
Abstract
Objectives:
A diagnostic system that fails to deliver clinically useful information will not be utilized and consequently will be unable to provide valuable data for health policy and clinical decision making. Therefore, it is imperative to obtain an accurate depiction of the clinical utility of the eleventh revision of the International Classification of Diseases (ICD-11) Personality Disorder (PD) model. The current mixed-methods systematic review aimed to determine the clinical utility of the ICD-11 PD classification system.
Method:
An electronic screening of six databases was conducted and resulting studies were subjected to specific exclusion criteria, which elicited eight studies of interest. Study characteristics were tabulated and methodological quality was appraised.
Results:
Four studies offered strong support for the model’s clinical utility, three offered some support accompanied by notable limitations and one study could only offer criticisms.
Conclusion:
Future investigation of the ICD-11 PD classification system’s (a) communicative value between clinicians and their patients, and between clinicians and their patient’s families; (b) ease of use; and (c) feasibility in terms of practical application is required to achieve a complete understanding of its clinical utility and ultimately bring clarity to the current ambiguous findings.
The International Classification of Diseases, 10th Edition (ICD-10; WHO, 1992) and the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5; American Psychiatric Association [APA], 2013) are well known for their inherently problematic, categorical approaches to personality disorder (PD) diagnosis, despite insufficient evidence supporting the notion that PDs are categorical entities (Livesley, 2021; Trull and Durrett, 2005). Due to the significant shortcomings of categorical models such as arbitrary diagnostic thresholds (e.g. Clark et al., 1997), extensive overlap between categories (e.g. Krueger, 2013) and inadequate clinical utility (e.g. Clark, 2007; Tyrer et al., 2015), personality pathology is being increasingly conceptualized as dimensional (Barroilhet et al., 2019; Kim et al., 2014; Mulder et al., 2016).
This transition was first officially acknowledged with the publication of the DSM-5 in May 2013, which proposed a hybrid categorical-dimensional approach to PD diagnosis – the Alternative Model of Personality Disorder (AMPD; APA, 2013). The AMPD was notably endorsed as a research model rather than for clinical application due to its unclear clinical utility (Hopwood et al., 2018; Krueger and Markon, 2014; Pilkonis et al., 2011; Zachar and First, 2015). The World Health Organization (WHO) subsequently released the preliminary version of the 11th Edition of the International Classification of Diseases (ICD-11; WHO, 2021) in June 2018 that consisted of an entirely dimensional PD classification.
The initial proposal that relied on level of PD complexity, psychosocial impairment and harm to self and others (Tyrer et al., 2015) was operationalized by the Standardized Assessment of the Severity of Personality Disorder (SASPD; Olajide et al., 2018). However, this proposal was met with criticism for its lack of assessment of more complex features of self-functioning (Herpertz et al., 2017). Specifically, this initial ICD-11 proposal, inclusive of the SASPD, was not considered to cover specific features of self-functioning such as sense of coherent self, self-directedness and sense of self-worth (Bach and Anderson, 2020; Zimmermann et al., 2020), which comprise essential aspects of the now official ICD-11 PD classification (WHO, 2021). The subsequent revisions of the initial proposal aimed to include a substantially richer and more informative operationalization of PD severity (Huprich et al., 2018; Reed, 2018), leading to the official model being comprised of a severity rating of overall self- and interpersonal functioning and a five-domain dimensional trait model consisting of negative affectivity, detachment, dissociality, disinhibition and anankastia (Tyrer et al., 2019).
The ICD-11 PD classification is consistent with the AMPD by equally integrating aspects of self and interpersonal functioning (Bach and First, 2018; Huprich et al., 2018; Reed, 2018; Tyrer et al., 2019). It essentially differs from the AMPD by its exclusion of the psychoticism domain, which is consistent with the way Schizotypal PD is conceptualized in the ICD-10 (WHO, 1992). Importantly, and in contrast to the AMPD which was presented with its own measures, the ICD-11 classification was not presented with a measure that provides a formal operationalization of the classification system. Thus, researchers have endeavoured to establish new measures (e.g. Kim et al., 2020; Oltmanns and Widiger, 2018) or employ algorithms for existing measures (e.g. Bach et al., 2020; Bach and First, 2018; Gamache et al., 2021; McCabe and Widiger, 2020).
Clinical utility
The construction of a diagnostic system must include the consideration of whether (a) patients who meet the diagnostic criteria present with its hypothesized correlates and (b) the diagnostic criteria are useful for clinical practice (Kendell and Jablensky, 2003). There is a plethora of research emphasizing the importance of such constructs; validity (e.g. Borsboom et al., 2004; Strauss and Smith, 2009) and clinical utility (e.g. Mullins-Sweatt et al., 2016), though evidently the two concepts do not exclusively occur simultaneously and there is significant empirical ambiguity regarding their conceptual boundaries (Kendell and Jablensky, 2003; Spitzer, 2001). WHO specifically defined the clinical utility of a model as dependent on: (a) its value in communicating among practitioners, patients, families, administrators; (b) its implementation characteristics in clinical practice, including its goodness of fit [i.e. diagnostic accuracy], its ease of use and the time required to use it; and (c) its usefulness in selecting interventions and in making clinical management decisions. (Reed, 2010: 461)
In accordance with previous reviews, we maintain a firm distinction between construct validity and clinical utility while concurrently acknowledging the inevitable overlap when investigating outcomes pertaining to the latter (First et al., 2004; Milinkovic and Tiliopoulos, 2020).
Operationalizations of the ICD-11 PD classification system have robust construct validity (Bagby and Widiger, 2020; Crego and Widiger, 2019; Oltmanns and Widiger, 2018, 2019), have high convergences with criterion measures (Bach et al., 2018; McCabe and Widiger, 2020; Oltmanns and Widiger, 2020) and show reliability cross-culturally (Bach and El Abiddine, 2020; Bach et al., 2020; Gutierrez et al., 2020; Kim et al., 2020; Somma et al., 2020). While construct validity is an essential requirement for the endorsement of a classification system, it is not sufficient (Hopwood et al., 2018). A diagnostic model must also be clinically useful in aiding the identification of individuals requiring mental health services while simultaneously indicating treatments that are most likely to be efficacious (Bach and Simonsen, 2020; Evans et al., 2013; Reed et al., 2011).
The current review
There have been a number of empirical reviews in the field of PD diagnosis. While researchers have systematically reviewed the validity (e.g. Sharp and Wall, 2021; Watters, Bagby and Sellbom, 2019) and clinical utility (e.g. Bornstein and Natoli, 2019; Milinkovic and Tiliopoulos, 2020) of the AMPD and have provided relevant, influential literary reviews (e.g. Mullins-Sweat and Lengel, 2012; Widiger, 2019), there has been no attempt to systematically determine the clinical utility of the ICD-11 PD Classification System. The ICD-11 will become the authoritative classification system for the 194 member states of WHO. Not surprisingly, given that the ICD-11 has yet to be officially released, it has received considerably less empirical attention than the AMPD (McCabe and Widiger, 2020). The current review aims to determine the clinical utility of the ICD-11 prior to its official availability in January 2022. Synthesizing the literature, to date, is essential to making recommendations for future research to avoid the literature developing in a piecemeal manner.
Method
Protocol and registration
The current review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2015). The protocol strictly adhered to the Cochrane Handbook for systematic reviews (Higgins and Green, 2011) and was registered prospectively with PROSPERO (CRD42020190523).
Search strategy
A comprehensive electronic screening of PsycINFO, Medline, Scopus, Web of Science, Science Direct and PubMed was conducted on 5 June 2020. The key search terms (see Table 1) were applied in a multi-field format to screen the relevant databases. The reference lists of included studies were searched manually for additional studies of relevance, which may not have resulted from the initial database screening.
Key words and search terms used in electronic database screening.
ICD: International Classification of Diseases.
Study selection
The resulting output was imported into Cochrane’s recommended online systematic reviewing platform – Covidence (Higgins and Green, 2011). Duplicate studies were eliminated from the initial pool of studies. The titles and abstracts were screened by the first and another author and removed if they were inconsistent with the inclusion criteria. The eligibility of the remaining manuscripts was evaluated in alignment with the full exclusion criteria by both authors. Any disagreement between the reviewers over the eligibility of specific studies was resolved through discussion and consensus. If a disagreement could not be resolved, a third expert reviewer was engaged.
Inclusion criteria
Peer-reviewed journal articles and postgraduate dissertations were included in the current review if published in the English language, between 18 June 2018 – the release date of the Eleventh Edition of the International Classification of Diseases (ICD-11; WHO, 2018) – and 5 June 2020.
Exclusion criteria
Design
Longitudinal studies that commenced prior to the inclusion time frame or studies that utilized earlier versions of the ICD-11 that distinctly differed from the current version (e.g. Sanatinia et al., 2016; Tyrer et al., 2014) were excluded. Studies that exclusively utilized approaches to personality disorder diagnosis other than the ICD-11 and/or its dimensional operationalizations were excluded from the current review (e.g. Leichsenring et al., 2019; Samuel et al., 2018). While conceptual, theoretical and critical literary contributions were used in the formation of the introduction, this non-empirical research was also excluded (e.g. Bach and Bernstein, 2018; Bagby and Widiger, 2020; Ekselius, 2018; Hopwood et al., 2018; Tyrer et al., 2019).
Population
Studies that solely incorporated non-clinical populations, such as community-dwelling participants (Bach et al., 2020; Somma et al., 2020) or general medical admission (Barroilhet et al., 2020), or participants under the age of 18 (Polek et al., 2018) were excluded. Specifically, clinical participants were inclusive of individuals with current or previous mental health problems and/or mental health professionals. Clinical research simultaneously investigating participants experiencing psychosis or psychotic disorders were deemed ineligible.
Outcome
Eligible studies investigated some form of ICD-11 operationalization – or another dimensional assessment of personality pathology consistent with this approach – in relation to one or more of the three clinical utility outcomes: communicative value (CV), implementation characteristics (IC) or usefulness (U) in selecting interventions and in making clinical management decisions. Research that investigated outcomes that were inconsistent with this focus, such as measure validation, were excluded (e.g. Brazil et al., 2018; Gutiérrez et al., 2020; Kotelnikova et al., 2019; Oltmanns and Widiger, 2018, 2019, 2020; Sellbom et al., 2020). Effects were systematically allocated by the authors, with any author disagreement regarding the relevance of study outcome/s being resolved through rigorous discussion. In the event that consensus could not be achieved, a third expert reviewer was consulted.
Data extraction
The extraction and recording of key data was conducted via the application of a standardized extraction form designed specifically for this style of review by the first author. The extracted information consisted of the country in which the research was conducted, study design, setting and population, outcome/s assessed, measures used, statistical analyses and results, and key findings. The final summation of data was reviewed by a second author, with any disagreements reaching resolution via collaborative discussion or consultation with a third author. Study characteristics and clinical utility outcomes investigated are depicted in Table 2 and Figure 1, respectively.
Characteristics of included studies.
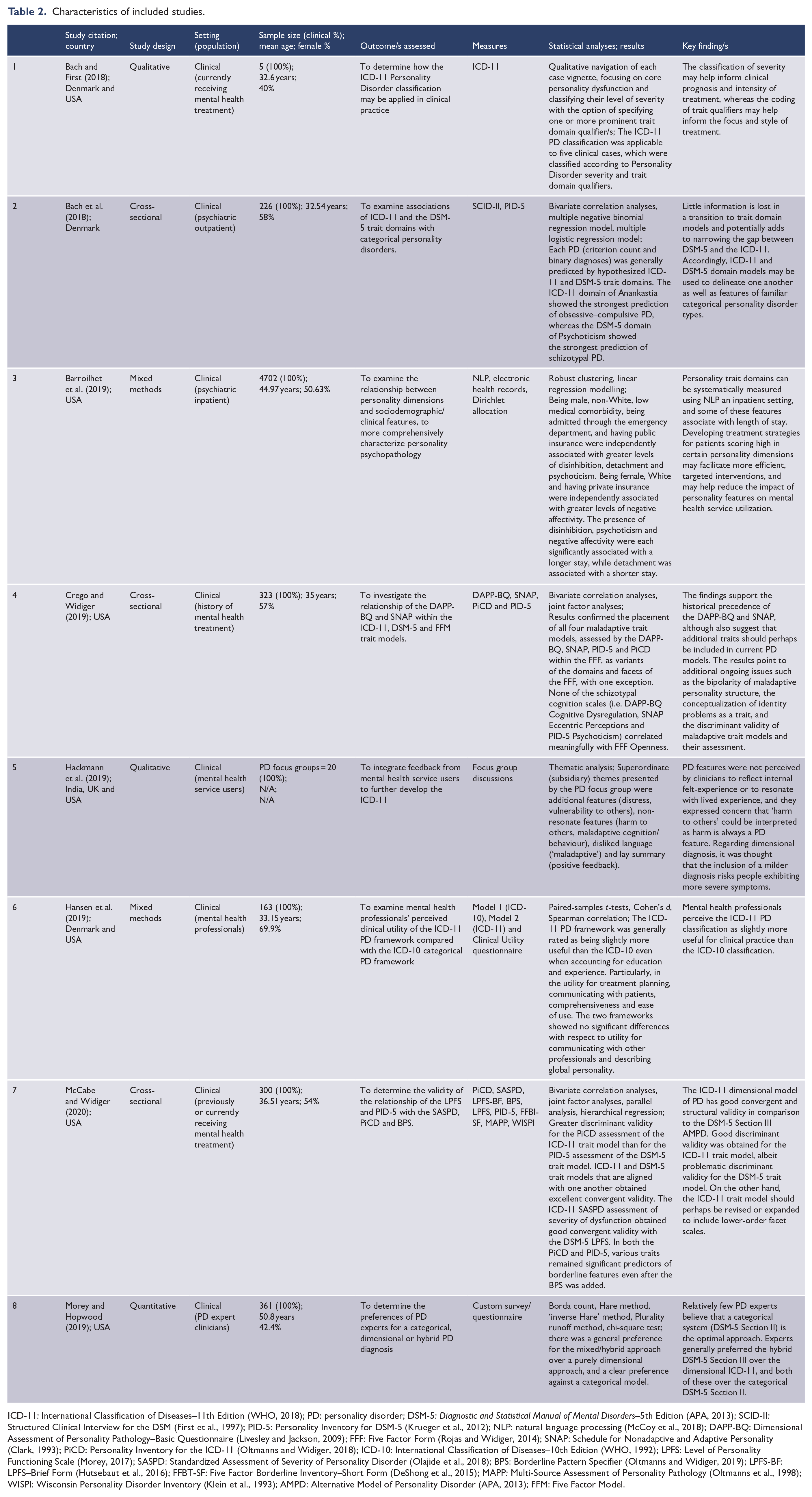
ICD-11: International Classification of Diseases–11th Edition (WHO, 2018); PD: personality disorder; DSM-5: Diagnostic and Statistical Manual of Mental Disorders–5th Edition (APA, 2013); SCID-II: Structured Clinical Interview for the DSM (First et al., 1997); PID-5: Personality Inventory for DSM-5 (Krueger et al., 2012); NLP: natural language processing (McCoy et al., 2018); DAPP-BQ: Dimensional Assessment of Personality Pathology–Basic Questionnaire (Livesley and Jackson, 2009); FFF: Five Factor Form (Rojas and Widiger, 2014); SNAP: Schedule for Nonadaptive and Adaptive Personality (Clark, 1993); PiCD: Personality Inventory for the ICD-11 (Oltmanns and Widiger, 2018); ICD-10: International Classification of Diseases–10th Edition (WHO, 1992); LPFS: Level of Personality Functioning Scale (Morey, 2017); SASPD: Standardized Assessment of Severity of Personality Disorder (Olajide et al., 2018); BPS: Borderline Pattern Specifier (Oltmanns and Widiger, 2019); LPFS-BF: LPFS–Brief Form (Hutsebaut et al., 2016); FFBT-SF: Five Factor Borderline Inventory–Short Form (DeShong et al., 2015); MAPP: Multi-Source Assessment of Personality Pathology (Oltmanns et al., 1998); WISPI: Wisconsin Personality Disorder Inventory (Klein et al., 1993); AMPD: Alternative Model of Personality Disorder (APA, 2013); FFM: Five Factor Model.
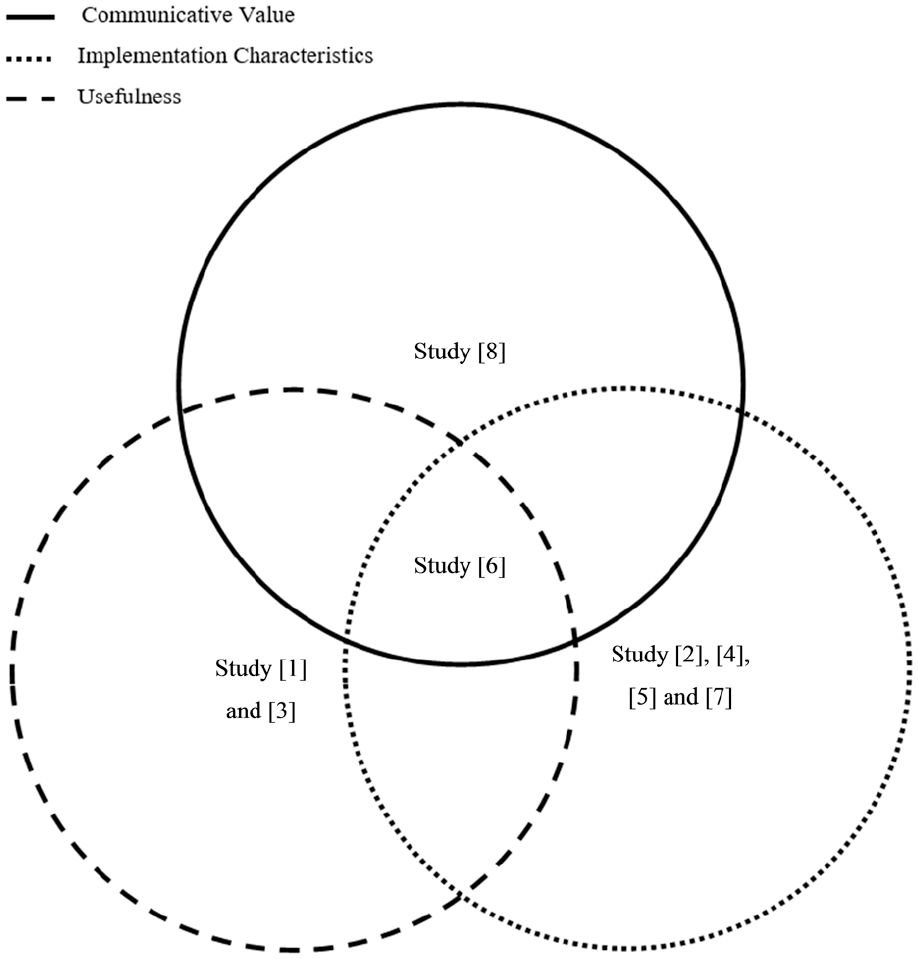
Venn diagram of included studies and investigated clinical utility outcomes.
Assessment of methodological quality
Crowe and Sheppard’s (2011) review of critical appraisal tools found the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018) to be the only tool that effectively addresses the quality of mixed-methods studies. In light of significant disparities in design and target outcome/s across included studies, the MMAT was deemed the most appropriate tool to assess their methodological quality. Each study was allocated to the appropriate study design category for appraisal. The answer to each of the five questions pertaining to that study’s design was categorized as ‘yes’ (Y), ‘no’ (N) or ‘cannot tell’ (CT). Given that the authors of the MMAT discourage the calculation of an overall score and encourage a contrast of results (Hong et al., 2018), a sensitivity analysis is visually depicted in Table 3. The first author conducted the initial assessment, which was then discussed in detail with a second author. Disagreements were resolved via collaborative discussion.
Assessment of methodological quality for included studies via the MMAT criteria.
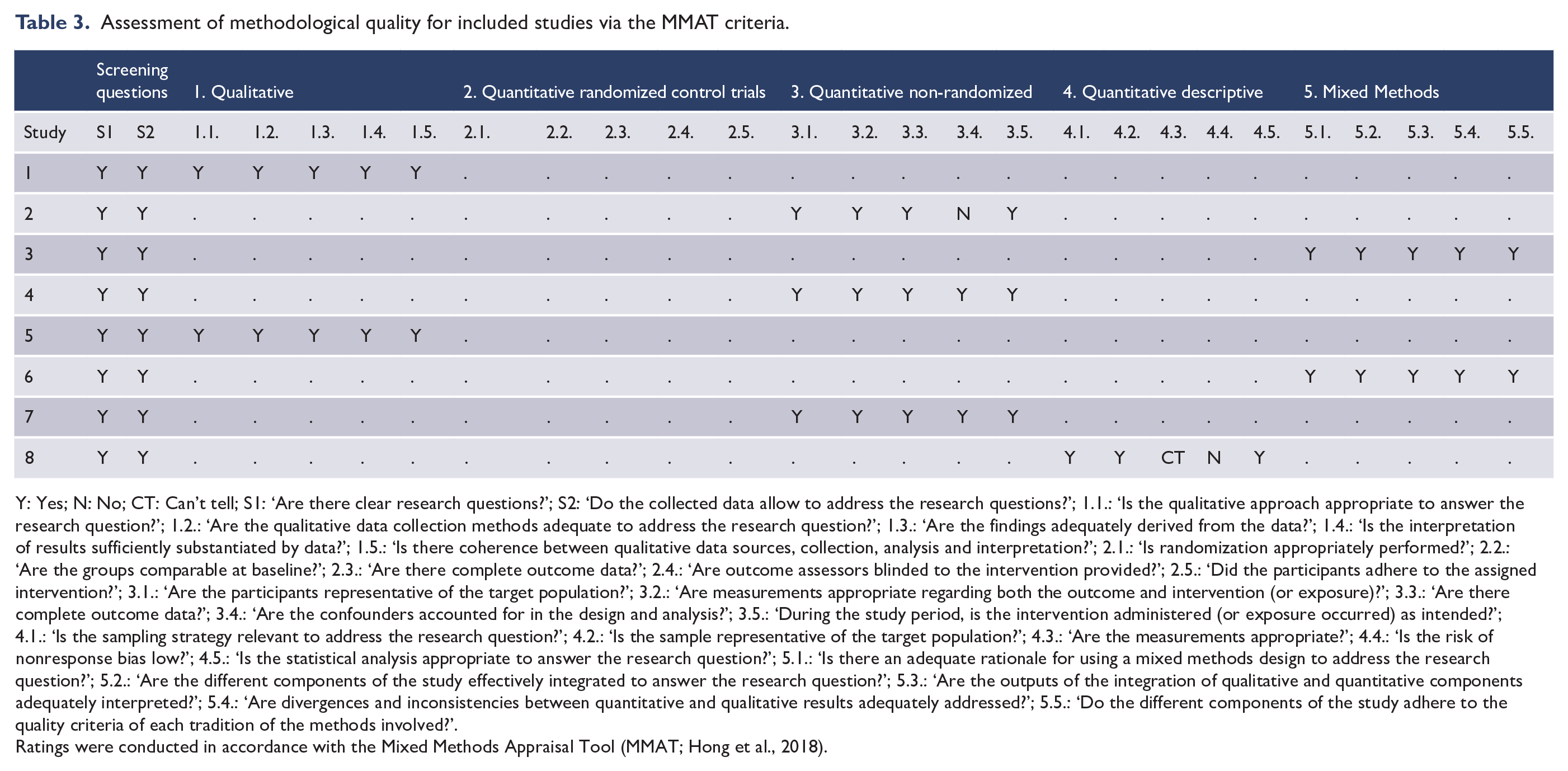
Y: Yes; N: No; CT: Can’t tell; S1: ‘Are there clear research questions?’; S2: ‘Do the collected data allow to address the research questions?’; 1.1.: ‘Is the qualitative approach appropriate to answer the research question?’; 1.2.: ‘Are the qualitative data collection methods adequate to address the research question?’; 1.3.: ‘Are the findings adequately derived from the data?’; 1.4.: ‘Is the interpretation of results sufficiently substantiated by data?’; 1.5.: ‘Is there coherence between qualitative data sources, collection, analysis and interpretation?’; 2.1.: ‘Is randomization appropriately performed?’; 2.2.: ‘Are the groups comparable at baseline?’; 2.3.: ‘Are there complete outcome data?’; 2.4.: ‘Are outcome assessors blinded to the intervention provided?’; 2.5.: ‘Did the participants adhere to the assigned intervention?’; 3.1.: ‘Are the participants representative of the target population?’; 3.2.: ‘Are measurements appropriate regarding both the outcome and intervention (or exposure)?’; 3.3.: ‘Are there complete outcome data?’; 3.4.: ‘Are the confounders accounted for in the design and analysis?’; 3.5.: ‘During the study period, is the intervention administered (or exposure occurred) as intended?’; 4.1.: ‘Is the sampling strategy relevant to address the research question?’; 4.2.: ‘Is the sample representative of the target population?’; 4.3.: ‘Are the measurements appropriate?’; 4.4.: ‘Is the risk of nonresponse bias low?’; 4.5.: ‘Is the statistical analysis appropriate to answer the research question?’; 5.1.: ‘Is there an adequate rationale for using a mixed methods design to address the research question?’; 5.2.: ‘Are the different components of the study effectively integrated to answer the research question?’; 5.3.: ‘Are the outputs of the integration of qualitative and quantitative components adequately interpreted?’; 5.4.: ‘Are divergences and inconsistencies between quantitative and qualitative results adequately addressed?’; 5.5.: ‘Do the different components of the study adhere to the quality criteria of each tradition of the methods involved?’.
Ratings were conducted in accordance with the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018).
Evidence synthesis
A convergent, narrative synthesis of results was appraised by the authors as the most appropriate approach due to extensive design disparity and differences in target outcomes across the included studies.
Results
The initial search produced 662 publications of interest (refer to sFigure 2). After removing 99 duplicates, a further 521 were removed on the basis of incompatible title and abstract, and the full text of the remaining 43 articles was comprehensively assessed for their eligibility. After completing the full-manuscript screening, eight studies met the current inclusion criteria.
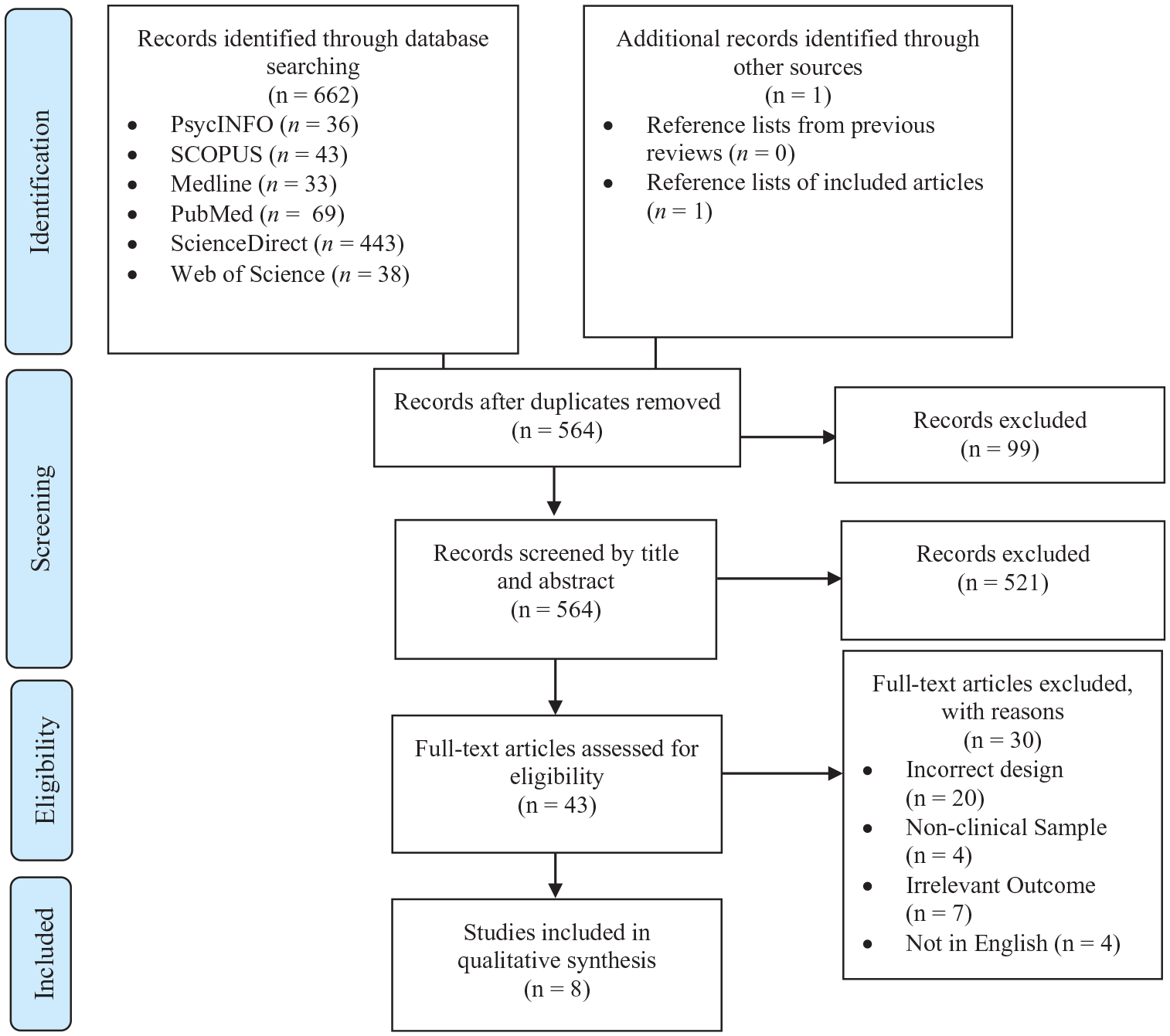
Study selection process via PRISMA flow chart.
Study characteristics
Of the eight included studies, three studies were conducted in multiple countries, with one study being conducted between India, the United Kingdom and the United States (Hackmann et al., 2019), and two between Denmark and the United States (Bach and First, 2018; Hansen et al., 2019). Of the remainder, one study was conducted in Denmark (Bach et al., 2018) and the remaining four in the United States. Three of the included studies were cross-sectional in design, two were qualitative, one was quantitative and two had mixed-methods designs. The accumulated population consisted of 5637 clinical participants and 463 clinicians. Participant mean age identified in seven of the eight studies ranged from 32.54 to 50.8 years (M = 37.94, SD = 7.14). Female participants made up 53.13% of the population. One study (Hackmann et al., 2019) did not provide age or gender statistics.
Methodological quality
Examination of the MMAT application revealed that seven of the eight included studies were of low risk on all items. However, some risk of bias was indicated for study (Morey and Hopwood, 2019). It was unclear whether simply ranking three diagnostic models was a valid or accurate measurement of expert preferences in regard to clinical utility, and the degree to which these ‘expects’ were currently – or have been previously – engaged in clinical work. Second, the study’s non-response bias (Federal Committee on Statistical Methodology, 2001) was deemed high due to its 39.1% response rate. Nevertheless, the overall quality of the included studies is methodologically sound and we can therefore have confidence in the findings from the body of evidence.
Clinical utility outcomes
This mixed-methods review aimed to determine the clinical utility of the ICD-11’s PD classification system within a clinical population. To reiterate, the clinical utility of a diagnostic model can be established by systematically examining research investigating the model’s communicative value across practitioners, patients and families; the model’s implementation characteristics inclusive of diagnostic accuracy, ease of use and timeliness of application; and the model’s use in aiding clinical decision making and facilitating intervention selection (Mullins-Sweatt et al., 2016; Reed, 2010).
Two of the eight studies focused on the ICD-11’s communicative value, evidencing moderate and strong support, respectively (Hansen et al., 2019; Morey and Hopwood, 2019). Of the five studies investigating the model’s implantation characteristics, two evidenced some support (Crego and Widiger, 2019; McCabe and Widiger, 2020) for the model’s diagnostic accuracy, two robustly supported the model’s implementation in general (Bach et al., 2018; Hansen et al., 2019) and one (Hackmann et al., 2019) could only offer limitations. Finally, the three studies investigating outcomes pertaining to the ICD-11’s usefulness were unanimously supportive.
Communicative value
Two of the eight studies investigated the ICD-11’s communicative value, specifically focusing on mental health practitioners, finding moderate support for the model via expert preferences (Morey and Hopwood, 2019) and strong support via clinician perceptions (Hansen et al., 2019). While study (Morey and Hopwood, 2019) found that experts generally preferred dimensional approaches over a categorical system, the AMPD was preferential over the ICD-11. An additional comparison of dimensional models revealed that clinicians perceive the ICD-11 PD classification as significantly more useful for clinical practice than the ICD-10 classification (Hansen et al., 2019), though the effect size was small.
Of the two studies investigating communicative value, one study offered strong support while the other could only offer moderate support. Notably, these findings were only specific to communicative value among practitioners and highlight a need for further research, both to clarify of these mixed findings and to address the absence of research investigating the ICD-11’s value in communicating between clinicians and their patients, and their patients’ families.
Implementation characteristics
Five of the eight studies investigated outcomes pertaining to the ICD-11’s implementation characteristics. Of these five, three studies examined associations between various diagnostic models and evidenced moderate (Crego and Widiger, 2019; McCabe and Widiger, 2020) to strong (Bach et al., 2018) support for the model’s goodness of fit. Of the remaining two studies, one showed very limited support for diagnostic accuracy via clinician feedback (Hackmann et al., 2019) and one showed strong support for both diagnostic accuracy and ease of use via clinician perceptions (Hansen et al., 2019). Hackmann et al. (2019) elicited feedback from mental service users to further develop the ICD-11, which highlighted that clinicians did not perceive PD features to be reflective of internal felt-experience or to resonate with lived experience. They expressed concerns around, ‘harm to others’ being interpreted as synonymous with PD features and thought that the inclusion of a milder diagnosis risks individuals presenting with more severe symptomatology. Notably, their aim was to obtain recommendations from mental health professionals, which may explain the critical nature of the responses. Hansen et al. (2019), however, found that clinicians perceived the ICD-11 PD framework as comprehensive, useful for describing global personality and easy to use, regardless of education and experience, and when compared to the ICD-10.
The findings from the five studies investigating the ICD-11’s implementation characteristics were mixed, with support ranging from limited to strong. In addition, there was a significant empirical deficit in investigations of the model’s ease of use and a stark absence of research on its feasibility in terms of timeliness for practical application.
Usefulness
Three of the eight included studies investigated the ICD-11 PD Classification’s utility in clinical decision making and intervention selection. Bach and First (2018) qualitatively navigated five clinical cases and demonstrated how classification of severity may inform clinical prognosis and treatment intensity, and how the coding of trait qualifiers may be helpful in informing the focus and style of intervention. Study 3 (Barroilhet et al., 2019) systematically measured trait domains and their relationship with sociodemographic/clinical features to more comprehensively characterize personality psychopathology, as a means of facilitating more efficient, individualized interventions, and reducing the impact of personality features on mental health service utilization. Finally, Hansen et al. (2019) exhibited support for the ICD-11’s usefulness via clinician perceptions, finding that clinicians perceive the ICD-11 PD Classification more useful for clinical practice than the ICD-10 and particularly in the utility for treatment planning, even when accounting for clinician education and experience.
The three studies that investigated outcomes pertaining to the ICD-11’s usefulness in treatment selection and clinical decision making were all robustly supportive of the model. While research was scarce, studies did capture all aspects of the model’s clinical usefulness.
Discussion
This mixed-methods review is the first to attempt to investigate the clinical utility of the ICD-11 PD Classification within a clinical population. While findings were mixed across the eight available studies, the two studies that investigated communicative value between clinicians were supportive of the model and particularly in comparison to previous categorical approaches, though no research investigated this effect between clinicians and patients or between their patients’ families. Similarly, studies on clinical usefulness were broadly supportive. Results were less clear for implementation characteristics, where support ranged across studies from limited to strong support. Overall, these results are not entirely consistent with the AMPD’s high clinical utility (Milinkovic and Tiliopoulos, 2020) and with findings of the ICD-11’s high validity (e.g. Bagby and Widiger, 2020; Oltmanns and Widiger, 2018, 2019) in previous reviews.
This inconsistency may be interpreted in a number of ways. First, WHO member states were introduced to the ICD-11 with a dimensional model that drastically differed from the ICD-10. As the AMPD was introduced as a hybrid model, clinicians may have been more comfortable with a model that was perceived as ‘transitional’. Similarly, the fact that the ICD-11 was in practice immediately – in contrast to the AMPD’s inclusion as a research model only – may have made clinicians more open to considering benefits, such that their opinions can influence change, rather than being expected to implement an already-adopted model they are unfamiliar with. As clinicians become more familiar with the ICD-11, future assessments of the model’s clinical utility may differ (e.g. Garcia et al., 2018).
In this vein and as aforementioned, the ICD-11 is the authoritative nomenclature of 194 culturally diverse WHO member states. While the American DSM-5 Section III AMPD is considered to be compatible with the ICD-11 (McCabe and Widiger, 2020), it is possible that when applied cross-culturally such a dimensional model and/or its application is problematic. This makes sense given (a) variance in culturally diverse PD populations (McGilloway et al., 2010; Selby and Joiner, 2008); (b) the fact that despite fewer studies, there was noticeably more cultural diversity in the current review when compared to Milinkovic and Tiliopoulos’ (2020) review of the AMPD; and (c) that in contrast to the ICD, the DSM is largely applied in Western societies exclusively. Finally, while the current results do not show unambiguous support for the ICD-11 PD classification, it should be noted that there is, as yet, very scarce research. Indeed, the current body of evidence is less than half the size of that presented in Milinkovic and Tiliopoulos’ (2020) review. It is perhaps premature to establish a clear picture of the ICD-11’s clinical utility and more research in the previously named areas, identified through the current review, is crucial in achieving clarity.
Promisingly, females and males were equally represented in the current body of evidence. Half of the included studies were conducted cross-culturally, and the majority were adequately powered with reasonable sample sizes. However, a few limitations were evident. First, the relatively low mean age is problematic for generalizability to older adults, who have PD prevalence estimates ranging from 3% to 13% in the general population (van Alphen et al., 2012, 2015). Two of the eight studies were qualitative case studies; a methodology well known for researcher and selection biases (George and Bennett, 2005; Sprock, 2003). Third, the aims and methodologies of the included studies were extremely diverse ranging from ICD-11 application to case vignettes (Bach and First, 2018), to predicting sociodemographic and clinical outcomes (Barroilhet et al., 2019), to examining clinician perceptions and expert preferences (Hackmann et al., 2019; Hansen et al., 2019; Morey and Hopwood, 2019). This diversity added complexity to the synthesis and interpretation of the cumulative evidence. Finally, clinicians were starkly underrepresented when compared to clinical participants, though this makes sense given that the ICD-11 is not yet formally in use. As the ICD-11 is a diagnostic tool used by clinicians, it is of utmost importance to gather more information regarding their preferences, experiences and recommendations to gage user acceptability after the ICD-11’s formal adoption (Samuel and Widiger, 2010).
Several additional recommendations can be derived from the current body of evidence. First, gaping deficits in empirical research examining the communicative value of the ICD-11 between clinicians and their patients, and their patients’ families, and the model’s implementation characteristics – specifically, its ease of use and its feasibility in terms of time taken for application – denote clear future research directions. Second, future research needs to focus not only on clinician perceptions and experiences but also how they use the ICD-11 PD classification system (First et al., 2018). Even the most valid and clinically useful model would be deemed a failure if it is never or rarely utilized, or utilized incorrectly (First et al., 2004). Potential avenues include how often and under what circumstances clinicians apply the diagnostic guidelines (First et al., 2014; Garb, 2005), how often they consult the physical text and what percentage of clinicians utilize the ICD-11 in exclusivity (First et al., 2014; Mullins-Sweatt et al., 2016).
Any new classification system must be critically and comprehensively analysed. As the watchwords of the ICD-11 are clinical utility (Tyrer et al., 2019), it is imperative for researchers and clinicians alike to have an accurate portrayal of the ICD-11 PD nomenclature’s clinical utility. The current review supports the ICD-11’s clinical utility. Specifically, four studies offered robust support for the model’s clinical utility, three offered moderate support in addition to notable limitations and one study could only offer recommendations. Future investigation of the ICD-11 PD classification system’s (a) communicative value between clinicians and their patients, and between clinicians and their patient’s families; (b) ease of use; and (c) feasibility in terms of practical application is required to bring clarity to the ICD-11 PD classification’s blurred picture of clinical utility. A diagnostic model should serve the function of a decision tool for its practitioners and have significant utility in clinical management and treatment planning (Bach, 2018, 2020; Bach and Presnall-Shvorin, 2020; Bach and Simonsen, 2020; Huprich, 2020). In essence, while still requiring further research, the WHO’s shift to dimensionality can be considered as a step in the right direction in adhering to their primary aim; of first and foremost providing a useful diagnostic scheme for clinicians worldwide that ultimately aids the reduction of suffering among individuals with mental disorders (First et al., 2004; Hansen et al., 2019; Keeley et al., 2016).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.