
Abstract
Objective:
While there is considerable current emphasis on youth and early psychosis, relatively little is known about the lives of people who live with psychotic disorders into middle age and beyond. We investigated social functioning, physical health status, substance use and psychiatric symptom profile in people with psychotic disorders aged between 50 and 65 years.
Methods:
Data were collected as part of the Survey of High Impact Psychosis, a population-based survey of Australians aged 18–65 years with a psychotic disorder. We compared those aged 50–65 years (N = 347) with those aged 18–49 years (N = 1478) across a range of measures.
Results:
The older group contained more women and more people with affective psychoses compared to the younger group. They were also more likely to have had a later onset and a chronic course of illness. The older group were more likely to have negative symptoms but less likely to exhibit positive symptoms; they also had lower current cognition, compared to the younger group. Compared to the younger group, the older group were more likely to be divorced/separated, to be living alone and to be unemployed. They had substantially lower lifetime use of alcohol and illicit substances, but rates of obesity, metabolic syndrome and diabetes mellitus were higher.
Conclusion:
Our findings suggest that the characteristics of people with psychosis change significantly as they progress into the middle age and beyond. A better understanding of these differences is important in informing targeted treatment strategies for older people living with psychosis.
Introduction
Evidence describing the life circumstances and physical and psychological well-being of older people with psychotic disorders is limited (Galletly et al., 2016). Most research relating to older patients with psychosis has focused on people with late-onset disorders (Castle and Murray, 1993; Cohen et al., 2020; Vahia et al., 2010). While early intervention and youth-based psychosis paradigms are important, people who do not achieve full recovery and grow old with a psychotic disorder also deserve attention. The few studies describing this group suggest that many older people with psychotic disorders remain symptomatic and impaired (Auslander and Jeste, 2004; Jeste et al., 2003). Older people living with a mental illness are affected by stigma and systemic ageism (Wells et al., 2020). Service providers may tolerate symptoms, side effects and physical and social disadvantage as inevitable for this population, providing a passive approach to management (Jolley et al., 2004). Older people with long-standing mental illness have been found to be at high risk of homelessness, inappropriate treatments, poor medical and end-of-life care, or missing out on service provision altogether (McCleery et al., 2008; McGrath and Holewa, 2004).
People with psychotic disorders have higher rates of medical morbidity and early mortality compared to the general population, leading to the estimated loss of around 15 years of potential life (Hjorthoj et al., 2017). Using the Australian Survey of High Impact Psychosis (SHIP) data, Saha et al. (2014) found the standardised mortality rate of people with psychotic disorders to be 5.5, indicating that overall mortality in people with psychotic disorders was more than five times that of the general population. One perspective on this premature mortality is to conceptualise schizophrenia as a disorder of premature ageing (Kirkpatrick and Kennedy, 2018), with factors such as epigenetic changes, inflammation and metabolic changes causing cell ageing and death. To support this, studies of people who are in earlier stages of schizophrenia have shown shortened telomeres, an index of cellular ageing (Galletly et al., 2017). Given this premature biological ageing, it is likely that the social and physical challenges associated with ageing occur earlier in people with psychotic disorders, compared to the general population. The older psychosis cohort are therefore those who have survived – delineating differences from people earlier in their illness course may give some indication of factors associated with such individuals living into middle age and beyond. Furthermore, a detailed exposition of the challenges and complexities associated with this older patient cohort is critical in informing best-practice care provision, especially given that the number of people with schizophrenia aged over 60 years is forecast to double by 2050 (Cohen et al., 2020).
The findings of the SHIP provided a rare opportunity to explore the profile of Australians with a psychotic disorder using a large, representative national prevalence sample. This paper investigates social functioning, physical health status, psychiatric symptom profile and substance use in older Australians living with a psychotic disorder (aged 50–65 years) compared to younger participants (aged between 18 and 49 years). Based on the existing literature, it was anticipated that the older participants would have more severe symptoms, psychosocial impairment and physical health complications compared to the younger cohort.
Methods
The 2010 SHIP was conducted within seven catchment sites across five Australian states, covering a population of some 1.5 million people aged 18–64 years, approximately 10% of the Australian population in this age range (Morgan et al., 2012). The survey used a two-phase design. In Phase 1, screening for psychosis took place in public specialised inpatient and community mental health services and in non-government organisations supporting people with mental illness in the census month (March 2010). A psychosis screener was used to identify individuals likely to meet criteria for formal diagnosis (Jablensky et al., 2000; Morgan et al., 2012). A total of 7955 people screened positive for psychosis and met eligibility criteria. In Phase 2, 1825 people who were screened positive were randomly selected, stratified by catchment site and age group (18–34 years and 35–64 years), and interviewed. The research protocol for the study was approved by all relevant institutional ethics committees at each catchment site and all participants gave written informed consent.
Assessments
The interview consisted of 32 modules including demographic characteristics, social participation and functioning, physical health and activity, and psychopathology. In addition, each participant had a physical health assessment, and the majority (1286) provided a fasting blood sample. The interview was administered by trained interviewers who were mental health professionals.
Diagnostic classification
Diagnostic assessment was based on a semi-structured clinical research interview, the Diagnostic Interview for Psychosis–Diagnostic Module (DIP-DM) (Castle et al., 2006). The DIP uses prompts adapted from the Schedules for Clinical Assessment in Neuropsychiatry (SCAN) (World Health Organization, Division of Mental Health, 1994) to elicit signs and symptoms, then applies the Operational Criteria Checklist for Psychosis (OPCRIT) (McGuffin et al., 1991) algorithm embedded into a software package to generate diagnoses according to several classification systems including the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR).
Demographic variables
For demographic variables examined, the age of onset of psychosis was determined by participant’s response to the following questions: ‘When did you first experience mental health problems?’, ‘When did you feel something was not right?’ and ‘When did others first say that they thought you had a psychiatric problem?’ Course of illness was assessed and rated by the interviewers capturing the number of episodes of mental illness that a person experiences and the degree of recovery after each episode (Castle et al., 2006). The course was dichotomised into non-chronic (single episode with good recovery or multiple episodes with good or partial recover between) or chronic (continuous chronic illness with or without deterioration). The type of psychotic disorder was determined according to DIP-DM (Castle et al., 2006). The diagnoses were then divided into non-affective (schizophrenia, delusional disorder and other non-organic psychosis) or affective psychosis (schizoaffective disorder, bipolar disorder and depression with psychosis), derived using the DSM-IV-TR.
Social and functional variables
We examined 10 variables relating to social and functional capacities. Country of birth was based on the question ‘What country were you born in?’ and responses were dichotomised into either born in Australia or not born in Australia. Marital status was divided into (1) married or de facto; (2) separated, divorced or widowed; and (3) single, never married. Living arrangements were divided into either living alone or living with others. Homelessness over the previous 12 months was self-reported. Employment status was determined according to whether or not the participant was in any employment in the 12 months prior to the interview. Number of friends and the contact frequency with friends were self-reported, as well as support from the non-government health agencies in the past 12 months. Loneliness was rated from none to severe according to agreement with the following statements; ‘I have plenty of friends, and have not been lonely’ (none), ‘Although I have friends, I have been lonely occasionally’ (mild), ‘I have some friends but have been lonely for company’ (moderate) and ‘I have felt socially isolated and lonely’ (severe); for the current analyses, the ‘none’ and ‘mild’ groups were combined into one category. Functional disability was measured using the Personal and Social Performance Scale (PSP) (Morosini et al., 2000). The PSP provides a global functioning rating score out of 100, subdivided into 10 equal intervals. The main areas of functioning considered are social activities, relationships, self-care, and disturbing and aggressive behaviours. For the purpose of this study, the categories were grouped into the following: poor functioning, varying degrees of disability, and absence of disability or only mild difficulties. Life satisfaction was based on response to the question; ‘During the last 12 months how have you been feeling about your life as a whole taking into account what has happened in the last 12 months and what you expect to happen in the future?’. For this study, the responses were categorised into the following groups: (1) Mostly dissatisfied or worse (Terrible, Unhappy and Mostly dissatisfied), (2) Mixed (Mixed) and (3) Mostly satisfied or better (Mostly satisfied, Very pleased and Delighted).
Physical health variables
We examined five variables related to physical health. Physical activity was measured using the International Physical Activity Questionnaire (IPAQ) (Craig et al., 2003). For the purpose of this study, we dichotomised physical activity status into two groups – low (low IPAQ physical activity level only) versus moderate-high (moderate and high IPAQ physical activity levels combined) as previously done using the SHIP data (Suetani et al., 2016). Body mass index (BMI) was calculated using the participant’s height and weight. It was categorised into underweight (less than 18.5), normal (between 18.5 and 24.9), overweight (between 25.0 and 29.9) and obese (more than 30.0). We combined the underweight and normal categories together for our analysis. ‘At risk’ waist circumference was defined as a waist circumference of at least 94 cm in men or 80 cm in women. Metabolic syndrome was classified using the International Diabetes Federation harmonised criteria (Alberti et al., 2009). These criteria require three of the following five risk factors to make the diagnosis: at-risk waist circumference; at-risk diastolic and/or systolic blood pressure; at-risk levels of fasting blood glucose, triglycerides or high-density lipid (HDL). People receiving medications for hypertension, hyperlipidaemia or hyperglycaemia were considered to meet the relevant criterion. Diabetes mellitus diagnosis was made based on the response to the question; ‘Do you have diabetes or have you been told your blood sugars are high?’
Substance use variables
The Fagerström test for nicotine dependence was used to categorise current smoking status into low or high (Heatherton et al., 1991). Participants were asked to self-report lifetime use of alcohol, cannabis and amphetamine. The responses were dichotomised into either any or no use.
Psychiatric symptoms
We examined four main psychiatric symptom domains – positive symptoms, negative symptoms, cognitive symptoms and mood symptoms. Positive symptoms were assessed as present if the participants had ever experienced delusions, hallucinations or subjective thought disorder in their lifetime according to DIP-DM questionnaire. Negative symptoms were assessed to be present if the interviewers rated presence of any of the following: restricted affect, poverty of speech or diminished sense of purpose. Two tests were used to assess cognitive symptoms. First, the National Adult Reading Test (NART-R) is a word-reading test widely used as an estimate of premorbid IQ (Schretlen et al., 2005). Based on summary NART-R scores (M = 97.88, standard deviation [SD] = 11.46), premorbid IQ was categorised into the three following levels: Below Average (>1 SD below sample mean), Average (within 1 SD of sample mean) and Above Average (>1 SD above sample mean). Likewise, the Digit-Symbol Coding task (DSCT) from the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) (Randolph et al., 1998), a test of speed of processing, was used to assess current cognitive ability. The lower the test score, the poorer a person’s speed-based performance. Based on summary DSCT scores (M = 38.65, SD = 10.74), current cognitive ability was categorised into three levels: Below Average (>1 SD below sample mean), Average (within 1 SD of sample mean) and Above Average (>1 SD above sample mean). Finally, mood symptoms (depressive and manic symptoms) were assessed using the DIP-DM questionnaire.
Data analyses
For the purpose of this study, we dichotomised the age at interview into two groups: the older group (those aged between 50 and 65 years) and the younger group (those aged between 18 and 49 years). Group differences in demographic characteristics (sex, age, age of onset, duration of illness, course of illness and DSM-IV-TR diagnoses) were assessed using t-test for continuous variables and chi-square test for categorical variables. We also undertook within-gender comparisons on metabolic, substance use, symptoms and cognitive variables using t-test for continuous variables and chi-square test for categorical variables. A series of logistic regression models were developed to examine factors associated with age group. The primary binary outcome variable was the older group versus the younger group. We calculated the odds ratios (ORs) with 95% confident intervals (CIs) adjusted for sex to estimate the likelihood of participants being in the older group. All analyses were performed using R (version 4.0.0) (R Core Team, 2020) packages tidyr (Wickham and Henry, 2020) and dplyr (Wickham et al., 2020).
Results
Demographic characteristics
Demographic characteristics are summarised in Table 1. The majority of the 1825 participants (81.0%, n = 1478) were aged between 18 and 49 years (M = 34.4, SD = 8.2) while the remaining 19.0% (n = 347) were aged between 50 and 65 years (M = 55.2, SD = 3.9). The older group had a significantly higher proportion of females compared to the younger group (51.9% vs 38.6%, p = 0.001). Age of onset was significantly earlier in the younger age group (22.2 years vs 30.0 years, p < 0.001) but it should be noted that by definition the older group has the potential to include more individuals with later onset illness due to their age. As expected, the duration of illness was significantly shorter in the younger age group (12.2 years vs 25.2 years, p = 0.001). The older group was more likely to have chronic course of illness as opposed to non-chronic course (36.3% vs 29.1%, p = 0.010) and a higher proportion of affective psychosis diagnoses compared to the younger group (44.1% vs 36.5%, p = 0.005).
Demographic characteristics.
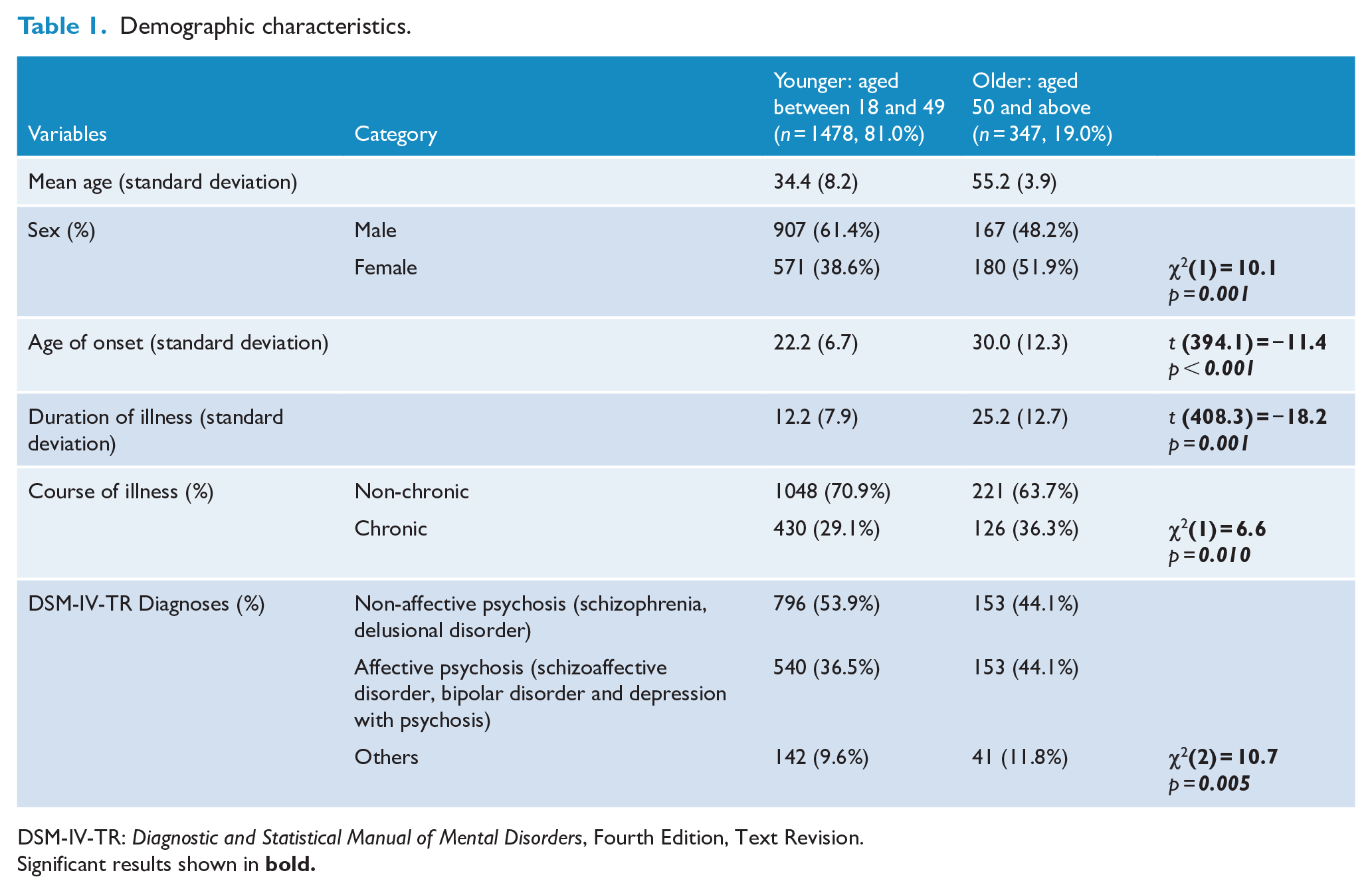
DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision.
Significant results shown in
Social and functional variables
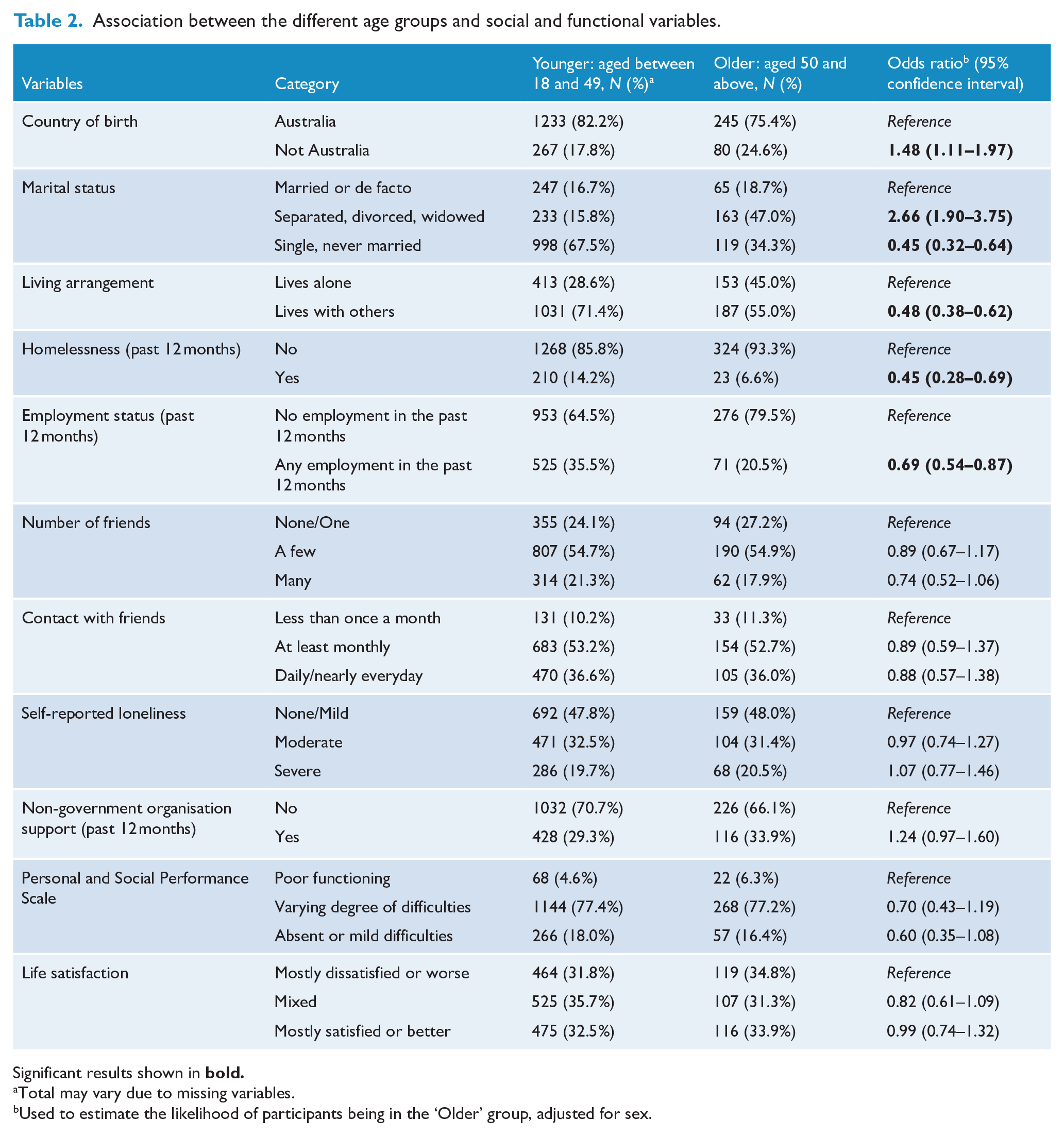
Table 2 presents associations between age group and social and functional variables. Compared to the younger group, the older group were more likely to be born overseas (OR = 1.48, 95% CI: [1.11, 1.97]) and to be divorced/separated (OR = 2.66, 95% CI: [1.90, 3.75]), and less likely to be single (OR = 0.45, 95% CI: [0.32, 0.64]), living with others (i.e. more likely to be living alone) (OR = 0.48, 95% CI: [0.38, 0.62]), to have experienced homelessness in the previous 12 months (OR = 0.45, 95% CI: [0.28, 0.69]) and to have been employed in the previous 12 months (OR = 0.69, 95% CI: [0.54, 0.87]). There were no differences between age groups for the following variables: number of friends, contact with friends, reported loneliness, PSP scores and overall life satisfaction.
Association between the different age groups and social and functional variables.
Significant results shown in
Total may vary due to missing variables.
Used to estimate the likelihood of participants being in the ‘Older’ group, adjusted for sex.
Physical health
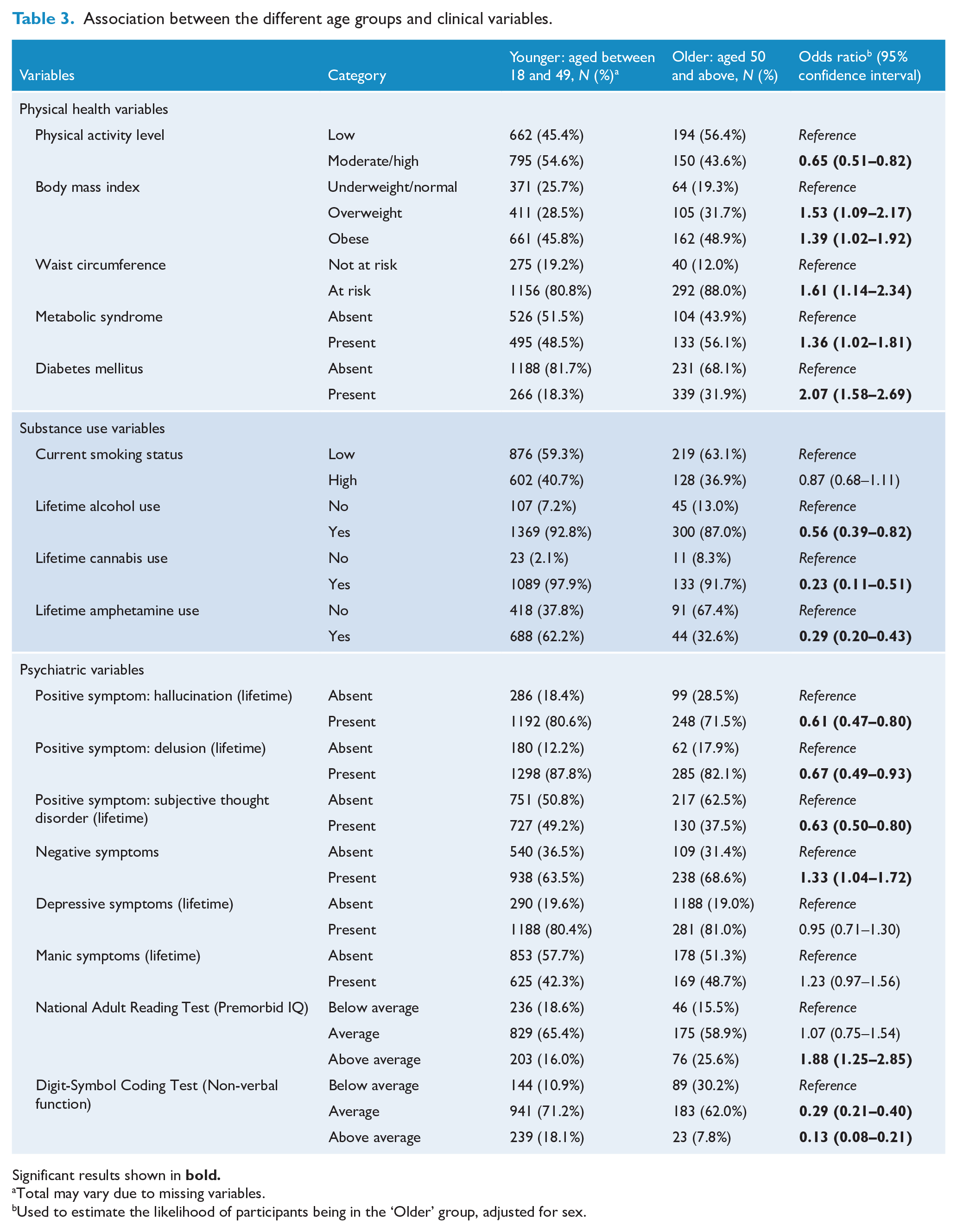
Table 3 shows the association between age group and physical health. Compared to the younger group, the older participants were less likely to be physically active (OR = 0.65, 95% CI: [0.51, 0.82]) and were more likely to be either overweight (OR = 1.53, 95% CI: [1.09, 2.17]) or obese (OR = 1.39, 95% CI: [1.02, 1.92]) and to have an at-risk waist circumference (OR = 1.61, 95% CI: [1.14, 2.34]), metabolic syndrome (OR = 1.36, 95% CI: [1.02, 1.81]) or diabetes mellitus (OR = 2.07, 95% CI: [1.58, 2.69]).
Association between the different age groups and clinical variables.
Significant results shown in
Total may vary due to missing variables.
Used to estimate the likelihood of participants being in the ‘Older’ group, adjusted for sex.
Substance use
Table 3 presents the association between age group and substance use variables. Compared to the younger group, the older group were less likely to report lifetime use of alcohol (OR = 0.56, 95% CI: [0.39, 0.82]), cannabis (OR = 0.23, 95% CI: [0.11, 0.51]) or amphetamines (OR = 0.29, 95% CI: [0.20, 0.43]). There was no association between age group and the current smoking status.
Psychiatric symptoms
Table 3 summarises the association between age group and psychiatric symptoms. Three aspects of positive symptoms were examined. People in the older group were less likely to experience all three positive symptoms compared to people in the younger group. These included hallucinations (OR = 0.61, 95% CI: [0.47, 0.80]), delusions (OR = 0.67, 95% CI: [0.49, 0.93]) and subjective thought disorder (OR = 0.63, 95% CI: [0.50, 0.80]). In contrast, people in the older group were more likely to experience negative symptoms compared to the younger group (OR = 1.33, 95% CI: [1.04, 1.72]). There were no associations between age group and mood symptoms (either depressive symptoms or manic symptoms).
Cognition
In terms of cognitive symptoms, people in the older group were more likely to achieve ‘higher than average’ scores in the NART (OR = 1.88, 95% CI: [1.25, 2.85]), indicating better pre-morbid intelligence, but were less like to achieve either ‘average’ (OR = 0.29, 95% CI: [0.21, 0.40]) or ‘more than average’ (OR = 0.13, 95% CI: [0.08, 0.21]) performance on the DSCT compared to the younger group, indicating poorer attention and working memory.
Gender Differences
We examined gender differences in the patterns of change with ageing. In general, these changes were similar in both genders. Increased rates of at-risk waist circumference were significant in older men (83.5%) compared with younger men (74.7%), χ2 (1, N = 180) = 5.87, p = 0.015, but not in older women (92.9%) compared with younger women (90.7%), χ2 (1, N = 167) = 0.52, p = 0.470. This reflected the much higher rates of at-risk waist circumference in younger women (90.7%), compared to young men (74.7%). The increase in rates of diabetes was significant in both men and women. Lifetime alcohol, cannabis and amphetamine used declined with age in both genders, but overall were lower in women (Table 4).
Changes in substance use and cognition with age, by gender.
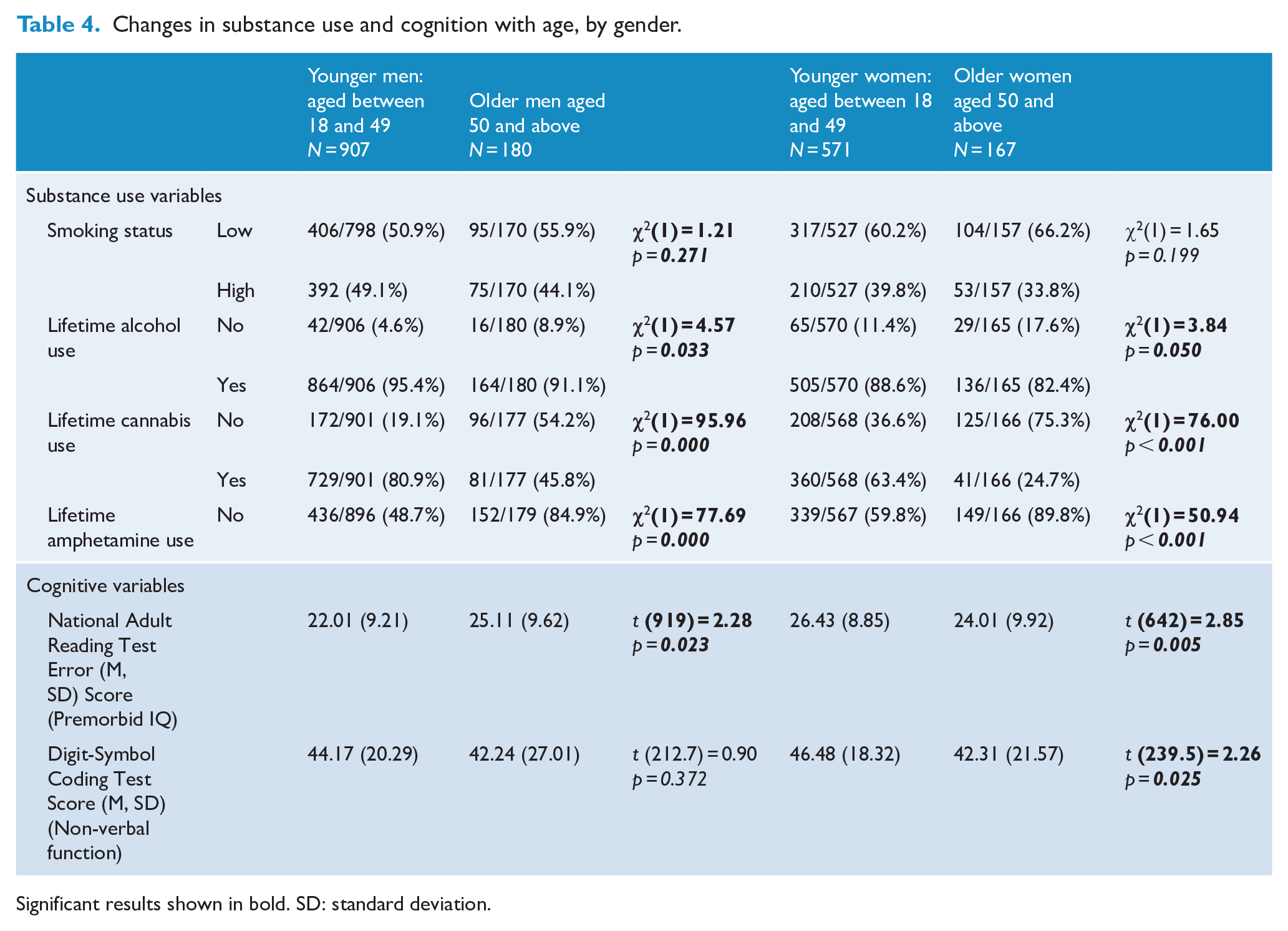
Significant results shown in bold. SD: standard deviation.
Both men and women had a reduction in positive symptoms and increase in negative symptoms with age. Interestingly, older men and younger women had higher NART scores, indicating higher premorbid intelligence, compared with the other group of the same gender. Both genders had a decline in DSCT scores with age, indicating poorer attention and working memory, but this reached significance only in women.
Discussion
Using a large cross-sectional national dataset, we compared a wide range of variables between people with psychosis who were currently 18–49 years and those who were 50 years or older. The older group contained a higher proportion of women and more people with affective psychoses. Age of onset was significantly earlier in the younger age group (22.2 years vs 30.0 years, p < 0.001), but it should be noted that the older group has the potential to include more individuals with later onset illness due to their age.
Even though the older people were more likely to be divorced, unemployed or living alone, there were no significant differences in level of social engagement between the two groups. As anticipated, older people were less likely to be physically active and more likely to have physical health issues such as obesity, metabolic syndrome and diabetes mellitus. Despite having lived for longer, the older participants were also less likely than their younger counterparts to have used alcohol, cannabis or amphetamines in their lifetime. Finally, in terms of psychiatric symptoms, people in the older group were less likely to be experiencing positive symptoms but more likely to manifest negative symptoms. The higher NART scores in the older group suggest higher premorbid IQ, while the lower scores on the Digit-Symbol Coding Test (DSCT) indicate more severe current cognitive impairment, although there were gender differences, as described later.
To our knowledge, this is the first comprehensive, nationally representative study of people living with a psychotic disorder, to compare younger people with psychosis with those in middle age (50–65 years), who have experienced more years living with their illness. There are several possible explanations for the differences between these two groups. Some of these could reflect societal changes over time in Australia. For example, there might be greater use of illicit substances by people born after 1960. A previous comparison between the 1997 and 2010 SHIP cohorts (Moore et al., 2012) found that there had been an increase in prevalence of alcohol and illicit substance use in 2010, while tobacco use stayed about the same. This suggests that the change we see in this study may be a cohort effect, rather than being driven by ageing per se. At the same time, it could also be hypothesised that the absence of illicit substance use in the older group may reflect healthier lifestyle, thus increasing the likelihood of the individuals ‘surviving’ to the older age. Illicit drug use in older people is increasing worldwide, and this has implications for future service delivery and the long-term health impacts of drug use on people ageing with a psychotic disorder and comorbid drug use (Beynon, 2009). The lower rates of substance abuse in the older participants were found in both genders, but both younger and older women used less drugs and alcohol than men. This gender difference is typical of general societal patterns of substance use.
We also postulate that there may be attrition due to premature mortality, affecting some subgroups more than others – for example, men with schizophrenia may have been more likely to die young, leading to a relative excess of women with affective psychosis in the older age group. Inclusion in the SHIP study was defined by contact with public mental health services and non-government organisations in the preceding 12 months. It is possible that more men had substance-induced psychoses and later recovered with age and maturity, so these older men were not included in the study.
People with a more favourable course of illness or better cognitive functioning may also cease service contact before they reach the middle age and beyond, simply because they are well or symptoms have remitted (for instance, it is estimated that 20–50% of older people with psychotic disorders achieve remission or significant improvement in symptoms; Cohen et al., 2020). In addition, some of the differences between the younger and older participants might be the normal course of ageing with a psychotic disorder – such as a gradual reduction in positive symptoms and increase in negative symptoms. It is also possible that the improvement in positive symptoms is attributable to better self-management and coping mechanisms (e.g. acceptance and humour; Cohen et al., 2020).
Other factors such as poorer cognitive function, a more chronic course of illness and a greater likelihood of living alone might also be a consequence of ageing with psychosis. It is worth noticing, however, that despite these declines, the older group do not demonstrate further deterioration in social functioning but rather seem to have levelled out (Cohen et al., 2015). Some of these findings may be attributed to the concept of the paradox of ageing – that is, despite the age-related decline in physical and cognitive function, older people report improved psychosocial functioning and subjective quality of life. This may result from an increasing awareness and acceptance of the finitude of life, while continuing to engage in living within the context of changing levels of frailty and dependence on others (Anderson and Albans, 2019). It has been proposed that this paradoxical effect is more striking in people with psychotic disorders than the general population (Jeste et al., 2011). This may be due to many older people with psychotic disorders developing better illness management through positive coping strategies and increased social support, leading to increased clinical remission, reduced relapse or hospitalisation, and enhanced self-esteem (Cohen et al., 2020). This subjective perception of ageing well in this population may also reflect an improved ability to personally engage with valued activities, to maintain positive relationships, including with the person’s health care professionals, and developing a sense of acceptance of challenges and mastery over their mental illness (Smart, 2018).
Our findings are largely consistent with recent findings that show considerable fluctuation in clinical and psychosocial parameters in the course of psychosis in later life (Cohen et al., 2020). Morgan et al. (2017) have identified the following challenges for people living with psychotic disorder: financial problems, loneliness, poor physical health, uncontrolled symptoms of mental illness and unstable housing. In this study, we found that most of these challenges are present in the older group, but there are some differences. For the older group, poor physical health, negative symptoms and cognitive impairment were more prominent challenges compared to the younger group. We also suspect that the nature of the challenges such as loneliness and financial difficulties might be more nuanced compared to the young cohort. That is, the challenges in the older cohort might arise from the accumulative losses, rather than acute losses. The ongoing challenges in life are likely to have resulted from the struggle between trying to achieve a ‘normal’ life and living with consequences of psychotic disorder; it is an accumulation of social and familial rejections, hospitalisations and treatment side effects, loss of potential employment and life that could have been or should have been over the preceding decades (Cohen et al., 2020). In the context of these challenges, people ageing with a severe mental illness have increased risk of unwanted institutionalisation, typically against their preferences, either in residential aged care or state care (Bartels, 2003; Druss et al., 2000; Mueser et al., 2010).
In view of this, we urgently require further consideration of how we address the unique needs of older people living with psychotic disorders. For example, our findings suggest that the older cohort may benefit more from specific interventions targeting their physical health and cognitive difficulties rather than the focus on family intervention and substance use issues which are more prominent in the current model of service provision. The Helping Older People Experience Success (HOPES) study used a randomised controlled trial over 3 years to evaluate a programme for people over the age of 50 living with severe mental illness, integrating psychosocial skills training with medical case management, including a focus on primary prevention. The study demonstrated improved outcomes in negative symptoms and well-being, including uptake of preventive healthcare interventions across the 3 years (Bartels et al., 2014; Mueser et al., 2010).
While we are hopeful that the increased attention to the importance of physical health of people with psychotic disorders in recent years (Suetani et al., 2017) is starting to have significant downstream benefit, the current findings highlight the fact that for any lifestyle intervention to be truly meaningful, benefits need to be sustainable. In practical terms, for example, for an older population with significantly lower levels of physical activity (Suetani et al., 2016), low-intensity interventions such as walking groups may have long-lasting impact. Previous studies using the SHIP data have found that people with psychotic disorders showed earlier onset of cardiovascular risk indicators compared to the general population (Foley et al., 2015). Despite this, even when physical health conditions were identified, there was often suboptimal management of these conditions (Galletly et al., 2012). These findings strongly indicate that there should be an increased service focus on the physical health of people with psychotic disorders, especially those who are aged over 50 years. Likewise, given the differences in the cognitive profile of the older group compared to the younger group, there is a need for more assertive assessment and provision of targeted interventions in this cohort. In fact, we argue that for those aged above 50, even those who are not old enough to qualify for specialist psychogeriatric services, there should be a subtle shift in the focus of care with the emphasis on disease and disability shifting to positive health and well-being (i.e. successful ageing and adaptation to the illness). When attention to physical well-being is combined with the promotion of improved psychosocial functioning through meaningful activity and community engagement, the dividends for older people with psychotic disorders may be profound. This provides positive direction for the enhancement of mental health service delivery for this population but has implications for workforce development to meet the needs of the growing population ageing with psychosis (Bartels et al., 2014).
There were some gender differences in metabolic health; most strikingly, younger women had very high rates of at-risk waist circumference. There may be gender differences in the types of interventions that are preferred and most effective. While gender differences in assessment, prescribing and service provision for women with schizophrenia and related disorders have been described (Galletly et al., 2016), there has been little research into developing the most effective physical health interventions for these women despite the very significant need.
A shift in the focus of service provision may also lead to an increase in clinical research into improving non-pharmacological interventions for this group. For example, it would be possible to assess the feasibility of a trial of reduction or discontinuation of antipsychotic medication in the older population, such as has been proposed for the early psychosis population (Galletly et al., 2018). This is particularly important in view of established physical side effects and possible cognitive side effects on long-term exposure to antipsychotic medication (Cohen et al., 2020). Similarly, deprescribing of other medications can be associated with health benefits (Liacos et al., 2020). Taking all of these considerations into account, it is possible that the unique needs of older people with psychotic disorders, who may be experiencing important life and health transitions, may be best met by specialist teams, similar to the early psychosis teams (i.e. late psychosis teams), or by enhanced collaborations between younger and older adult mental health services along with improved access to geriatric medicine.
Limitations
A major strength of this study was that we were able to examine a wide range of variables in a large, nationally representative sample of people with psychotic disorders. However, there are a number of limitations and the interpretation of our findings requires caution. The survey was cross-sectional, so there may be inaccurate recall of items such as lifetime hallucinations and delusions. The survey design did not include a control population; thus, we cannot make inferences about how individuals with psychotic disorder differ from the general population. Moreover, as the study was conducted in Australia, the findings may not be generalisable to other countries.
The cross-sectional nature of the data precludes making any causal inferences linking age group and the examined variables. In addition, even though the SHIP sample is representative of people receiving support from public mental health services and non-government organisations, it does not include those in the private mental health services or those who have dropped out of treatment altogether.
Finally, due to its methodology (the recruitment was stratified by age group), the current dataset had a disproportionally higher number of younger participants, aged between 18 and 34 years, compared to the older group. However, within the younger group, there was an almost equal proportion of participants aged less than 35 years (n = 773, 52.3%) and those aged between 35 and 49 years (n = 703, 47.7%), thus making it unlikely that the results of our findings were disproportionally impacted by those younger than 35 years.
The SHIP survey had an upper age limit of 65 years and it is acknowledged that further investigation of this population is warranted, as they age beyond 65. Future surveys should consider the importance of this fast-growing cohort and ensure continuity in research beyond the age of 65 years, rather than be limited by service delivery age cut-offs that reflect administrative divisions rather than true progression of the cohort. At the same time, investigators should be cautious of the diagnostic overlap between psychotic disorders and age-related neurocognitive impairment.
Conclusion
Our findings suggest that there are some significant differences between younger people with psychosis and those who are older. To ensure better support and care for older people with psychotic disorders, an improved understanding of the challenges and complexities encountered by this population is needed.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw and H. Stain. Ethical approval for the study was obtained from relevant institutional human research ethics committees. The study was funded by the Australian Government Department of Health and Ageing. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by the Australian Government Department of Health and Ageing.