
Abstract

There has been concerted political advocacy for early intervention among young people (aged 12–25), leading to substantial investment in youth mental health, especially via headspace and Better Access, in Australia (Looi et al., 2019, 2020, in press). However, Jorm and Kitchener (2020) have concluded that since the introduction of the Better Access scheme and headspace centres, there has been no reduction in the population prevalence of youth psychological distress, ‘Rather, there appeared to be a worsening of youth mental health from around 2015 onwards . . .’ with a 47% increase in the population prevalence of very high and high levels of youth psychological distress, compared to 2003–2006, prior to the commencement of headspace and Better Access (Jorm and Kitchener, 2020). Youth psychological distress increased from 15% to 22% of the youth population over the period.
Better Access and headspace centres were also expected to prevent youth suicide. However, there also appears to have been a worsening of self-harm-related hospitalisations and youth suicide (see Table 1 – Australian Bureau of Statistics (ABS), 2020; Australian Institute of Health and Welfare (AIHW), 2020), in parallel with the observed rise in psychological distress (Jorm and Kitchener, 2020).
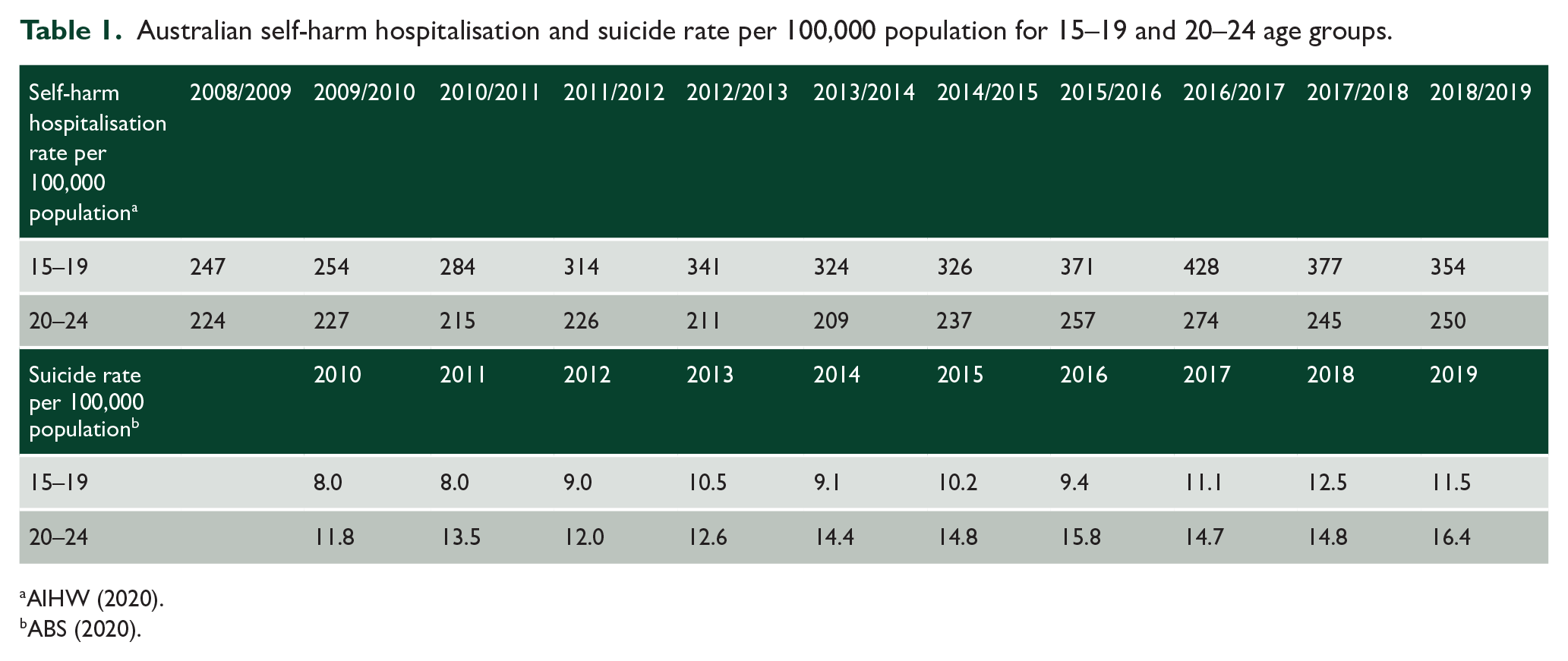
Australian self-harm hospitalisation and suicide rate per 100,000 population for 15–19 and 20–24 age groups.
Youth self-harm hospitalisation and suicide rates are rising
Self-harm hospitalisation rates for the 15–19 age group (see Table 1 – AIHW, 2020) increased by 43%, rising from 247 per 100,000 population in 2008/2009 to 354 per 100,000 population in 2018/2019. Self-harm hospitalisation rates for the 20–24 age group have risen by 12%, increasing from 224 per 100,000 population in 2008/2009 to 250 per 100,000 population in 2018/2019.
Suicide rates for the 15–19 age group (see Table 1 – ABS, 2020) increased by 43%, rising from 8 per 100,000 population in 2010 to 11.5 per 100,000 population in 2019. Suicide rates for the 20–24 age group increased by 39% from 11.8 per 100,000 population in 2010 to 16.4 per 100,000 population in 2019.
Therefore, we agree with Jorm and Kitchener (2020) that Australian investment in headspace and Better Access urgently needs to be reviewed in light of the rising levels of psychological distress, self-harm and suicide among young people.
Are there structural and quality of care issues?
Jorm and Kitchener (2020) advocate for a national discussion about youth mental health in the context of declining youth mental health outcomes despite significant national investment. We agree, highlighting the lack of coordination between the Federally funded headspace centres and State mental health services. The Federal Government committed funding to headspace without adequate coordination with State governments, which led to duplication, confusion and fragmentation in the youth sector (Looi et al., 2019) that might have contributed to the poorer population mental health outcomes (Jorm and Kitchener, 2020). headspace centres are often not integrated with local communities because they are not properly linked with the state mental health services and therefore may not be attuned to local mental health planning requirements (Looi et al., 2019, in press). These concerns are reflected in the Productivity Commission’s Report on Mental Health (#95) recommending that the allocation for headspace from pooled State/Federal funds be no longer ring-fenced. In contrast to the non-governmental organization (NGO)-led model, public mental health services are lead agencies for some headspace centres in Melbourne, allowing a single point of entry and coordinated services, which presents a more effective integrated youth mental healthcare model (Looi et al., 2020).
We agree with Jorm and Kitchener (2020) that there are important sociological determinants of youth mental health for which the headspace and Better Access healthcare interventions may have limited efficacy and that the performance of headspace and Better Access may be somewhat limited.
Jorm and Kitchener (2020) have also proposed a possible ‘quality gap’ in terms of patients not receiving minimally adequate psychological treatment duration, to partially explain the lack of effectiveness of Better Access and headspace. In particular, we highlight the lack of psychiatric leadership and management of suicide risk in both initiatives. Headspace centres have established 115 separate NGO-led stand-alone clinics staffed by multidisciplinary clinicians (Looi et al., in press). However not all headspace centres have medical staff, which necessitates referral to general practitioners (GPs) and psychiatrists if medical care is needed, and it is not clear that subsequent care is coordinated with public mental health services (Looi et al., 2019, in press). This specific lack of specialist psychiatric input within headspace impacts on the delivery of comprehensive biopsychosocial care, including appropriate case formulation and pharmacological management. In summary, the lack of psychiatrists in leadership, clinical governance and clinical involvement within headspace centres means that complex cases presenting in crisis and suicidal ideation are often referred to public mental health services and emergency departments (Looi et al., 2019) and these referrals likely contribute to the rise in self-harm presentations to the emergency departments. Like headspace clinicians, Better Access clinicians might also be inexperienced in managing acute mental health presentations and may need to refer these patients to emergency departments. Better Access clinicians may also lack specific expertise and training in adolescent and youth mental health and therefore are not be able to work systemically across family, partner and peer interactions across home, education and work domains.
Accordingly, there should be further innovative research into the most appropriate Australian youth mental healthcare model, and clinical outcomes, in addition to ongoing evaluation of Better Access and headspace.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.