
Abstract

To the Editor
This article provides a case history of sudden onset diabetes in the absence of weight gain and suggests that olanzapine may induce an atypical form of diabetes.
A 31-year-old Japanese male with schizophrenia of normal weight (body mass index [BMI]: 23 kg/m2) was admitted to our hospital because of drowsiness. He had been treated with olanzapine 20 mg/day for 8 weeks and was quite well with HbA1c of 5.3% 1 month ago. On admission, he showed severe hyperglycemia (30.3 mmol/L) and a high HbA1c level (7.6%) with urine ketone bodies, indicative of ketoacidosis. Tests for anti-glutamic acid decarboxylase antibody and anti-insulinoma-associated antigen-2 antibody were negative. He also had no family history of diabetes. Olanzapine was discontinued and 6 weeks of insulin therapy resulted in a decrease in fasting blood glucose (30.3–5.7 mmol/L) and an increase in C-peptide (0.2–2.3 ng/mL). Consequently, insulin replacement therapy was not needed to control blood glucose.
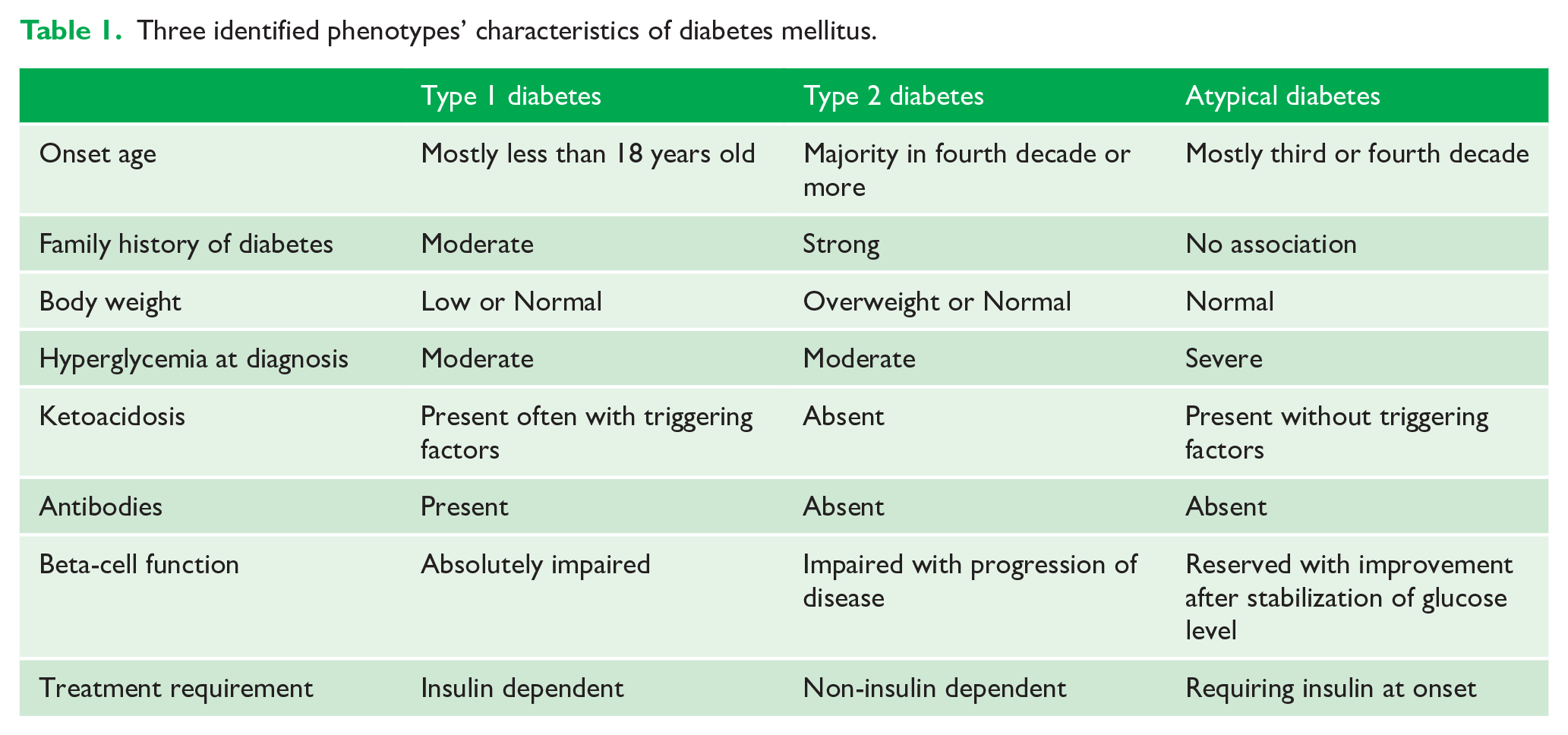
There are two main types of diabetes. Type 1 diabetes is characterized by immune-mediated destruction of the insulin-secreting beta-cells, which usually leads to absolute insulin deficiency and dependence on exogenous insulin. Type 2 diabetes is an undefined polygenic disorder with various degrees of insulin resistance preceding progressive insulin secretory defects. However, olanzapine may cause an atypical presentation of diabetes that does not fit into the definition of these two classic recognized types (Nagamine, 2018). Atypical diabetes, like type 1 diabetes, is diagnosed when an individual presents with severe hyperglycemia and ketoacidosis. However, unlike type 1 diabetes, patients with atypical diabetes become insulin-independent after temporary insulin replacement therapy. They also do not have the antibodies found in patients with type 1 diabetes. To establish the differential diagnosis, factors including antibodies and beta-cell function should be taken into account (Table 1). The underlying mechanisms linking olanzapine and diabetes onset are not fully explained. One possible mechanism involves pancreatic muscarinic M3 receptor blockade by olanzapine, resulting in loss of ability to respond to changes in blood glucose levels (Hahn et al., 2011). Another possibility involves olanzapine-induced proinsulin misfolding that is due to the impairment of proper disulfide bond formation, resulting in impaired insulin secretion (Ninagawa et al., 2020).
Three identified phenotypes’ characteristics of diabetes mellitus.
In conclusion, while most diabetic schizophrenia patients have type 2 diabetes, there may be an atypical form of diabetes when using olanzapine. Clinicians should be aware of this rare form of diabetes because adequate treatments could attenuate this type of diabetes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.