
Abstract
Background:
Lithium in drinking water may have significant mental health benefits. We investigated the evidence on the association between lithium concentrations in drinking water and their neuropsychiatric outcomes.
Methods:
We conducted a systematic review and meta-analysis and searched Pubmed, Embase, Web of Science, PsycINFO and CINAHL up to 19 January 2020, for peer-reviewed research examining the association between lithium concentrations in drinking water and neuropsychiatric outcomes. We used a pairwise analysis and a random effects model to meta-analyse suicide rates and psychiatric hospital admissions. We assessed for publication bias using Egger’s test and Duval and Tweedie’s Trim and Fill analysis.
Results:
Twenty-seven studies including 113 million subjects were included in this systematic review. Meta-analysis of 14 studies including 94 million people found higher lithium concentrations were associated with reduced suicide rates (r = −0.191, 95% confidence interval = [−0.287, −0.090], p < 0.001) and meta-analysis of two studies including 5 million people found higher lithium concentrations were associated with fewer hospital admissions (r = −0.413, 95% confidence interval = [−0.689, −0.031], p = 0.035). We found significant heterogeneity between studies (Q = 67.4, p < 0.001, I2 = 80.7%) and the presence of publication bias (Egger’s test; t value = 2.90, p = 0.013). Other included studies did not provide sufficient data to analyse other neuropsychiatric outcomes quantitatively.
Conclusion:
Higher lithium concentrations in drinking water may be associated with reduced suicide rates and inpatient psychiatric admissions. The relationship with other neuropsychiatric outcomes and complications remains unclear. Further research is required before any public health recommendations can be made.
Introduction
Even after 70 years since John Cade’s (2000) ground-breaking discovery, lithium remains the ‘gold standard’ for bipolar disorder (Malhi et al., 2015, 2017; Tondo et al., 2019). In the clinical setting, the recommended lithium serum level is 0.60–0.80 mmol/L (Malhi et al., 2018b, 2020; Nolen et al., 2019). This can be reduced to 0.40–0.60 mmol/L where there is good response but poor tolerance or, alternatively, increased to 0.80–1.00 mmol/L for insufficient response but good tolerance (Nolen et al., 2019). The mechanism of its action, however, is still not completely understood (Malhi et al., 2013; Malhi and Outhred, 2016). Active research is currently undergoing to elucidate the mechanism of action, as well as the expansion of lithium’s therapeutic horizons in light of its neuroprotective properties (Lauterbach and Mendez, 2011; Malhi, 2018) and its suicide-preventing qualities (Bauer and Gitlin, 2016; Tondo et al., 2019).
One developing area of interest is the presence of lithium in drinking water. Lithium is a natural trace element often present in drinking water and is a naturally occurring food ingredient (Dolara, 2014). Although the concentration in drinking water is markedly lower than that used in clinical practice (Pompili et al., 2015), a growing body of literature suggests that trace amounts of lithium in drinking water may be protective against various neuropsychiatric outcomes.
The potential benefit of lithium in drinking water was first suggested by Dawson et al. (1970) who found that higher concentrations of lithium in drinking water were associated with lower rates of hospital admissions. Since then, many large epidemiological studies have investigated the effects of lithium in drinking water on neuropsychiatric conditions and complications including suicide (Blüml et al., 2013; Giotakos et al., 2013; Ishii et al., 2015; Kapusta et al., 2011; Liaugaudaite et al., 2017, 2019; Ohgami et al., 2009; Schrauzer and Shrestha, 1990; Shiotsuki et al., 2016; Sugawara et al., 2013), dementia (Kessing et al., 2017a; Parker et al., 2018), bipolar disorder (Kessing et al., 2017b; Parker et al., 2018; Schullehner et al., 2019), schizophrenia (Schullehner et al., 2019) and depression (Parker et al., 2018). To our knowledge, there has been no study that has systematically reviewed and meta-analysed the potential therapeutic benefits of lithium in drinking water across different neuropsychiatric outcomes. In the current systematic review, we examined the effect of differing lithium concentrations in drinking water on a wide range of neuropsychiatric outcomes. We hypothesised that higher concentrations would be associated with lower rates of neuropsychiatric outcomes.
Method
Search strategy and selection criteria
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline (Moher et al., 2009). We searched Pubmed, Embase, Web of Science, PsycINFO and CINAHL until 19 January 2020, for studies investigating lithium in drinking water and neuropsychiatric outcomes. We also used SCOPUS to check the references and citations of included studies and relevant reviews. Our search terms focused on lithium, drinking water and the neuropsychiatric outcomes of interest (Supplementary Table 1). These included suicide, psychiatric hospital admissions, bipolar disorder, dementia, schizophrenia, major depressive disorder, psychotic experiences and depressive and anxiety symptoms. The inclusion criteria for our review included (1) an observational design (cohort, cross-sectional, case–control or longitudinal), (2) published in a peer-reviewed journal and represented original research and (3) an investigation of lithium concentrations in drinking water and its relationship with the chosen neuropsychiatric outcomes. We had no language restrictions. This study was prospectively registered with PROSPERO (registration number: CRD42018090145).
Two authors (E.M. and B.E-W.) independently screened titles and abstracts for eligible studies, followed by a full-text review for studies that met the inclusion criteria. Any disputes were settled through discussion with another author (S.S.). Two authors (E.M. and B.E-W.) independently extracted the following data from the included studies: authors, publication year, study region, study design, years investigated, sample size, region number, lithium concentration, neuropsychiatric outcomes, neuropsychiatric outcome assessment tools and all relevant results. Authors of eligible studies were contacted for additional information if further clarification was needed.
Data analysis
We found studies investigating the relationship between lithium concentration in drinking water and suicide, psychiatric hospital admissions, bipolar disorder, dementia, major depressive disorder, schizophrenia, schizophrenia spectrum disorders, psychotic experiences and depressive and anxiety symptoms. The correlations were reported using incidence rate ratios (IRR), relative risk (RR), rates of incidence, odds ratio and beta (β), T, r and r2 values. Significance was reported as p values or confidence intervals (CI).
Regression coefficients extracted from each of studies were converted to the correlation coefficient ‘r’, using published formulas (Lipsey and Wilson, 2001; Peterson and Brown, 2005) in order to standardise the effect sizes between studies (Supplementary Table 2). Data from the most adjusted findings from each paper, including log-transformed lithium concentrations if the distribution of lithium was skewed, and adjustments accounting for confounders were used. Following this, Comprehensive Meta-Analysis 3.0 was used to pool the correlation coefficients from individual studies in a meta-analysis and conduct a pairwise analysis (Supplementary Table 3). Studies which only provided data by year (Pompili et al., 2015) or gender (Kapusta et al., 2011; Sugawara et al., 2013) were included as separate datapoints by year or gender, then combined to provide overall study data.
Subgroup analyses were applied to hospital admissions to examine differences by psychiatric diagnoses. Random-effects models were used throughout, in order to account for the expected heterogeneity between studies. A sensitivity analysis was also conducted excluding low-quality studies and Ohgami et al. (2009) as the standardised β coefficient was outside the −0.5 to 0.5 range that is recommended to transform β to r values (Peterson and Brown, 2005). We further excluded Liaugaudaite et al. (2017) in a separate sensitivity analysis, as it shared some data with a larger study conducted by Liaugaudaite et al. (2019). A sensitivity analysis of excluding studies that did not provide adjusted results was undertaken, as was a sensitivity analysis of removing each individual study to explore each study’s impact on overall effect.
As the lithium concentrations and its correlations with neuropsychiatric outcomes were measured across geographical regions rather than individuals, we used the number of municipalities investigated as the population in our analyses (Table 1). In addition, a meta-regression was conducted on studies investigating suicide rates where the mean lithium concentration was reported to assess whether a dose–response relationship existed.
We used a modified Newcastle-Ottawa scale to assess the risk of bias (Mata et al., 2015). The scale assesses the following: (1) the representativeness of the sample, (2) sample size, (3) non-respondents, (4) ascertainment of neuropsychiatric outcome and (5) quality of descriptive statistics reported. A score of 3 or more was classified as low risk, and a score of 2 or less was classified as high risk (Supplementary Table 4). Publication bias was investigated by Egger’s test (Egger et al., 1997), Duval and Tweedie’s Trim and Fill analysis (Duval and Tweedie, 2000) and examining the funnel plot.
Summary of included studies for the association between lithium in drinking water and neuropsychiatric outcomes: a systematic review and meta-analysis from across 2678 regions containing 113 million people.
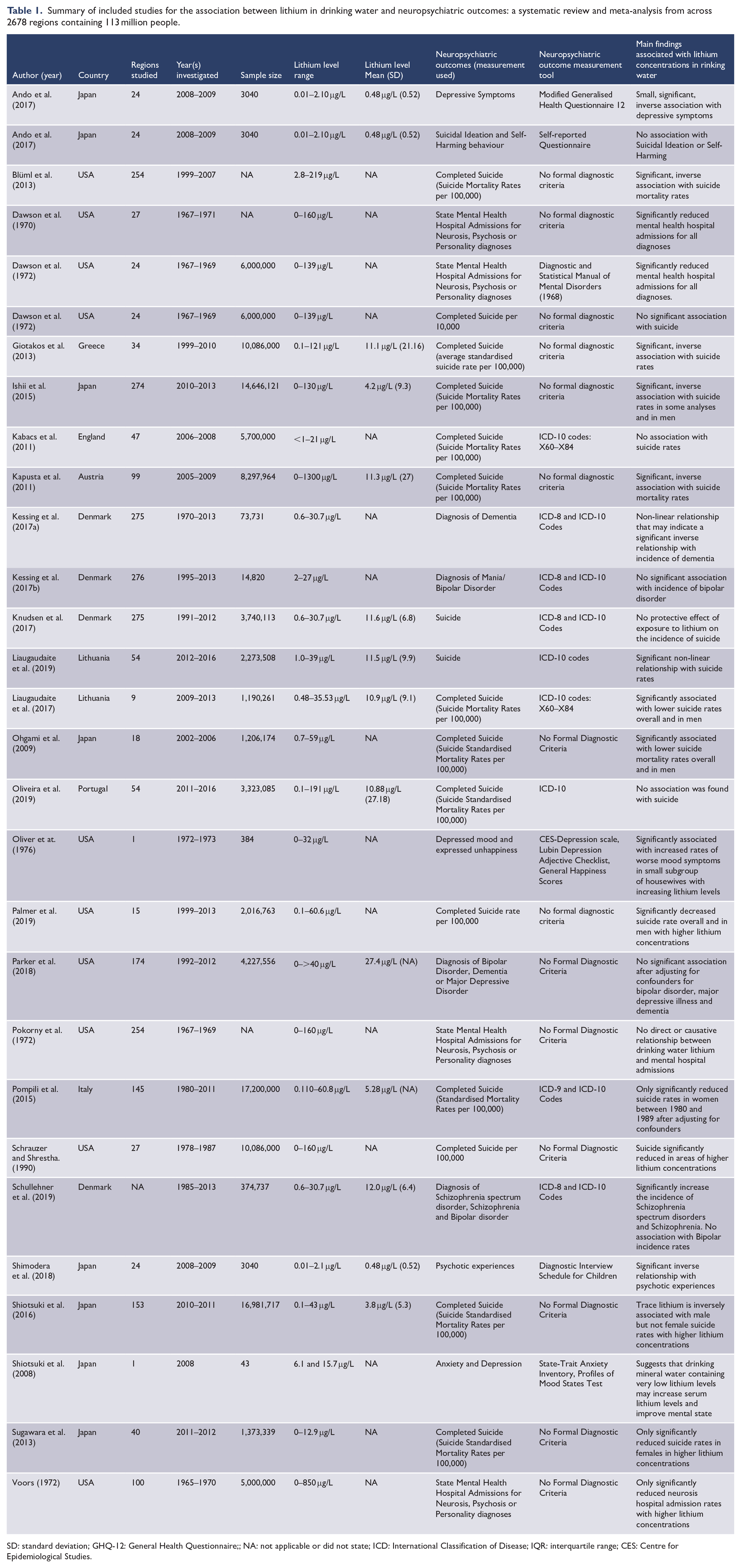
SD: standard deviation; GHQ-12: General Health Questionnaire;; NA: not applicable or did not state; ICD: International Classification of Disease; IQR: interquartile range; CES: Centre for Epidemiological Studies.
No specific ethics approval was necessary for this study. Patient consent was not required for our study.
Results
Searches and sample of studies
We identified 2305 articles. After removing 1003 as duplicates, we screened the titles and abstracts of the remaining 1302 and identified 37 articles that met the inclusion criteria. After the full-text review, 10 papers were excluded. In total, 27 articles were included in our systematic review (Ando et al., 2017; Blüml et al., 2013; Dawson et al., 1970, 1972; Giotakos et al., 2013; Ishii et al., 2015; Kabacs et al., 2011; Kapusta et al., 2011; Kessing et al., 2017a, 2017b; Knudsen et al., 2017; Liaugaudaite et al., 2017, 2019; Ohgami et al., 2009; Oliveira et al., 2019; Oliver et al., 1976; Palmer et al., 2019; Parker et al., 2018; Pokorny et al., 1972; Pompili et al., 2015; Schrauzer and Shrestha, 1990; Schullehner et al., 2019; Shimodera et al., 2018; Shiotsuki et al., 2008, 2016; Sugawara et al., 2013; Voors, 1972), with 16 used in our meta-analysis (Blüml et al., 2013; Dawson et al., 1970; Giotakos et al., 2013; Ishii et al., 2015; Kabacs et al., 2011; Kapusta et al., 2011; Liaugaudaite et al., 2017, 2019; Ohgami et al., 2009; Oliveira et al., 2019; Palmer et al., 2019; Pompili et al., 2015; Schrauzer and Shrestha, 1990; Shiotsuki et al., 2016; Sugawara et al., 2013; Voors, 1972). A PRISMA flow diagram outlines this process (Figure 1), and a table of excluded studies after full-text review is provided as Supplementary Table 5.
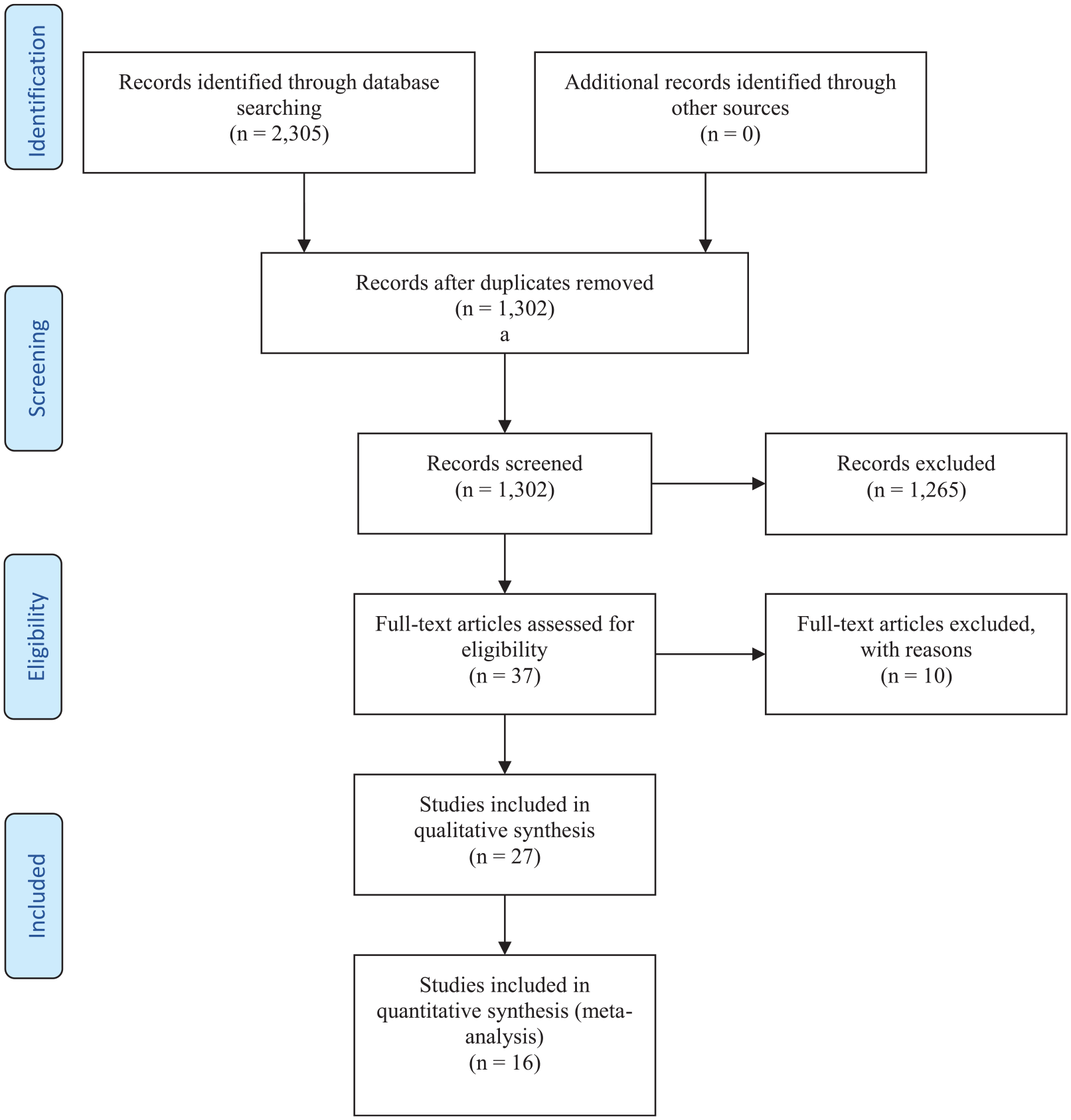
PRISMA flowchart for the association between lithium in drinking water and neuropsychiatric outcomes: a systematic review and meta-analysis from across 2678 regions containing 113 million people.
The characteristics of the 27 included studies are shown in Table 1. In all, 20 studies were longitudinal (Blüml et al., 2013; Dawson et al., 1970, 1972; Giotakos et al., 2013; Ishii et al., 2015; Kabacs et al., 2011; Kapusta et al., 2011; Liaugaudaite et al., 2017, 2019; Ohgami et al., 2009; Oliveira et al., 2019; Palmer et al., 2019; Parker et al., 2018; Pokorny et al., 1972; Pompili et al., 2015; Schrauzer and Shrestha, 1990; Schullehner et al., 2019; Shiotsuki et al., 2016; Sugawara et al., 2013; Voors, 1972), 3 were case–control studies (Kessing et al., 2017a, 2017b; Knudsen et al., 2017) and 4 were cross-sectional studies (Ando et al., 2017; Oliver et al., 1976; Shimodera et al., 2018; Shiotsuki et al., 2008). Of the longitudinal studies, 14 investigated suicide rates (Blüml et al., 2013; Giotakos et al., 2013; Ishii et al., 2015; Kabacs et al., 2011; Kapusta et al., 2011; Liaugaudaite et al., 2017, 2019; Ohgami et al., 2009; Oliveira et al., 2019; Palmer et al., 2019; Pompili et al., 2015; Schrauzer and Shrestha, 1990; Shiotsuki et al., 2016; Sugawara et al., 2013), 3 examined hospital admissions (Dawson et al., 1970; Pokorny et al., 1972; Voors, 1972) and 1 studied both suicide and hospital admissions (Dawson et al., 1972). One study investigated bipolar disorder, dementia and major depression (Parker et al., 2018). Another study examined bipolar disorder, schizophrenia and schizophrenia spectrum disorder (Schullehner et al., 2019). The three case–control studies investigated the rates of suicide (Knudsen et al., 2017), dementia (Kessing et al., 2017a) and bipolar disorder (Kessing et al., 2017b), respectively. In terms of cross-sectional studies, one investigated depressive symptoms and suicidal ideation (Ando et al., 2017), another investigated depressed mood (Oliver et al., 1976), one examined depression and anxiety symptoms (Shiotsuki et al., 2008) and the fourth psychotic experiences (Shimodera et al., 2018). The mean lithium concentration in the studies ranged from 0.48 to 27.4 μg/L, and the sample size from 43 to 17.2 million. The regions included in each study ranged from 1 to 276, with a mean of 99. Eleven studies came from Europe (Giotakos et al., 2013; Kabacs et al., 2011; Kapusta et al., 2011; Kessing et al., 2017a, 2017b; Knudsen et al., 2017; Liaugaudaite et al., 2017, 2019; Oliveira et al., 2019; Pompili et al., 2015; Schullehner et al., 2019), nine from the United States (Blüml et al., 2013; Dawson et al., 1970, 1972; Oliver et al., 1976; Palmer et al., 2019; Parker et al., 2018; Pokorny et al., 1972; Schrauzer and Shrestha, 1990; Voors, 1972) and seven studies from Japan (Ando et al., 2017; Ishii et al., 2015; Ohgami et al., 2009; Shimodera et al., 2018; Shiotsuki et al., 2008, 2016; Sugawara et al., 2013). Studies commonly adjusted for age, gender and population size, although these were inconsistently applied and varied widely. Less common confounders included population density, urbanicity, annual mean temperature and availability of mental health services.
The quality of the included studies is shown in Supplementary Table 6. Out of the included 27 studies, 15 studies were classified as being at low risk of bias (Ishii et al., 2015; Kabacs et al., 2011; Kapusta et al., 2011; Kessing et al., 2017a, 2017b; Knudsen et al., 2017; Liaugaudaite et al., 2017, 2019; Ohgami et al., 2009; Oliveira et al., 2019; Pompili et al., 2015; Schullehner et al., 2019; Shiotsuki et al., 2016; Sugawara et al., 2013; Voors, 1972). Studies that scored higher on our scale were generally from Japan or Europe.
Systematic review
We were unable to combine data from the following studies quantitatively.
Knudsen et al. (2017) conducted a nested case–control study in Denmark investigating the incidence of suicide. Each Danish citizen’s lithium exposure was determined by concentrations in their residential drinking water and was subsequently followed for 22 years assessing for suicide incidence rates. The findings indicated no association between suicide and lithium concentrations on an individual level.
Kessing et al. (2017b) found that lithium concentrations in drinking water were not associated with the incidence of bipolar disorder in a nested case–control study. Similar findings were demonstrated by Schullehner et al. (2019) which examined a subpopulation of Kessing et al. (2017b) Danish population. Parker et al. (2018) also found no association between high lithium concentrations and the prevalence of bipolar disorder in the United States (RR = 0·95, 95% CI = [0.75, 1.21]).
Parker et al. (2018) further assessed the RR of dementia and lithium concentrations to find no correlation between the two (RR = 1.02, 95% CI = [0.85, 1.23]). However, Kessing et al. (2017a) found a non-linear association between lithium concentrations and dementia rates. In the Danish sample consisting over 70,000 individuals, they found that compared to those with the lowest lithium levels in drinking water (2.0–5.0 μg/L), dementia was more common among those exposed to lithium concentrations between 5.1 and 10.0 μg/L (IRR = 1.22, 95% CI = [1.19, 1.25]). The study found no difference among those with the lithium concentration between 10.1 and 15.0 μg/L (IRR = 0.98, 95% CI = [0.96, 1.01]), and dementia was significantly less common (IRR = 0.83, 95% CI = [0.81, 0.85]) in the highest lithium concentration group (15.1–27.0 μg/L) (Kessing et al., 2017a).
Parker et al. (2018) found no association between lithium concentrations and the prevalence of major depressive disorder (RR = 1.12, 95% CI = [0.96, 1.29]).
Among 3040 junior high school pupils aged between 12 and 15 in Japan, Ando et al. (2017) found that the increased lithium concentration was significantly correlated with reduced depressive symptoms as measured using the General Health Questionnaire (β = −0.23, standard error [SE] = 0.09, p = 0.02). However, there was no association between lithium concentration and suicidal ideation (β = −0.06, SE = 0.28, p = 0.82). Oliver et al. (1976) used the Centre for Epidemiologic Studies Depression scale and found an association between increased lithium concentration and increased rates of depressed mood in housewives and retired women (high lithium concentrations: 42.6%, low lithium concentrations: 10.7%, p < 0.01). Finally, Shiotsuki et al. (2008) measured the anxiety and depression scores using the State-Trait of Anxiety Inventory and the Profiles of Mood States Test of 43 participants before and after they ingested spring water rich in lithium. They found a significant improvement in depression (51.1 ± 7.4 to 48.8 ± 8.0, p < 0.02) and tension and anxiety scores (47.6 ± 7.2 to 45.3 ± 9.2, p < 0.01).
An initial paper from Japan found an inverse association between lithium levels in tap water and psychotic experiences in adolescents as measured by the Diagnostic Interview Schedule for Children (β = −0.37, p = 0.021) (Shimodera et al., 2018). By contrast, a Danish study (Schullehner et al., 2019) found that those exposed to the highest concentrations of lithium in drinking water were at greater risk of developing a schizophrenia spectrum disorder (IRR = 1.21, 95% CI = [1.07, 1.35]) or schizophrenia (IRR = 1.23, 95% CI = [1.05, 1.44]), compared to those exposed to the lowest concentrations of lithium. However, unlike the Japanese study, outcomes were based on clinical diagnoses rather than derived from a structured psychiatric interview.
Pokorny et al. (1972) re-analysed the findings from Dawson et al. (1970) and found that geographic proximity to hospitals was a better explanation for hospital admission rates rather than lithium concentrations. Conversely, Dawson et al. (1972) re-analysed his data from his previous paper (Dawson et al., 1970) in 1972 and found that higher lithium concentrations were associated with reduced mental health hospital admissions (r = −0.5118, p < 0.01) but suicide rates were not affected (r = −0.2354, p > 0.05). Both studies were excluded from the meta-analysis, as they re-analysed the same population existing in Dawson et al. (1970), and thus provided no additional information.
Meta-analysis
We were able to meta-analyse the following outcomes: (1) suicide rates and (2) hospital admission rates for our chosen ecological studies.
Figure 2 shows the forest plot of the association between lithium concentration and suicide rate. Fourteen longitudinal studies with over 94 million people across 1223 geographical regions were included in this analysis (Blüml et al., 2013; Giotakos et al., 2013; Ishii et al., 2015; Kabacs et al., 2011; Kapusta et al., 2011; Liaugaudaite et al., 2017, 2019; Ohgami et al., 2009; Oliveira et al., 2019; Palmer et al., 2019; Pompili et al., 2015; Schrauzer and Shrestha, 1990; Shiotsuki et al., 2016; Sugawara et al., 2013). In the primary analysis, higher lithium levels were associated with reduced incidence of suicide across the geographical regions (r = −0.191, 95% CI = [−0.287, −0.090], p < 0.001), with significant heterogeneity between studies (Q = 67.4, p < 0.001, I2 = 80.7%). These results remained significant when only high-quality studies were included (r = −0.227, 95% CI = [−0.362, −0.082], p = 0.002; Q = 54.5, p < 0.001, I2 = 81.7%) (Ishii et al., 2015; Kabacs et al., 2011; Kapusta et al., 2011; Liaugaudaite et al., 2017, 2019; Ohgami et al., 2009; Oliveira et al., 2019; Pompili et al., 2015; Shiotsuki et al., 2016; Sugawara et al., 2013), when Ohgami et al. (2009) was excluded (r = −0.168, 95% CI = [−0.263, −0.070], p = 0.001), when excluding Liaugaudaite et al. (2017) (r = −0.190, 95% CI = [−0.288, −0.088], p < 0.001), and when studies that did not provide adjusted results (Giotakos et al., 2013; Schrauzer and Shrestha, 1990) were excluded (r = −0.135, 95% CI = [−0.220, −0.048], p = 0.002). In the sensitivity analysis of each study removed in turn, the results remained significant throughout. There was also a significant indication of publication bias influencing the findings (Egger’s test; t value = 2.90, p = 0.013). Duval and Tweedie’s Trim and Fill analysis found no missing studies to left of the mean, with five studies trimmed to the right of mean with adjusted values (r = −0.080, 95% CI = [−0.188, 0.029]).
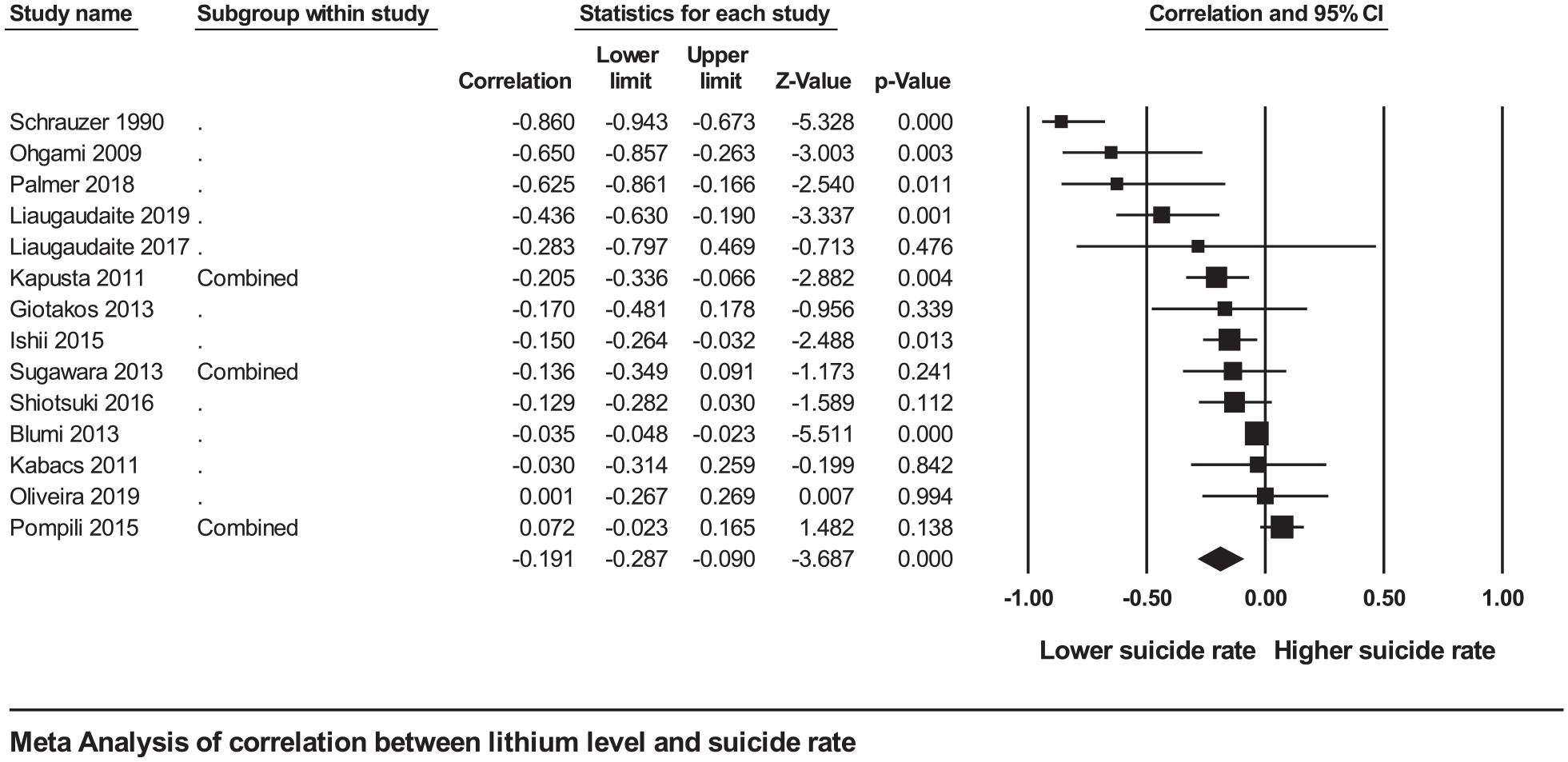
Forest plot of the meta-analysis between lithium in drinking water and suicide rates in the most adjusted models for the association between lithium in drinking water and neuropsychiatric outcomes: a systematic review and meta-analysis from across 2678 regions containing 113 million people.
The funnel plot for publication bias with imputed missing studies is provided as Supplementary Figure 1. A meta-regression analysis of eight studies reporting mean lithium concentrations ranging between 3.8 and 11.5 μg/L found no significant association of mean lithium levels and suicide rates (Giotakos et al., 2013; Ishii et al., 2015; Kapusta et al., 2011; Liaugaudaite et al., 2017, 2019; Oliveira et al., 2019; Pompili et al., 2015; Shiotsuki et al., 2016).
Two studies of over 5 million people were included in the meta-analysis of lithium levels and psychiatric hospitalisations (Dawson et al., 1970; Voors, 1972). We found that increased lithium concentration was associated with reduced hospital admissions (r = −0.413, 95% CI = [−0.689, −0.031], p = 0.035) (Figure 3). Sub-analyses showed only admissions for neurotic disorders were significantly reduced (r = −0.526, 95% CI = [−0.643, −0.385], p < 0.001) (Supplementary Figure 2), while admissions for personality (r = −0.358, 95% CI = [−0.754, 0.229], p = 0.227) (Supplementary Figure 3) and psychotic outcomes (r = −0.327, 95% CI = [−0.734, 0.253], p = 0.266) (Supplementary Figure 4) were both non-significant.
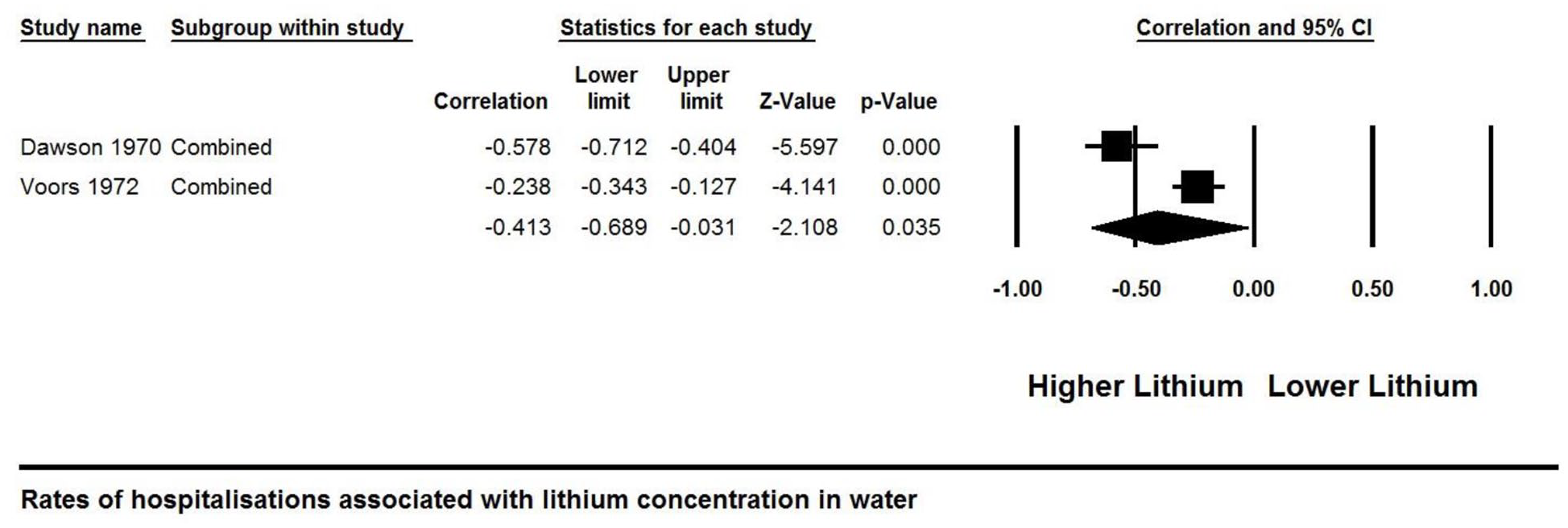
Forest plot of the meta-analysis between lithium in drinking water and hospital admissions for the association between lithium in drinking water and neuropsychiatric outcomes: a systematic review and meta-analysis from across 2678 regions containing 113 million people.
Discussion
Findings
In our meta-analysis, we found that higher lithium concentrations were associated with reduced suicide rates and hospital admissions. This inverse relationship with suicide rates and hospital admissions was seen in seven studies and two studies, respectively. There was no observable dose–response relationship between lithium concentrations and suicide rates. We also found in our systematic review that while some studies suggested improvement in depression and anxiety symptoms scales, there was mixed evidence for dementia and psychosis rates and no association between lithium concentration and the rates of bipolar disorder or major depressive disorder.
Our main findings are mostly consistent with previously published studies that investigated sources of lithium in the environment other than drinking water. For example, König et al. (2017) demonstrated lower suicide rates in regions where higher concentrations of lithium were found in Chilean soil. In a randomised controlled trial, microdoses of lithium were shown to have positive mood effects when provided as an oral supplement (Schrauzer and de Vroey, 1994). Furthermore, higher lithium levels in drinking water significantly reduced the prevalence of depressive temperament in Japan (Ishii et al., 2018). A similar systematic review and meta-analyses found lithium in drinking water were dose-dependently associated with reduced suicide mortality (Barjasteh-Askari et al., 2020). However, this review was limited by the fact that the authors used unadjusted effect sizes and did not explore outcomes beyond suicide.
Our findings are also consistent with those relating lithium macro-doses with suicide. In a recent meta-analysis, Cipriani et al. (2013) found that using long-term lithium therapy in mood disorders significantly reduced the risk of suicide. These findings were supported by more recent studies (Lewitzka et al., 2015; Smith and Cipriani, 2017).
While its exact anti-suicidal mechanism of action remains uncertain, lithium’s effect on the brain appears to be multi-faceted. These include reducing impulsive and aggressive behaviours (Müller-Oerlinghausen and Lewitzka, 2016), increasing glutamine synthetase expression (Kalkman, 2011) and improved decision-making in those with mood disorders (Adida et al., 2015). Other effects include increasing the availability of vitamin B12 which may improve mood (Schrauzer et al., 1992) and reducing testosterone levels which may reduce suicidality in men (Sher, 2015).
Lithium’s neurobiology has also been a topic of intense research given its ability to affect multiple cellular pathways and expression of hundreds of genes (Bauer and Gitlin, 2016; Malhi et al., 2012; Rybakowski, 2020). Lithium-induced inhibition of glycogen synthase kinase 3β restores neurotransmission and corrects cellular dysfunction, which may underpin lithium’s mood stabilising, suicide-preventing and neurocognitive properties (Beurel and Jope, 2014; Malhi and Outhred, 2016; Malhi et al., 2012, 2018a). In addition, lithium’s effect on inositol monophosphatase influences neuroprotection by enhancing cell survival (Bauer and Gitlin, 2016). Lithium also stimulates neurotrophic factors, brain-derived neurotrophic factor and vascular endothelial growth factor (Forlenza et al., 2014) and has been found to influence the neuropathology of dementia (Bauer and Gitlin, 2016).
Lithium appears to modulate genes involved in neuroprotection, neuronal plasticity and other neuronal functions including neurotrophy (Malhi et al., 2012). This was further shown in a recent study where magnetic resonance imaging (MRI) scans showed increased grey matter, putamen, hippocampal and thalamic volumes in patients taking lithium as a consequence of lithium-induced gene expression (Anand et al., 2020). Further neuroprotection is evidenced as lithium prevents stress-induced dendritic damage (Wood et al., 2004) and shows anti-apoptotic activity (Bachmann et al., 2009; Chen and Chuang, 1999). Subtherapeutic lithium levels demonstrate anti-inflammatory properties by modulating the secretion of pro-inflammatory and anti-inflammatory cytokines in hippocampal and cortical neurons (De-Paula et al., 2016). The above-described neuroprotective properties may be apparent in those with and without mood disorders (Bauer and Gitlin, 2016), possibly at subtherapeutic levels (Vo et al., 2015).
Combining these multi-faceted mechanisms with a study showing animal models can accumulate lithium intracellularly (Foulks et al., 1952), it is plausible that long-term intake of subtherapeutic doses of lithium may reduce suicide and have additional neuropsychiatric benefits.
We further postulate that the anti-suicidal effect of lithium may not be as closely dose-dependent as its mood stabilising effects. For example, it has been previously discussed that lithium may demonstrate an anti-suicidal effect without having mood stabilising effects (Terao et al., 2009). A significant reduction in suicidal attempts has been noted among patients with affective disorders on lithium even if they do not have improvement in mood symptoms (Ahrens and Müller-Oerlinghausen, 2001).
Strengths and limitations
To our knowledge, this is the first systematic review and meta-analysis to examine the association between lithium concentrations in drinking water and rates of multiple neuropsychiatric outcomes. Our review included over 113 million subjects from 27 studies in nine different countries. That said, some important limitations need to be mentioned.
First, we emphasise the presence of publication bias within the meta-analysis and have tried to address this as follows. We investigated its presence using Egger’s test, Duval and Tweedie’s Trim and Fill analysis. We further examined the funnel plot for visual inspection.
In the absence of mandatory pre-registration, epidemiological studies such as those included here may be vulnerable to the ‘file-drawer problem’, thus increasing the possibility of publication bias. This, however, may occur both ways. A finding of no association between differences in drinking water lithium concentrations and mental health outcomes may not be considered sufficiently novel by researchers or journal editors to warrant publication. Conversely, journals may favour publishing papers with null findings, as some viewers may find lithium’s purported effects at such low concentrations to be implausible.
Future studies using pre-registered analyses are recommended to further explore the association between lithium and reduced suicide rates. Further analysis of publication bias present in this topic of literature would also be useful.
The formula for deriving r from the standardised coefficient was based on a previously published formula where validation was based on a range of β values between −0.5 and 0.5 where most of the data points were. Our results for values outside that range should be treated with caution. However, the results remained significant in a sensitivity analysis of the effects of only including β values between −0.5 and 0.5.
There was significant heterogeneity between studies, and as such these results should be treated with caution in both the size and the direction. We have attempted to address this using random effects models throughout, as well as undertaking sensitivity and subgroup analyses, as well as meta-regression.
Our results must also consider the ecological fallacy, being correlations found at a population-based level cannot be assumed to have the same effect on an individual-based level (Robinson, 1950). In the context of our findings, while the increased lithium concentration in drinking water is associated with the reduced risk of suicide or hospital admission at a population level, it is unknown whether any given particular individual’s susceptibility for suicide or hospital admission is improved.
In addition, many included studies also suffered from the lack of ascertainment of neuropsychiatric outcomes and low quality of descriptive statistics reported as evidenced in the quality appraisal. For example, the two studies that examined hospital admission rates were both from the 1970s and so may be less applicable to current practice or the availability of beds (Dawson et al., 1970; Voors, 1972). Even in the 1970s, hospital accessibility was suggested as a more plausible explanation than the effect of lithium concentration (Pokorny et al., 1972). Further contemporary research is required to better establish our hospital admissions results given only two older studies could be meta-analysed.
It should also be noted that suicide is the product of multiple factors including genetic, biological, psychosocial and environmental (Hawton and van Heeringen, 2009). While some of these potential confounders have been adjusted for in the included studies, they were not consistent between studies as was the methods of ascertaining lithium-level concentrations and the measurements used to report suicide and lithium levels. Despite this, we believe our methodology is robust enough to allow us to meta-analyse some of the findings.
Supplementation of drinking water with lithium may offer a cheap and effective opportunity to reduce the distressing symptoms and costly burden of neuropsychiatric outcomes. Although our findings suggest potential benefit, especially in suicide and hospital admissions, further research is needed to confirm these results. Safety of utilisation is of particular uncertainty, considering excessive lithium concentrations in drinking water may be associated with a number of physical complications such as compromised thyroid function (Broberg et al., 2011; Harari et al., 2015a), disruption of vitamin D and calcium homeostasis in pregnant women (Harari et al., 2016) and impaired birth size (Harari et al., 2015b). High concentrations in bottled water could also cause lithium toxicity in those already prescribed lithium (Dabeka et al., 2002). To better discern the net benefits of lithium in drinking water, future research should also focus on the precise concentration of lithium that provides the most significant neuropsychiatric benefit while demonstrating no substantial harms at the population and individual level.
Given the recent controversy around fluoridation (Green et al., 2019), there may also be broader clinical, societal and philosophical objections to adding a further element to the water supply. There may also be greater resistance to a measure to promote mental as opposed to dental health. Adding lithium to bottled water would allow greater individual choice but equally disadvantage those on low incomes. The economic and environmental effects should also be considered. For instance, there is laboratory evidence for the harmful effect of lithium on marine life (Shahzad et al., 2017), but data from the environment are more limited and generally confined to areas of high industrial pollution (Mathis and Cummings, 1973; Shahzad et al., 2017).
Conclusion
Our findings suggest that higher concentrations of lithium in drinking water may be associated with reduced suicide rates and psychiatric hospital admission. The effect on other neuropsychiatric outcomes is less clear. Further research is necessary on the risks and benefits of lithium in the water on neuropsychiatric and physical health outcomes before any public health recommendations could be made.
Supplemental Material
20200825_Lithium_Supplementary_tables_and_figures.docx – Supplemental material for The association between lithium in drinking water and neuropsychiatric outcomes: A systematic review and meta-analysis from across 2678 regions containing 113 million
Supplemental material, 20200825_Lithium_Supplementary_tables_and_figures.docx for The association between lithium in drinking water and neuropsychiatric outcomes: A systematic review and meta-analysis from across 2678 regions containing 113 million by Brenton Eyre-Watt, Eesharnan Mahendran, Shuichi Suetani, Joseph Firth, Steve Kisely and Dan Siskind in Australian & New Zealand Journal of Psychiatry
Footnotes
Author Contributions
B.E.-W., E.M., S.S., J.F., S.K. and D.S. designed the study. B.E.-W. and E.M. extracted all data. B.E.-W., D.S., S.K. and J.F. analysed the data. B.E.-W., E.M. and S.S. wrote the initial draft. All authors participated in the revision of the text and approved the final version of this paper. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: All authors have completed the ICMJE uniform disclosure form at ![]() and declare no support from any organisation for the submitted work; J.F. is supported by a Blackmores Institute Fellowship; no other relationships or activities that could appear to have influenced the submitted work.
and declare no support from any organisation for the submitted work; J.F. is supported by a Blackmores Institute Fellowship; no other relationships or activities that could appear to have influenced the submitted work.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Data Sharing Statement
Relevant study data can be found in the online supplementary files. Further statistical data are available on request to the corresponding author with publication, indefinitely for anyone that wishes to access the data, for any purpose.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.