
Abstract
Objective:
Trans and gender diverse young people experience mental health difficulties self-harm and suicidality at markedly higher rates than the general population, yet they often feel isolated from mental health services. There is little qualitative research on the experiences of trans and gender diverse young people accessing mental health support in Australia. The objective of this study was to comprehensively explore the experiences of trans and gender diverse young people in Australia who have sought mental health support from therapists, counsellors, psychiatrists and/or inpatient care providers.
Methods:
We report on findings from the Trans Pathways study, which was a mixed-methods study to evaluate the experiences of trans and gender diverse young people accessing mental health services: specifically, therapy and counselling services, psychiatric services and mental health inpatient services.
Results:
A total of 859 trans and gender diverse young people aged 14–25 years across Australia completed an anonymous online questionnaire. Therapy and/or counselling services (64.4%) were most frequently sought by trans and gender diverse young people in this study, followed by psychiatric services (43.0%) and mental health inpatient services (12.3%). The findings demonstrated that many mental health professionals lacked expertise in gender diversity, and that trans and gender diverse young people found it difficult to locate mental health professionals who were able to meet their needs in a timely manner.
Conclusion:
These findings indicate that training is necessary for all mental health professionals to improve their knowledge of gender diversity, enhance the support provided to trans and gender diverse young people and help to address the high rates of poor mental health. The findings outlined here provide insight into the areas in which clinicians could optimise their care of trans and gender diverse young people.
Introduction
Trans and gender diverse (TGD) 1 young people have a gender incongruent with the sex assigned to them at birth. Recent research indicates that 2.3% of high-school-aged young people in Australia are trans and/or gender diverse (Fisher et al., 2019), which is similar to some recent estimates in other parts of the world (2.7% of US adolescents, for example, reported a transgender or gender nonconforming identity) (Rider et al., 2018). TGD young people commonly report negative life experiences, including discrimination, insufficient familial support, bullying and isolation. These experiences are in turn associated with alarmingly high rates of mental health difficulties: notably, depression, anxiety, post-traumatic stress disorder, self-harm and suicidal ideation and attempts (Strauss et al., 2020a). Our recent study found that three in four TGD young people in Australia have been diagnosed with depression and/or anxiety, and almost one in two have ever attempted suicide (Strauss et al., 2020a). This contrasts sharply with the reported 15% and 26.3% of Australians in the general population (aged 16 years and older) who will experience (respectively) depression and anxiety during their lifetimes (Australian Bureau of Statistics, 2007).
TGD young people in Australia experience barriers in accessing mental health services, even when they are seeking support for general mental health concerns that may not be directly related to gender identity or gender-affirming medical interventions (Riley et al., 2011). Service providers that specialise in TGD mental health often have long waiting lists (Erasmus et al., 2015), which further contributes to poor outcomes (Rotondi et al., 2013). Furthermore, TGD young people may be hesitant to access mental health services due to stigma and the expectation of discrimination from health professionals (Ho and Mussap, 2017; Telfer et al., 2018). Geographical barriers for TGD young people who live in rural locations may also prevent access to both mainstream and specialised services (Telfer et al., 2018). Such barriers to health care pose a threat to the resilience of TGD youth (Singh et al., 2014). The sense of isolation from services that TGD young people experience has been associated with symptoms of depression and anxiety, as well as higher rates of self-reported self-harming behaviours and suicide attempts (Strauss et al., 2020a).
Previous research has shown that major issues in psychological practice involving TGD youth include an avoidance of gender discussions, (conversely) over-focusing on gender, insufficient education on TGD health on the part of the care provider and gatekeeping (Chisolm-Straker et al., 2017; Mizock and Lundquist, 2016). TGD individuals often feel mental health practitioners are poorly informed about gender concerns and experiences (Ellis et al., 2015). An Australian report in 2014 indicated 66% of TGD young people had seen a mental health professional within the prior 12 months, and that more than half of them reported at least one negative experience in this context (Smith et al., 2014). Misgendering is being disrespectful of an individual’s gender identity (e.g. through using incorrect pronouns), and this is a stigmatising and potentially traumatic experience, and can lead to an avoidance of health care services later in life (Dolan et al., 2020; Riggs et al., 2014).
There is at present minimal research on the experiences of access to mental health services among TGD young people in Australia. The strengths and limitations of service provision for TGD young people still remain largely unknown and understudied in the national context. Considering the elevated rates of poor mental health within this population, access to comprehensive and TGD-competent care is vital (Reisner et al., 2016). One of the principle aims of the Trans Pathways project discussed in this paper was to comprehensively explore the experiences of TGD young people in Australia who have sought mental health support from therapists, counsellors, psychiatrists and/or inpatient care providers.
Methods
We conducted a national cross-sectional survey (Trans Pathways) to assess the mental health and experiences of services by TGD young people. The online survey was developed in partnership with local TGD community members, and encompassed questions on mental health, drivers of mental health difficulties, positive factors influencing mental health and barriers to mental health services. Participants were recruited across Australia, through social media, gender clinics, youth mental health services, LGBTIQ (lesbian, gay, bisexual, transgender, intersex and questioning) support groups, parent and youth groups and word of mouth. Participants received a participant information form and consented to the study online. Parental consent was waived for this study. The study was approved by the Ethics Committee of the University of Western Australia (No. RA/4/1/7958). Qualtrics online survey software was used to construct and host the questionnaire, which utilised branch, display and skip logic based on participant responses. All questions were voluntary, except those used to determine eligibility (i.e. TGD identification, age, place of residence).
Measures
This paper reports on findings related to experiences in accessing therapy/counselling services, psychiatric services and mental health inpatient care. Using open-ended questions, participants were asked about reasons for service access, age at first access attempt, length of wait until first access and frequency of access attempts. Participants also rated their satisfaction with each service (once accessed) using a five-point Likert-type scale, and indicated whether staff at the specific service were respectful of their gender identity. For each service, participants were also provided with the opportunity to describe their experience in more detail.
Statistical methods
IBM SPSS Statistics (version 24) was used to calculate the frequencies of access rates. Participant age at the time of service access was stratified into those below 18 years versus 18 or older. Access rates were also analysed by sex assigned at birth. For all questions, participants who stated ‘I don’t know’ or ‘I can’t remember’ were not included in the sub-analysis of waiting times and number of appointments. Qualitative responses were coded using NVivo, including reasons for accessing the service and experiences of the service attendance. Qualitative data were read and reread by two researchers (P.S. and Z.W.) to determine common themes and to ensure rigour in the analysis. Given the paucity of literature in this specific field, a general inductive approach was used to inform the qualitative data analysis. This was selected in order to draw themes directly from the data rather than approaching the responses with a predetermined set of themes (Thomas, 2006). Because of the large sample size and range of responses, only major themes are reported here.
Results
Participants
We surveyed 859 TGD young people aged 14–25 years in the Trans Pathways study. The overall sample had a mean age of 19.37 (SD = 3.15) years, with 74.4% of participants assigned female at birth (N = 639) and 25.6% assigned male at birth (N = 220). Participants described their gender identity in an open text box, and these gender identities have been categorised into non-binary (48.5%, N = 417), male/trans male (29.7%, N = 255), female/trans female (15.0%, N = 129) and ‘other’ including questioning and unsure (6.8%, N = 58). Additional demographic details on this cohort have been described in detail elsewhere (Strauss et al., 2017, 2020a, 2020b).
Summary of services accessed
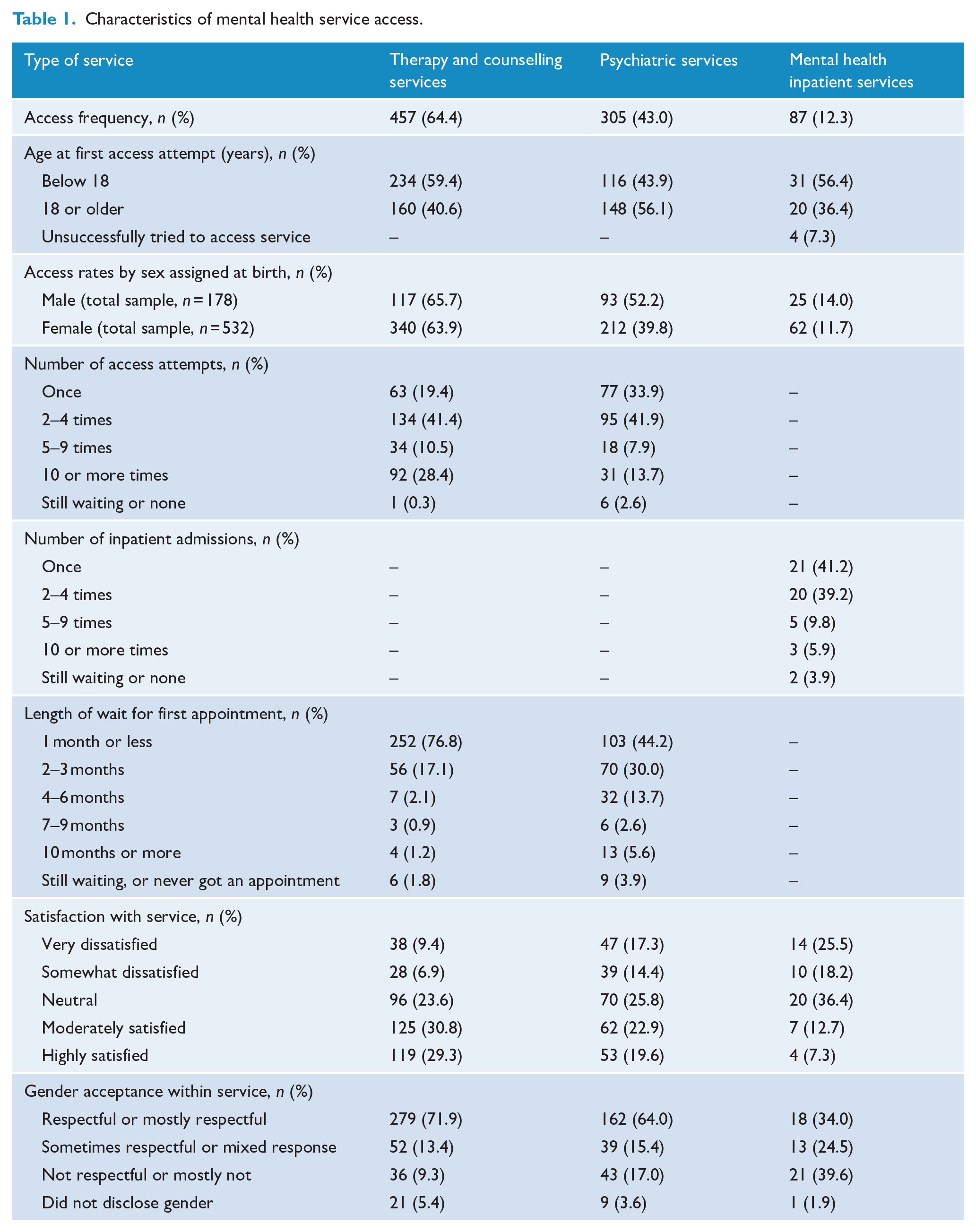
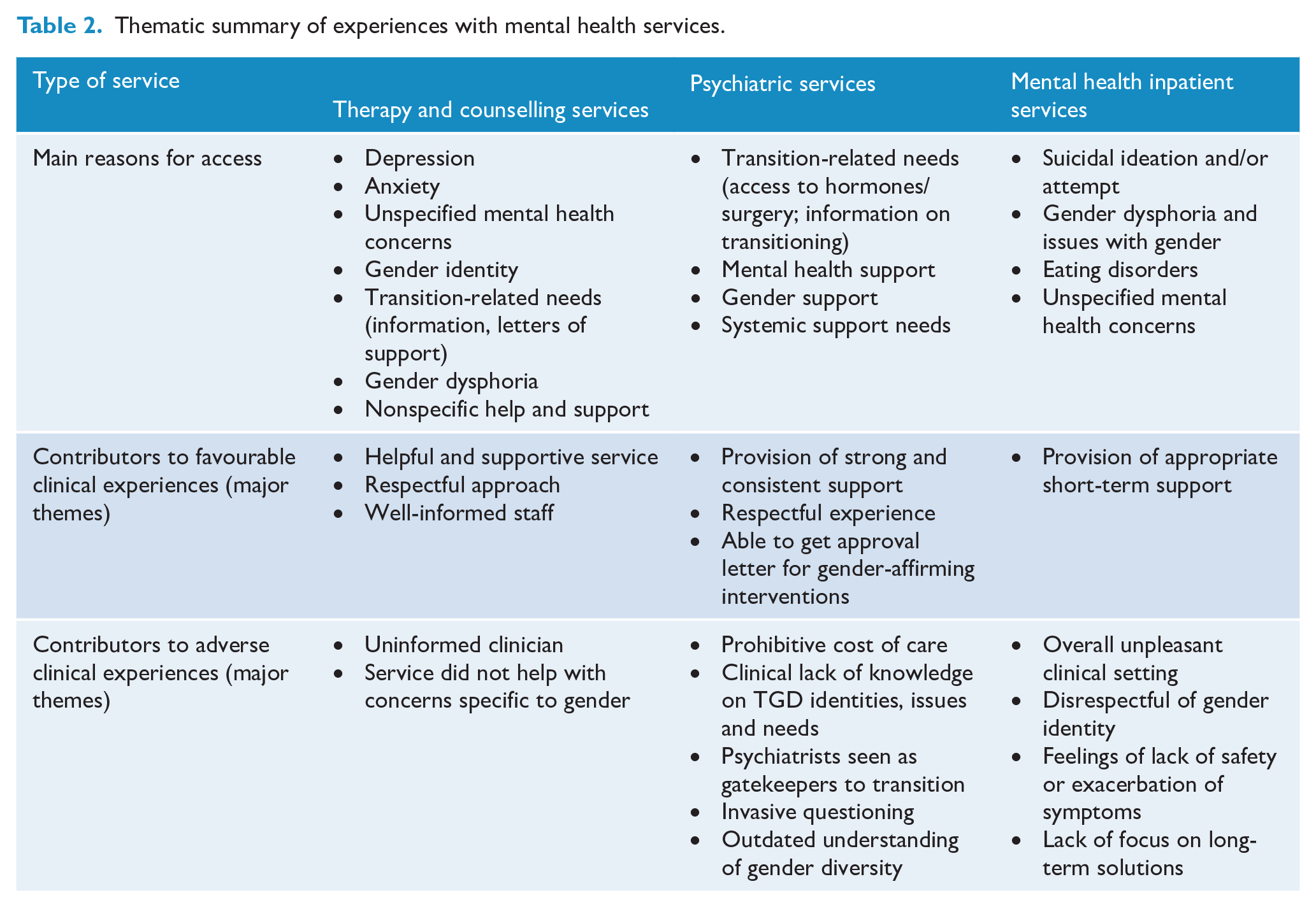
Table 1 reports on characteristics of service access, including age at access, differences in accessing services by sex assigned at birth, number of times accessed before receiving help, length of wait for appointment, satisfaction with the service and whether gender was respected within the service. Therapy and counselling services, as well as mental health inpatient services, were more commonly accessed by participants below 18 years of age, whereas psychiatric services were more commonly accessed by individuals aged 18 years or older. The type of service accessed was broadly comparable across sex assigned at birth, with the exception of psychiatric services which were more commonly accessed by participants assigned male at birth (52.2% compared to 39.8%). Table 2 reports on major themes emerging from the qualitative data relating to (a) the reasons for accessing each type of mental health service and (b) experiences within the specific service. The main findings for each mental health service are described in detail below.
Characteristics of mental health service access.
Thematic summary of experiences with mental health services.
Therapy and counselling services
Participants tended to access therapeutic services at younger ages, with 59.4% being below the age of 18 years. One-third of participants were seen by a private psychologist (33.3%), 21.3% attended a public mental health service, 23.8% accessed headspace (a youth-focused national mental health service; McGorry et al., 2007), 10.3% were seen by their university or school psychologist and 11.3% accessed other counselling and therapy services. Therapy and counselling services were reported to be largely respectful or mostly respectful of the young person’s gender (71.9%), and the majority of participants were moderately or highly satisfied with the service (60.1%).
Many participants had relatively short wait times (76.8% had 1 month or less) for their first appointment with a therapist or counsellor. The underlying reasons for this finding were complex. For example, one participant reported that they only waited 3 days for an appointment because they were already in hospital for a suicide attempt. Other participants described similar circumstances around their initial appointments, in which suicidal thoughts and behaviours increased the likelihood of being promptly reviewed by a mental health professional:
Immediately, as I was in crisis when I wanted to see [a mental health professional] so they let me see them right away which was very lucky.
Most participants accessed therapy and counselling services for help with depression, anxiety, gender-related needs (namely, gender identity, dysphoria, transitioning) and non-specific mental health concerns (e.g. ‘to get help’). Many participants sought therapy to assist with multiple issues they were experiencing such as ‘gender dysphoria and associated stress and academic struggles and anxiety’. Often the desired help and support related to adapting to their gender, and seeking help to ‘navigate the world’ (including relationships with families, school, friends) as their true selves:
To help with the stressful situations in my life; such as family, being accepted as trans, how to cope with others treating me differently because of being trans.
Participants also commonly sought out therapeutic services to track and support their mental health as they started on hormonal intervention:
Assistance in dealing with/overcoming social anxiety in relation to being trans, as well as monitoring through HRT [hormone replacement therapy] process.
Other gender-related concerns were specifically around sourcing information about gender and the young person’s understanding of their own gender:
To understand more about gender and how that could relate to me and how to not hate myself and worry about other people hating me. As well as decisions for future options that could arise linked to transitioning.
For many TGD young people in this study, experiences with therapy and counselling services were largely positive:
My current psychologist is very helpful. She’s helped me come up with techniques to mitigate my depression and help me feel better. She also helps me deal with my family and has spoken to my parents on my behalf, giving her professional opinion as a psychologist. She’s told me about many resources and helped me get them when needed.
Some participants said that the experience benefitted them more than they had initially anticipated. Many respondents also felt their experience within the counselling service overall was supportive of their gender, sexuality and/or general mental health:
I have been to so many psychologists that I can’t remember most. But the last 2 (past 4 years) have been very supportive and very understanding of my sexuality and gender identity.
Within this theme, some participants noted that although the experience itself felt generally supportive, the clinical and auxiliary staff at the service did not always have much knowledge about gender diversity, particularly dysphoria and transitioning. However, respect within services and a clear desire to help the young person were valued by participants, even when the professional lacked knowledge of gender diversity:
It was just the school psychologist because I wasn’t allowed a private one for gender issues because my parents view my dysphoria as being caused by anxiety . . . [the school psychologist] was very respectful of pronouns and helped me talk to my parents about it and tried to get me a mental health plan which they decided was not necessary but at least he tried.
Many participants had mixed experiences, in which they reported negative experiences with some professionals, but positive experiences with others. Respondents often saw multiple mental health professionals before settling on one who was able to respond to their needs, although cost or other factors sometimes prevented the young person from accessing ongoing care:
One psychologist talked about me to other people, one guilt tripped me, one my parents cut off because she was too good and was helping me lots and they didn’t like that, and the most recent one doesn’t help at all and doesn’t care.
In terms of negative experiences, concerns that were commonly raised by study participants related to feelings of invalidation and of being dismissed for wanting to talk to a professional about gender:
The service ended up making me feel worse than when I arrived. Also, there was a general tendency not to take my body dysphoria or my need to see someone who was actually knowledgeable about transgender issues seriously. People asked questions that made it clear they didn’t really know anything, and seemed to think they knew more about my problems than I did.
Psychiatric services
Psychiatric services were accessed more frequently by participants aged 18 years or older (56.1% vs 43.9% for below 18 years). Participants did not typically experience protracted delays before their first psychiatric appointment: 44.2% saw a psychiatrist within 1 month, and 30% saw a psychiatrist within 2–3 months. However, some participants commented that they often faced lengthy wait times for review by a psychiatrist who was known to be TGD friendly, which resulted in delays in beginning gender-affirming medical intervention.
Participants sought psychiatric services mainly for transition-related needs, for conversations and support specific to their gender identity, general mental health support and systemic support needs (mostly referrals to other services, including transition-related services such as endocrinologists). Transition-related needs most commonly involved facilitating access to hormones and/or surgery, discussion and information on transition, assistance with legal gender affirmation and unspecified transition needs. One participant stated that the principal reason for seeking psychiatric services was,
To be diagnosed with gender identity disorder/gender dysphoria, and be approved for hormones and surgeries.
Many participants sought assistance from psychiatric services to help them with multiple concerns with their mental health, general support and assistance, as well as for information on gender and transition:
Feeling suicidal and anxious, wanting help understanding and validating my gender identity.
I was confused and afraid and suicidal.
The level of satisfaction with psychiatric services was varied. Many participants had positive experiences and largely felt the service was respectful or mostly respectful of their gender identity (64%). The main themes emerging from these encounters were around the psychiatrist generally being very supportive of the young person’s gender and being respectful:
She was very welcoming, very open and immediately used the correct name and pronouns for myself, so it was easier and more relaxing to talk to her.
Very friendly and open space, non-judgemental staff, understanding and competent clinician, understood my needs and followed the guidelines appropriately.
Other positive experiences included feeling that the psychiatrist was truly helping the young person to explore their gender and jointly discussing and the deciding the next steps they wanted. Others reported positive aspects of psychiatric appointments included receiving a letter of support for further transition. He made sure I wasn’t jumping in too fast, as well as helping me find what direction to go next.
Furthermore, psychiatrists assisted young people with a range of other mental health difficulties they were experiencing, including depression, gender dysphoria and anxiety. There was, however, considerable evidence of ambivalence and outright dissatisfaction with psychiatrists, and many participants elaborated on these experiences. Gatekeeping of hormonal and other types of medical intervention was a common issue faced by participants. Psychiatrists were, in effect, viewed as the arbiters of whether or not the young person would be allowed to transition. Psychiatrists were seen as providing
Access to letters that allowed me to change my gender marker on university documentation, as well as referrals to other specialists.
This gatekeeping role of providing access was seen by young people in a negative light, whereby the young person lost autonomy over their own body. Young people reported feeling that psychiatrists restricted them from accessing medical interventions. Many perceived that psychiatrists acted in an uncompromising and even patronising manner:
The psychiatrist I visited was extremely arrogant and condescending and had a very strong ‘gatekeeper’ approach to trans healthcare. I felt like I had to prove that I was ‘really trans’ (whatever the heck that means), despite living full time as female and having been on feminising hormone therapy for over a year at that point. I strongly objected to this kind of treatment, since it started from the assumption that I was somehow lying or deluded about my gender.
Some participants, especially those who identified as non-binary, felt they had to hide their true gender identity in order to obtain the support and help they were seeking:
I lied and said I was a binary trans man to gain access to the services I needed. The psych was very focused on gender norms and binary identities, and I felt judged and ‘not trans enough’ because some of my hobbies are traditionally ‘feminine’ things.
Other participants shared experiences of being misgendered by psychiatrists, called by the wrong name and felt their clinicians did not have adequate knowledge on gender diversity. This left participants feeling as if their gender was not being taken seriously or that they were unable to be open with their clinician about any issues they were having. Others faced invasive questions and comments from their psychiatrist (e.g. around sexual behaviours and desires, and outdated ideas of gender). Often – other than obtaining a letter in support of transition – a number of participants felt that their appointment with the psychiatrist was ‘wasted time’.
Among the negative experiences of psychiatric care, one of the most commonly reported themes related to the cost of treatment compounding other concerns with the clinical interaction:
I found the experience [of psychiatric care] awful. I left crying on many appointments. It was also expensive, and my parents pushed for me to see this guy because he was ‘the best’ in [capital city of the state]. I found him very rude and dismissive of my identity and pronouns . . . He told my parents that non-binary genders aren’t real.
For many study participants, cost was seen as an issue regardless of their perceptions of the appointment. Even if the participant expressed satisfaction with their appointment, cost concerns marred the experience, especially as many participants had waited significant amounts of time to be reviewed by a TGD-friendly psychiatrist.
Mental health inpatient services
The majority of participants accessing mental health inpatient services were below the age of 18 years (56.4% vs 36.4% for 18 years or older). An additional 7.3% stated they were unable to access the service despite trying to. Most participants were admitted within their first few access attempts: 41.2% were admitted on their first access attempt and 39.2% within 2–4 times of trying to access the service. The experience within mental health inpatient services was largely considered to be unsatisfactory (43.7% rated their experience as very or somewhat unsatisfactory, while only 20% rated the experience as moderately or highly satisfactory), and 39.6% found the service to be not respectful or mostly not respectful of their gender identity.
The reasons for accessing mental health inpatient services were varied, with most relating to self-harm, suicidal thoughts or attempts, eating disorders, depression and anxiety. A smaller number of participants specified other reasons, including sexual assault, anger issues and being a risk to others. Some participants attributed their admission to gender dysphoria or other mental health issues related to their gender. These were not mutually exclusive categories, given that many participants had either accessed the service multiple times or attributed the reason for access to multiple categories.
Experiences within inpatient services were very mixed, with participants frequently reporting high levels of dissatisfaction and noting that their gender was not respected. This invalidation of identity was viewed as harmful for the individual’s recovery process:
My chosen name and pronouns were mostly ignored by staff which was extremely unhelpful to my short-term recovery.
Participants also reflected that, although some staff in the service respected their identity through use of the correct name and pronouns, other staff in the same environment did not behave as respectfully (either intentionally or inadvertently). Negative clinical experiences included experiencing transphobia, and comments and actions that were not affirmative of diverse genders:
While during the one stay in a public hospital I was under the care of a transphobic psychiatrist who said I was delusional and that everyone regrets transitioning.
Others reported that the services were generally unable to help them, made them feel worse, ‘shuffled’ them to other services and were unable to ensure long-term safety:
There was not much help in relation to counselling or long terms plans that they could give me. It was useful for keeping me safe in the short term, but there seemed to be no specific help or information they could give me. I was told to go to the [LGBTIQA+ community service] to help with gender stuff.
The few positive comments about experiences within inpatient services were that safety was maintained in the short-term, and that other young people who had also been admitted to the services were respectful of their gender identity.
Discussion
These results demonstrate that TGD young people in this study sought mental health support for a variety of reasons, but in many cases reported that they did not receive optimal care. Although a number of mental health professionals provided care that was inclusive of gender diversity, the responses presented here highlight how many mental health service providers in Australia are undertrained to treat TGD clients in an affirmative manner. Overall, therapy and counselling services were mostly supportive of TGD young people, but there were many other interactions described that highlight the need for more education in gender diversity for professionals working in the field. Considering how frequently TGD young people experience mental health difficulties (with 79.7% of TGD young people in Australia having self-harmed and 48.1% having attempted suicide; Strauss et al., 2020a), the service gaps have serious implications. While the reasons behind negative clinical experiences are multi-factorial (i.e. a young person may recall an interaction in a negative light because of persisting severe mental health difficulties), the commentary from participants reflects clinical care that is not inclusive of gender diversity.
Some participants reported experiencing long waiting periods for clinical review or difficulties locating a professional with experience in gender diversity. A previous Canadian study has highlighted that lengthy waiting times contributed to adverse mental health impacts among TGD young people (Rotondi et al., 2013). It is also notable that a significant number of participants were older than 18 years when they were accessing some services. This pattern could imply that participants may have been waiting until they were of an older age before initiating treatment, and therefore may have been doing so without parental support or knowledge.
Previous research in Australia has highlighted issues relating to staff inexperience with TGD health (Hyde et al., 2014). This is likely a reflection of the individual’s lack of education in the area (Dickey and Singh, 2017). Even mental health professionals who view themselves as competent in TGD health may sometimes use inappropriate language (Whitman and Han, 2017). TGD young people who are experiencing psychological distress or are reaching out for help need to be able to access support from professionals who are knowledgeable about gender diversity. To provide truly affirmative care, professionals should be accepting and welcoming of the very core of the young person’s identity.
In addition to being knowledgeable about gender diversity, mental health professionals should also be aware of the high rates of mental health difficulties, self-harm and suicidality commonly experienced by TGD young people and the clinical complexity associated with these elevated rates (Bradlow et al., 2017; Strauss et al., 2020a). Professionals should also recognise that many TGD young people are exposed to negative life experiences, including trauma, discrimination and a lack of family support (Strauss et al., 2020b), which can have significant effects on their mental health, including affecting developmental milestones through adolescence to early adulthood (Dickey et al., 2017).
A common theme emerging from these findings was that mental health care providers were seen as gatekeepers to accessing hormonal treatments, especially psychiatrists. Previous research indicates that establishing an authentic and honest relationship with TGD clients is made challenging for professionals because of the gatekeeping role they play (Ellis et al., 2015). A recent study with trans people in the United Kingdom found that 30.9% of participants had withheld information from, or lied to, health practitioners because of concerns about disclosing information that could impede access to medical treatment (Ellis et al., 2015). Participants in this study also reported feeling pressure to conform to outdated, cisnormative notions of gender from mental health professionals.
The debate surrounding whether there should be a psychiatric diagnosis for gender diverse individuals (i.e. gender dysphoria or gender incongruence) becomes even more complex when considering how health systems operate and who pays for medical care. For the costs of medical care to be fully or partially covered by health insurers, a formal diagnosis is usually required. Participant dissatisfaction with psychiatric services often relates to this requirement for formal diagnostic ‘confirmation’ by a psychiatrist to begin gender-affirming medical intervention. TGD young people commonly experience this process as pathologising, prohibitive and acting to undermine their autonomy over their own body and lives.
A number of recommendations for improving the mental health care of TGD young people are suggested by this research. It is evident that obtaining an appointment with a professional appropriate for the needs of the individual was a difficult process for many study participants. Referral processes for TGD young people to connect them to professionals with gender-expertise need to be streamlined to provide timely support. Increasing the number of specialised gender clinics and training programmes for existing services would help to decrease wait times. Advocacy, policy development and expansion of professional training programmes would reduce the negative experiences faced by TGD young people, including misgendering and discrimination (Acevedo-Polakovich et al., 2013; Riggs et al., 2014).
There is evidence that professionals who have received specific training on working with TGD clients exhibit more positive attitudes, and – when combined with experience – demonstrate a higher level of clinical competency (Riggs and Bartholomaeus, 2016). More generally, mental health providers can also overcome these barriers through using the correct name and pronouns for a client, even if this name is not recognised on legal documents, including the provision of using both sex assigned at birth and gender (Dolan et al., 2020; Samuels et al., 2018; Vance and Mesheriakova, 2017). Having inclusive clinical forms also helps ensure that all staff at the service, including reception and other auxiliary staff, are aware of the appropriate terminology to use when addressing the client to validate the young person’s identity.
Limitations
All self-report survey data have inherent limitations because of its reliance on accurate reporting from respondents that is difficult to validate when using an anonymous online approach to recruitment. In addition, the cross-sectional nature of this study only captured data at a single timepoint in the individual’s often complex personal and clinical journey. This research may not be representative of all TGD young people and their experiences within clinical settings. In addition, in our study, there were more participants assigned female at birth compared to those assigned male at birth. Finally, the scope of the health and related services reviewed in the current study was limited.
Conclusion
These findings indicate the need for improved service provision through various strategies, including addressing affordability of ongoing mental health support, enhancing levels of professional awareness and understanding of gender diversity, and the removal of barriers to existing service and referral pathways. Further research should evaluate the knowledge that mental health professionals have in relation to TGD physical and mental health and examine ways in which training could be provided to maximise knowledge uptake. Improving the mental health care provided for TGD young people in Australia will help to minimise distress and address the high rates of mental ill-health in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PS was supported by an Australian Government Research Training Program Scholarship at the University of Western Australia at the time of writing this manuscript. AL is supported by an NHMRC Career Development Fellowship [#1148793]. ZW is supported by an Australian Government Research Training Program Scholarship at the University of Western Australia.