
Abstract
Background:
Many refugees experience bereavement, and as a result they suffer elevated rates of prolonged grief disorder. Evidence also indicates that elevated rates of psychological disturbance in refugee children can be associated with parental mental health. This study examined the extent to which prolonged grief disorder in refugees is associated with their parenting behaviour and in turn with their children’s mental health.
Methods:
This study recruited participants from the Building a New Life in Australia prospective cohort study of refugees admitted to Australia between October 2013 and February 2014. The current data were collected in 2015–2016 and comprised 1799 adults, as well as 411 children of the adult respondents. Adult refugees were assessed for trauma history, post-migration difficulties, harsh and warm parenting, probable prolonged grief disorder and posttraumatic stress disorder. Children were administered the Strengths and Difficulties Questionnaire. The current analyses on bereaved refugees comprise 110 caregivers and 178 children.
Results:
In this cohort, 37% of bereaved refugees reported probable prolonged grief disorder. Path analysis indicated that caregivers’ grief was directly associated with children’s emotional difficulties. Caregiver warmth was associated with reduced emotional problems in children of refugees with minimal grief but associated with more emotional problems in caregivers with more severe grief. More harsh parenting was associated with children’s conduct problems, and this was more evident in those with less severe grief.
Conclusion:
Severity of prolonged grief disorder is directly linked to refugee children’s mental health. The association between parenting style, grief severity and children’s mental health highlights that managing grief reactions in refugees can benefit both refugees and their children.
The surge of refugees worldwide has drawn renewed attention to the mental health plight of those who flee persecution. Refugees are at elevated risk of a range of mental disorders, including posttraumatic stress disorder (PTSD), depression and anxiety (Charlson et al., 2019). One of the major stressors facing refugees is the loss of loved ones. Bereavement can be a common event for refugees because they and their loved ones can be exposed to life-threatening experiences. One study found that 56% of West Papuan refugees reported traumatic losses, including witnessing murders, violent death of loved ones and disappearance of family members (Tay et al., 2016).
Despite the susceptibility of refugees to bereavement, there has been a surprising lack of focused study of problematic grief in this population. The conceptualization of problematic grief has been recently recognized in International Classification of Diseases, 11th Revision (ICD-11), which has proposed prolonged grief disorder (PGD) as a new diagnostic construct (Maercker et al., 2013). This diagnosis is defined as persistent yearning for the deceased together with associated emotional pain, difficulty in accepting the death, a sense of meaninglessness, bitterness about the death and difficulty in engaging in new activities (World Health Organization, 2018). According to this definition, PGD can only be recognized if the symptoms persist at least 6 months after the death. One meta-analysis indicates that prevalence of PGD in bereaved samples is 9.8% (Lundorff et al., 2017). This highlights that PGD is a significant public health issue because it leads to a range of adverse psychological, medical and functional difficulties (Prigerson et al., 2009). Rates of probable PGD in refugees have varied between 8% and 54% (Craig et al., 2008; Schaal et al., 2010). This marked disparity of PGD incidence may reflect differences in the nature of conflict exposure and occurrence of loss but may also reflect instability in prevalence rates associated with small and non-representative samples. A recent systematic review noted that the pooled prevalence of PGD in refugees was 33.2% (Kokou-Kpolou et al., 2020).
This study aimed to investigate the contributors and consequences of PGD in a nationally representative sample of refugees. A particular focus of this study was the extent to which PGD symptoms may impact the mental health of affected refugees’ children. There is evidence that parental and child mental health is associated (Lambert et al., 2014), a finding that is replicated across number of studies of refugees (Montgomery and Foldspang, 2006; Rousseau et al., 1998). There is also evidence that parental bereavement is association with poorer mental health in their children (Hamdan et al., 2012). In terms of bereavement, the association between parental and childhood mental health appears to be moderated by the level of parenting stability following the bereavement (Brent et al., 2012); specifically, adverse impacts of bereavement on child mental health are reduced by warm and structured parenting (Luecken et al., 2009). Numerous studies from non-refugee populations indicate that parental emotional difficulties adversely impacts parenting behaviour, which in turn negatively impacts children’s psychological health (Crosby et al., 2013; McLeod et al., 2007). Relevant to refugee populations is evidence that being the victim of interpersonal trauma can promote harsh parenting, which can adversely impact children’s mental health (Field et al., 2013). In terms of refugees, there is evidence that poor parental psychological functioning is associated with greater anger towards children (Hinton et al., 2009), that the cohesion of the family unit influences children’s mental health (Thabet et al., 2009) and that parental PTSD levels increase harsh parenting behaviour, which in turn is associated with children’s psychological difficulties (Bryant et al., 2018).
No studies to date have investigated how parental grief may impact on children’s mental health in a refugee population. This study indexed potential predictors of PGD in refugees, including exposure to traumatic events and level of post-migration difficulties because mental health in refugees has been strongly linked to trauma exposure and post-migration stressors (Porter and Haslam, 2005). We also assessed the association between PGD and parenting behaviour, and the interactive effect between caregiver mental health and parenting behaviour on children’s mental health. We hypothesized that PGD would result in increased harsh parenting and decreased warm parenting, which would be linked to poorer mental health of refugee children.
Method
Participants
Refugee participants in this study were embedded in the Building a New Life in Australia (BNLA) study, which was undertaken by the Australian Government (Edwards et al., 2018). The BNLA is a longitudinal population-based cohort study of refugees who were recruited on the basis of being granted permanent humanitarian visa status. The first wave of data was collected between October 2013 and February 2014. Subsequent waves were conducted annually, with Wave 3 data being collected between October 2015 and February 2016. Data analysed in this study were taken from Waves 1 and 2. BNLA participants were recruited from 11 sites across Australian major cities and regional areas to reflect concentrations of refugees across visa classes.
The BNLA eligibility criteria comprised being the principal or secondary applicant (i.e. the refugee applicant within a family unit) for a humanitarian visa awarded between May 2013 and December 2013) and being at least 18 years old. Following principal applicants consenting to participate, secondary applicants were invited to participate in the BNLA study if they were residing with the principal applicant. In contrast to previous waves, the Wave 3 data also included assessment of participants’ PGD and also assessment of participants’ children. The primary caregiver (PC) was invited to complete a child module with respect to up to two children in their care; if there were more than two eligible children in a household, two children were randomly selected. Two principles were applied to sampling children (1) up to two children from each family could participate and (2) older children (aged between 11 and 17 years) were preferentially selected over younger children because the former were able to provide self-report responses in addition to parental reports. Specifically, two youth aged 11–17 years old in each migrating unit were randomly selected. When there were two or more children aged 11–17 years old, two randomly selected children in this age group were selected. Where there were only children aged 5–10 years old in the migrating unit, up to two children aged 5–10 years old per household were randomly selected. The current child data focuses on the child self-reports because this allows for independent assessment of children’s mental health that is not confounded by parental appraisals of their children.
Interviews were conducted using computer-assisted personal interview (CAPI) and computer-assisted self-interview (CASI). In the CAPI, field interviewers asked questions and entered responses directly into a computer. In the CASI, participants responded privately to self-report questions using a computer interface (with assistance provided when needed). Interview materials were translated from English into nine languages including Arabic, Burmese, Dari, Hazaragi, Persian, Chin Haka, Nepali, Swahili and Tamil. Participants were typically matched with an interviewer who was a native speaker of their respective language, although some participants opted for translated/interpreted interviews. The Wave 3 data was collected after a residency period of 2–3 years in Australia (for 87% of the sample). In an addition to questions asked in the previous waves, Wave 3 included an assessment of bereavement and probable PGD. At Wave 3, there were 1843 adult (aged 18 years or more) refugees interviewed, and of whom 424 PCs potentially provided mental health data relevant to these analyses on 692 children.
Measures
Demographic interview
An array of demographic, household and re-settlement factors were assessed.
PGD
Questions related to grief were asked of all bereaved primary applicants (one per migration unit or ‘family’) and, if the primary applicant was not the PC, they were asked of the PC as well. Initially, to index bereavement, respondents were asked if someone close to them had died. The descriptor of the deceased as ‘someone close to you’ was adopted because it is consistent with the terminology used in the ICD-11 PGD criteria. In the case of an affirmative response, they were then administered the PGD measure. If they responded negatively, this measure was not administered. To assess probable PGD, a screening measure for PGD was used. This measure has previously been employed with individuals affected by Hurricane Katrina (Shear et al., 2011). Four questions were asked about grief in the past 30 days: (1) How often have you found yourself or yearning for the people who died? (2) Have you had trouble accepting the death? (3) Do you feel bitter over their death? (4) Do you feel that life is unfulfilling, empty or meaningless since their death? Each response was answered on a 5-point scale (1 = not at all, 5 = Several times a day/Overwhelmingly). To strengthen the case that we were indexing PGD, a final question asked whether the yearning for deceased had persisted for at least 6 months. Probable PGD was defined to be consistent with the ICD-11 definition of PGD criteria, comprising the presence of yearning for the deceased at least every day, and at least two of the three other potential PGD symptoms being endorsed at least at moderate levels. Furthermore, yearning had to persist for at least 6 months.
Posttraumatic Stress Disorder – 8
The Posttraumatic Stress Disorder – 8 (PTSD-8) (Hansen et al., 2010) is an 8-item self-report screening measure for probable PTSD that is derived from the Harvard Trauma Questionnaire (Mollica et al., 1992). The PTSD-8 assesses four intrusion, two avoidance and two hypervigilance items. Participants rate how much each symptom bothered them in the past week symptoms on a 4-point Likert-type scale (1 = not at all, 4 = most of the time). Probable diagnosis of DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th ed.) PTSD is met if at least one symptom from each of the three PTSD-8 subscales has an item score of 3 or 4 (Hansen et al., 2010). This measure was administered to adult respondents at all three waves and had an internal consistency (Cronbach’s alpha) of 0.91–0.92 across waves.
Trauma exposure
To assess the extent of exposure to traumatic events at Wave 3, caregivers completed a modified version of the Harvard Trauma Questionnaire Trauma Events Module (Mollica et al., 1992) that indexed 10 potentially traumatic events that are relevant to refugee experience (e.g. combat exposure, imprisonment, murder/disappearance of family members) and has been widely used with refugee populations (Hollifield et al., 2002); the number of events experienced were summed to provide a total score.
Post-migration stressors
To assess post-migration stressors commonly experienced by refugees, respondents were asked to dichotomously indicate if any of 10 current life events caused them stress; events included work, housing, finances, family safety, discrimination, school/study, caring for family, conflict with neighbours, language barriers or acculturation; the number of events experienced was summed to provide a total score.
Parenting style
To index parenting style, caregivers were assessed for warm and harsh parenting styles derived from questionnaires employed in the Longitudinal Study of Australian Children (Zubrick et al., 2014). The warm parenting scale comprised five items derived from Child Rearing Questionnaire (Paterson and Sanson, 1999) and assessed parental displays of affection and awareness of the child’s needs. The harsh parenting scale comprised five items derived from the Early Childhood Longitudinal Study of Children (Department of Education, 2001) and included items indexing negativity, physical discipline and rigid enforcement of rules. These constructs were employed as they can differentially moderate childhood mental health (Bayer et al., 2006). The internal consistencies of the warmth and hostility scales in this study are 0.73 and 0.74, respectively.
Strengths and Difficulties Questionnaire
The Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001) was used to assess children’s psychological problems. The SDQ comprises 25 items that index behavioural, emotional and social problems that children can report on a 3-point Likert-type scale (0 = not true, 2 = certainly true). The SDQ comprises five subscales encompassing conduct problems, hyperactivity, emotional symptoms, peer problems and prosocial behaviour (this study focuses on the four difficulties subscales). We summed all items (except the prosocial items) were summed to establish a total difficulties score (range: 0–40). The SDQ possesses good internal consistency for screening child psychiatric disorders (Goodman, 2001) and is commonly used among refugee youth where it has comparable factor structures across ethnic groups (Richter et al., 2011).
Data analysis
The descriptive statistics of the participants included in the model use unweighted data because of recommendations that this weighted data is not indicated in causal models (Solon et al., 2015). The association between PGD and childhood mental health was tested in a path analysis using the independent variables outlined above with child SDQ scales scores, both those reported by the PC as the outcome measure. The model examined the potential influence of PGD severity on parenting behaviour and each of the four domains of child mental health problems. The path model acknowledged the longitudinal sequence of the measurements, and the path model was defined so that within waves paths reflected the implied temporal order (e.g. pre-arrival trauma preceded other Wave 1 variables); the causal order favoured in the literature (e.g. post-migration stressors affect PTSD at the same wave, though potentially in either direction longitudinally); or that of the primary hypothesis, namely that SDQ was the endpoint (thus, for example, SDQ was not allowed to ‘cause’ harsh parenting). In addition, all models included the following covariates to consider the potential differential pathways of gender and age of the child: (1) PC post-migration difficulties were regressed on the respondent’s age and gender and (2) the parenting and SDQ variables were regressed on the child’s age and gender. Always including age and gender as covariates ensured a consistent sample as there were no cases with a missing value on an x-variable (an x-variable is a variable not regressed on any other variable: cases with missing values on these variables are always excluded from a model). Furthermore, to index the extent to which parenting interacted with caregivers’ grief to influence children’s mental health, we included two interaction variables: PC grief with harsh and warm parenting (calculated using centred variables). Within this framework, a sequence of models was fitted, with paths identified either from theory or via modification indices. A series of models was fitted: after each model fit, non-significant paths (with significance based on a p-value ⩽ 0.05 for the non-standardized coefficient) were removed (except for the covariates noted above, and lower-order variables when the interaction was significant), and then the model re-fitted; a final model reported is restricted to significant paths (as well as covariates). We specifically did not allow residuals to correlate, first as doing so produced implausible indices of model fit, and second to minimize potentially inflating the apparent fit of the path component. In models of this kind, the possibility of different models by gender (of either child or caregiver) arises.
As a number of PCs provided reports on two children, the data were analysed with the family identified as the clustering unit. The survey weights were not used as we were using a specific subset of respondents and therefore less applicable. All analyses were conducted using Mplus Version 824. Figures exploring interaction terms are based on estimates obtained from equations defined using the MODEL CONSTRAINT and PLOT options in Mplus.
Results
Participant characteristics
Within those migration units that provided child data the bereavement question was asked of all caregivers, and answered by 97.6%, equally so by females and males (Table 1). Of those, 42.8% (n = 177) reported the death of someone close, and of these 65.5% (n = 116) reported the death as being more than 6 months ago (in females 62.9% [n = 83/132] and in males 73.3% [n = 33/45]; χ2 = 1.62, p = 0.20), making them eligible for this study. In the model reported below, missing data for variables reduced the sample to 110 PCs (94.8%) with associated data on 178 children. Three quarters of respondents reported being married or having a partner (71.8%, 79/110), with proportionally far fewer females (62.0%, 49/79) than males (96.8%, 30/31) so reporting (χ2 = 13.28, p < 0.001). Regarding country of origin, the majority of these participants came from Iraq or Afghanistan (93, 84.5%); and the remainder chiefly from Bhutan or Myanmar (6, 5.5%), Iran (5, 4.5%) and Sub-Saharan Africa (5, 4.5%). Calculating the rate of probably PGD was based on 106 caregivers because there was a missing variable for four participants, which precluded determining PGD. Basing probable PGD on ICD-11 criteria (where available), 36.8% (39/106) satisfied criteria for probable PGD (in females 42.7% [32/75] and in males 22.6% [7/31]; χ2 = 3.81, p = 0.051).
Participant characteristics.
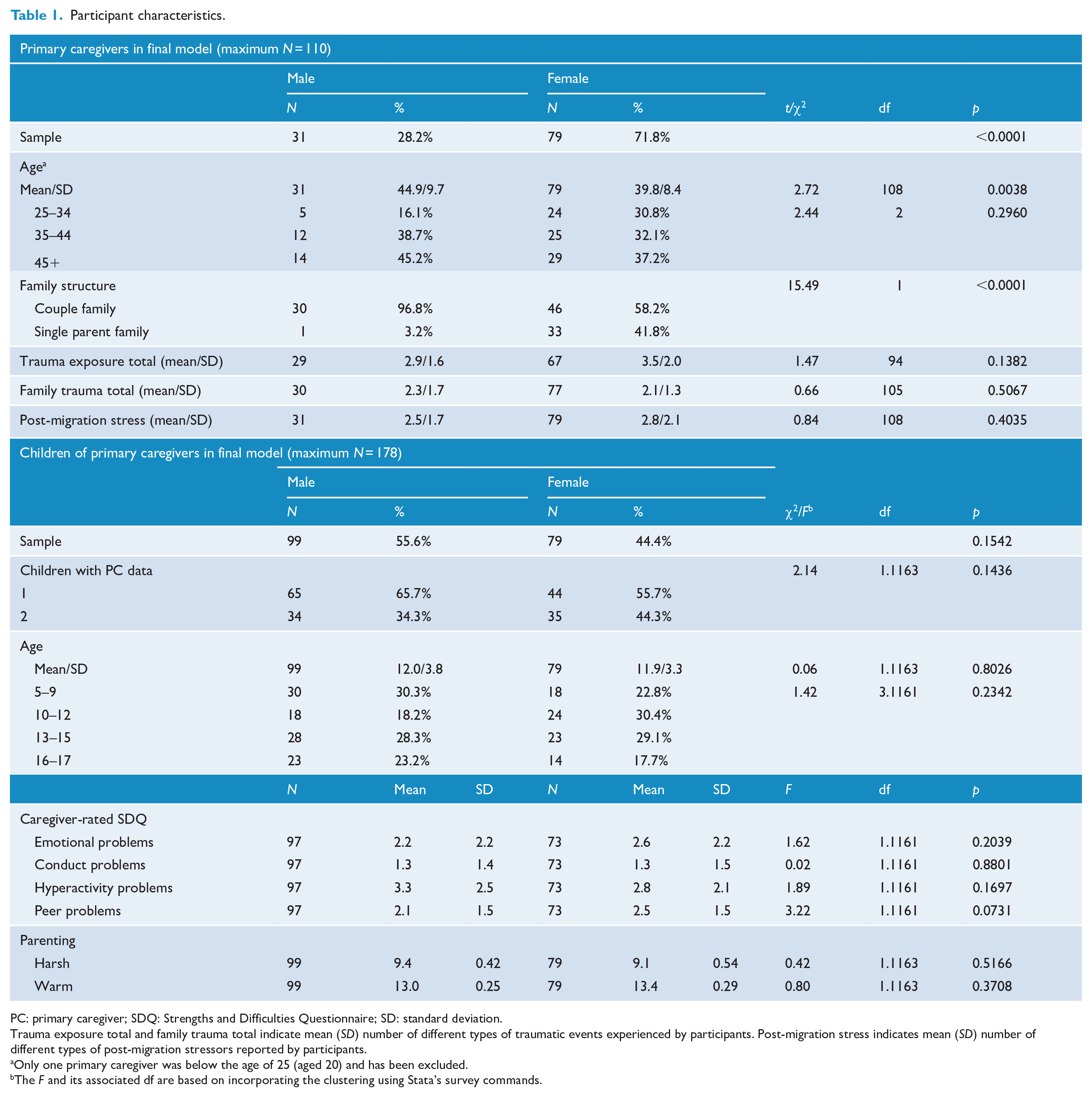
PC: primary caregiver; SDQ: Strengths and Difficulties Questionnaire; SD: standard deviation.
Trauma exposure total and family trauma total indicate mean (SD) number of different types of traumatic events experienced by participants. Post-migration stress indicates mean (SD) number of different types of post-migration stressors reported by participants.
Only one primary caregiver was below the age of 25 (aged 20) and has been excluded.
The F and its associated df are based on incorporating the clustering using Stata’s survey commands.
Path analysis of prolonged grief and children’s mental health
Path model
Figure 1 depicts the model displaying (1) standardized estimates for all direct paths where the unstandardized path was significant (Table 2); 1 and (2) non-significant paths from age and gender, or related to interactions, that were retained in the model. The model yielded an adequate fit (χ2 [44] = 63.7, p = 0.0273, comparative fit index [CFI] = 0.863, Tucker–Lewis index [TLI] = 0.764, root mean square error of approximation [RMSEA] = 0.050, 90% confidence interval [CI]: [0.017, 0.076]).
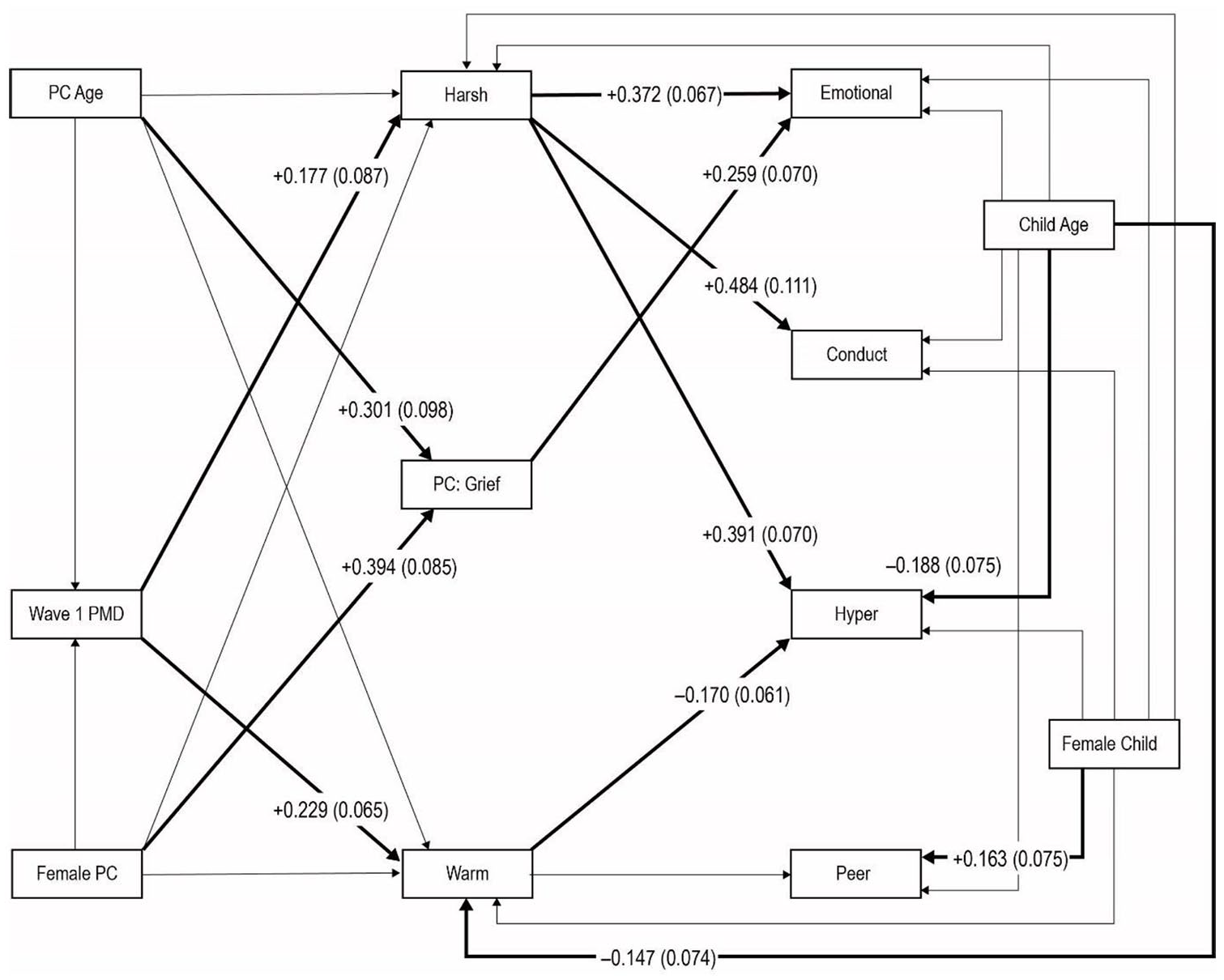
Path diagram for relationships trauma history, post-migration difficulties, prolonged grief, parenting, and caregiver-reported Strengths and Difficulties Questionnaire.
Estimates from path model for primary caregiver-rated SDQ.
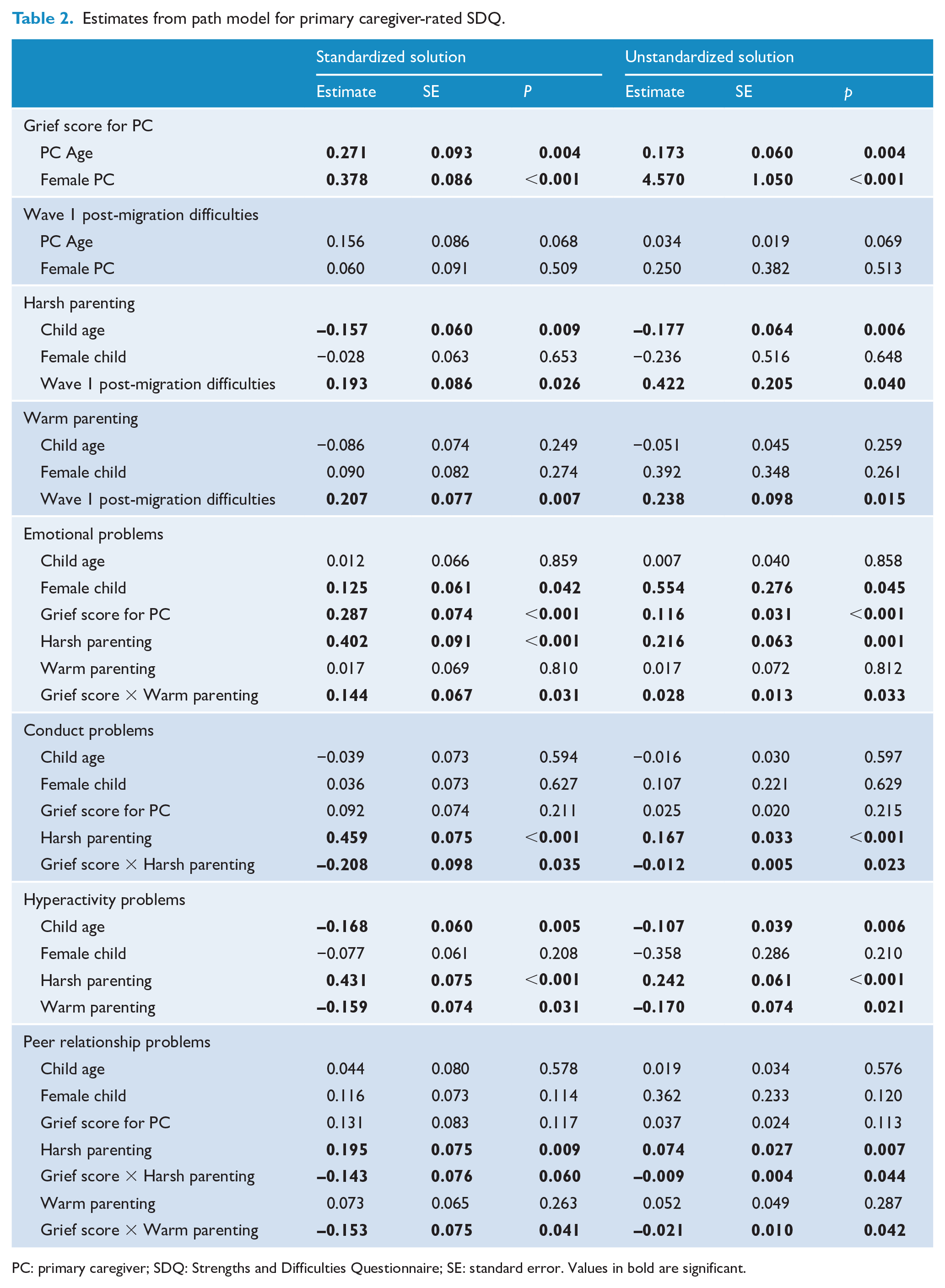
PC: primary caregiver; SDQ: Strengths and Difficulties Questionnaire; SE: standard error. Values in bold are significant.
There was a direct significant path from PGD severity to childhood emotional difficulties (β = 0.287 [B = 0.116, p < 0.001]; we report standardized estimates for interpretability, followed by unstandardized estimates and their p values). There were significant paths from female adult gender and older age to PGD severity, and there were significant indirect paths to emotional difficulties: from age (β = 0.078 [B = 0.020, p = 0.019]) and from female gender (β = 0.108 [B = 0.531, p = 0.008]). It is worth noting that the paths from PGD to the other SDQ scores, if included, are clearly non-significant (for conduct p = 0.215, for hyperactivity p = 0.659 and for peer relationships p = 0.113).
There were significant paths from harsh parenting to emotional problems (β = 0.402 [B = 0.216, p = 0.001]), conduct problems (β = 0.459 [B = 0.167, p < 0.001]), hyperactivity (β = 0.431 [B = 0.242, p < 0.001]) and peer relationship problems (β = 0.195 [B = 0.074, p = 0.007]). As harsh parenting was affected by post-migration difficulties at Wave 1 (β = 0.193 [B = 0.422, p = 0.040]), there was an effect of the latter via harsh parenting on emotional difficulties (β = 0.078, [B = 0.091, p = 0.018]), conduct problems (β = 0.088 [B = 0.070, p = 0.020]), hyperactivity problems (β = 0.083 [B = 0.102, p = 0.015]) and peer relationship problems (β = 0.038 [Β = 0.031, p = 0.038]). Warm parenting affected hyperactivity problems (β = –0.170 [B = –0.170, p = 0.021]), but not the indirect path from post-migration difficulties via the latter (p = 0.132).
Importantly, PGD severity and parenting also had effects via interaction terms: PGD × harsh parenting on conduct problems (β = –0.208 [B = –0.012, p = 0.023]) and peer relationship problems (β = –0.143 [B = –0.009, p = 0.044]); and PGD × warm parenting on emotional problems (β = 0.144 [B = 0.028, p = 0.033]) and peer relationship problems (β = –0.153 [B = –0.021, p = 0.042]).
To facilitate the interpretation of significant interaction terms, we have graphed aspects of these effects in Supplemental Figures S1–S3. Supplemental Figure S1 shows the relationship between caregiver-reported harsh parenting and child conduct problems, in the presence of a caregiver grief × harsh parenting interaction effect on conduct problems. The relationship is shown – separately for male and female children, though the difference is non-significant – at three levels of grief corresponding to the 20th, 50th and 80th percentiles. The figure shows that increasingly harsh parenting leads to an increasing level of conduct problems, with this increase strongest for those reporting the least grief.
Supplemental Figure S2 shows the relationship between caregiver-reported harsh parenting and child peer relationship problems, in the presence of two interaction effects on the child’s problems: caregiver grief × harsh parenting and caregiver grief × warm parenting. The relationship is shown – separately for male and female children, the difference is significant – at the three levels of grief (as warm parenting is in the model, this variable has been held constant at its 50th percentile). Similar to the previous figure, problems increase with increasingly harsh parenting, and the increase is most marked for those with little or no grief.
Supplemental Figure S3 shows the relationship between caregiver-reported harsh parenting and child emotional problems, in the presence of a caregiver grief × warm parenting interaction effect on the child’s problems. The relationship is shown – separately for male and female children, the difference is significant – at the three levels of grief (as harsh parenting is in the model, and significant, this variable has been held constant at its 50th percentile). The figure shows that increasingly warm parenting leads to a decreasing level of emotional problems for caregivers with little or no grief, but an increasing level of emotional problems in children when caregivers have the highest levels of grief.
Discussion
Approximately one-third of refugees who experienced bereavement reported that they suffered probable PGD. Notably, this is higher than the rate of PGD in bereaved people reported in a recent meta-analytic study of non-refugee populations, in which the incidence of PGD was 9.8% (Lundorff et al., 2017). Considering this sample was drawn from a large nationally representative cohort of resettled refugees, this suggests that PGD is a significant mental health issue in refugee populations and is more prevalent than in many other bereaved samples. The rate of probable PGD in this sample accords with a previous systematic review that reported that 33.3% of bereaved refugees experience PGD (Kokou-Kpolou et al., 2020).
The focus of this study was the potential relationship between parental PGD and children’s psychological well-being. The direct path from PGD severity to childhood emotional difficulties may be attributed to the adverse effects of persistent grief on the mood of caregivers, modelling of maladaptive patterns of behaviour, social withdrawal or a focus on the deceased to the extent that the caregiver cannot function adequately within the family unit. It is also possible that PGD severity may involve other factors or behaviours that could result in poorer psychological functioning in children. PGD has been associated with substance abuse, cognitive disturbances, sleep impairment and functional difficulties, which may negatively impact the child’s mental health (Shear, 2015).
There was evidence of interaction effects between parental grief and parenting behaviour on childhood mental health. For example, more harsh parenting was associated with children’s conduct problems, and this was most apparent in caregivers with less severe grief. The finding of a relationship between harsh parenting and children’s conduct problem accords with prior research that this form of parental behaviour tends to exacerbate externalizing problems in children (MacKenzie et al., 2015). The observation that this relationship was less apparent in those with more severe grief appears counter-intuitive because prior studies have found that psychological difficulties can negatively affect refugee parenting, which in turn adversely impacts children’s mental health (Bryant et al., 2018; Gruhn et al., 2016; McLeod et al., 2007). It is possible that more severe grief tempers the impact of harsh parenting on conduct disorders because it promotes the need for greater attachment to others, including family members, which may result in the effects of harsh parenting being mitigated by more attentive behaviour towards children. Although speculative, this interpretation is consistent with prevailing models of PGD that posit that grief activates one’s need for attachment figures (Shear et al., 2007).
An interesting pattern emerged regarding warm parenting insofar as it predictably was associated with reduced emotional problems in children of caregivers with minimal grief, but associated with more emotional problems when the caregiver had more severe grief. Much evidence attests to the positive impact of warm parenting on children’s emotion well-being (Morris et al., 2007). It is possible that in the context of more severe grief reactions the nature of warm parenting may have adverse consequences on the child’s mental health because warm parenting may involve overprotective behaviours that can increase a child’s anxiety (Bayer et al., 2011). Alternately, PGD is known to be strongly associated with adult separation disorder (Pini et al., 2012), and there is considerable evidence of the impact of maternal anxiety on parenting behaviour and children’s emotional problems (Drake and Ginsburg, 2011; Stevenson-Hinde et al., 2011); it is possible that more severe grief leads caregivers to be anxious about their relationships with others, leading to excessively dependent behaviours that can promote emotional difficulties in children.
Harsh parenting was associated with children’s emotional difficulties, hyperactivity and conduct problems, and warm parenting was associated with reduced hyperactivity. This accords with much evidence that negative parenting practices, including hostile expression and excessive discipline, can lead to a range of psychological difficulties in children (Wiggins et al., 2015). Furthermore, the finding that children’s younger age was associated with greater hyperactivity is consistent with evidence that hyperactivity reduces as children develop (Larsson et al., 2011). The finding that female gender was associated with more severe peer problems is surprising in the context of evidence of normative data indicating that boys have more difficulties in this domain (Tobia and Marzocchi, 2018). Most of this evidence comes from studies of non-refugee populations, and so it is possible that acculturation and related issues may contribute to refugee girls having greater difficulties in peer functioning than their male counterparts. The observation that warm parenting was associated with younger age of the child is somewhat unexpected and may be interpreted as reflecting caregivers’ greater warmth to younger children because of the perceived need to care for the needs of younger children as they acclimatize to their new environments.
It is worth noting that there was a path from post-migration difficulties at Wave 1 and harsh parenting, which had an effect on children’s emotional difficulties, conduct problems, hyperactivity and peer relationship problems. There is a robust literature on the adverse effects of post-migration difficulties on refugees (Heptinstall et al., 2004; Porter and Haslam, 2005; Ziaian et al., 2012), which supports models of refugee adjustment that emphasize the critical contribution that ongoing stressors in the host country can play in refugees’ mental health (Miller and Rasmussen, 2010). These daily stressors, which can include financial, housing, employment, acculturation and discrimination challenges, may impact on refugees adopting harsher parenting behaviours, which are known to adversely affect children’s psychological health (Bayer et al., 2006).
These observations are qualified by several methodological limitations. First, probable PGD was assessed with an abridged measure of PGD; although our measure complies with the ICD-11 definition of PGD, greater confidence in the observed rates of probable PGD would be achieved with a fuller measure of PGD. Relatedly, we recognize that cultural variations exist in the conceptualization of prolonged grief, and our measure may not have optimally accommodated for these differences in the different ethnicities represented in this cohort. Second, this assessment of bereavement responses was embedded in a large study of many factors relevant to refugee adjustment, and accordingly many factors directly relevant to development of PGD could not be adequately assessed; this precluded investigation into many potential predictors, such as the type of death, relationship to the deceased, attachment issues and mourning rituals. We also could not assess subjective responses to each traumatic event, and the summed total of reported events may not accurately reflect subjective reactions to different events. Third, this sample focused on refugees who were granted permanent protection visa prior to arrival in Australia and did not include current asylum applicants; this sampling resulted in this cohort not including refugees who may had some of the adverse experiences associated with seeking asylum, such as being in a detention facility. Fourth, most of the samples were accompanied by family members, which may moderate the extent to which we observed problematic grief reactions. Fifth, respondents were able to respond to questions using self or interview-administered formats, and this may have introduced some variability; we were not able to differentiate between these formats because respondents chose the format for each question depending on their literacy and confidentiality needs in response to specific questions. Finally, the limited sample size resulted in not being able to conduct multiple-group analyses or include gender interaction terms.
In summary, this report highlights the risk that PGD in refugees poses for the mental health of their children. Although we emphasize that path analyses do not confer causation in the directionality of any direct or indirect paths, the observed associations nonetheless suggest that PGD may be associated with poor psychological functioning in children. There is currently strong evidence for efficacious psychotherapeutic interventions for PGD (Bryant et al., 2014; Shear et al., 2005), and accordingly target PGD is affected refugees may yield important benefits for both the refugees and their children.
Supplemental Material
Supplementary_Materials – Supplemental material for Prolonged grief in refugees, parenting behaviour and children’s mental health
Supplemental material, Supplementary_Materials for Prolonged grief in refugees, parenting behaviour and children’s mental health by Richard A Bryant, Ben Edwards, Mark Creamer, Meaghan O’Donnell, David Forbes, Kim L Felmingham, Derrick Silove, Zachary Steel, Alexander C McFarlane, Miranda Van Hooff, Angela Nickerson and Dusan Hadzi-Pavlovic in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by a National Health and Medical Research Council Grant (1073041). The funder had no role in study design, data collection or analysis, or report preparation. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.