
Abstract
Background:
Postpartum depression is one of the most common postpartum diseases, which has an important impact on the interaction between mother, infant, partner and family, as well as the long-term emotional and cognitive development of infants. However, there are still great disagreements on whether the delivery mode will affect the risk of postpartum depression. The purpose of this study is to explore whether the mode of delivery will affect the risk of postpartum depression through the comprehensive network meta-analysis of elective cesarean section, emergency cesarean section, instrumental vaginal delivery and spontaneous vaginal delivery.
Methods:
We searched in three electronic databases: PubMed, EMBASE and Cochrane Library.
Results:
This paper included 43 studies with a total sample size of 1,827,456 participants. Direct meta-analysis showed that the odds ratio of postpartum depression risk was 1.33 (95% confidence interval = [1.21, 1.46]) between cesarean section and vaginal delivery. The odds ratios of high Edinburgh Postpartum Depression Scale score between cesarean section and vaginal delivery in the three postpartum periods (within 2 weeks, within half a year and over half a year) were basically the same. There was no difference between cesarean section and vaginal delivery in the risk of severe postpartum depression at the Edinburgh Postpartum Depression Scale cut-off point ⩾13 (odds ratio = 1.07; 95% confidence interval = [0.99, 1.16]). Network meta-analysis showed that the risk of postpartum depression in the pairwise comparisons emergency cesarean section vs spontaneous vaginal delivery and elective cesarean section vs spontaneous vaginal delivery was odds ratio = 1.53 (95% confidence interval = [1.22, 1.91]) and 1.47 (95% confidence interval = [1.16, 1.86]).
Conclusion:
The mode of delivery has a significant effect on the occurrence of mild postpartum depression. Women who give birth by cesarean section, especially who give birth by emergency cesarean section, are at a higher risk of mild postpartum depression. We should carefully monitor the progress of postpartum mental disorders in women who delivered by cesarean section and make it possible for women to have a quick access to mental healthcare.
Introduction
Postpartum depression (PPD) is one of the most common postpartum diseases. About 10–15% of women have PPD (O’Hara and Swain, 2009). Although the birth of a baby is a pleasant and exciting thing, PPD can be the beginning of a nightmare for women who have experienced the disease (Buultjens and Liamputtong, 2007). Typical symptoms of PPD include depression, anxiety, lack of happiness, appetite and sleep disturbances, physical agitation, fatigue, feeling worthless and excessively guilty, decreased concentration and constantly thinking about death or suicide (Chandrasekaran et al., 2018). PPD is a health issue that has a significant impact on the mother, family, partners, mother–infant interaction and the long-term emotional and cognitive development of the baby. Henderson et al. (2003) suggest in report that PPD may have significant negative effects on mother-to-child interaction, child growth and breastfeeding. In addition, the children of the mothers with PPD tend to form insecure attachments with peers and develop social difficulties. PPD differs from other forms of depression in that it occurs at a specific time in life characterized by new childbearing events that require physical and psychological adaptation (Meky et al., 2020). Women experience adaptive physical and psychological changes during pregnancy, childbirth and the puerperium, making them vulnerable to mental illness (Zanardo et al., 2018). In addition to changes in the reproductive system and the physiological changes associated with pregnancy, women also experience psychosocial changes after childbirth, transition to parenthood, re-establish relationships and strive to meet the physical and emotional needs of newborns and other family members (Goker et al., 2012).
PPD occurs because of a combination of biological and psychosocial factors, genetic factors and important life experiences. However, there is still a considerable disagreement as to whether delivery patterns affect the risk of PPD, and many studies have not found an independent relationship between them (Carter et al., 2006; Eisenach et al., 2008; Hannah et al., 2002; Nielsen Forman et al., 2000; Patel et al., 2005; Sword et al., 2011). Studies have even shown that cesarean section (CS) is a protective factor for PPD in some cases (Chaaya et al., 2002). Some studies, however, suggest that the delivery mode may be a risk factor for PPD. According to the latest research of Zanardo et al. (2018), the scores of women who gave birth by CS are significantly higher than women who gave birth through normal vaginal delivery (VD) on the Edinburgh Postpartum Depression Scale (EPDS), especially with regard to anxiety and depression symptoms.
Based on the above introduction, this study aims to conduct a comprehensive network meta-analysis of elective cesarean section (ELCS), emergency cesarean section (EMCS), instrumental vaginal delivery (IVD) and spontaneous vaginal delivery (SVD) to explore whether the delivery mode affects the risk of PPD.
Methods
Protocol and guidance
This systematic review and network meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Liberati et al., 2009).
Eligibility criteria
In this paper, cohort and cross-sectional studies were included. All studies had to cover one or more of the following four delivery modes: (1) SVD, (2) IVD (vacuum- or forceps-assisted delivery), (3) EMCS and (4) ELCS. ELCS were those with prior planning, and EMCS were those without prior planning or that took place after labor started (Patel et al., 2005). The participants who delivered by SVD were assigned to a control group. The participants who met the eligibility criteria were all age-appropriate mothers without limited parity, and their psychological status was assessed after childbirth. The outcome of the included studies was the prevalence of high EPDS score or the odds ratio (OR) of delivery methods as a risk factor for PPD.
Information sources and search strategy
We searched articles published before 20 January 2020, regardless of language or data, in three electronic databases: PubMed, EMBASE and Cochrane Library. The articles were selected by manual screening. The search strategy was: search ((Postpartum depression[Title]) OR (post-partum depression[Title]) OR (post-natal depression[Title]) OR (Postnatal depression[Title]) OR (puerperal depression[Title]) OR (postnatal psychiatric[Title]) OR (Depression, Postpartum[MeSH Terms])) AND ((Cesarean[Title/Abstract]) OR (Caesarean[Title/Abstract]) OR (Cesarean Section[MeSH Terms]) OR (forceps[Title/Abstract]) OR (vacuum extraction[Title/Abstract]) OR (assisted vaginal[Title/Abstract]) OR (Operative delivery[Title/Abstract]) OR (delivery mode[Title/Abstract]) OR (Delivery method [Title/Abstract]) OR (mode of delivery[Title/Abstract]) OR (Type of delivery[Title/Abstract]) OR (method of birth[Title/Abstract]) OR (Mode of birth[Title/Abstract])).
Study selection
The two methodologically trained independent reviewers screened titles and abstracts to determine whether they met the eligibility criteria. The reviewers read the full text and extracted relevant data after a consensus was reached. Any differences were resolved through discussion and arbitration, if necessary, by a third reviewer. The reasons for inclusion or exclusion were recorded in detail. Case reports, letters and minutes of meetings were excluded. The PRISMA flow diagram was used to summarize the study selection processes.
Data extraction
The two investigators used a predefined data extraction sheet to independently extract data from each included study, such as authors, publication year, study design, sample size, grouping and number of patients in the group, cross-sectional data, including counts and effect estimates (OR), country, depression assessment time point, checklist used for depression assessment, title and conclusion. The third investigator independently reviewed the data to ensure accuracy. If no data in digital format were available, we used the free software Plot Digitizer to estimate data from the graphs.
Definition of outcomes
The outcome of the network meta-analysis is the OR of high EPDS score (defined as EPDS score ⩾ 9) in pairwise comparisons between any two of the four delivery modes. The outcome of the direct meta-analysis is the OR of high EPDS score between the cesarean delivery and the VD mode.
EPDS was used to evaluate PPD in this study. EPDS was designed and developed by the University of Edinburgh in Scotland in 1987. It is a simple and comprehensive scale for assessing PPD (Cox et al., 1987). The EPDS score from ⩾9 to ⩽12 is defined as mild PPD in this study.
Statistical analysis
The direct meta-analysis was used to compare the risk of high EPDS score between CS and VD. The generic inverse variance was used to combine the OR of high EPDS score. The heterogeneity was assessed using Q test and I2 statistic. The network meta-analysis was used to evaluate the comparative effect by combining direct and indirect evidence of the four delivery modes. First, to visualize network geometry and node connectivity, we summarized the geometry of the evidence network using network plots. We conducted a network meta-analysis of the relationship between delivery modes and PPD using a multivariate random-effects (restricted maximum likelihood estimation) meta-analysis model. To obtain treatment hierarchies, we used a parametric bootstrap procedure with 5000 resamples to compute ranking probabilities. Mean rankings as well as surface under the cumulative ranking curve (SUCRA) values were computed for each delivery mode. We checked the consistency of the network using local and global inconsistency tests. All analyses were conducted in Stata/SE, version 14.
Assessment of risk of bias in individual studies
The quality of studies was independently assessed by two authors. Any disagreement was resolved by a senior author. We applied the cross-sectional study evaluation criteria of AHRQ (the agency for healthcare research and quality) to evaluate cross-sectional studies, including 11 items, with ‘yes’, ‘no’ and ‘unclear’ answers, respectively.
Assessment of small study effects
To evaluate the presence of small study effects, we visually inspected comparison-adjusted funnel plots for each outcome. We produced funnel plots not only for direct comparison between CS and VD but also for indirect comparison between four delivery modes.
Subgroup analysis
Since the timing of PPD assessment may affect the analysis results, the women were divided into three subgroups: within 2 weeks after giving birth, within 6 months after giving birth and more than 6 months after giving birth. Moreover, since a threshold score of EPDS for the diagnosis of PPD varies between different studies, we formed a subgroup with an EPDS score ⩾13 for more detailed evaluation. Finally, considering that PPD is affected by a variety of social and clinical factors, and the crude OR may be more heterogeneous, we conducted a pooled study to provide an adjusted OR of high EPDS score between CS and VD for a more comprehensive analysis.
Results
Study selection
The initial search of three databases yielded 1072 articles. We obtained 131 articles after reading the title and abstract, excluding duplicates and irrelevant articles. After screening the full texts manually, 88 articles were excluded for reasons including review article (n = 11), not relevant to delivery mode (n = 36), not relevant to PPD (n = 6) and not available data (n = 35). Eventually, 43 studies were included in this network meta-analysis (Figure 1).
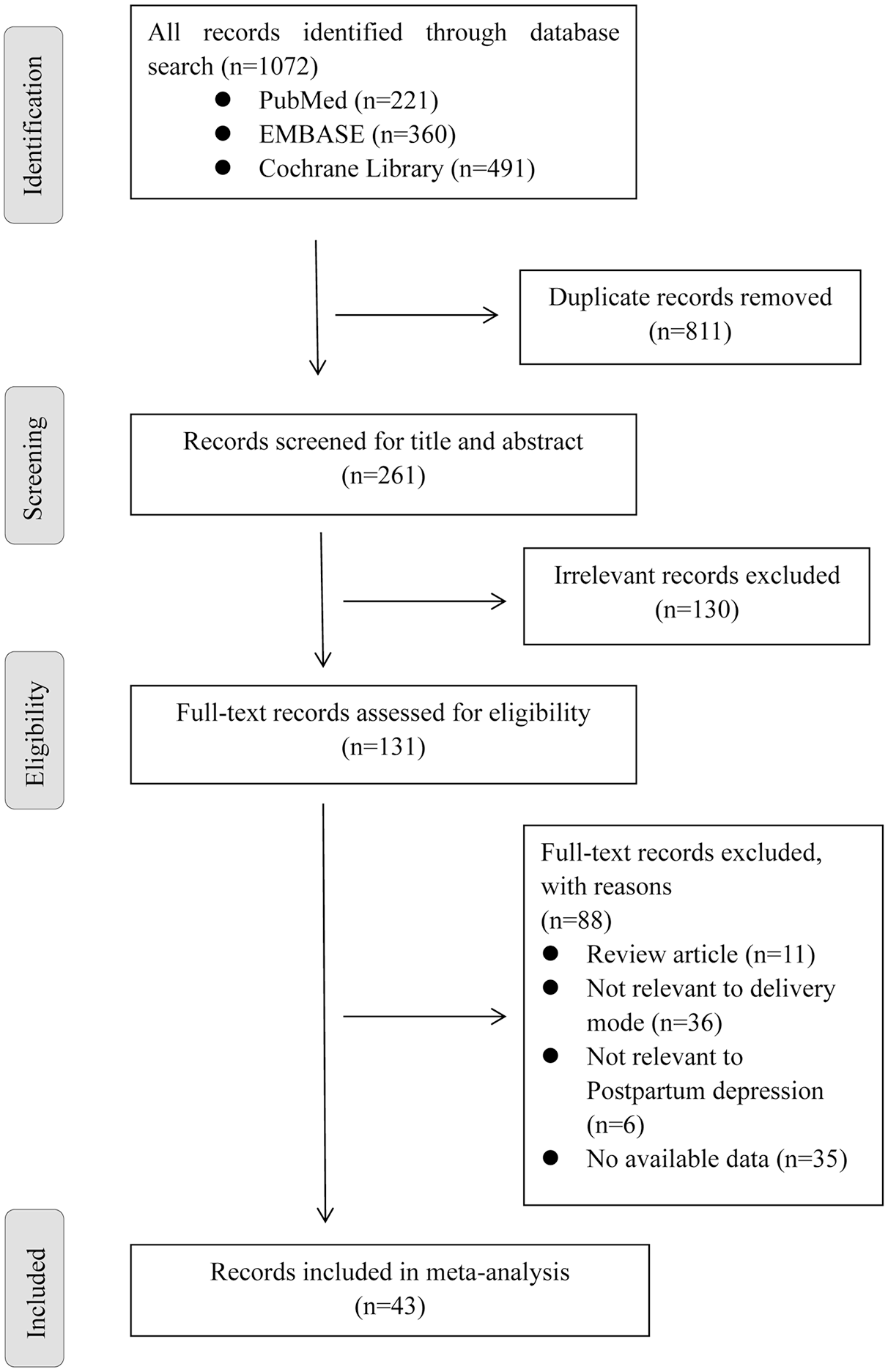
Flowchart of study selection.
Study characteristics
In this network meta-analysis, 43 studies were included, comprising a total sample size of 1,827,456 participants. The 43 studies included 16 cross-sectional studies and 27 cohort studies. Among them 13 studies involved SVD, 11 studies concerned IVD, 15 studies reported EMCS and 14 studies discussed ELCS, all of them were subject to network meta-analysis. A total of 36 studies were subject to direct meta-analysis of VD and CS. The summary data of each included study are shown in Table 1, and the network plot is shown in Figure 2.
Characteristics of included studies.
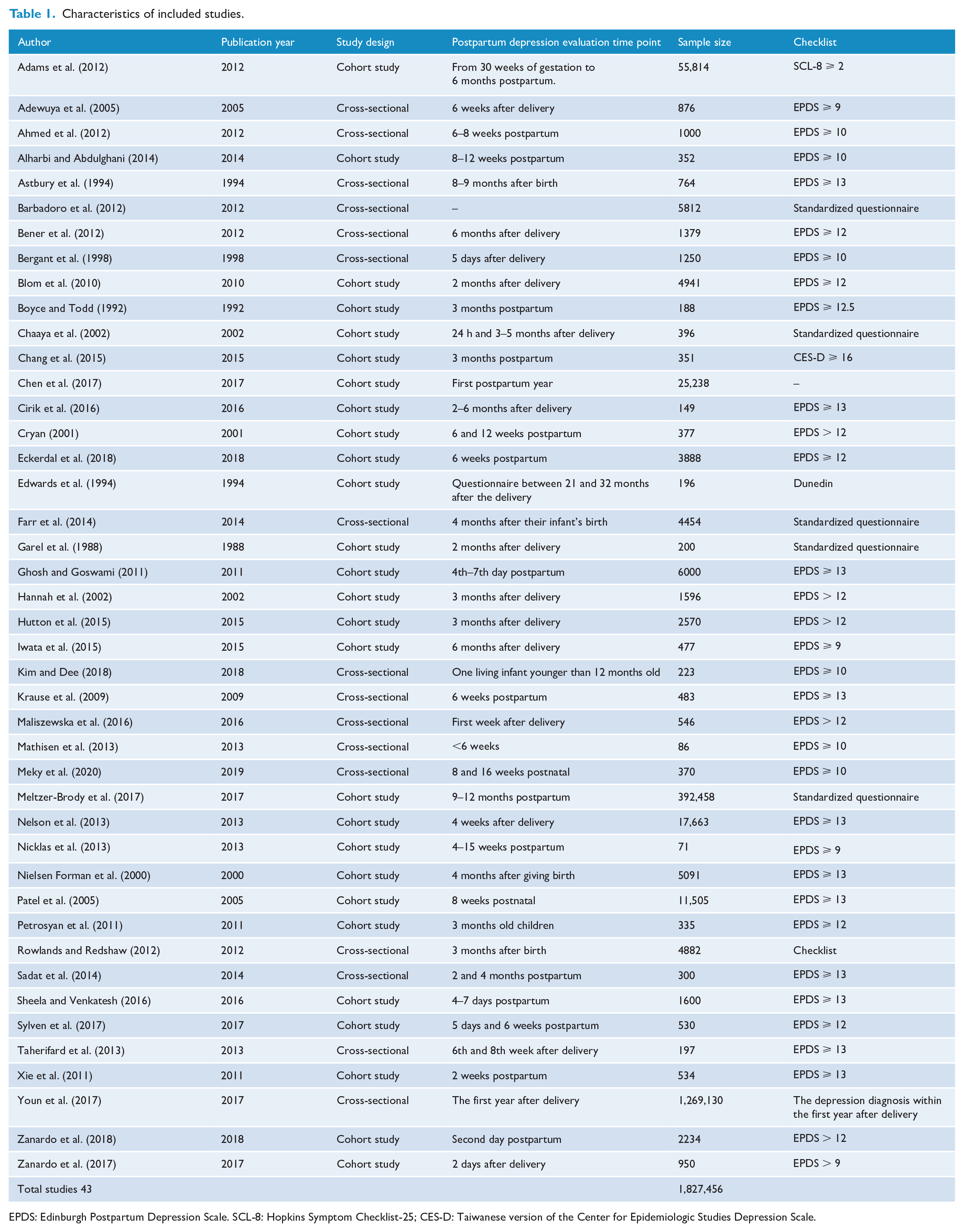
EPDS: Edinburgh Postpartum Depression Scale. SCL-8: Hopkins Symptom Checklist-25; CES-D: Taiwanese version of the Center for Epidemiologic Studies Depression Scale.
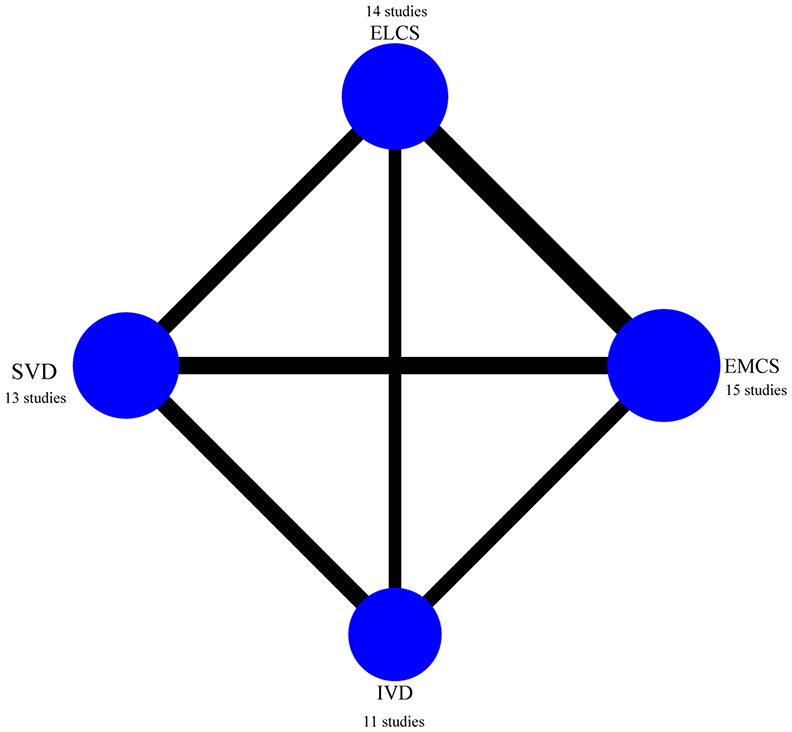
Network plot for all studies.
Risk of bias within studies
An 11-point scale was used to measure AHRQ, and the average total score of 43 included articles was 9.3 points. One point-lost item ‘Describe how confounding was assessed and / or controlled’ had an average 0.5 out of 1 point. Another point-lost item ‘Clarify what follow-up, if any, was expected and the percentage of patients for which incomplete data or follow-up was obtained’ had an average 0.5 out of 1 point.
Synthesis of results
The OR of high EPDS score (directly compared between VD and CS)
First, the OR of PPD between CS and VD was 1.33, 95% confidence interval (CI) = [1.21, 1.46], p-value < 0.00001, I2 = 61%, indicating that the risk of high EPDS score in CS was 1.33 times that in VD. Second, the OR of PPD between CS and VD was: for ‘within 2 weeks postpartum’ subgroup, OR = 1.38, 95% CI = [1.07, 1.79], p-value = 0.01, I2 = 80%, Figure 3(a); for ‘from 2 weeks to 6 months postpartum’ subgroup, OR = 1.3, 95% CI = [1.13, 1.50], p-value = 0.0003, I2 = 59%, Figure 3(b); for ‘More than 6 months postpartum’ subgroup, OR = 1.31, 95% CI = [1.21, 1.46], p-value < 0.00001, I2 = 61%, Figure 3(c). The above results showed that the risk of high EPDS score after CS was significantly higher than that after VD in three time periods. Third, the OR of PPD in the subgroup with EPDS score ⩾ 13 was 1.07, 95% CI = [0.99, 1.16], p-value = 0.08, I2 = 46%, indicating that there was no significant difference between CS and VD in risk of high EPDS score in the subgroup with severe PPD, Figure 4(a). Finally, the adjusted OR of the risk of PPD was OR = 1.34, 95% CI = [1.15, 1.56], p-value = 0.0002, I2 = 44%, indicating that the risk of PPD in CS was 1.34 times that in VD after adjusting for various influential factors related to PPD, Figure 4(b). Considering the across-studies heterogeneity may be caused by different PPD measurement checklists, we conducted a subgroup analysis involving only EPDS and found that the variety of conflated effect value was too small to change the statistical significance (Supplementary Figure S1). Furthermore, we conducted subgroup analyses of cohort studies and cross-sectional studies and found that the combined results of the two types of studies were basically the same, except for the ‘within 2 weeks postpartum’ subgroup in cohort study, where the combined results changed to statistically insignificant (Supplementary Figures S2 and S3).
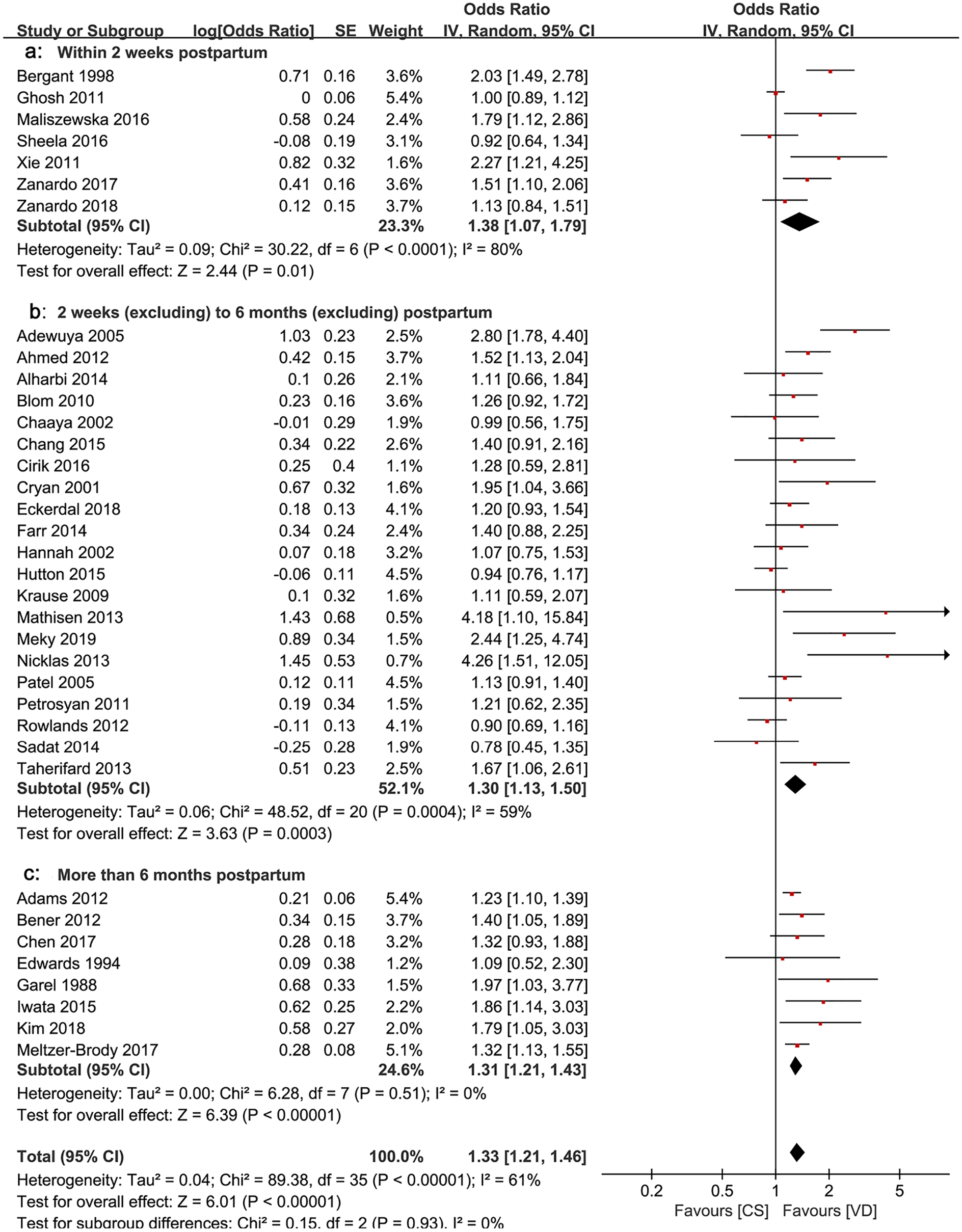
Forest plot of odds ratio of PPD between CS and VD: (a) within 2 weeks postpartum, (b) 2 weeks to 6 months postpartum and (c) more than 6 months postpartum.
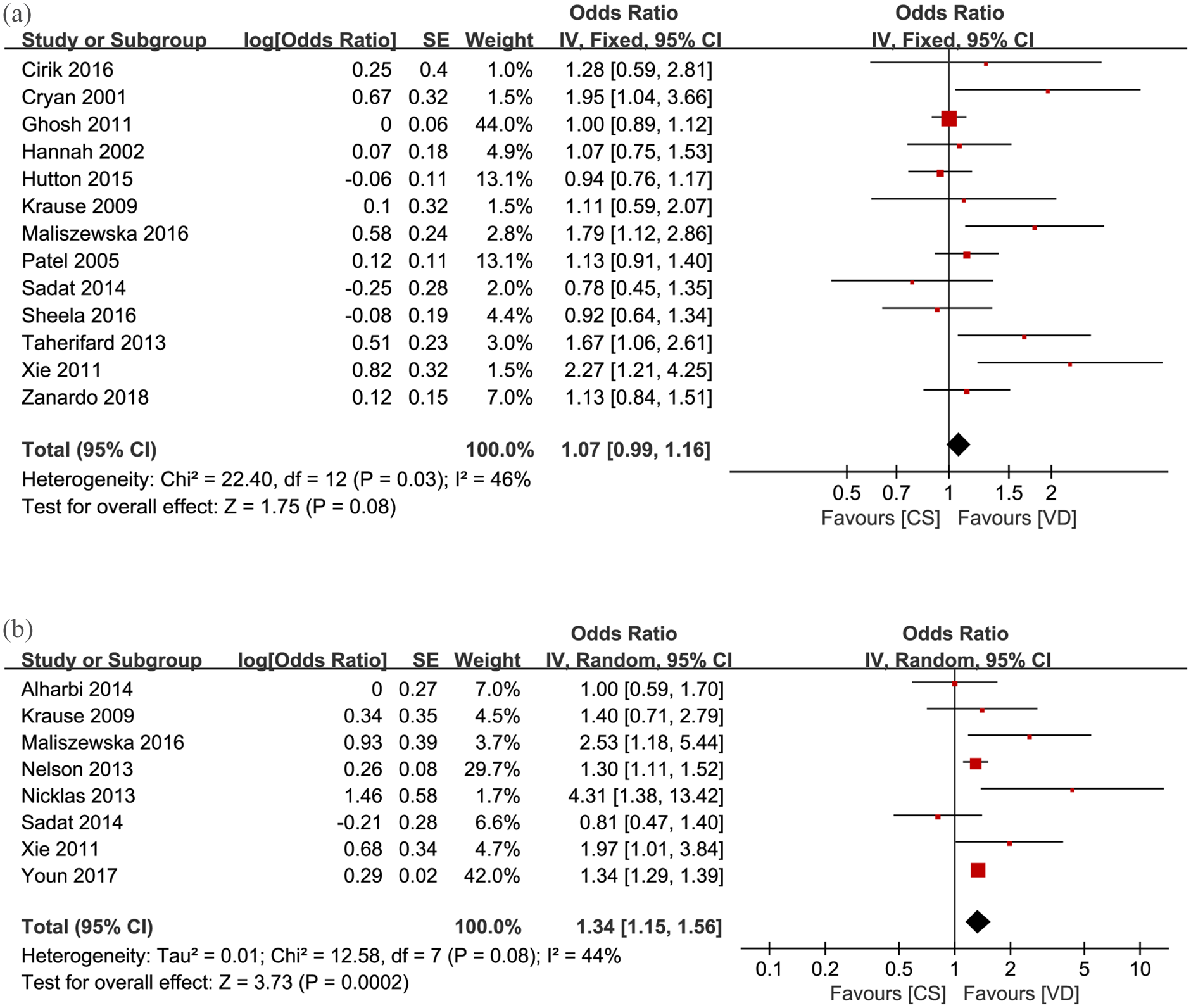
(a) Forest plot of odds ratio of PPD in the subgroup with EPDS score ⩾ 13 and (b) Forest plot of the adjusted odds ratio of the risk of PPD.
The OR of high EPDS score in four delivery modes analyzed by network meta-analysis approach
The risk of high EPDS score in EMCS was 1.53 times that in SVD, and the risk of high EPDS score in ELCS was 1.47 times that in SVD, showing significant differences. The ORs were 1.53 (95% CI = [1.22, 1.91]) and 1.47 (95% CI = [1.16, 1.86]), respectively. The risk of high EPDS score was statistically insignificant in the pairwise comparisons of other delivery modes (Figure 5(a)). Furthermore, we conducted a subgroup analysis to differentiate between the use of vacuum or forceps and found no difference between their risks of high EPDS score, as displayed in Supplementary Figure S4.
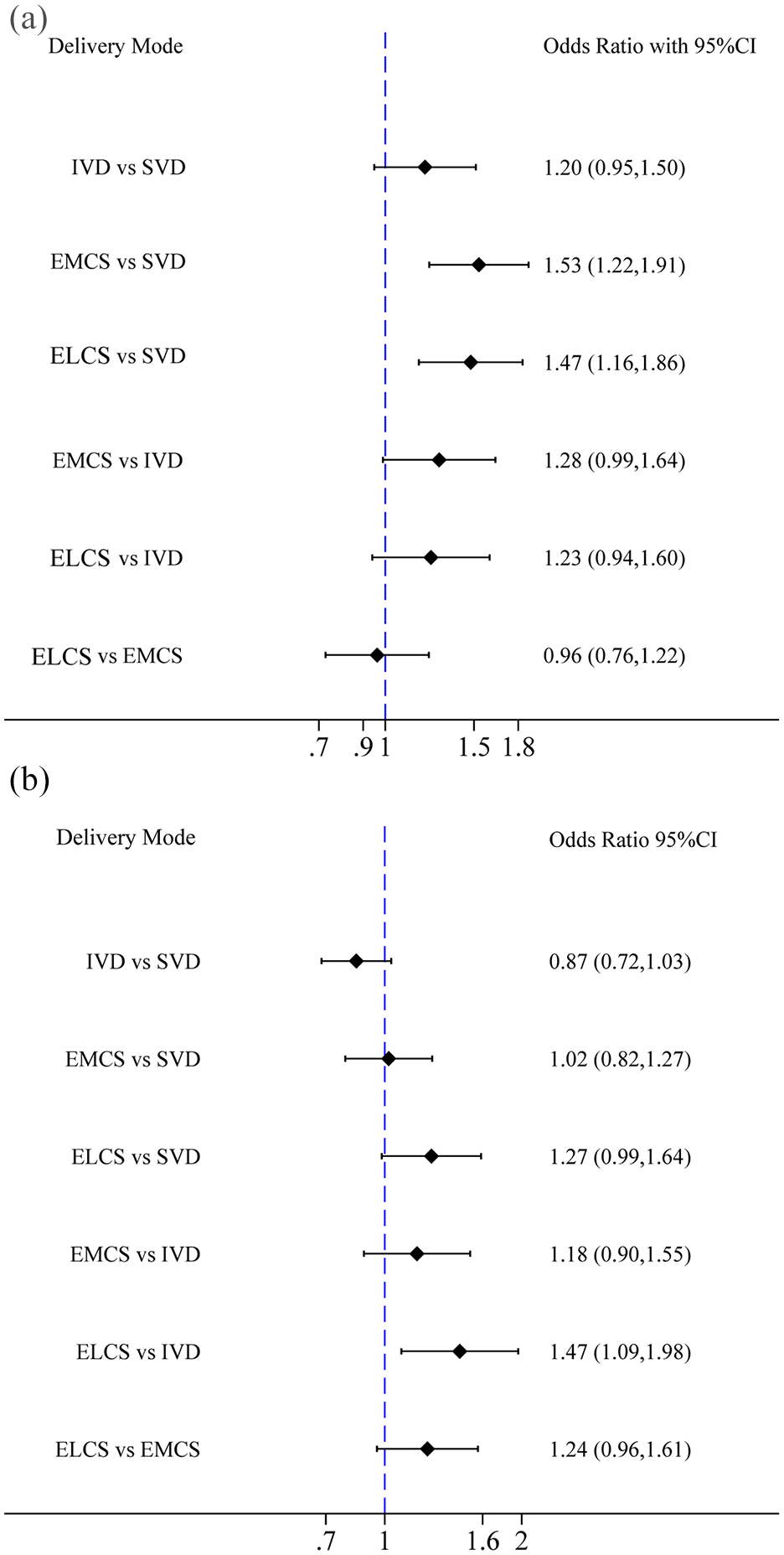
(a) Forest plot of odds ratio of PPD pairwise comparisons among four delivery modes (SVD, IVD, EMCS, ELCS) and (b) Forest plot of odds ratio of PPD pairwise comparisons among four delivery modes (SVD, IVD, EMCS, ELCS) in the subgroup with EPDS score ⩾ 13.
The network meta-analysis of the risk of high EPDS score in four delivery modes with EPDS ⩾ 13 showed that the risk of EPDS score ⩾ 13 in ELCS was 1.47 times that in IVD and the OR was 1.47 (95% CI = [1.09, 1.99]). The risk of EPDS score ⩾ 13 was statistically insignificant in the pairwise comparisons of other delivery modes (Figure 5(b)).
Ranking probabilities
According to SUCRA, the risk of high EPDS score in four delivery modes is shown in Table 2. From the view of point of the high EPDS score, EMCS had the highest risk, followed by ELCS, IVD ranked third and SVD had the lowest risk.
Ranking probabilities.
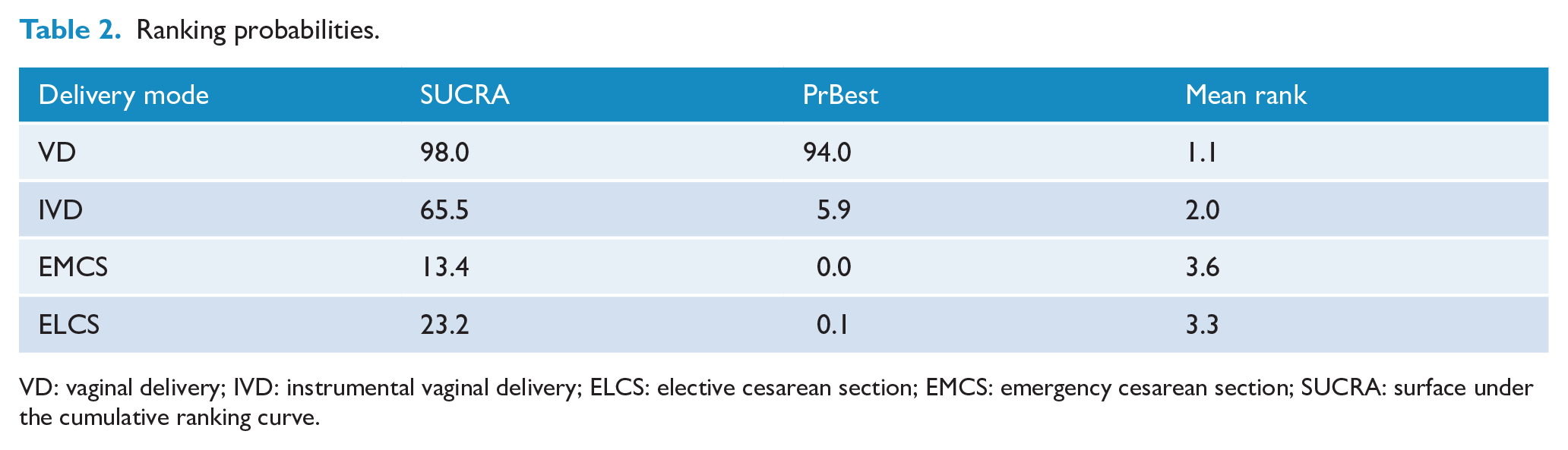
VD: vaginal delivery; IVD: instrumental vaginal delivery; ELCS: elective cesarean section; EMCS: emergency cesarean section; SUCRA: surface under the cumulative ranking curve.
Inconsistency test
No evidence for statistically significant inconsistency (Global inconsistency tests p = 0.200) was found.
Risk of bias across studies
Publication bias was detected in the direct meta-analytical funnel plot (Figure 6). According to the trim-and-fill method, we filled nine studies and adjusted the pooled effect value from 1.33 (95% CI = [1.21, 1.46]), p-value < 0.00001, to 1.20 (95% CI = [1.09, 1.33]), but did not produce substantial effect, indicating that the results of the direct meta-analysis were not significantly affected by publication bias (Figure 7). The network meta-analytical funnel plot was shown in Figure 8. The funnel plot was relatively symmetrical, showing no evidence of publication bias.
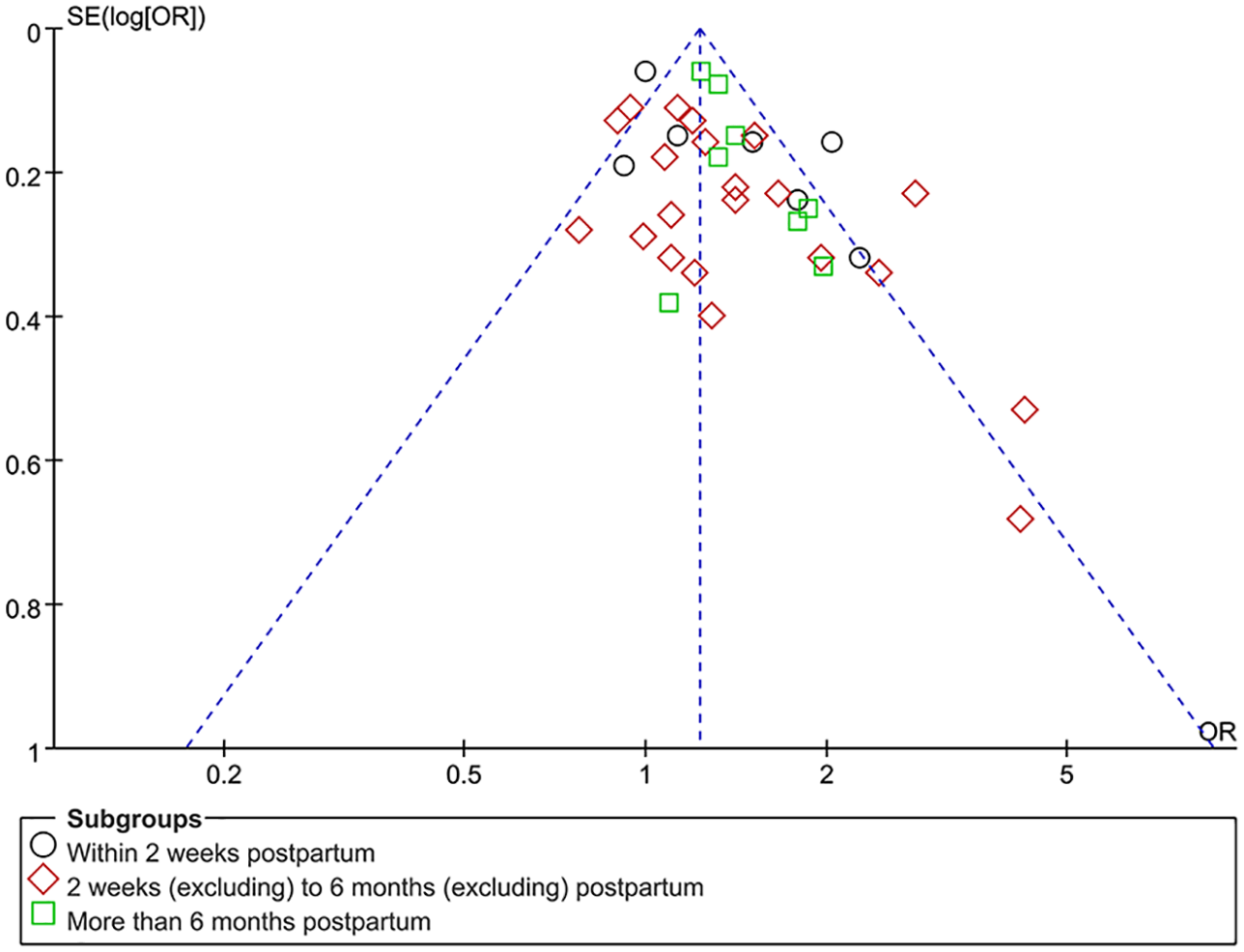
Funnel plot of odds ratio of PPD between CS and VD.
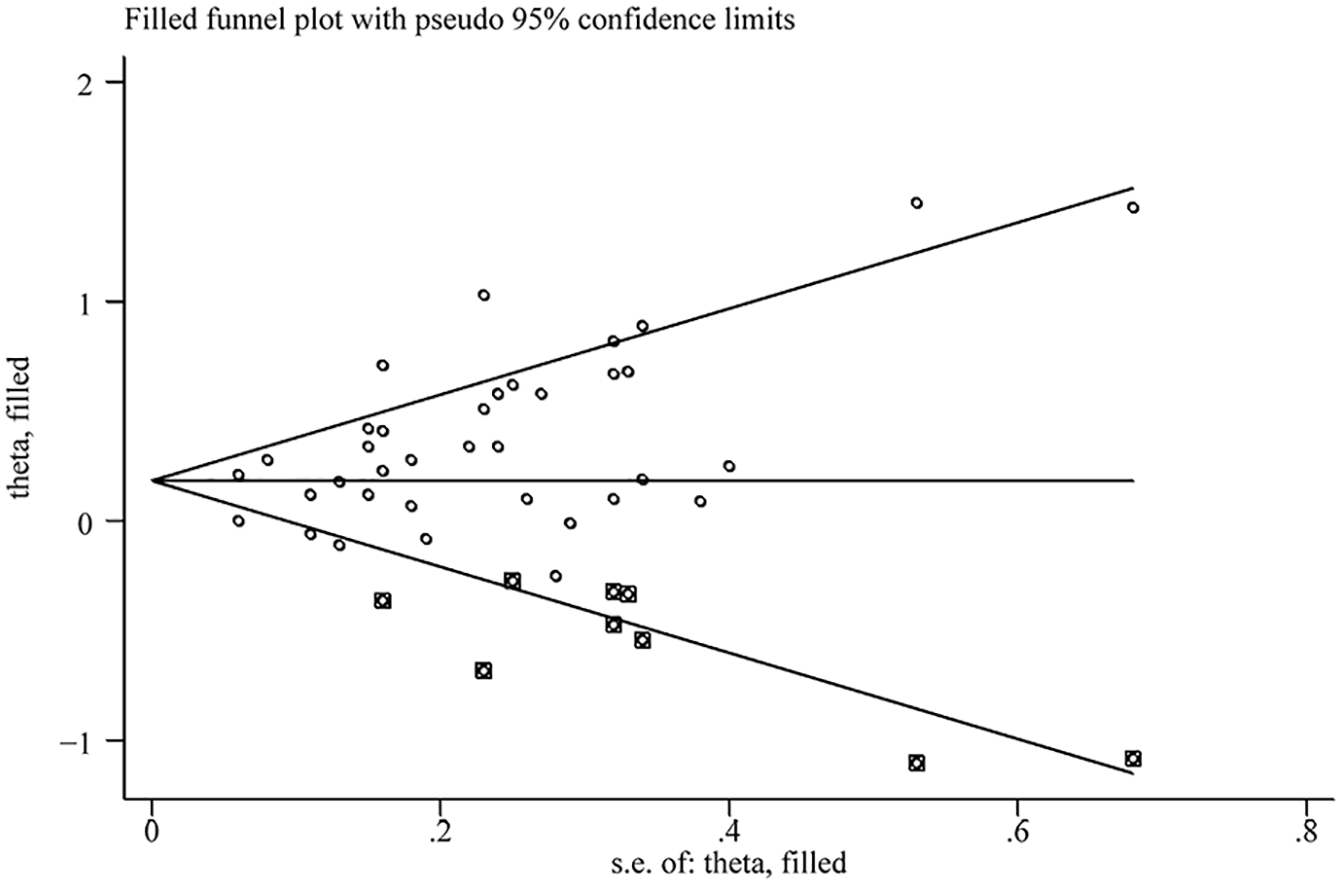
Filled funnel plot of odds ratio of PPD between CS and VD.
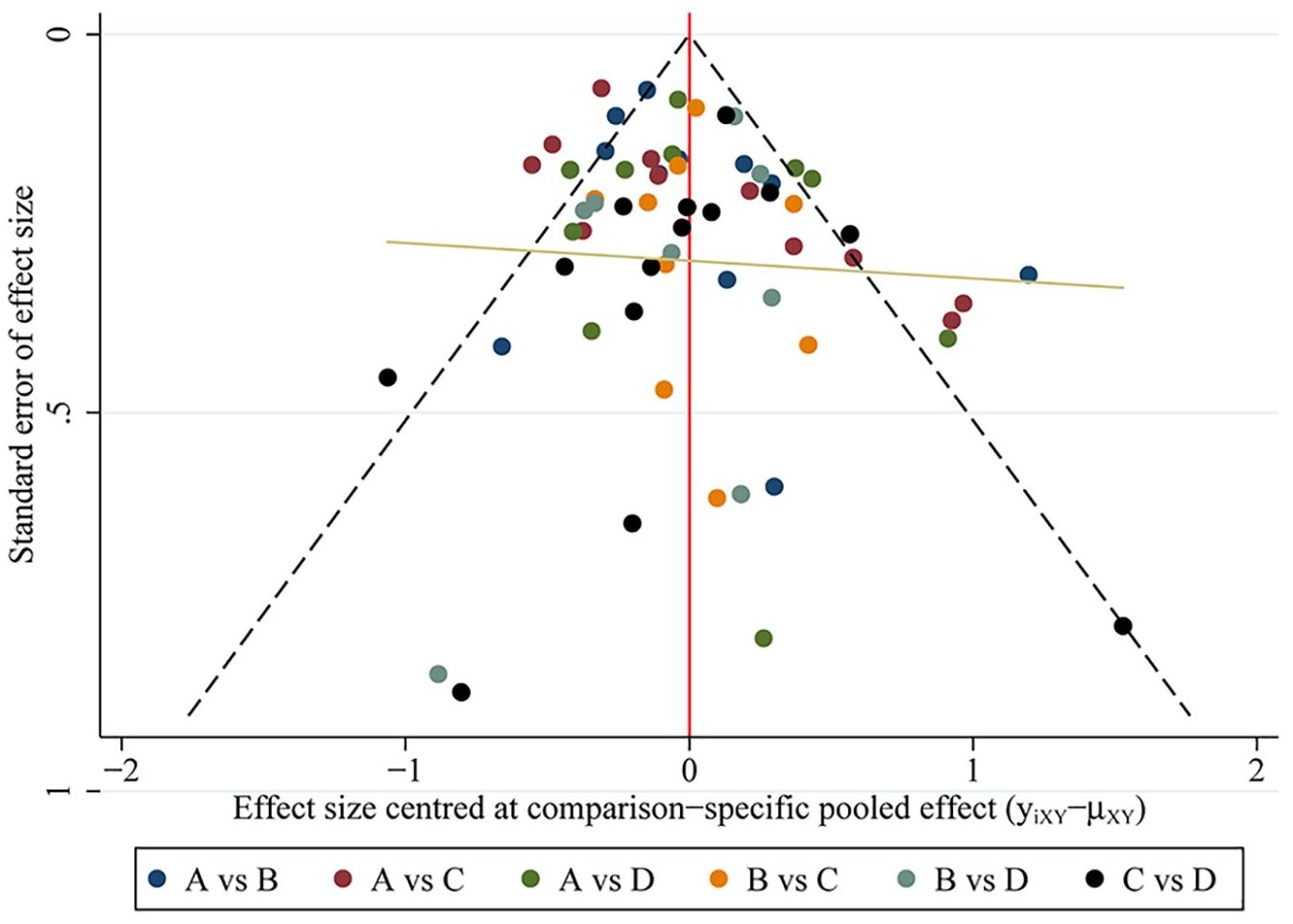
The network meta-analytical funnel plot: A = SVD, B = IVD, C = EMCS and D = ELCS.
Discussion
This meta-analysis included 43 studies with a total sample size of 1,827,456 participants. This study systematically explored the relationship between delivery mode and PPD from two perspectives. On one hand, we measured the high EPDS score after CS and VD. On the other hand, we analyzed the high EPDS score in ELCS, EMCS, IVD and SVD by network meta-analysis.
The comparative risk of PPD between CS and VD
Our study found that the unadjusted risk of PPD in CS was 1.33 times that in VD. Baby blues usually begins a few days after childbirth and lasts for 10–14 days and can be regarded as a mild and brief postpartum disorder. Although for most women (26–85%) PPD is relatively mild and usually resolves within 2 weeks (Complojer et al., 2009), 10–15% of women experience more severe and lasting PPD (Warner et al., 1996). Since the timing of PPD assessment may affect the prevalence, we formed three subgroups for comparative analysis: 2 weeks after delivery, 2 weeks to 6 months after delivery and more than 6 months after delivery. Basically, the same results were obtained for three time periods: the risk of PPD in CS group was 1.38 times, 1.30 times and 1.31 times that in VD, respectively. In addition, due to the different threshold scores of EPDS in the diagnosis of PPD in different studies, we further analyzed PPD women with EPDS scores ⩾ 13. (A woman with a score of 13 or more is considered to be severely depressed, with scores of 10–12 being classified as marginal cases and scores of 0–9 as being without depression) (Cox et al., 1987; Eberhard-Gran et al., 2001). Our study found that there was no significant difference in the risk of severe PPD between women who delivered by CS and women who delivered by VD, and women who delivered by CS were more likely to have mild PPD than women who delivered by VD. In addition, PPD is the result of many factors. On the basis of comprehensive factors, we calculated and obtained the adjusted OR, which showed that the adjusted risk of PPD in women delivering by CS was 1.34 times that in women delivering by VD, which was consistent with the unadjusted value, fully showing that CS was an important factor of PPD. This result can be explained both physically and psychologically. Physiologically, a large amount of cortisol is released during VD. Cortisol is a stress hormone caused by a stress response. Studies have shown that the link between high cortisol levels and PPD caused by surgical stress may be related to the reduction of brain 5-hydroxytryptamine (5-HT), which makes susceptible subjects prone to depression (Dinan, 1994; Edwards et al., 1994). Second, the inflammation, associated pain and stress caused by surgery theoretically increase the susceptibility of women to depression (Eckerdal et al., 2018). Third, oxytocin also affects PPD. Oxytocin is important for uterine contraction and breastfeeding. Oxytocin levels are usually lower in women delivering by CS than in women delivering by VD. In the process of VD, the content of oxytocin in the brain of pregnant women will increase, which will help reduce stress and improve happiness, thereby reducing the possibility of postpartum mental disorders (Kim et al., 2014; Lonstein et al., 2014; Mottolese et al., 2014). Psychologically, many women have negative emotions after VD, such as inferiority, sense of failure, loss of control or disappointment. Nursing wounds, slow postpartum recovery and the effects of complications may increase the risk of PPD. In addition, women who undergo CS have a lack of confidence because they cannot give birth naturally. Women’s lack of self-confidence can be stressful when raising children. In addition, changes in physical pain and adaptation to life after childbirth will cause mental disorders and then develop into PPD (Loto et al., 2010).
The comparative risk of PPD between ELCS, EMCS, IVD and SVD
This study used a network meta-analysis to analyze the risk of PPD in ELCS, EMCS, IVD and SVD. The results showed that the risk of PPD in women giving birth by EMCS was 1.53 times that of women by SVD, and the risk of PPD in women giving birth by ELCS was 1.47 times that of women by SVD, but there was no significant difference in the risk of PPD among women giving birth by IVD and SVD. We also analyzed women with an EPDS score ⩾ 13 and found that women who gave birth through one of four delivery modes had no significant difference in the risk of severe PPD. We found that EMCS was associated with the highest risk of mild PPD, followed by ELCS and IVD, while SVD was associated with the lowest risk of mild PPD. From a physiological point of view, this difference may be related to the use of anesthetics. Some studies found that the majority of participants giving birth by EMCS used general anesthesia, while the participants giving birth by ELCS used almost spinal anesthesia (Meky et al., 2020). General anesthesia may cause depression through certain biochemical mechanisms that function at the molecular level. There is an evidence that the volatile anesthetics inhibit 5-HT uptake; that thiopentone decreases transmission at serotonergic, dopaminergic and noradrenergic synapses; and that nitrous oxide can interfere with the synthesis of S-adenosyl methionine and thereby that of monoamines. The effect of barbiturates and benzodiazepines in increasing GABAergic transmission is well known, and there is a possibility that these drugs can precipitate depression (Edwards et al., 1994). In addition, from a physiological point of view, EMCS, as well as the accompanying obstetric and neonatal complications, leads to negative experience and increases the risk of PPD. It has been reported that EMCS has more complications and a longer recovery time than SVD and ELCS (Bergholt et al., 2003; Jansen et al., 2007). Women who give birth by EMCS may experience physical fatigue due to the failure of VD, as well as the psychological burden and subjective feeling of being unable to give birth. All of these can lead to a negative delivery experience, resulting in depression (Eckerdal et al., 2016; Silverman et al., 2017).
Strengths
Our research has several advantages. First of all, our study is the largest meta-analysis of the relationship between delivery modes and PPD on basis of analysis of 1.82 million samples. Second, we analyzed not only VD and CS, but also four delivery modes through network meta-analysis. This is a comprehensive meta-analysis of the relationship between various delivery modes and PPD. Third, this study is the first meta-analysis to distinguish between severe and mild PPD and modes of delivery.
Limitations
First, most of the included studies used questionnaires to assess PPD, while EPDS is used to screen for clinical symptoms of PPD, not PPD itself. However, EPDS scores are closely related to clinical diagnosis and are often used to measure PPD. Second, PPD is related to many confounding factors. Most studies provide only crude results, and the number of studies we used to combine the adjusted effect values was slightly smaller.
Conclusion
In conclusion, although there are many factors that affect PPD, our study shows that the mode of delivery has a significant impact on the occurrence of mild PPD. The risk of mild PPD was 33% higher in women delivering by CS than in women delivering by VD, and 53% higher in women delivering by EMCS than in women delivering by SVD. Given the large number of CSs per year, the number of women who may be affected by PPD will be high. If used properly, CS is an important lifesaving operation. However, unnecessary CS will not only increase the cost of medical treatment but also increase the risk of maternal and infant health. Therefore, we suggest to take necessary measures to reduce unnecessary CS. The risks associated with CS should be informed to the maternal and relevant medical professionals. We should carefully monitor the progress of postpartum mental disorders in women who delivered by CS and make it possible for women to have a quick access to mental healthcare.
Supplemental Material
Supplemental_material – Supplemental material for Association between mode of delivery and postpartum depression: A systematic review and network meta-analysis
Supplemental material, Supplemental_material for Association between mode of delivery and postpartum depression: A systematic review and network meta-analysis by Lei Sun, Su Wang and Xi-Qian Li in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would like to thank Beijing Zhiyun data technology co. LTD for providing data analysis service.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.