
Abstract
Background:
There is a growing realisation that anxiety symptoms and disorders during pregnancy are associated with various negative outcomes. The aims of this study were to identify latent classes of anxiety symptom trajectories during pregnancy, compare anxiety levels between pregnancy trimesters and ascertain the predictors of anxiety symptom trajectories.
Methods:
Two hundred pregnant women in their first trimester who attended obstetric clinics at the local hospital were recruited. Three self-report questionnaires assessing anxiety levels were administered at three time points during pregnancy. Latent class growth analysis was used to identify anxiety symptom trajectories, and logistic regression analysis was performed to ascertain the predictors of latent class membership.
Results:
Data for analyses were available for 188 women. Two anxiety symptom trajectories were identified: a ‘high-anxiety’ trajectory (13.3% of participating women) and ‘low-anxiety’ trajectory (86.7%). This finding was consistent across all the anxiety measures used in the study. Overall, anxiety levels gradually decreased during pregnancy, with a significant decrease between the first and second trimesters on some measures. Past mental disorders and significant stressors in the preceding 6 months predicted membership in the ‘high-anxiety’ trajectory group.
Conclusions:
These findings support an early assessment of anxiety in pregnant women. If untreated, a high level of anxiety in the first trimester is likely to persist throughout pregnancy, although it may decrease somewhat. An early recognition of pathological anxiety during pregnancy allows its timely treatment and prevention of unfavourable outcomes.
Introduction
Anxiety symptoms during pregnancy are very common (Lee et al., 2007; Soto-Balbuena et al., 2018). Despite that, anxiety symptoms and anxiety disorders during pregnancy are understudied compared to other psychopathology. However, this is changing (e.g. Fawcett et al., 2019; Soto-Balbuena et al., 2018; Viswasam et al., 2019), possibly because of the growing realisation that pathological anxiety during pregnancy is associated with significant negative outcomes.
Research suggests that anxiety symptoms and disorders during pregnancy cause significant distress and difficulty in daily functioning (Martini et al., 2015; Schofield et al., 2014). In addition, prenatal anxiety has been associated with postnatal anxiety, mood symptoms (Grant et al., 2008; Mauri et al., 2010), pre-term delivery, difficult mother–infant bonding and early childhood developmental delays (Biaggi et al., 2016; Martini et al., 2015; Mughal et al., 2018; Sutter-Dallay et al., 2004). Therefore, it is important to better understand and recognise anxiety during pregnancy, including its course and predictors. This might help develop more effective interventions and prevent harmful outcomes for mother and child.
Several studies examined the trajectories of both anxiety and depressive symptoms from pregnancy to the postpartum period, and some reported predictors of these trajectories. Using the Taiwanese version of the State Anxiety Inventory (Chung and Long, 1984), Kuo et al. (2014) assessed women in the third trimester of pregnancy and at four points during the postpartum period and reported four trajectories of anxiety symptoms based on the severity of anxiety: low, mild (largest group), high and very high (smallest group). Bayrampour et al. (2016) assessed women in the second and third trimesters of pregnancy and twice during the postpartum period and identified five trajectories of anxiety symptoms by means of the State–Trait Anxiety Inventory (STAI [Spielberger and Gorsuch, 1983]): minimal anxiety (largest group), mild anxiety, ‘postpartum’ (elevated, but sub-clinical anxiety levels during the second and third trimesters of pregnancy, which increased during the postpartum period), ‘antepartum’ (increased anxiety levels during pregnancy, which decreased after delivery and remained moderate at one year postpartum) and chronic anxiety (smallest group). In this study, history of abuse/neglect, low social support and history of mental health issues were ‘common risk factors of anxiety across all groups’. Ahmed et al. (2018, 2019) assessed women twice during pregnancy (within 20 weeks of gestation and 30 weeks of gestation) and in the early postpartum period and reported three severity-based trajectories of anxiety symptoms using the Edinburgh Postnatal Depression Scale, Anxiety Subscale (Matthey et al., 2013): very low-stable, low-stable and moderate-stable. High levels of stress, history of depression and lower income were significant risk factors for belonging to the moderate-stable anxiety trajectory group.
Two studies investigated trajectories of anxiety symptoms in the perinatal period. Using the STAI (Spielberger, 2010), Agrati et al. (2015) assessed women in the second trimester of pregnancy and 2 years postpartum and found two trajectories of maternal anxiety: a general U-shaped pattern (women who experienced significant adverse life events reported higher anxiety in pregnancy, decreasing at delivery and increasing postpartum) and an increasing linear trajectory (women with low levels of previous adversity showed a moderate increase in their anxiety during the postpartum period). Mughal et al. (2018) assessed women in mid-pregnancy (<24.6 weeks gestation) and 3 years postpartum and identified three trajectory groups by means of the STAI (Spielberger et al., 1970): minimal anxiety symptoms (largest group), sub-clinical anxiety symptoms and high-anxiety symptoms (smallest group).
The aforementioned studies report between two and five trajectories of anxiety symptoms during the perinatal period and different predictors of trajectories, which may be due to methodological factors and differences between samples. The trajectories were identified based on the assessments at different times during pregnancy and the postpartum period, apparently without considering that pregnancy and the postpartum period are associated with different biological and psychological factors that may affect anxiety levels. The trajectories in three out of five studies were based only on one assessment during pregnancy, precluding any conclusion about the course of anxiety symptoms during pregnancy. One study included only pregnant women who considered an elective Caesarean Section (Kuo et al., 2014), which could have influenced anxiety symptom trajectories.
In view of the inconsistent findings of previous studies, the first aim of the current study was to investigate prospectively the course of anxiety symptoms during pregnancy by identifying latent classes of anxiety symptom trajectories. We focused only on pregnancy because of the unique biological, social and psychological factors associated with it and we used several measures of anxiety to avoid reliance on any single instrument and associated potential biases. The second aim of our study was to compare the levels of anxiety between various trimesters of pregnancy, while the third aim was to ascertain the predictors of different trajectories of anxiety symptoms during pregnancy. We undertook the study expecting it to contribute to a better understanding of the course and severity of anxiety during pregnancy and thereby improve detection of a clinically significant anxiety and planning of treatment approaches to anxiety at this period in women’s lives.
Given that the majority of previous studies identified at least three anxiety symptom trajectories during the perinatal period, we hypothesised that there would be three severity-based trajectories of anxiety symptoms in the present study. We also hypothesised that pre-existing mental disorders and recent stressful events might predict higher levels of anxiety during pregnancy. We had no specific hypothesis about the course of anxiety symptoms across the pregnancy trimesters, that is, we did not hypothesise whether these symptoms tended to increase, decrease or remain stable.
Methods
Recruitment
Pregnant women in their first trimester attending ultrasound and antenatal clinics at Nepean Hospital, Penrith, Australia were approached for participation in the study. Two hundred pregnant women who met the inclusion/exclusion criteria were recruited. Ethics approval was obtained from the Nepean Blue Mountains Local Health District Human Research Ethics Committee (HREC reference number: LNR/15/NEPEAN/77 – Study 15/34), and the study was conducted in accordance with the World Medical Association (WMA) Declaration of Helsinki. Participants signed a consent form after the study had been explained to them.
Inclusion and exclusion criteria
Inclusion criteria for participation in the study were a low-risk pregnancy and being over 18 years of age. There were several exclusion criteria: current presence or lifetime history of schizophrenia, other psychotic disorders or bipolar affective disorder and presence of serious medical conditions and maternal/foetal obstetric complications, such as foetal abnormalities.
Assessments
Women who agreed to participate in the study were asked to complete the Demographic and Clinical History Questionnaire and the Perinatal Anxiety Screening Scale (PASS). They were subsequently administered the remaining self-report questionnaires during their first trimester (12–16 weeks gestation). The same instruments were administered to participants in their second trimester (17–28 weeks gestation) and third trimester (29–42 weeks gestation).
Instruments
Demographic and Clinical History Questionnaire
A short questionnaire was designed with the aim of obtaining demographic data (age, educational level, relationship status, employment status, country of birth) and information on the relevant health behaviours (smoking and use of alcohol and illicit drugs) and clinical history. The questions pertaining to the planned or unplanned nature of current pregnancy, any previous pregnancies, history of miscarriage or loss of a baby, significant life stressors in the previous 6 months, history of mental disorders and use of psychotropic medications were constructed to elicit dichotomous ( ‘yes’ or ‘no’) responses.
PASS
The PASS is a 31-item self-report measure used to screen for anxiety disorders in the perinatal period (Somerville et al., 2014, 2015). It consists of four subscales that measure specific symptoms of anxiety in antenatal and postnatal women: (1) General Worry & Specific Fears; (2) Perfectionism, Control & Trauma; (3) Social Anxiety and (4) Acute Anxiety & Adjustment. Each item is scored on a 4-point Likert-type scale ranging from 0 (not at all) to 3 (almost always). The total PASS score is obtained by adding the scores on all PASS items, with this score ranging from 0 to 93. Scores from 0 to 20 denote being ‘asymptomatic’ of anxiety, scores between 21 and 41 reflect mild to moderate anxiety and scores of 42 and above suggest severe anxiety.
The PASS was selected because of its relevance for use in pregnant women and because it was developed in Australia and is therefore suitable for administration in an Australian setting. In the present study, the PASS was used to assess the severity of anxiety during pregnancy (Somerville et al., 2015). The PASS has demonstrated excellent reliability (Somerville et al., 2015) and has been used in several other studies (Pereira et al., 2019; Priyadarshanie et al., 2020; Yasmin and Islam, 2018; Yazici et al., 2019). Internal consistency (Cronbach’s α) values for the PASS total score and PASS subscales in the present study ranged from 0.88 to 0.96 at the first trimester assessment.
Depression, Anxiety and Stress Scale 21
The Depression, Anxiety and Stress Scale 21 (DASS-21) is a commonly used 21-item instrument that measures symptoms of depression, anxiety and stress on three subscales over the preceding week (Lovibond and Lovibond, 1995). Each item is scored on a 4-point Likert-type scale ranging from 0 (‘did not apply to me at all’) to 3 (‘applied to me very much’). The DASS provides a total score and separate scores on each subscale; these scores are calculated by adding the respective item scores. The DASS-21 has demonstrated a sound internal consistency (Henry and Crawford, 2005; Osman et al., 2012). Internal consistency (Cronbach’s α) values for the DASS subscales in the present sample ranged from 0.88 to 0.92 at the first trimester assessment.
The six-item Spielberger State Anxiety Inventory
The six-item version of the Spielberger State Anxiety Inventory (STAI) measures the intensity of state anxiety and has been found to be a valid and reliable instrument for use in perinatal women, with internal consistency values (Cronbach’s α) ranging from 0.91 to 0.93 (Bayrampour et al., 2014; Marteau and Bekker, 1992). Responses are rated on a 4-point Likert-type scale from 1 (not at all) to 4 (very much). Internal consistency for the STAI in the present sample was 0.79 at the first trimester assessment.
Statistical analyses
Data analysis was performed in two stages. The first stage involved calculation of descriptive statistics and non-parametric comparisons of self-report questionnaire scores in IBM SPSS Statistics 25. The second stage involved conducting latent class growth analyses in MPlus version 7.31 (Muthén and Muthén, 1998−2010) before performing regression analyses to predict latent class membership in IBM SPSS Statistics 25.
The expectation maximisation (EM) algorithm in IBM SPSS Statistics 25 was used to estimate values in lieu of missing values for self-report questionnaire total scores prior to proceeding to inferential tests. Given that demographic variables were categorical (except for age), these were not included in the estimation.
The distributions of almost all the scores on self-report symptom measures indicated a pronounced positive skew. Friedman tests were therefore used to compare the rank order of scores on each of these measures (PASS, DASS and STAI). Post hoc comparisons between scores for each respective pair of assessment points were made using the Wilcoxon Signed Ranks Test, while Bonferroni corrections were used for multiple comparisons.
The second stage of the analysis explored latent classes of anxiety symptom trajectories. Latent class growth analysis (LCGA) divides the trajectories of groups of participants into mutually exclusive and exhaustive classes (Collins and Lanza, 2010), which are ‘latent’ in that class membership is not directly observed or measured (O’Donnell et al., 2017). The number of classes is determined partly on the basis of theory (parsimony being favoured) and partly on the basis of a number of fit indices. The Akaike Information Criterion (Akaike, 1987) and Bayesian Information Criterion (Schwartz, 1978) are goodness-of-fit indices where lower values correspond to improved model fit. The Lo–Mendell–Rubin Likelihood Ratio Test (Lo et al., 2001) provides a p value that indicates if a model fits the data better than a model with one class less (Nylund et al., 2007). The entropy values, which indicate the classification accuracy of a solution, are also reported, with values closer to 1 indicating a relatively stronger class classification accuracy (Geiser, 2010).
All models included an intercept and slope term, with the number of random starts set to 1000 and the number of iterations set to 200. Preliminary analyses were conducted using latent growth mixture models (LGMM). However, due to convergence problems with the LGMM models, we had to constrain all within-class variances to zero, consistent with the LCGA approach (Jung and Wickrama, 2008). Once the number of trajectory classes was determined, the most likely class membership of each participant was regressed upon hypothesised variables to determine the predictors of symptom trajectories. We report the LCGA and logistic regression results for the PASS total score because the PASS was developed and validated with the purpose of indexing anxiety symptoms during pregnancy. The results of similar LCGA and logistic regression analyses for the DASS Anxiety subscale and STAI are provided as supplementary online material.
Results
Of 200 women who consented to participate, there were missing data on key demographic variables for 12 (6%) women. Therefore, these participants’ data were removed from the analysis, leaving the overall sample of 188 women. Table 1 summarises the demographic and clinical characteristics of this sample; of note, one-third of women had a previous miscarriage or loss of baby and in two-thirds, the current pregnancy was unplanned.
Demographic and clinical characteristics at first trimester assessment (N = 188).
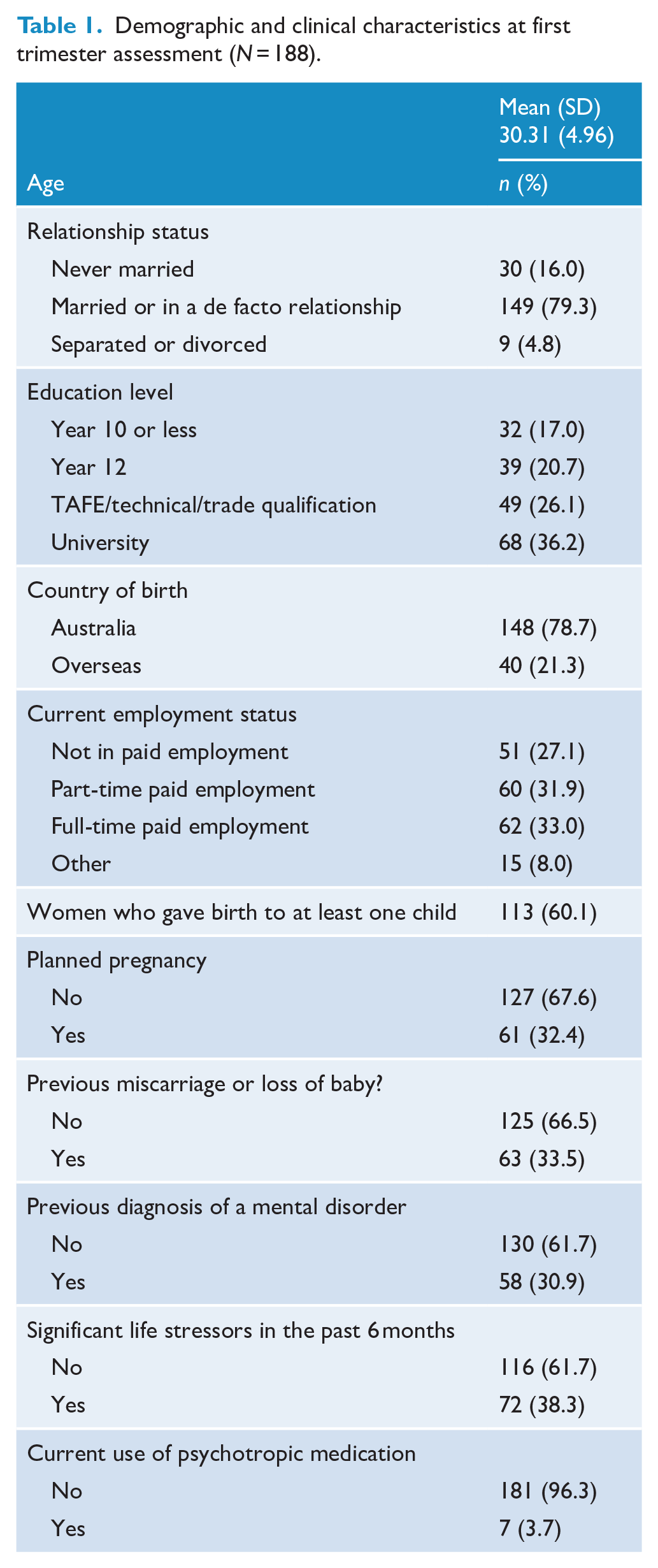
Questionnaires were completed by 156 (83%) participants in the first trimester, 145 (77%) participants in the second trimester and 139 (74%) participants in the third trimester. Of 49 participants who did not complete the questionnaires in the first, second or third trimester, 37 (76%) were lost to follow-up for various reasons (e.g. being unable to commit to completing questionnaires, no longer interested in participating in the study, unable to be contacted). Other reasons for not completing the questionnaires include miscarriage (4 participants), foetal abnormalities (3), premature delivery (2), foetal loss (2) and pregnancy complication (1).
The EM algorithm was applied to data in the first, second and third trimesters consecutively, given that conducting missing value analyses separately within each cluster when working with clustered data is recommended (Graham, 2009). Inspection of Little’s MCAR statistics indicated that data were missing completely at random at the first trimester assessment (χ2 = 104.40, df = 112, p = 0.68) and third trimester assessment (χ2 = 39.84, df = 38, p = 0.39), but not at the second trimester assessment (χ2 = 109.30, df = 75, p = 0.01).
Table 2 shows the means and standard deviations on each questionnaire in the first, second and third trimesters. Overall, levels of anxiety decreased on almost all measures across the pregnancy. Pairwise comparisons indicated that anxiety levels decreased significantly between the first and second trimesters on the PASS General Worry & Specific Fears, PASS Perfectionism, Control & Trauma and PASS Total Score.
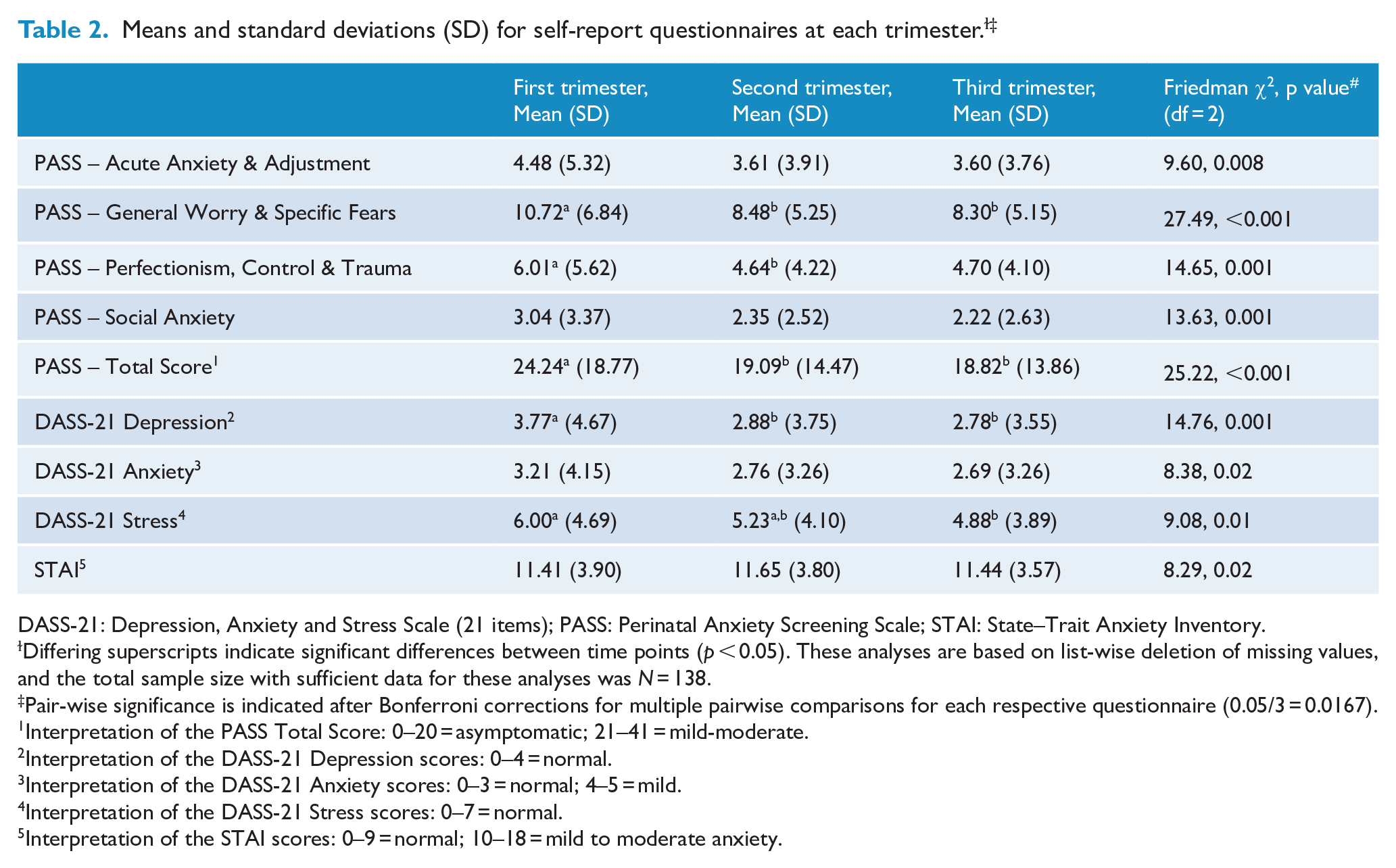
DASS-21: Depression, Anxiety and Stress Scale (21 items); PASS: Perinatal Anxiety Screening Scale; STAI: State–Trait Anxiety Inventory.
Differing superscripts indicate significant differences between time points (p < 0.05). These analyses are based on list-wise deletion of missing values, and the total sample size with sufficient data for these analyses was N = 138.
Pair-wise significance is indicated after Bonferroni corrections for multiple pairwise comparisons for each respective questionnaire (0.05/3 = 0.0167).
Interpretation of the PASS Total Score: 0–20 = asymptomatic; 21–41 = mild-moderate.
Interpretation of the DASS-21 Depression scores: 0–4 = normal.
Interpretation of the DASS-21 Anxiety scores: 0–3 = normal; 4–5 = mild.
Interpretation of the DASS-21 Stress scores: 0–7 = normal.
Interpretation of the STAI scores: 0–9 = normal; 10–18 = mild to moderate anxiety.
The results of the LCGA for the PASS Total Score are summarised in Table 3. The results of additional LCGA for the DASS Anxiety subscale and STAI are reported in Supplementary Tables 1 and 2, respectively. Inspection of AIC, BIC and LMRLRT statistics suggest that a two trajectory-class solution is most parsimonious: one class of participants who remained consistently high on the PASS Total Score throughout their pregnancy (the ‘high-anxiety’ group; n = 25 [13.3%]) and another class who remained consistently low on the PASS Total Score throughout their pregnancy (the ‘low anxiety’ group; n = 163 [86.7%]). There was a distinct decrease in the rate of diminution in the AIC and BIC values beyond two groups, with the LMRLRT indicating that while a two-group solution was significantly better than one, a further class identification did not provide a significantly better fit beyond the two-class solution. Furthermore, the entropy value for the two-class solution indicated excellent classification accuracy for this solution. It is noteworthy that a two-class solution was also found when LCGA was conducted for the DASS Anxiety and STAI (Supplementary Tables 1 and 2). With regard to the PASS Total Score, participants from both the low and high classes tended to report decreasing anxiety symptoms across time at a similar rate (Figure 1).
Incremental fit statistics and classification accuracy for latent class growth model for PASS total scores (N = 188).
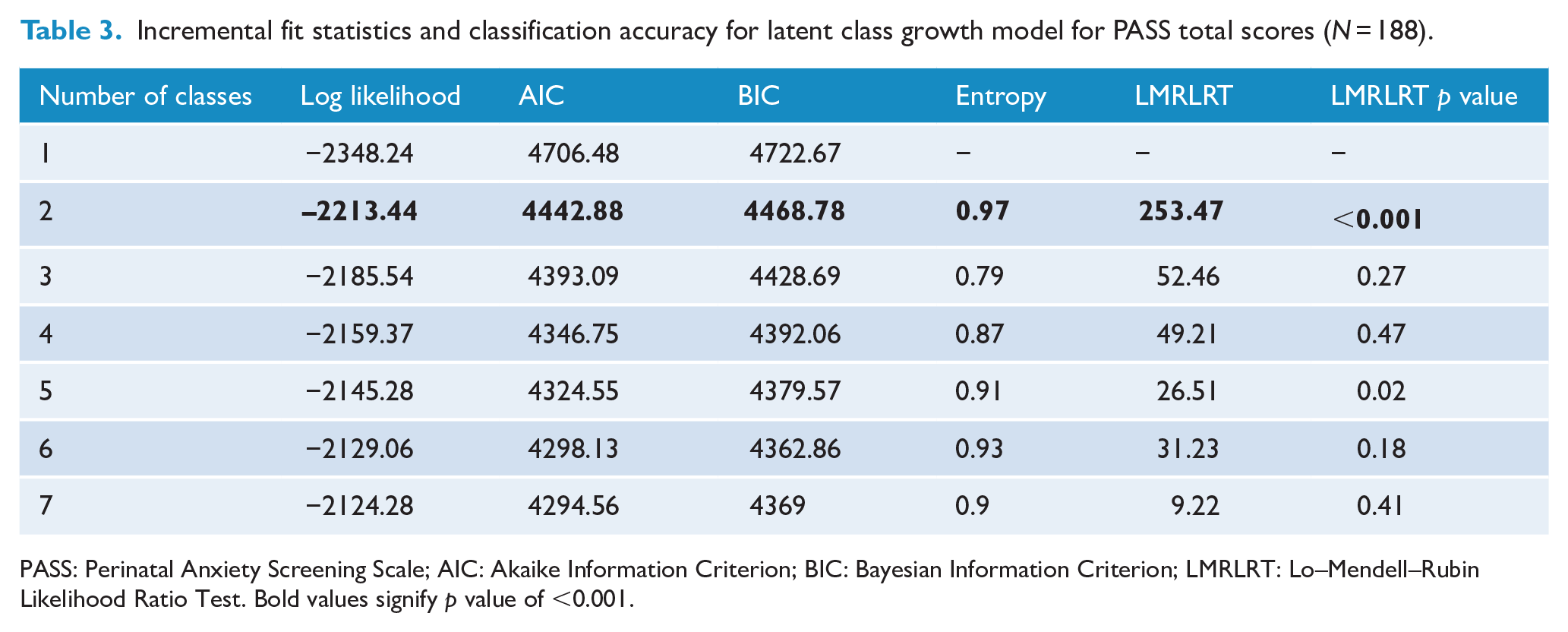
PASS: Perinatal Anxiety Screening Scale; AIC: Akaike Information Criterion; BIC: Bayesian Information Criterion; LMRLRT: Lo–Mendell–Rubin Likelihood Ratio Test. Bold values signify p value of <0.001.
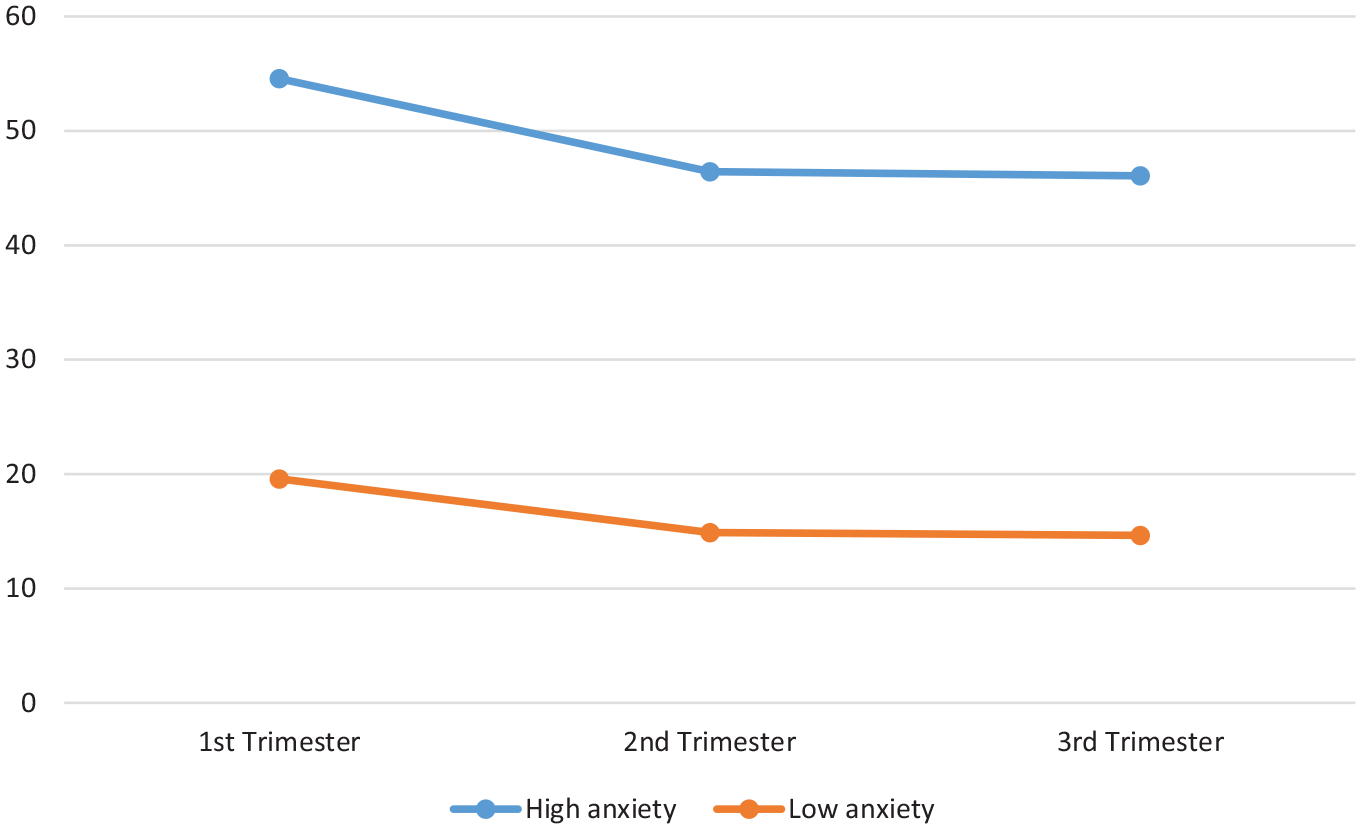
Perinatal Anxiety Screening Scale (PASS)-based class trajectories.
The results of the logistic regression analysis are summarised in Table 4, where the variable summarising each participant’s assigned latent trajectory-class membership based on the PASS Total Score was regressed on pregnancy-related variables (first pregnancy, planned pregnancy and history of miscarriage), history of any mental disorder and presence of recent life stressors. All variance inflation factor values were less than 2, indicating that multicollinearity was not problematic. Only past diagnosis of any mental disorder (95% CI = [3.41, 26.42]) and the presence of stressors in the preceding 6 months (95% CI = [1.63, 12.23]) were significant independent predictors of membership in the high PASS Total Score class.
Logistic regression analysis predicting membership in the high PASS class, based on the PASS Total Score (N = 188).
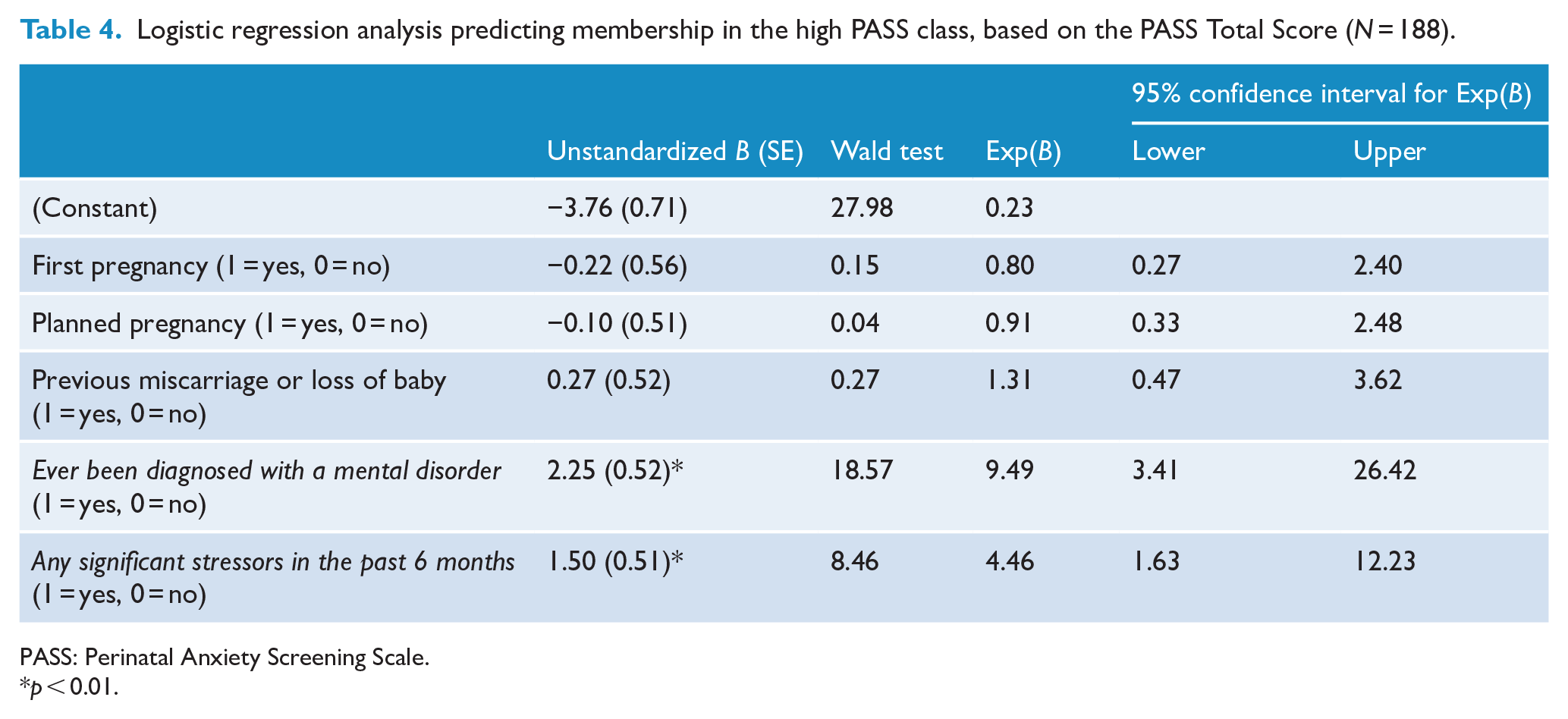
PASS: Perinatal Anxiety Screening Scale.
p < 0.01.
A similar pattern of results was found when logistic regression analyses were run to predict membership in high and low classes based on the DASS Anxiety and STAI scores, respectively (Supplementary Tables 3 and 4). In addition, a logistic regression analysis found that a past diagnosis of any mental disorder and presence of recent stressors were significant predictors of membership in a class with high DASS Stress scores.
Discussion
The current study identified two anxiety symptom trajectories during pregnancy: high-anxiety trajectory where anxiety levels were consistently high throughout pregnancy and low-anxiety trajectory in which women demonstrated low anxiety levels throughout pregnancy. Thus, both trajectories reflect a relatively stable course of anxiety during pregnancy. This finding is broadly consistent with the number of trajectories (between two and five) reported by other studies (Agrati et al., 2015; Ahmed et al., 2018, 2019; Bayrampour et al., 2016; Kuo et al., 2014; Mughal et al., 2018), especially when considering the trajectories based on symptom severity. However, other studies identified these trajectories across the whole perinatal period, whereas our study only focused on pregnancy.
We also found that anxiety levels decreased on almost all measures between the first and second trimesters, with a significant decrease on the scores of the PASS Total, PASS – General Worry & Specific Fears and PASS – Perfectionism, Control & Trauma. A decrease in anxiety levels from the first to the second trimester has also been reported by other studies (Lee et al., 2007; Madhavanprabhakaran et al., 2015; Soto-Balbuena et al., 2018). Levels of anxiety decreased further on almost all measures between the second and third trimesters, but these changes were smaller and statistically non-significant. It is important to note that changes in the levels of anxiety during pregnancy occurred within the identified trajectories of either generally high or generally low levels of anxiety (Figure 1).
Higher levels of anxiety in the first trimester can result from a fearful anticipation of uncertainties and challenges associated with pregnancy, including physical discomfort and health-related issues (e.g. Soto-Balbuena et al., 2018), bodily and body image changes, different partner expectations and altered partner dynamics. An unplanned or unwanted pregnancy in the first trimester can also be anxiety-provoking, given its potentially negative impact on marital and family relationships, work and finances, as well as its possible adverse psychosocial consequences (Orr and Miller, 1997). Higher anxiety levels in the first trimester may also be a consequence of psychotropic medication cessation due to pregnancy; however, a small proportion (7.4%) of women in our sample stopped these medications. Previous research has suggested several other factors to be specifically associated with high levels of anxiety in the first trimester: being younger (Lee et al., 2007), bearing a first child (Lee et al., 2007; Teixeira et al., 2009), history of miscarriage (Biaggi et al., 2016) and fear of childbirth (Madhavanprabhakaran et al., 2015).
A decrease in the levels of anxiety between the first and second trimesters may be due to women feeling more secure and better adjusted in their second trimester (Soto-Balbuena et al., 2018). A similar confidence about the course and outcome of pregnancy may explain a further decrease in anxiety in the third trimester. Another reason for this finding is that a number of women in our study were treated for anxiety during pregnancy: 16.4% received psychological therapy, 2% recommenced psychopharmacotherapy and 4% received both psychological therapy and psychopharmacotherapy. Furthermore, birthing classes might have also decreased anxiety levels. However, closer to the time of delivery, anxiety levels could rise again due to concerns about childbirth, which may account for findings of some studies in the third trimester (Lee et al., 2007; Madhavanprabhakaran et al., 2015; Soto-Balbuena et al., 2018).
The final aim of the present study was to ascertain the predictors of high levels of anxiety during pregnancy. We found that a previous diagnosis of any mental disorder and presence of significant stressors in the preceding 6 months were important independent predictors of the membership in the high-anxiety trajectory group. These results are broadly consistent with previous research findings (Ahmed et al., 2018, 2019; Bayrampour et al., 2016; Biaggi et al., 2016; Deklava et al., 2015). Interestingly, factors that may be expected to be associated with heightened anxiety levels – first pregnancy, unplanned pregnancy and history of miscarriage or loss of baby – did not emerge as significant predictors of high-anxiety levels during pregnancy. This is an important finding, considering large proportions of women in our study were without a prior experience of giving birth (39.9%) and having an unplanned pregnancy (67.6%) and history of miscarriage or loss of baby (33.5%).
To the best of our knowledge, this is the first prospective study to compare the levels of anxiety at three time points during pregnancy using three validated self-report measures of anxiety. This comprehensive and continuous assessment of anxiety throughout pregnancy is the advantage of the current study compared to previous research. Further strengths of our study include the consistency in the number of trajectories and logistic regression findings across the different measures of anxiety and the focus on pregnancy, without the potentially confounding effects of the postpartum assessments of anxiety.
A unique contribution of our study is identification of the two severity-based anxiety symptom trajectories (‘high-anxiety’ and ‘low-anxiety’ trajectories) during pregnancy, along with a finding of a gradual decrease in anxiety levels within these trajectories from the first to the third pregnancy trimester. The main clinical implication of these findings is a strong support for assessment of anxiety in the first pregnancy trimester and in particular, a need to detect high-anxiety levels at that time. High-anxiety levels in the first pregnancy trimester are likely to persist throughout pregnancy, despite some decrease, which calls for treatment and prevention of complications.
Limitations
There are several limitations of the present study. First, it was based on self-report instruments that may be subject to bias. Second, clinical history information was obtained via Demographic and Clinical History Questionnaire which allowed only dichotomous ( ‘yes’ or ‘no’) responses, with no possibility of more nuanced responses (e.g. on a continuum). Third, the missing value analysis indicated that data might not have been missing completely at random at the second trimester assessment, potentially leading to bias in some estimates. However, the overall pattern of results was similar when we used a Listwise instead of the EM approach to missing data, thus providing confidence that the extent of any bias was small. Fourth, the fact that data were only collected at three assessment points precluded the identification of any non-linear trajectories of symptom changes. Fifth, our sample was not necessarily representative of the Australian pregnant women. For example, there was a larger proportion of pregnant women born in Australia in our sample compared to the 2017 maternal country of birth data in Australia (78.7% vs 64.4%) and we had no indigenous women, as opposed to 4.5% indigenous mothers in Australia in 2017 (Australian Institute of Health and Welfare, 2019). Furthermore, we could not control for treatment administered during pregnancy, and the fact that almost a quarter of women received treatment for anxiety is likely to have influenced our findings. Finally, while the proportions of the sample endorsing previous mental disorders and recent life stress provided adequate statistical power to detect class membership, the small proportions of women with first or planned pregnancy and of those who experienced a previous miscarriage resulted in attenuated statistical power to detect class membership. Future studies should aim to recruit larger or more balanced samples in these respects.
Conclusion
This prospective study makes several contributions to the literature. First, it has identified two severity-based anxiety symptom trajectories during pregnancy. Second, it has found that anxiety symptoms tend to decrease throughout pregnancy, especially from the first to the second trimester. Finally, the study has confirmed that previous mental health problems and recent stressors predict high levels of anxiety during pregnancy. Taken together, these findings strongly support a need for early identification of high anxiety levels in pregnant women, because it increases the opportunities for timely treatment. In addition, our study makes a strong case for continuous and comprehensive assessment of anxiety (and other mental health issues) during pregnancy. For reasons pertaining to the continuity of monitoring and care, specific characteristics of each pregnancy trimester and convenience, we suggest that such assessments occur during each pregnancy trimester. Future studies could expand our knowledge by being conducted in larger samples, by examining additional predictors of high anxiety levels during pregnancy and by focusing on anxiety symptom trajectories in pregnant women with pre-existing anxiety or depressive disorders.
Supplemental Material
Supplementary_Table_1 – Supplemental material for Trajectories and predictors of anxiety symptoms during pregnancy in an Australian sample
Supplemental material, Supplementary_Table_1 for Trajectories and predictors of anxiety symptoms during pregnancy in an Australian sample by Kirupamani Viswasam, David Berle and Vladan Starcevic in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Table_2 – Supplemental material for Trajectories and predictors of anxiety symptoms during pregnancy in an Australian sample
Supplemental material, Supplementary_Table_2 for Trajectories and predictors of anxiety symptoms during pregnancy in an Australian sample by Kirupamani Viswasam, David Berle and Vladan Starcevic in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Table_3 – Supplemental material for Trajectories and predictors of anxiety symptoms during pregnancy in an Australian sample
Supplemental material, Supplementary_Table_3 for Trajectories and predictors of anxiety symptoms during pregnancy in an Australian sample by Kirupamani Viswasam, David Berle and Vladan Starcevic in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Table_4 – Supplemental material for Trajectories and predictors of anxiety symptoms during pregnancy in an Australian sample
Supplemental material, Supplementary_Table_4 for Trajectories and predictors of anxiety symptoms during pregnancy in an Australian sample by Kirupamani Viswasam, David Berle and Vladan Starcevic in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.