
Abstract

To the Editor
The recently published Royal Australian and New Zealand College of Psychiatrists (RANZCP) mood disorders clinical practice guidelines (MDcpg2020) provide an excellent contemporary overview of the aetiology, classification and (suggestive, but non-prescriptive) management of mood disorders (Malhi et al., 2021). Recommendations are evidence-based or, where the evidence is insufficient, consensus-based – here the knowledge and experience of the authors come to the fore. Although some have criticized the document for being more textbook than guideline (e.g. there are 61 pages of information prior to any specific mood disorder management recommendation), overall the authors ought to be commended for a comprehensive publication.
RANZCP clinical practice guidelines (CPGs) continue to be published as stand-alone, pdf documents. This is problematic for three key reasons:
They take years to develop, during which time new evidence continuously arises, rendering the final document inexorably outdated the day it is published.
They cover umbrella areas (e.g. ‘mood disorders’) and so are unable to adjust for specific areas (e.g. adult with bipolar depression) if practice-changing information emerges.
They require the clinician to scroll through potentially reams of text in order to find the particular piece of information/recommendation they seek.
The RANZCP CPGs should evolve to an online, modular, ‘live’ tool akin to the National Institute for Health and Care Excellence (NICE, 2021) ‘Pathways’. Each NICE umbrella area has its own interactive flowchart that allows the busy clinician to rapidly seek out the information or recommendation they require (see Figure 1). With a click, each arm streams into specific areas that provide recommendations particular to the clinical issue at hand (e.g. adult with bipolar depression).
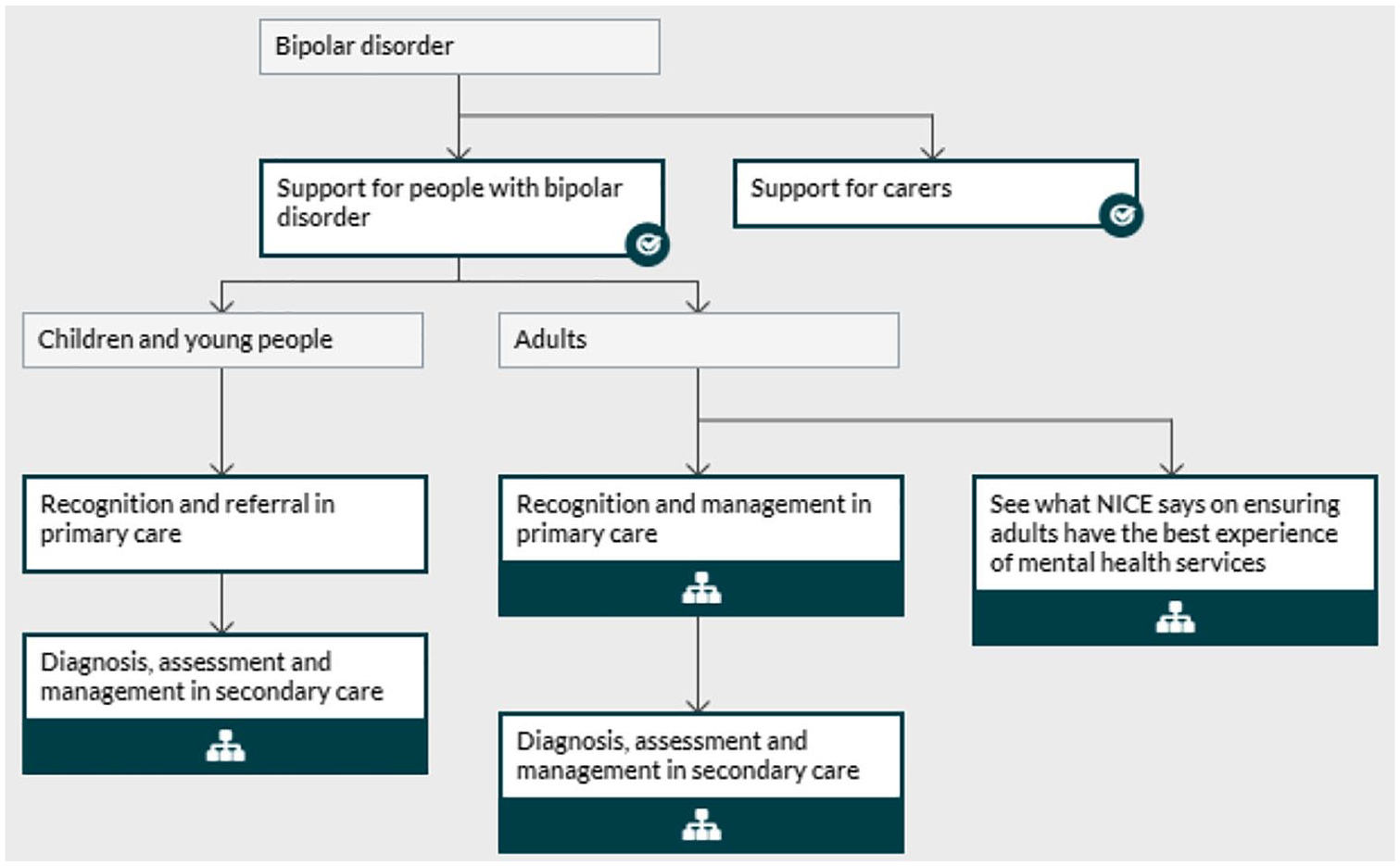
NICE interactive flowchart – bipolar disorder (NICE, 2021).
An RANZCP version could include recommendations accompanied by separate expandable sub-sections for ‘rationale’ (e.g. the useful background theories and models provided in the MDcpg2020) and ‘supporting evidence’ that could be viewed if and when desired. In terms of recommendations themselves, each specific area could easily adapt those of the current RANZCP CPGs (e.g. the ‘Actions, Choices, Alternatives’ model proposed in the MDcpg2020) (see Figure 2).
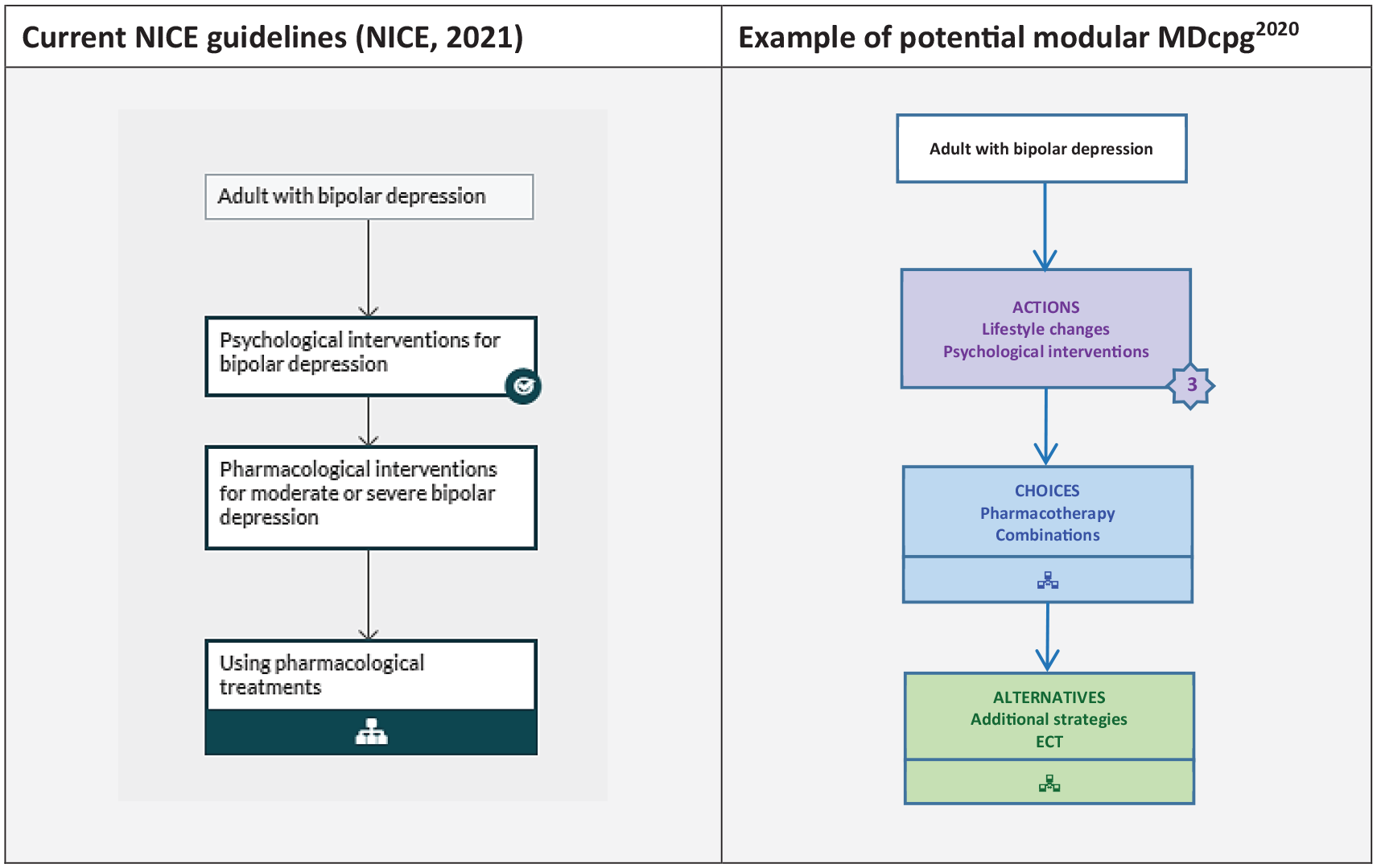
Specific area recommendations – for example, ‘adult with bipolar depression’.
A live, modular, MDcpg2020 could be continuously updated and adjusted as new evidence (or consensus) arises. In the absence of a governing national body (such as NICE), the authors of each specific area could be stated (as they are in UpToDate) and the date of the last revision listed. The option of attaching other resources (e.g. cultural) and/or information for patients would exist. Finally, each umbrella and/or specific area could easily be converted into a pdf and printed for those who prefer it the old way … at least then it’d always be (relatively) up to date!
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.