
Abstract
Objective:
Continued engagement with primary mental health services has been associated with the prevention of subsequent suicidal behaviour; however, there are few studies that identify determinants of treatment disengagement among those at risk of suicide in primary care settings. This study investigated determinants of treatment disengagement of those at risk of suicide who were referred to primary mental health care services in Western Sydney, Australia.
Method:
This study used routinely collected data of those referred for suicide prevention services provided through primary mental health care services between July 2012 and June 2018. Associations between sociodemographic, diagnostic, referral- and service-level factors and treatment non-attendance and early treatment cessation were investigated using a series of multivariable generalised estimation equations.
Results:
There were 1654 suicidal referrals for 1444 people during the study period. Those identified with a risk of suicide were less likely to never attend treatments (16.14% vs 19.77%), but were more likely to disengage earlier from subsequent service sessions (16.02% vs 12.41%), compared to those with no risk of suicide. A higher likelihood of non-attendance to any primary mental health care service sessions was associated with those aged 25–44, lower socioeconomic status, a presentation for substance use and a referral from acute care (either emergency department or hospital). Among those who attended an initial treatment session, younger age (18–24 years) and a longer waiting time for an initial follow-up appointment were associated with a higher likelihood of early treatment cessation from primary mental health care services.
Conclusion:
These findings can inform potential strategies in routine primary mental health care practice to improve treatment engagement among those at risk of suicidal behaviour. Youth-specific interventions, behavioural engagement strategies and prompt access to services are policy and service priorities.
Keywords
Introduction
Suicide continues to be a significant public health issue in Australia and remains the leading cause of mortality among those aged 15–44 years in Australia (Australian Institute of Health and Welfare, 2019). Suicide and non-fatal self-harm contribute a significant impact to the community and health system; however, timely access to suicide prevention services and mental health support can reduce the likelihood of potential suicidal behaviour (Motto and Bostrom, 2001; World Health Organization, 2014). Over the last two decades, the Australian government has made substantial investments in providing wider access to mental health support and suicide prevention services for those at risk of suicide. For example, nearly $10 billion was allocated for all primary and acute care mental health services in 2017–2018 (Australian Institute of Health and Welfare, 2020) and $49 million for the national suicide prevention strategy in 2015–2016 (Australian Institute of Health and Welfare, 2018).
Despite significant investments in providing wider access to mental health and suicide prevention services, the burden associated with suicidal behaviour has not changed substantially in the Australian context (Jorm, 2018). A greater emphasis on treatment disengagement in facilitating adequate access to suicide prevention services has been suggested (Appleby et al., 1999; Irigoyen et al., 2019; Lizardi and Stanley, 2010), and recent modelling has suggested that interventions to re-connect with those who disengage with services could potentially reduce both suicide and attempted suicide (Page et al., 2018).
Previous research has suggested that risk of suicide may increase the likelihood of treatment disengagement, compared to people at no risk of suicide, and that those at risk of suicide are more likely to abandon follow-up services (Clark and Fawcett, 1992; Di Bona et al., 2014). Identifying the characteristics among those at risk of suicide who are more likely to disengage with mental health services can inform strategies to facilitate continued contact with services. However, there are few studies that investigate factors associated with disengagement among those who are assessed as being at risk of suicide (Hom and Joiner, 2017), with most studies focussing on individuals referred to mental health services in general. It is not clear whether the sociodemographic, economic and service-level factors (Fenger et al., 2011; Kruse and Rohland, 2002; Marshall et al., 2016; Mitchell and Selmes, 2007; Reitzel et al., 2006; Self et al., 2005) associated with treatment disengagement in these studies are similar among individuals assessed as being at risk of suicide. This is important given the strong association between previous non-fatal self-harm and subsequent suicide (Carroll et al., 2014; Owens et al., 2002; Suominen et al., 2004) and the potential benefits of interventions that facilitate ongoing connection with services to reduce the risk of suicide (Hvid et al., 2011).
Accordingly, this study investigated the association between sociodemographic, diagnostic, referral- and service-level factors and treatment disengagement among those at risk of suicide in the population catchment of Western Sydney (Australia).
Methods
Design and procedures
This study was based on the Western Sydney PHN population catchment which covers four local government areas including Blacktown, Parramatta, Cumberland and Hills Shire in the western suburbs of Sydney, Australia. There were approximately 1 million people residing in this region, with a high proportion of people from culturally and linguistically diverse backgrounds (WentWest Primary Health Network, 2018). Routinely collected data on those aged ⩾18 with risk of suicide (see below) and who were referred to primary mental health care (PMHC) services (see below) during July 2012 to June 2018 were included in this study. The data used in this study were accessed in accordance with approval from the Western Sydney Human Research Ethics Committee (Approval No-H13040).
PMHC services
PMHC services considered in this study were federal government initiatives established to provide wider access to mental health support for those who otherwise would have no, or limited, access to mental health services. The Better Outcomes in Mental Health Care (BOiMHC) programme was established in 2001 (Hickie and Groom, 2002), and as part of this programme, GPs were provided incentives to work collaboratively with allied mental health professionals to refer people experiencing mild to moderate common mental health conditions under the Access to Allied Psychological Services (ATAPS) in 2003.
These services were complimented by other services from 2008, under ATAPS tier II, which targeted specific subpopulations and provision of suicide prevention services (Reifels et al., 2013). ATAPS services were first delivered through Divisions of General Practice, prior to these Divisions being reformed as Medicare Locals in 2011 (Department of Health, 2015). Recommendations from a major review of mental health services in 2014 shifted access to mental health and suicide prevention services to a regional level administered by primary health network (PHNs) in 2016 (National Mental Health Commission, 2014). Current PMHC services are provided under six main treatment areas including (1) low-intensity psychological interventions to those with mild mental health conditions, (2) psychological therapies delivered by mental professionals, (3) early interventions for youth and children, (4) treatments for those with severe and complex mental health conditions, (5) Indigenous-specific mental health conditions and (6) suicide prevention services.
Risk of suicide
Individuals were assessed to be at ‘risk of suicide’ and eligible for referral to PMHC services if they (1) presented to primary care following being discharged from an emergency department (ED) or hospital following a non-fatal suicide attempt or intentional self-harm, (2) presented to a GP or primary care setting following a non-fatal suicide attempt or intentional-self harm or (3) presented to a GP or other primary care setting expressing strong suicidal ideation. Those who were assessed to be at immediate risk of suicide were not referred to PMHC services, but were referred to acute care services (Australian Government Department of Health and Ageing, 2012).
Service disengagement
Disengagement with PMHC services was categorised as (1) those who were referred to PMHC services, but who never attended any sessions (service non-attendance); and (2) those who were referred to PMHC services but who discontinued after one or more sessions (service disengagement). This distinction was made based on previous research suggesting different associations for each of these groups by sociodemographic, economic, clinical and treatment-level variables (Fenger et al., 2011; Mitchell and Selmes, 2007).
It should be noted that there is no universal definition describing service disengagement. Previous studies of service disengagement from mental health services indicate that there are a number of methodological differences in terms of how service disengagement is defined (Barrett et al., 2008) and that inconsistencies in associations between sociodemographic and clinical factors and service disengagement partly reflect these different definitions.
Suicide prevention services provided by the PMHC programme provide an unlimited number of sessions for a short period (a 2-month period according to programme guidelines, but a most recent evaluation indicated 90% of those completed treatment within 3 months; (Nicholas et al., 2019), with those benefitting from PMHC services also likely to continue psychological treatment under a new non-suicide referral.
However, the reasons for closing an episode of contact were also poorly documented in the PMHC data. It was not possible to determine whether the non-attendance at subsequent sessions was mutually agreed between clinician and client, or whether this represented a discontinuation of service use. Previous research has been defined minimally adequate treatment for psychological therapy as receiving six or more sessions (Harris et al., 2015), and further recommendations indicated the need of 3–12 sessions to reduce the risk of self-harm among those over 8 years of age at risk of suicide (National Institute for Health and Care Excellence, 2011). Based on this evidence, and treatment guidelines about the number of sessions under suicide prevention services, it was assumed that a person who discontinued services before the third session would be unlikely to have recovered or reduced their risk of suicide. Therefore, this study defines failure of attendance more than 2 sessions among those initiated treatments as ‘early cessation’, and treatment disengagement considers as two distinct events (1) service non-attendance (never attended a session) and (2) early cessation of services (attended 1–2 sessions only).
Data sources
This study extracted data from two main data sources: (1) the PMHC minimum data set (MDS) and (2) the ATAPS MDS. The PMHC MDS was developed based on the ATAPS MDS, but collects a broader range of data items relevant to all mental health services than the ATAPS MDS. Both the ATAPS and PMHC MDS comprise items relating to key demographic and socioeconomic information, mental health diagnostic and referral- and service-level information. Since the establishment of the PMHC MDS in July 2016, all ATAPS data were combined with the PMHC MDS in July 2017 and the ATAPS MDS was no longer used after August 2018. Hereafter, the generic term ‘PMHC’ is used in this study to refer to mental health services. The Index of Socioeconomic Disadvantage (IRSD) for census years 2011 and 2016 were also obtained to classify each postcode of residence in the PMHC data sources (Australian Bureau of Statistics, 2018), and intercensal IRSD values calculated by weighted interpolation using the formula IRSD_i = IRSD_2016 + (IRSD_2016 – IRSD_2011)/(2016–2011) × (i-2016), for a given year ‘i’ between 2012 and 2018.
Study variables
The outcome for this study was service disengagement among those referred to PMHC services, defined mainly as two binary variables: (1) service non-attendance (never attended a session vs attended at least one session) and (2) early cessation of services (attended 1–2 sessions only vs attended > 2 sessions).
A series of time-dependent and time-independent variables were specified as covariates. Sociodemographic variables included gender (male, female), age group (18–24, 25–44, 45+), main language spoken at home (‘English’, ‘other’), English-language proficiency (‘very good’, ‘not very good’) and marital status (‘never married’, ‘married or De facto’, ‘divorced, separated or widowed’). Socioeconomic status (SES) variables included employment status (‘not employed’, ‘part time employed’, ‘full time employed’) and the area-based IRSD (categorising postcode of usual area of residence into population quintiles from ‘most deprived’ to ‘least deprived’).
A series of variables relating to the characteristics of the initial presentation were also defined. These variables included source of referral (‘emergency department or hospital’, ‘general practice’, ‘public mental health services or other’), presenting diagnosis (‘anxiety’, ‘depression’, ‘anxiety and depression’, ‘substance use disorder (either presented as the main diagnosis or as a comorbid condition)’, ‘other’) and current psychotropic medication use (‘yes’ or ‘no’). Psychotropic medications recorded on the PMHC MDS included ‘antidepressants’, ‘antipsychotics’, ‘anxiolytics’, ‘psychostimulants and nootropics’ or ‘hypnotics and sedatives’.
Service-level variables included previous service use either suicide-related PMHC services or other PMHC services (‘yes’, ‘no’) and waiting time to initiate the first treatment session (<7 days, 1–2 weeks, >2 weeks).
Statistical analysis
Preliminary analyses examined counts and percentages for each study outcome, stratified by the study factors described above. Generalised estimating equations (GEEs) with a logit link and exchangeable correlation matrix were employed to model the univariate and multivariate associations between time variant and invariant covariates and service disengagement outcomes (Hanley et al., 2003). Four models were fitted, including univariate and multivariate, to examine the effect of covariates on the service disengagement. ‘Marital status’ and ‘employment participation’ were not available in the ATAPS MDS; therefore, associations for service disengagement were restricted to PMHC MDS for these variables.
Missing data was evident for several variables, and over a quarter of observations were not available in the complete case multivariable GEE models to predict both treatment non-attendance (28.1%) and early cessation of services (28.4%). We performed multiple imputation using chained equations with 50 imputation cycles using MICE package in R (Buuren and Groothuis-Oudshoorn, 2010) under the assumption of data were missing at random to maximise the available information. Effect sizes of associations based on univariate GEE models were similar between non-imputed and imputed data (Models 1 and 3 in Table 2 and Models 1 and 3 in Supplementary Table 1). All the analyses were conducted using STATA 14.0 (StataCorp, TX, USA) and R version 3.6.0.
Results
There were 1654 suicide referrals made for 1444 individuals, and 9710 non-suicidal referrals made for 8225 individuals, for PMHC services over the period July 2012 to June 2018. Of these suicidal referrals, 16% did not attend any service sessions, and another 16% attended 1–2 sessions only, while only two-thirds of the referrals continued for more than two sessions. In comparison to non-suicide referrals, suicide referrals were less likely to never attend any treatment sessions (19.7% vs 16.1%), but were more likely to disengage earlier (before the third session) from PMHC services (12.4% vs 16.0%) (Figure 1).
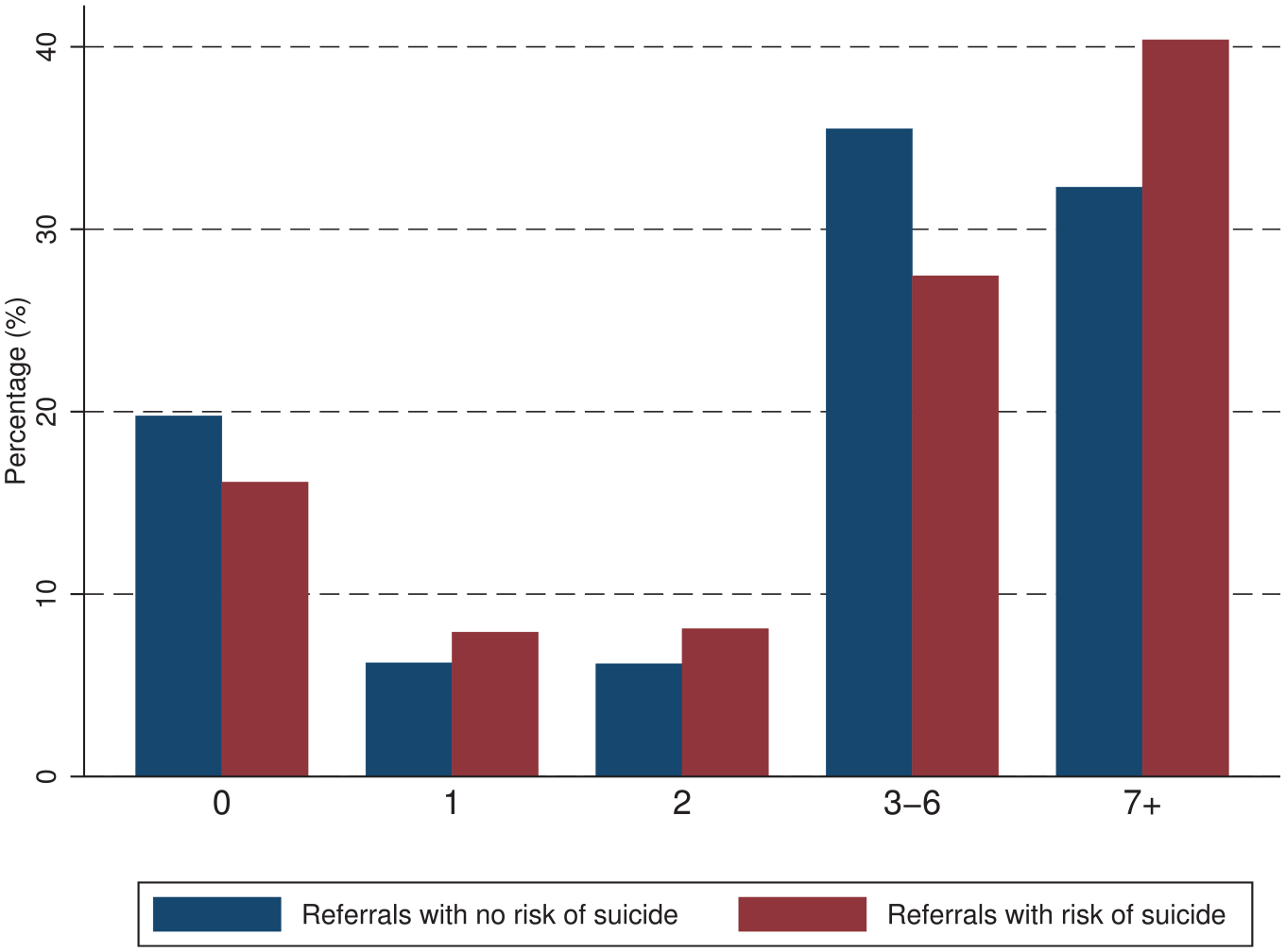
Number of primary mental health care service sessions: suicide vs non-suicide referrals (Western Sydney population catchment, 2012–2018).
A higher proportion of suicide referrals were evident among females (58.4%) than males (41.6%), and just under half of referrals were for those aged 25–44 years. Nearly 20% of those were residing in the most deprived areas, and General Practice settings were the main source of suicide referrals (59%), followed by public mental health or other organisations (35.9%) (Table 1). The majority of referrals presented to services with an affective disorder (30.7%), or co-morbid affective and anxiety disorder (26.3%), as the principal diagnosis. Nearly half of referrals initiated service sessions within the first week of the referral, and nearly 43% used a mental health medication at the time of being referred (Table 1).
Sociodemographic, diagnostic and referral-level profile and treatment engagement among those with suicide risk referred to PMHC services between 2012 and 2018.
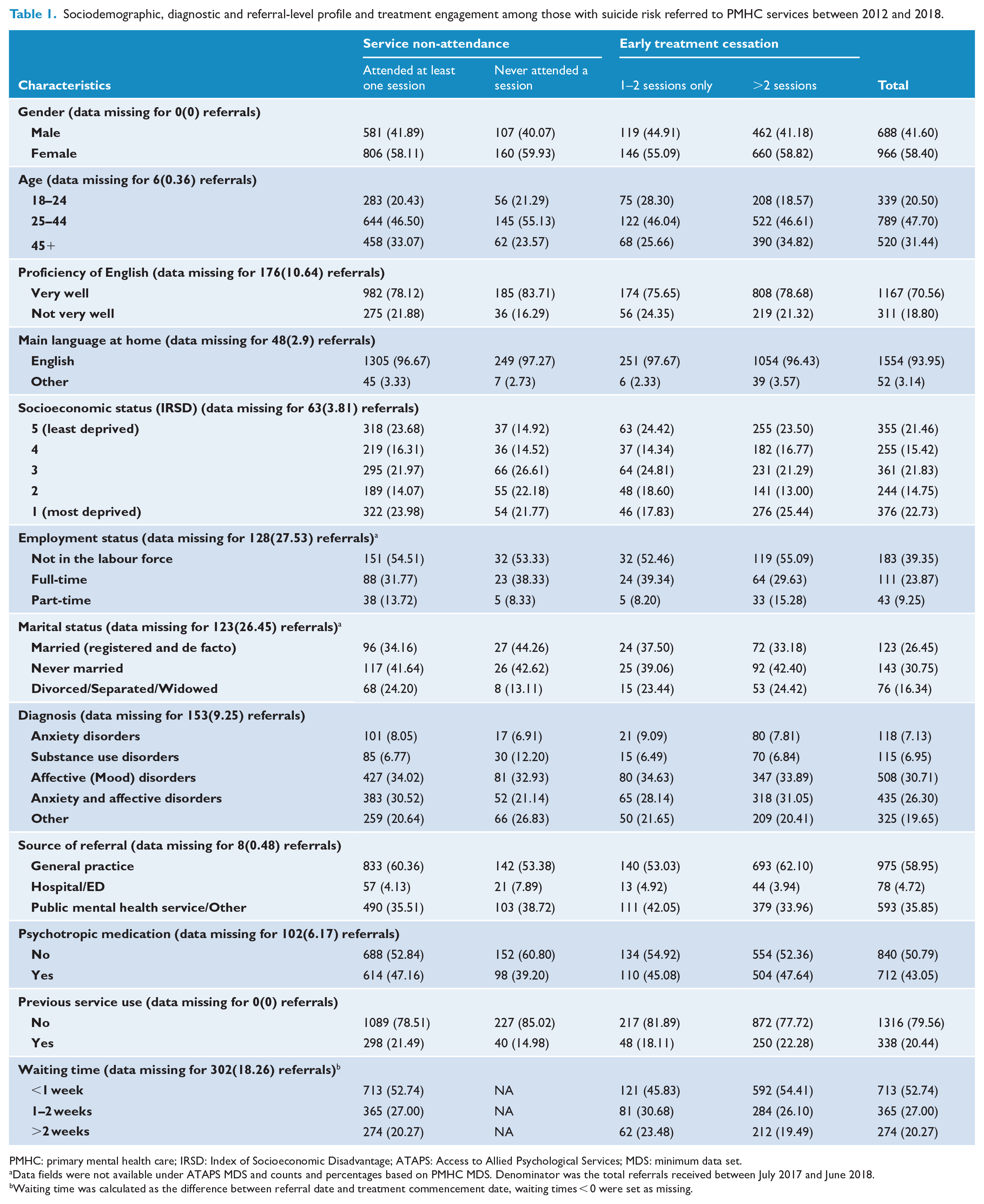
PMHC: primary mental health care; IRSD: Index of Socioeconomic Disadvantage; ATAPS: Access to Allied Psychological Services; MDS: minimum data set.
Data fields were not available under ATAPS MDS and counts and percentages based on PMHC MDS. Denominator was the total referrals received between July 2017 and June 2018.
Waiting time was calculated as the difference between referral date and treatment commencement date, waiting times < 0 were set as missing.
Those at risk of suicide who never attended a service session were more likely to be aged 25–44 years, compared to the age group 45+ (odds ratio [OR] = 1.48, 95% confidence interval [CI] = [1.07, 2.06]), presented with a substance use disorder (compared to anxiety disorders) (OR = 2.07, 95% CI = [1.05, 4.09]), lived in lower socioeconomic areas (ORs ranging from 1.36 to 2.13) (compared to highest socioeconomic quintile) and were referred from an acute care hospital setting (OR = 1.79, 95% CI = [1.01, 3.17]) (Table 2 and Figure 2).
Risk of non-attendance and treatment cessation by sociodemographic, diagnostic and health service-level factors referred to PMHC services between 2012 and 2018.
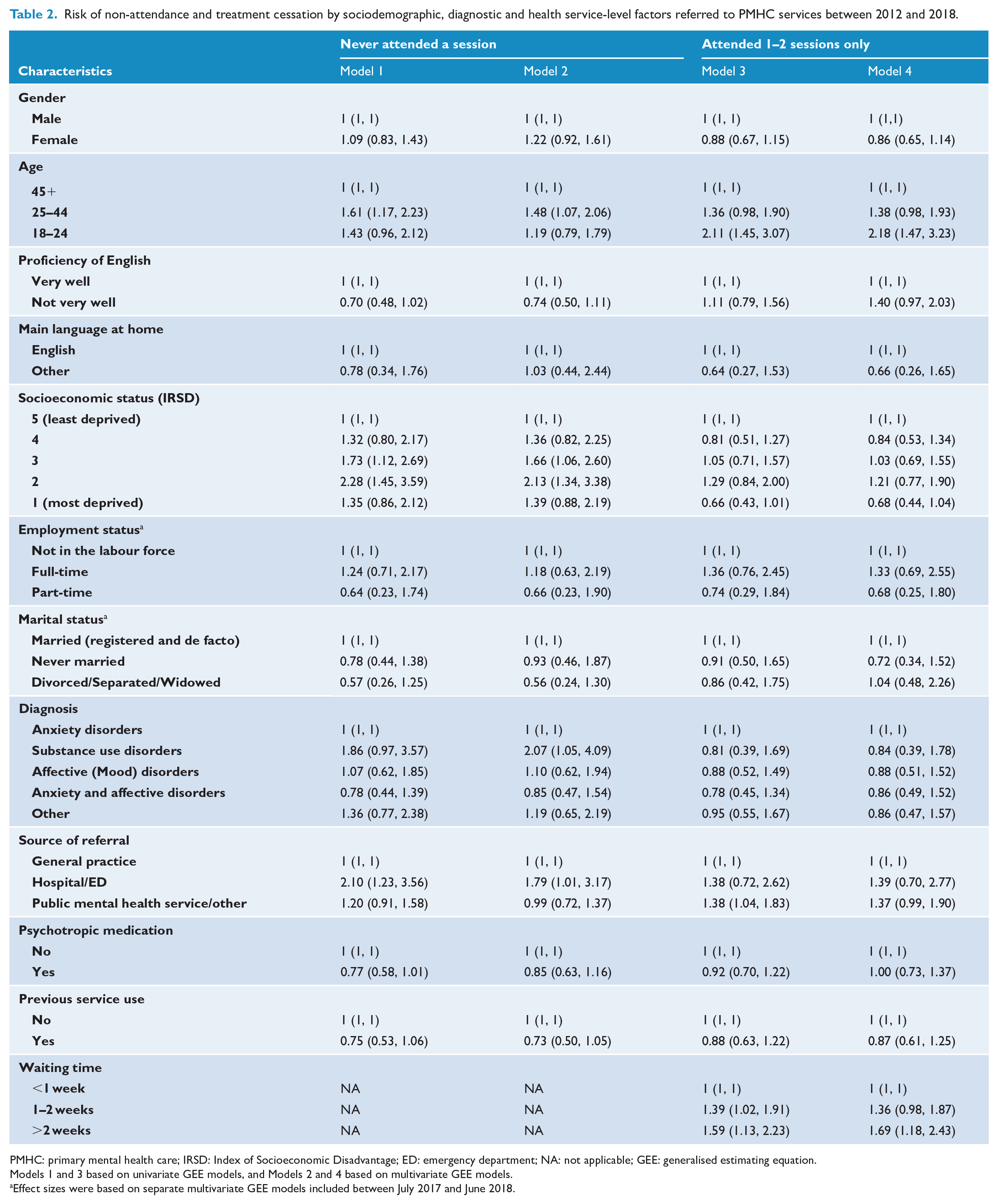
PMHC: primary mental health care; IRSD: Index of Socioeconomic Disadvantage; ED: emergency department; NA: not applicable; GEE: generalised estimating equation.
Models 1 and 3 based on univariate GEE models, and Models 2 and 4 based on multivariate GEE models.
Effect sizes were based on separate multivariate GEE models included between July 2017 and June 2018.
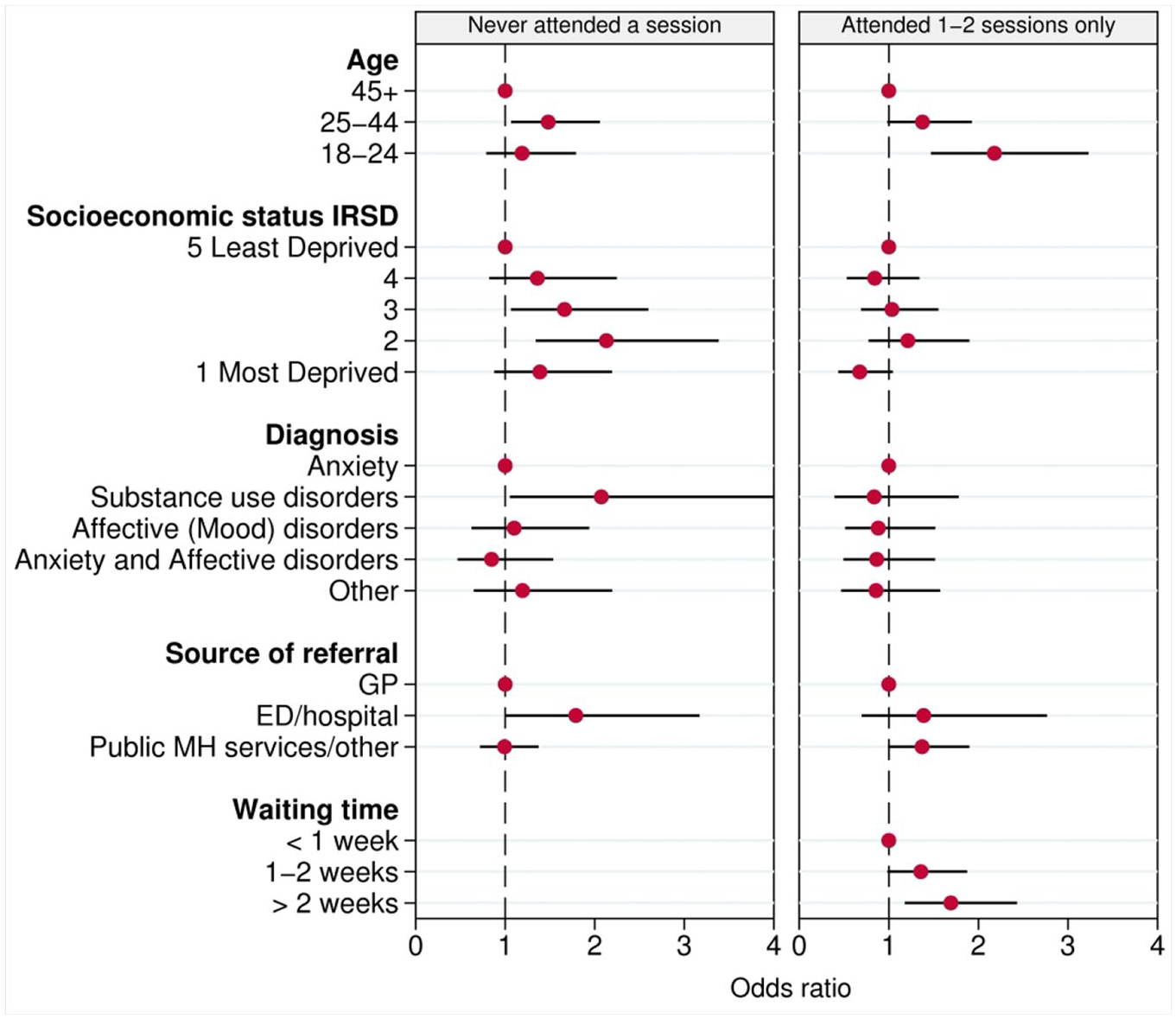
Determinants of treatment non-attendance and early cessation of those referred to PMHC services between 2012 and 2018 (odds ratio and 95% confidence interval).
Factors associated with early treatment cessation after 1–2 service sessions included longer waiting times >2 weeks to receive first treatment session (OR = 1.69, 95% CI = [1.18, 2.43]) compared to ‘<1 week’, and younger age (age 18–24) (OR = 2.18, 95% CI = [1.47, 3.23]), compared to those aged 45+ (Table 2 and Figure 2). Similar associations were observed for those who attended only one treatment sessions (Supplementary Table 2).
Discussion
This study investigated determinants of treatment disengagement among those at risk of suicide who were referred to PMHC services in Western Sydney, Australia. Overall, 16% of those assessed as at risk of suicide did not attend services, which was slightly higher than the national estimate of 14% (Nicholas et al., 2019). In total, nearly one-third of referrals attended a service with no more than three treatment sessions (16% never attended and another 16% did not attend more than 2 treatment sessions). The average number of sessions per referral was also higher than national estimates (6.75 > 5.5) (Nicholas et al., 2019).
Findings also indicated differential associations among service non-attendance and early cessation of service and exposure variables among those with risk of suicide, similar to previous studies of service disengagement from mental health services (Fenger et al., 2011; Mitchell and Selmes, 2007). Younger age, socioeconomic deprivation, substance use and referral from an acute setting or ED were associated with service non-attendance, while younger age and longer waiting time were associated with early service cessation.
Those who were younger in age (age < 45) were more likely to disengage with services, particularly those aged 25–44 years who were more likely to never attend any treatment sessions, while young adults (age 18–24) were more likely to terminate services prematurely, compared to the older age groups (age 45+). This finding is consistent with treatment engagement among those with mental health conditions who were referred for psychological treatments (Mitchell and Selmes, 2007). Attitudinal barriers, such as negative perceptions about the efficacy of treatments and perceptions that it is easier to manage problems alone or seek help from informal sources such as peers, have been identified as common barriers to care among those at risk of suicide (Bruffaerts et al., 2011; Mok et al., 2020), with these perceptions being more prevalent among younger age groups (Rickwood et al., 2007).
Sociodemographic variables such as gender, marital status and employment status were not strongly associated with service non-attendance or early service cessation, similar to previous studies (Hom and Joiner, 2017). However, our findings indicated, although not significant in 95% confidence level, those with poorer English-language skills were more likely to attend for an initial treatment session, but were also more likely to disengage with services prematurely. English-language barriers are common among those with non-English backgrounds and may create difficulties in persevering with mental health services. This study also found low SES was associated with a lower likelihood of attendance at the initial service session, and perhaps a reflection of locational disadvantage, transportation barriers and distance (Alonzo et al., 2016; Bruffaerts et al., 2011). However, SES was not associated with service cessation among those who initiated treatments.
Those clients presenting with substance abuse were less likely to attend for an initial treatment session, and this finding is consistent with an extensive body of literature on treatment engagement in primary care research (Hom and Joiner, 2017; Mitchell and Selmes, 2007). Substance dependence alone, or co-morbid with other conditions, impairs the level of daily functioning and presents additional burden on treatment-seeking behaviour (Mitchell and Selmes, 2007). In contrast to a recent study of treatment dropout among those with clinically significant suicidal ideation (Hom and Joiner, 2017), our study did not find substance use disorders to be associated with early treatment cessation, likely a reflection of the definition of treatment cessation (Barrett et al., 2008; Swift and Greenberg, 2012). For example, Hom and Joiner (2017) defined treatment cessation as unilateral termination of treatments, and this group also included those who did not attend any treatment sessions (Hom and Joiner, 2017). In this study, service non-attendance and early service cessation were considered as two separate events.
Despite the referral to receive PMHC service, a failure to attend the initial service session was higher among those referred from hospital or ED settings. This is also the group of clients who are more likely to attend an ED or be admitted to hospital following attempted suicide. Those who admitted to the hospital following a suicide attempt are also more likely to have higher levels of distress, hopelessness and previous history of suicidal behaviour, which may prevent them seeking care (Britton et al., 2011; Di Bona et al., 2014). It is acknowledged that a lack of information about therapeutic process and its importance at the time of referral is a potential barrier of subsequent treatment engagement (Alonzo et al., 2016; Mitchell and Selmes, 2007); however, past evidence has indicated that patients’ satisfaction about the care at ED or hospital is poor compared to the GP setting and other psychiatric settings (Shand et al., 2018). It may also be likely that this group has had negative experiences during their presentations to the ED or hospital.
Finally, this study found longer waiting times for treatment were associated with an increased risk of early treatment cessation. However, we were not able to find the impact of waiting time on treatment non-attendance as we defined waiting time as the time gap between the date of referral and the date of first treatment attendance. Previous research has indicated that a longer waiting time to get mental health treatments was associated with a lower likelihood of treatment initiation (Reitzel et al., 2006). Findings suggest timely access to the treatments is important to keep clients engaged with services, which is reflected in the current quality indicator that requires suicide prevention services under PMHC should commence within 1 week of the referral. Timely access to treatments is also important, especially for those attempted suicide, to avert potential suicide deaths as the risk of subsequent suicide is higher in the early period following a suicidal attempt (Hunt et al., 2009; Stokes, 2012). Longer waiting times and treatment non-attendance may also reflect that suicidal or behaviour relate to a period of crisis and that the motivation for treatment may change if there is an extended period before an available referral. Furthermore, longer wait times have also been associated with an increased risk of service cessation (Carter et al., 2012; Westin et al., 2014) and experiences of poor outcomes (Clark et al., 2018; Reichert and Jacobs, 2018).
Limitations
Although the large sample size is a strength, this study has a number of limitations. First, the early treatment cessation definition in this study is likely an underestimate of the total number of clients who ceased treatments. However, this study attempted to identify potential subgroups at increased risk of disengaging at ‘very early’ stages of treatments, which may not be considered as received adequate care they were supposed to receive. Second, this study did not include measures of distress and functional assessment which has shown to be associated with service engagement in previous other studies (Hom and Joiner, 2017; Killaspy et al., 2000), since these measures were unavailable for most the referrals. Third, there is no information available in the PMHC MDS to identify those with suicidal ideation and attempted suicide or self-harm to explicitly adjust models for this variable. Fourth, it might be possible that some clients who early ceased treatments accessed alternative services, for example, they were admitted to emergency care, or were referred crisis management services due to immediate risk of self-harm or suicidal behaviour. Fifth, it is also possible that some clients who did not attend or who early ceased PMHC services accessed other fee for service mental health support. This would perhaps be a small proportion of clients given the free access to suicide prevention services under PMHC services. Data linkage studies are warranted to better capture the trajectories of referrals among those presenting to primary health care with mental health issues.
Conclusion
This study investigated determinants of treatment disengagement among those at risk of suicide who were referred to PMHC services in Western Sydney, Australia. Findings suggest that age-appropriate treatment pathways which meet the needs of younger age-cohorts, transport facilities for those experiencing locational and material deprivation, especially among those reside in low SES areas, and treatment arrangements for those experiencing English-language barriers with a provider of similar cultural background, are important factors for consideration in improving treatment engagement in PMHC contexts. Behavioural engagement strategies and timely access to services, especially for those presenting with substance use disorder, and those being referred from outpatient suicide prevention services following discharge from acute care settings are areas where policy and service responses could improve treatment engagement among those at risk of suicide.
Supplemental Material
Supplementary_Material – Supplemental material for Determinants of treatment disengagement among those at risk of suicide referred to primary mental health care services in Western Sydney, Australia
Supplemental material, Supplementary_Material for Determinants of treatment disengagement among those at risk of suicide referred to primary mental health care services in Western Sydney, Australia by Sithum Munasinghe, Andrew Page, Haider Mannan, Shahana Ferdousi and Brendan Peek in Australian & New Zealand Journal of Psychiatry
Footnotes
Author Contributions
S.M. conceptualised the study, analysed the data and wrote the first draft of the manuscript. A.P., H.M., S.F. and B.P. provided advices to the study conception and to the analysis. A.P. contributed to critically revise the first draft and provided overall supervision for the manuscript. H.M., S.F. and B.P. made suggestions and revisions to the manuscript. All authors read and approved the final manuscript.
Availability of Data
The PMHC MDS and ATAPS MDS are owned by the Australian Government Department of Health. Western Sydney PHN has access to this data for Western Sydney PHN’s population catchment area.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.