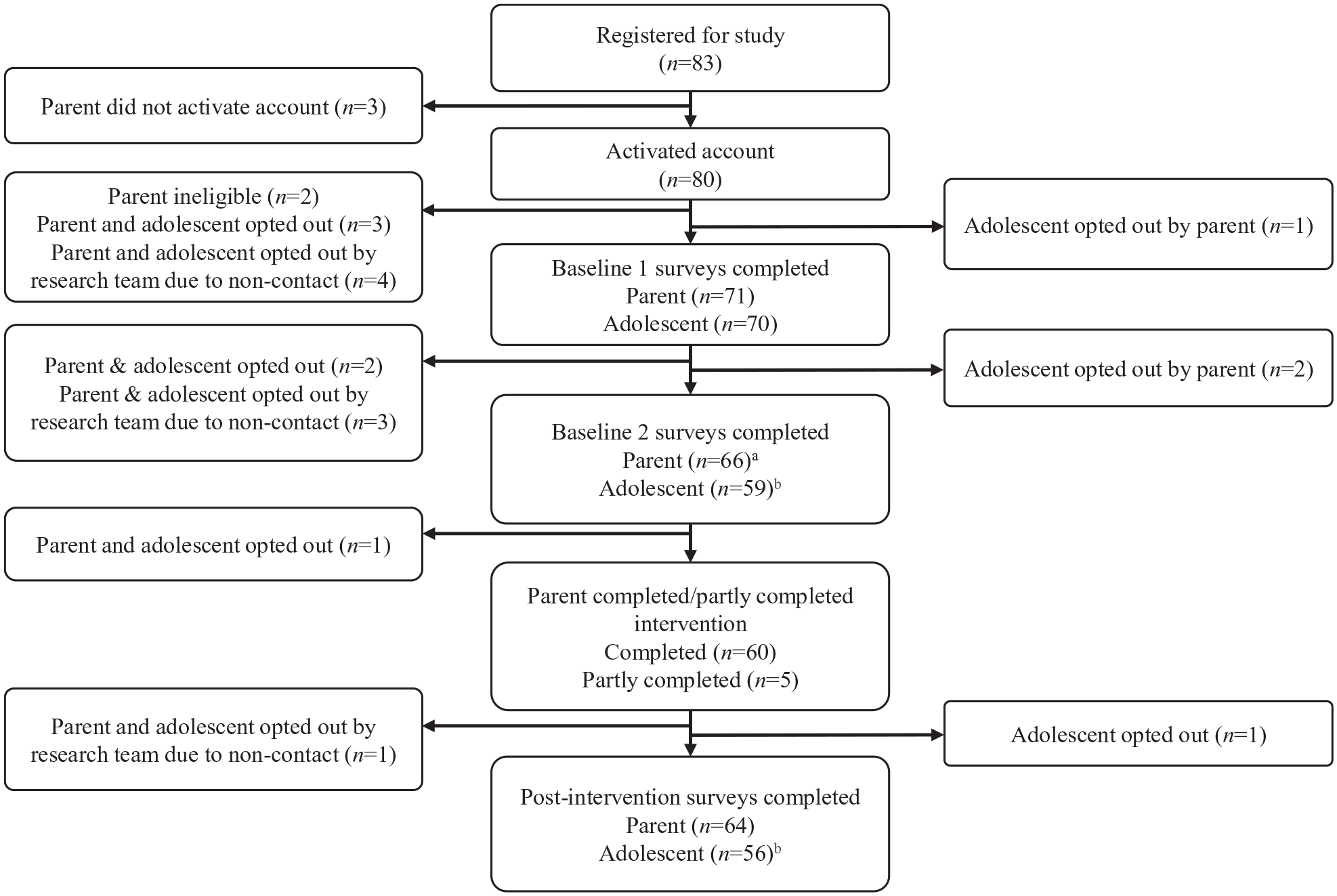
Participant flow diagram.
Participant characteristics
The mean ages of parents and adolescents were 47.72 (SD 5.14) and 15.02 (SD 1.56) years, respectively. Parent and adolescent sample characteristics at Baseline 1 are presented in Tables 1 and 2, respectively. Compared to 2016 Australian census data of Australians over 18 years (see Supplementary Material for details), participants were generally from higher neighbourhood socioeconomic positions (Z = 4.82, p < 0.001) but did not vary by population-distributed remoteness of geographical location, χ2(4) = 5.11, p = 0.276.
Parent characteristics at Baseline 1.
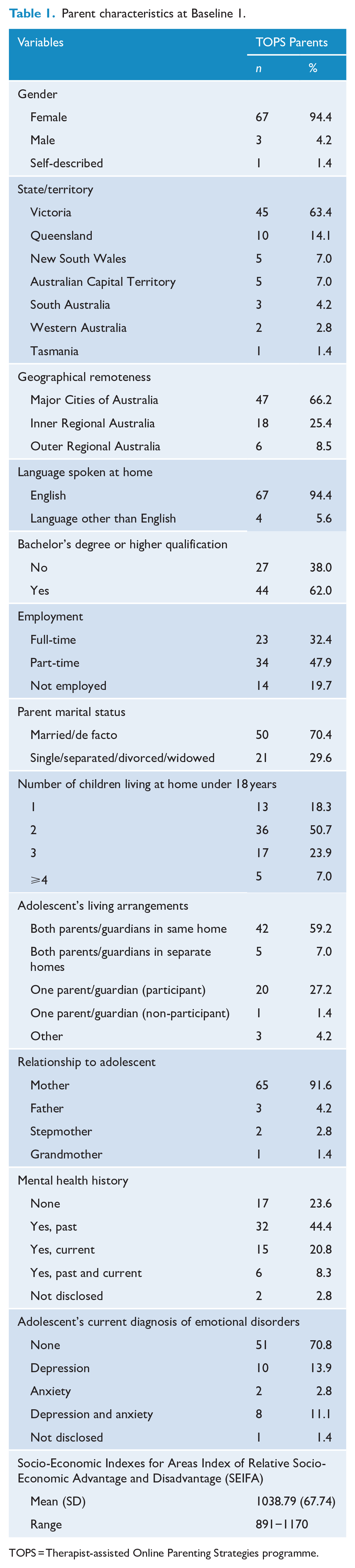
TOPS = Therapist-assisted Online Parenting Strategies programme.
Adolescent characteristics at Baseline 1.
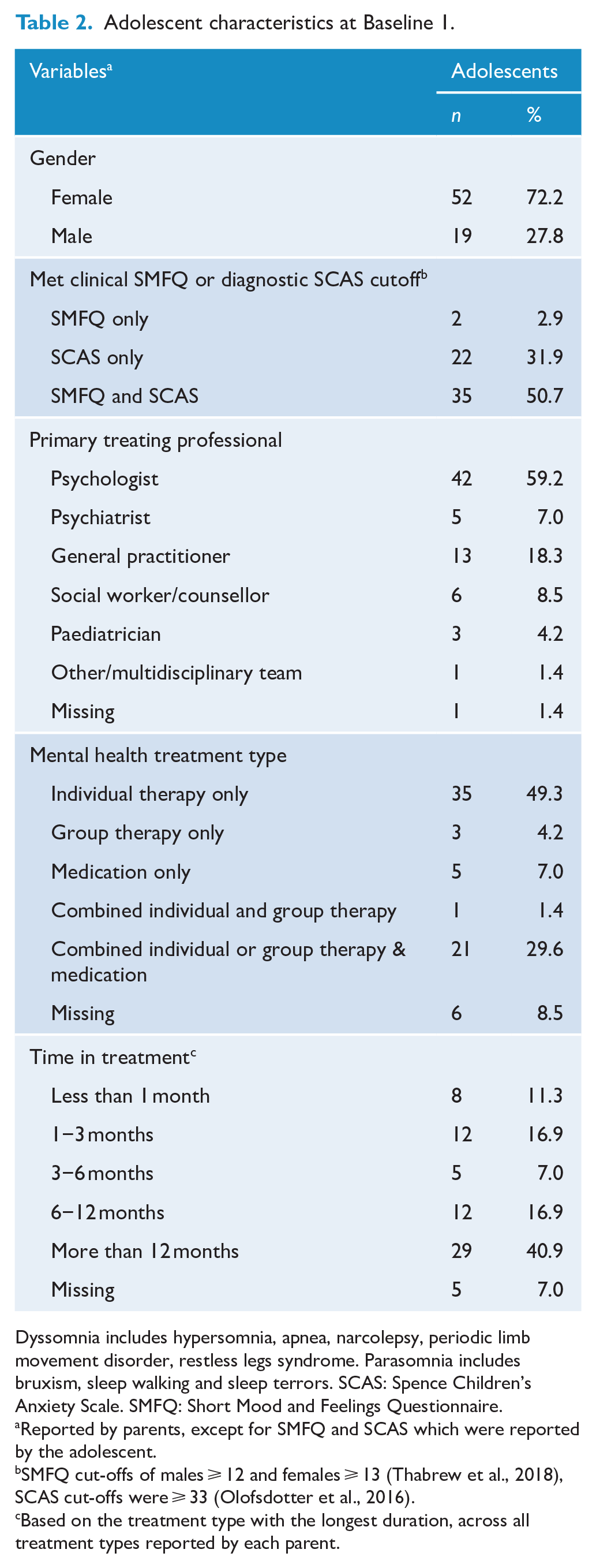
Dyssomnia includes hypersomnia, apnea, narcolepsy, periodic limb movement disorder, restless legs syndrome. Parasomnia includes bruxism, sleep walking and sleep terrors. SCAS: Spence Children’s Anxiety Scale. SMFQ: Short Mood and Feelings Questionnaire.
Reported by parents, except for SMFQ and SCAS which were reported by the adolescent.
SMFQ cut-offs of males ⩾ 12 and females ⩾ 13 (Thabrew et al., 2018), SCAS cut-offs were ⩾ 33 (Olofsdotter et al., 2016).
Based on the treatment type with the longest duration, across all treatment types reported by each parent.
Thirty-eight (53.5%) parents and 47 adolescents (68.1%) reported impairments to family functioning above clinical cut-offs (Miller et al., 1985) at Baseline 1. Family accommodation scores from the TOPS sample were similar to another study of clinically anxious youth (Lebowitz et al., 2014).
Thirty-seven (53.6%) and 57 (82.6%) adolescents independently met SMFQ clinical (Thabrew et al., 2018) and SCAS diagnostic (Olofsdotter et al., 2016) cut-off scores, respectively; of these, 36 (51.4%) met both SMFQ and SCAS cut-offs. Elevated suicidal ideation (SIQ > 30) was observed in 24 (34.8%) adolescents.
In addition, 43 (65.2%) adolescents slept less than National Sleep Foundation guidelines for their age (Hirshkowitz et al., 2015), and 50 (72.4%) and 44 (63.8%) scored one standard deviation above the normative mean for PROMIS sleep disturbance and sleep-related impairment, respectively (Forrest et al., 2018).
Parent attrition was highest between registration and Baseline 1 (n = 12, 14.5%), decreasing to 7.0% (n = 5) between Baseline 1 and 2, and 3.0% (n = 2) between Baseline 2 and post-intervention. Survey completion rate was lower for adolescents, although only four adolescents opted out of the study entirely between Baseline 1 and post-intervention. Adolescent survey non-completion was 16.9% (n = 12) between Baseline 1 and 2, and 6.8% (n = 4) between Baseline 2 and post-intervention. With the exception that parent participants who dropped out were more likely to be male, χ2(2) = 6.21, p = 0.045, retained participants and participants who dropped out were similar across demographic measures at registration and, parenting or adolescent mental health measures at Baseline 1.
Due to technical issues, module completion rates were only available for 55 parents. Parents were recommended a mean of 6.45 modules, of which they completed 87.6%. On average, parents who commenced the programme received nine TOPS-coaching sessions (SD = 2, range = 1−13) and a total coaching time of 6−9 hours. Four parents (7.27%) dropped out of the coaching component after commencing their programme, but continued to have access to online modules. Frequencies of each TOPS module delivered are shown in Table 3.
Frequencies of each TOPS module delivered (N = 55).
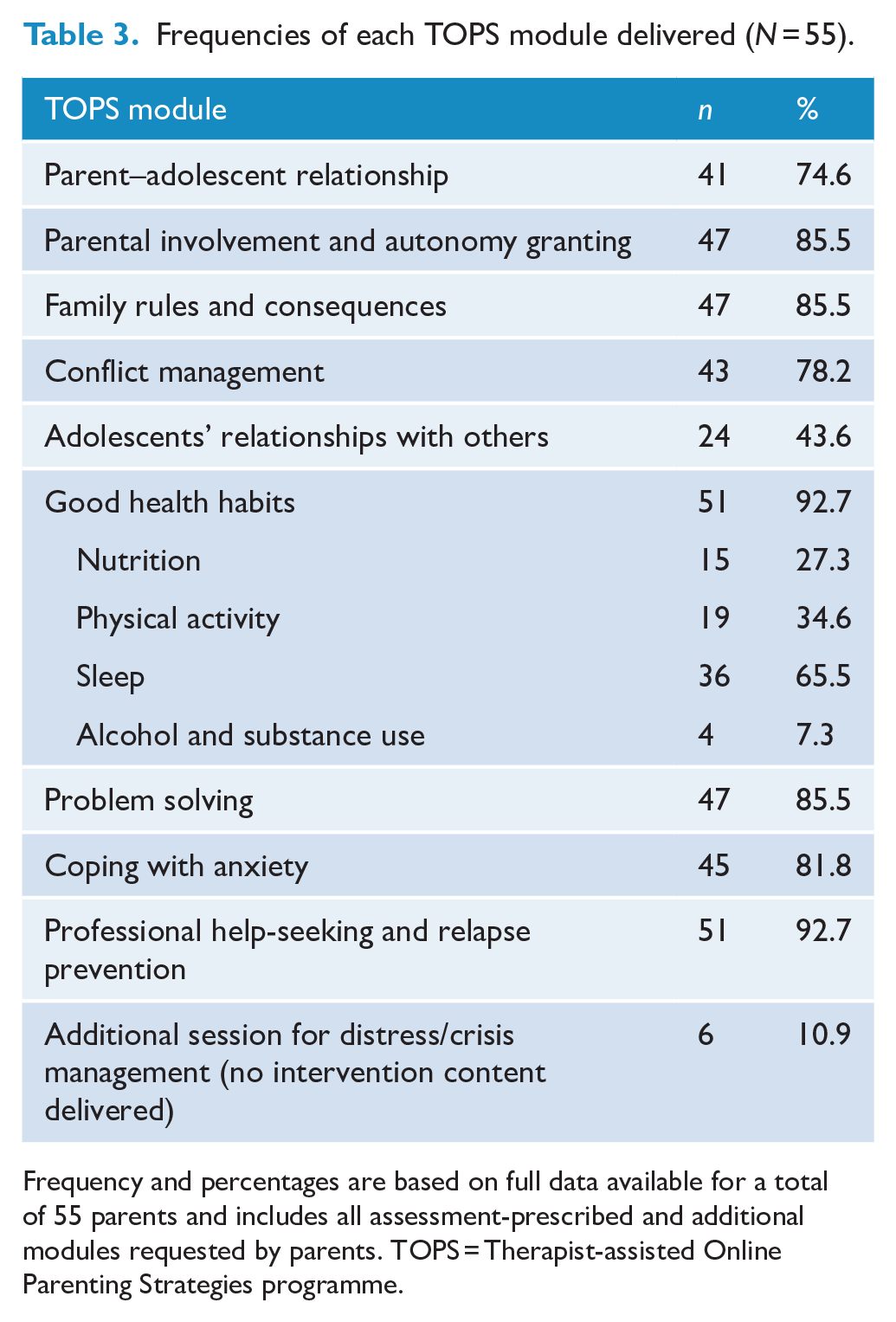
Frequency and percentages are based on full data available for a total of 55 parents and includes all assessment-prescribed and additional modules requested by parents. TOPS = Therapist-assisted Online Parenting Strategies programme.
Pearson correlations (Table 4) revealed medium to large positive correlations between parent- and adolescent-reported measures of family functioning, attachment, adolescent anxiety, depression, sleep disturbance and sleep-related impairment.
Pearson correlations between parent- and adolescent-reported measures at each timepoint.
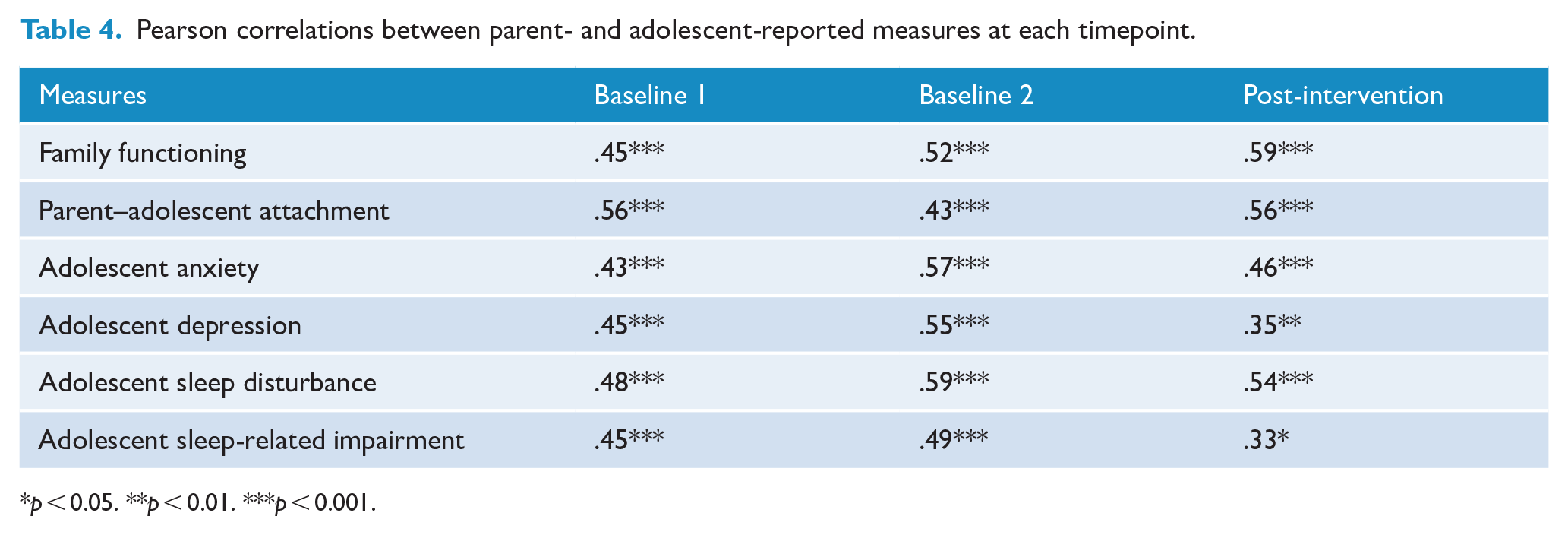
p < 0.05. **p < 0.01. ***p < 0.001.
Descriptive statistics and intervention effects for all outcomes are presented in Table 5.
Summary of outcomes and analyses from the TOPS intervention.
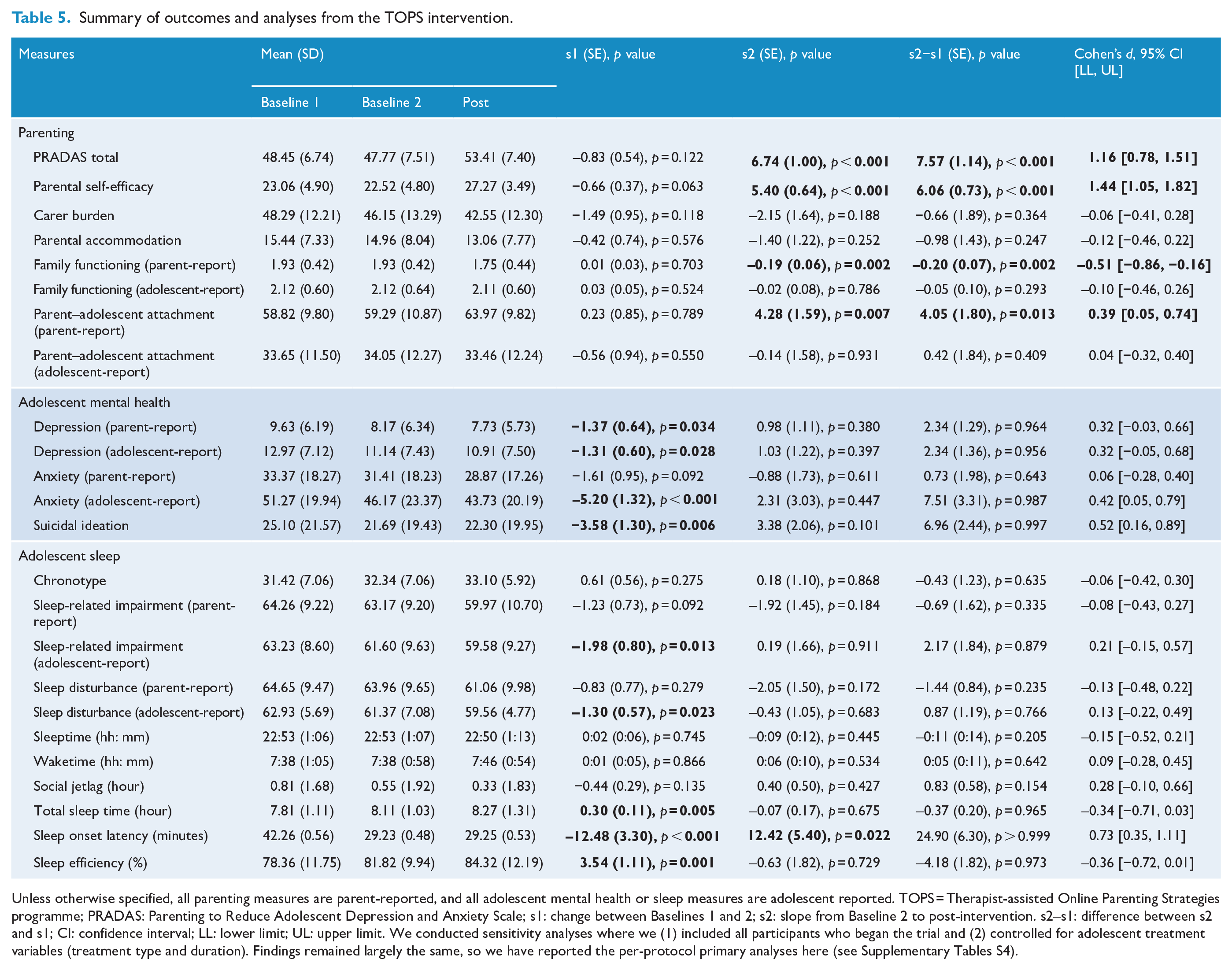
Unless otherwise specified, all parenting measures are parent-reported, and all adolescent mental health or sleep measures are adolescent reported. TOPS = Therapist-assisted Online Parenting Strategies programme; PRADAS: Parenting to Reduce Adolescent Depression and Anxiety Scale; s1: change between Baselines 1 and 2; s2: slope from Baseline 2 to post-intervention. s2–s1: difference between s2 and s1; CI: confidence interval; LL: lower limit; UL: upper limit. We conducted sensitivity analyses where we (1) included all participants who began the trial and (2) controlled for adolescent treatment variables (treatment type and duration). Findings remained largely the same, so we have reported the per-protocol primary analyses here (see Supplementary Tables S4).
Primary outcomes
Relative to changes across baseline assessments, parenting behaviours associated with reducing adolescent anxiety and/or depression as measured by the PRADAS total score were increased at post-intervention. The effect size was large. Post hoc analyses (see Supplementary Material) showed improvements to six of nine PRADAS parenting domains – parental involvement, family rules, home environment, good health habits, problem solving and coping with anxiety.
Secondary outcomes
Parent-reported outcomes of parental self-efficacy, family functioning and parent–adolescent attachment were improved at post-intervention relative to changes between baseline assessments. The effect size for parental self-efficacy was large, while effect sizes for family functioning and attachment were small-to-medium. Improvements to adolescent-reported family functioning or attachment were not observed. Carer burden, parent accommodation, and adolescent-reported family functioning and attachment showed non-significant improvements between Baseline 2 and post-intervention relative to the changes between the two baselines.
Fifty-four parents reported on both their level of distress (K6) at the beginning of the first (Mean = 11.72, SD = 3.73) and final (Mean = 8.91, SD = 2.93) TOPS sessions. Mean scores were below the cut-off score indicating probable mental illness (K6 < 19; Furukawa et al., 2003); however, a decrease in distress levels (t = 6.76, p < 0.001) of a large effect size (Cohen’s d = −0.84, 95% CI [–0.44, −1.23]) was observed.
Parents and adolescents reported significant improvements to adolescent depression symptoms between baseline assessments. Adolescents but not parents also reported significant improvements to their anxiety symptoms between baseline assessments. However, relative to changes between baseline assessments, both parent- and adolescent-reported adolescent anxiety and depression were not significantly different at post-intervention. While suicidal ideation decreased between baseline assessments, further improvement at post-intervention relative to the drop between baselines was not significant.
Improvements to adolescent-reported sleep measures of sleep disturbance, sleep-related impairment, TST and sleep efficiency between baseline assessments were significant, but there was no further improvement at post-intervention relative to the initial decrease. Sleep onset latency was increased at post-intervention relative to Baseline 2; however, this was not related to parents’ completion of the sleep module (p = 0.545) or PRADAS change scores (p = 0.429) between Baseline 2 and post-intervention. Chronotype, sleeptime, waketime, social jetlag and parent-reported sleep disturbance and sleep-related impairment were no different between baseline assessments or Baseline 2 and post-intervention.
Treatment fidelity
TOPS-coaches on average delivered 90.6% (SD = 9.4%; range = 58.4−100%) of the content in the standardised manual for each of their sessions to parents, as rated by two independent observers.
Programme evaluation
Sixty-two (96.9%) parents reported using parenting strategies discussed in TOPS at post-intervention. Parents were largely satisfied with the programme, with a majority reporting a good relationship with their coach. As a result of this relationship, parents reported being able to work on their chosen goals and apply the parenting strategies on offer (Figure 3). Most parents would highly recommend the programme to other parents with adolescents experiencing internalising problems.
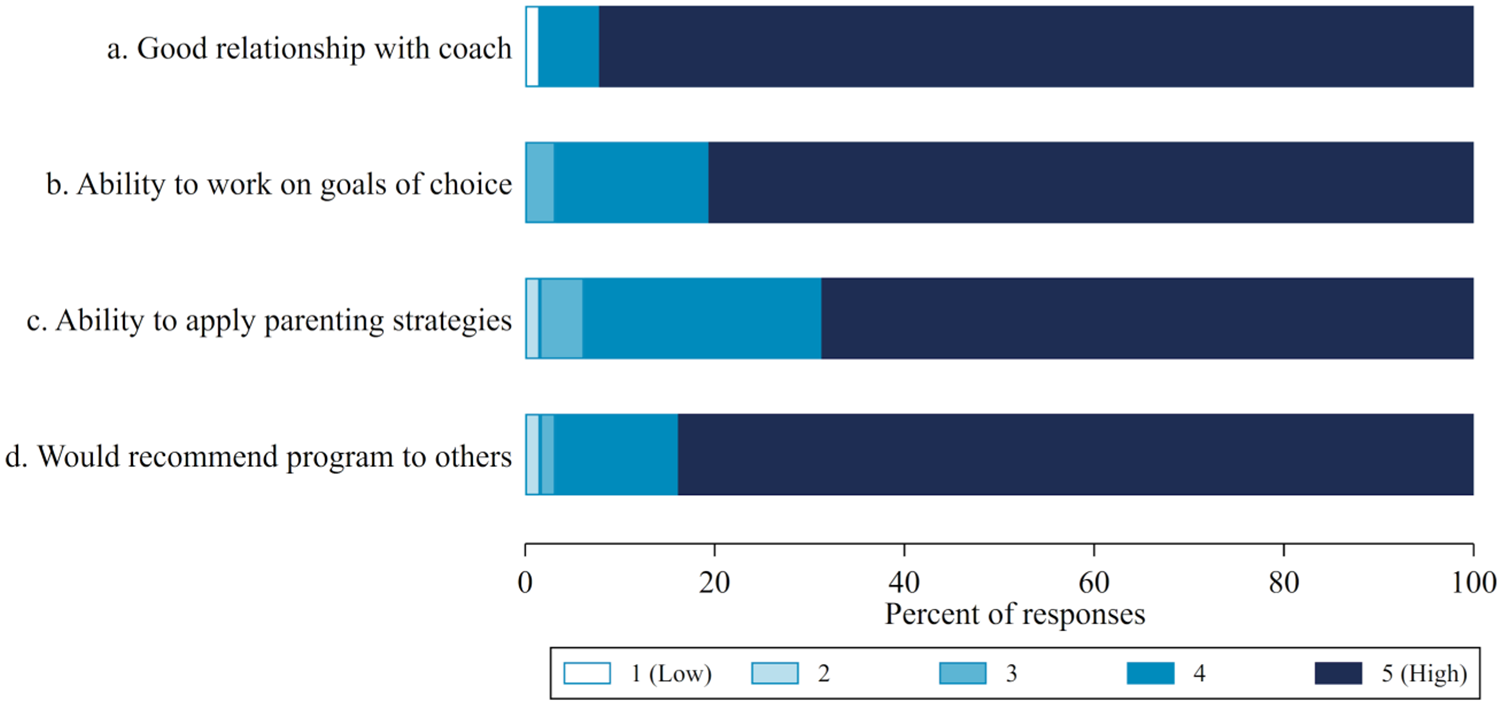
Evaluation of programme satisfaction at post-intervention.
Discussion
To the best of our knowledge, this study is the first to evaluate a therapist-assisted online parenting programme for parents who are supporting adolescents undergoing treatment for depression or anxiety. Over half of all parents reported scores above cut-off for family functioning impairments, but mean levels of parent distress remained below cut-off. Most adolescent participants reported anxiety symptoms above the cut-off score, and over half were above cut-off for depression; however, suicidal ideation was on average below cut-off. Using a single-arm double-baseline open-label trial design, we found improvements in parenting factors associated with anxiety and/or depression in adolescents, after controlling for naturalistic changes between two baselines taken over a 1-month period. Parents reported improvements in adaptive parental involvement and autonomy granting, age-appropriate family rules implementation, and adaptive conflict management, and supporting their adolescent’s problem solving and coping with anxiety. Due to ceiling effects, parents did not report improvements in the parent–adolescent relationship, their approach to professional help-seeking or in supporting their adolescents’ relationship with others.
The intervention was also associated with improved parent-reported parental self-efficacy, parent–adolescent attachment and family functioning at post-intervention, along with lowered parent distress at the end of the TOPS programme. The intervention was not associated with a significant reduction in levels of carer burden, parent accommodation, adolescent anxiety, depression, suicidal ideation or improved adolescent sleep, partly due to changes between baselines.
In the literature, interventions involving parents have shown greater efficacy in modifying parenting behaviours, compared to youth outcomes (MacDonell and Prinz, 2017). Effect sizes for this study were comparable to two other studies with technology-based parenting interventions non-specific to adolescent internalising problems, which secondarily assessed internalising symptoms (Kacir and Gordon, 2000; Villarruel et al., 2010). Yet, the literature has shown either much smaller effect sizes or mixed results on youth outcomes for these interventions (Nieuwboer et al., 2013). The TOPS programme, designed principally as a parenting-focussed intervention to support adolescent internalising problems, is no exception. We frame our interpretation of our findings around the target (problems being intervened with) and design (parent-focussed vs adolescent-focussed) of interventions as key factors to explain the limited effects of the intervention on adolescent outcomes.
First, externalising problems tend to be more reliably observed and interpreted by cross-informants than internalising problems, which being less perceptible, may be misidentified by external observers including parents (Achenbach et al., 1987; Youngstrom et al., 2000). As a result, parenting interventions that directly address externalising behaviours in adolescents (Sanders et al., 2014) have been more successful relative to those targeting internalising problems (Fang and Schinke, 2013), like in TOPS. Furthermore, TOPS coaches primarily work with the parent alone, with limited input from the adolescent, to address broader family-level systemic issues that may contribute to the adolescent’s internalising difficulties. To target adolescent internalising problems more accurately, inclusion of the adolescent as a part of the assessment process prior to the parent commencing their programme may be helpful in future studies.
Second, the extent and purpose of parental inclusion in interventions supporting adolescent internalising problems should be considered (MacDonell and Prinz, 2017). Most promising for adolescent outcomes were adolescent-focussed interventions targeting individual-level factors using cognitive-behavioural therapy, with parent involvement as behavioural coaches to support adolescents with the application of an exposure hierarchy protocol demonstrating short-term efficacy in reducing adolescent anxiety (Spence et al., 2011). In contrast, parent-focussed interventions may not necessarily provide direct treatment for the adolescent. Parents’ involvement in these interventions, whether through psychoeducation or parenting strategies to reduce problems originating at the family-system level, have consequently shown more mixed outcomes for adolescents in the short term. Given the primary purpose of TOPS is to support parents who are seeking alternative approaches to relate with their adolescent, it is perhaps not surprising that TOPS has demonstrated short-term efficacy with parenting but not adolescent outcomes.
Although the inconsistency in effects of parental involvement in the treatment of adolescent internalising disorders has been acknowledged (James et al., 2020), the case for targeting parent or family-factors in interventions remains (Schleider and Weisz, 2017). Specifically, longer term effects on adolescent internalising difficulties should not be discounted. The current study comprised mostly of adolescents who have been treated for long-term internalising difficulties, so improvements in parenting and parent–adolescent dynamics may require a longer timeframe to translate to adolescent internalising symptom reduction. As such, the 4-month post-intervention adolescent outcomes may not reflect changes that are expected in the longer term. Further support for this is provided in various parent-focussed interventions that target parent–adolescent socioemotional factors for youth internalising outcomes, reporting a significant reduction to internalising problems at 8–12 months follow-up timeframes rather than immediately at post-intervention (Kehoe et al., 2014; McGrath et al., 2011; Yap et al., 2019), as well as a review of parenting interventions where a range of adolescent outcomes were realised between 3 and 15 years post-intervention (Sandler et al., 2010).
Despite the limited short-term success with adolescent outcomes, the TOPS programme was associated with improvements in secondary outcomes of parental self-efficacy, parent–adolescent attachment, family functioning and parent distress. Positive-reinforcement of parental self-efficacy has been associated with successes in parenting and subsequent successes with youth outcomes, reductions in parental distress and ongoing use of adaptive parenting strategies (Jones and Prinz, 2005). Similar implications are indicated in TOPS, whereby parents have stronger beliefs in their own ability to influence their adolescents, will experience less distress and be more likely to persist with using parenting strategies provided. Furthermore, increases to parent–adolescent attachment indicated parent–adolescent relationships were improved as a composite of mutual trust and communication quality and relational alienation, while decreases in impairments to family functioning suggested improved family dynamics of cohesion, role organisation and communication. These findings support the generalisation of the TOPS intervention effects on primary targeted parental behaviours protective against adolescent anxiety and/or depression, through improving broader parent–adolescent relationship and family-level factors, while providing direct benefits to parents in reducing the distress they were experiencing.
The limited changes to carer burden and parental accommodation at post-intervention may be partly explained by the TOPS programme not addressing these domains adequately. TOPS-coaching sessions did not incorporate parent self-care, and while parents were encouraged to increase their adolescents’ autonomy, this was non-specific to reducing parental accommodation. So, any effect, if present, would be too small to be detected with this sample size. Moreover, as it is likely that carer burden would be positively correlated with adolescent mental health, the non-significant changes to carer burden may also be associated with the limited resolution of adolescent internalising symptoms at post-intervention.
Our study noted discrepancies between significant parent-reported and non-significant adolescent-reported attachment and family functioning outcomes, despite medium to large correlations between parent and adolescent reports. This is not unusual in parenting research (Branje et al., 2013), but remains an area for further investigation.
Strength and limitations
One strength of this study was the uptake of the TOPS programme by participants (about one-third) living in regional parts of Australia, who potentially had less access to psychological services. It renders support for the provision of online mental health–related services for those living in remote areas. The intervention itself addresses an important gap in support services for parents and carers of adolescents with internalising disorders, who might feel helpless either due to being excluded or dismissed in a service model that takes an individualised approach in treating adolescent mental health problems (Yap et al., 2017). Parents’ positive feedback about the programme, as well as low drop-out rates once they commenced their programme, offered further support for the programme’s acceptability. As one of few programmes offering professional support through a telehealth modality, along with high treatment fidelity, TOPS offers an indication that online delivery of psychological services can be efficacious in the context of parenting. Another strength of the study is the involvement of multiple informants for parenting and adolescent mental health outcomes, which provides a more holistic perspective of the intervention’s efficacy.
Because the TOPS intervention is new and deals with a vulnerable clinical sample, the trial utilised a single-arm open-label design prior to implementation in a randomised controlled trial. Although the double-baseline approach provided some control for potential confounds of testing effects, trajectory of concurrent adolescent treatment effects or naturalistic changes in internalising difficulties, ongoing confounding factors such as family situational factors, adolescent developmental changes over time and ongoing adolescent treatment effects cannot be fully accounted for with a single-arm design. For example, improvements to adolescent-reported anxiety, depression and some sleep domains between baselines were notable in our study. Given that over half of the adolescents had been in treatment for 6 months or more, and that parents reported decreased limit setting and increased professional help-seeking subscales of the PRADAS between the two baselines assessments, we speculated that at the point of study enrolment by parents, their adolescents may have been acutely unwell, with scope to resolve significantly between baselines. Nonetheless, sensitivity analyses controlling for adolescent treatment variables indicated that our findings were largely robust, despite a reduction in effect sizes. The only exception was with parent-reported adolescent sleep impairment, which showed a significant improvement after controlling for adolescent treatment variables. A trial with a control arm is required to better account for non-intervention related changes over time.
It is also noted that most parents in this sample were females or mothers, highly educated, with above-average socioeconomic positions, and were likely more motivated, on average, to persist with the programme. Therefore, generalisability of our findings may be limited to these demographic subgroups. Technical issues also resulted in the loss of some data (e.g. K6) for 10 parents.
Conclusion
Parents of adolescents being treated for anxiety and/or depression who received a therapist-supported online parenting intervention reported improved parenting, parental self-efficacy, parent–adolescent attachment and family functioning at post-intervention. Although intervention effects were not observed for adolescent mental health and sleep outcomes in the short term, results indicate the usefulness of such a programme in addressing a service gap for parents seeking professional help to support their adolescents.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211025695 – Supplemental material for Short-term outcomes of the Therapist-assisted Online Parenting Strategies intervention for parents of adolescents treated for anxiety and/or depression: A single-arm double-baseline trial
Supplemental material, sj-docx-1-anp-10.1177_00048674211025695 for Short-term outcomes of the Therapist-assisted Online Parenting Strategies intervention for parents of adolescents treated for anxiety and/or depression: A single-arm double-baseline trial by Sarah Pheik Hoon Khor, Catherine Margaret Fulgoni, Deborah Lewis, Glenn A Melvin, Anthony F Jorm, Katherine Lawrence, Bei Bei and Marie Bee Hui Yap in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to acknowledge the parent and adolescent participants, and the TOPS team who contributed to TOPS-coaching (Alice Gornall, Cassandra McEwen, Natasha Tung and Maddy Fernando), in project management (Mairead Cardamone-Breen), and intervention fidelity assessment (Jordan Bakker) and the research team that enabled the study to be undertaken.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The TOPS intervention was codeveloped by C.M.F., S.P.H.K., A.F.J., G.A.M., K.A.L., B.B. and M.B.H.Y. None of the authors derive any personal financial benefit from the intervention.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: S.P.H.K. and C.M.F. are supported by the Research Training Programme (RTP) Scholarship provided by the Australian Government. A.F.J. is supported by an NHMRC Investigator Grant (APP1172889). B.B. is supported by an NHMRC Health Professional Research Fellowship (APP1140299).
Supplemental Material
Supplemental material for this article is available online.