
Abstract

To the Editor
Patients with severe treatment-resistant depression (TRD) and radiation-induced brain injuries can respond well to electroconvulsive therapy (ECT). This case report describes the efficacy of ECT in a patient with severe TRD associated with radiation-induced brain injuries in the context of histiocytosis X.
A 49-year-old woman consulted our Psychiatry Department for TRD. She had a severe depression characterised by major hypokinesia, anhedonia, cognitive impairments, anorexia and insomnia (Montgomery–Åsberg Depression Rating Scale [MADRS] = 36/60). She poorly responded to several antidepressants (mianserine 60 mg/day, fluoxetine 20 mg/day, clomipramine 75 mg/day). Attempts to increase the dose of antidepressants were associated with severe adverse effects (dizziness, nausea, loss of balance and dry mouth).
In her past medical history, she also suffered from histiocytosis X (or Langerhans cell histiocytosis [LCH]), a rare proliferative disorder that can affect nearly every organ system (Demellawy et al., 2015). Histiocytosis X was complicated with a central diabetes insipidus and she was treated with desmopressin, corticotherapy and chemotherapy.
Her brain MRI, with T2* sequence, revealed several left cerebellar cavernomas. Interestingly, we found that as a child, she was treated with radiotherapy for right retro-auricular lesions. These lesions were described as characteristic of radiation-induced brain injuries (see Figure 1). We also used [18F]-fluorodesoxyglucose positron emission tomography (FDG-PET) brain scan to evaluate the impact of brain lesions on the brain metabolism. The FDG-PET revealed hypometabolism in prefrontal and anterior cingulate cortex associated with heterogeneous cortical fixation in parietal lobes (see Figure 1).
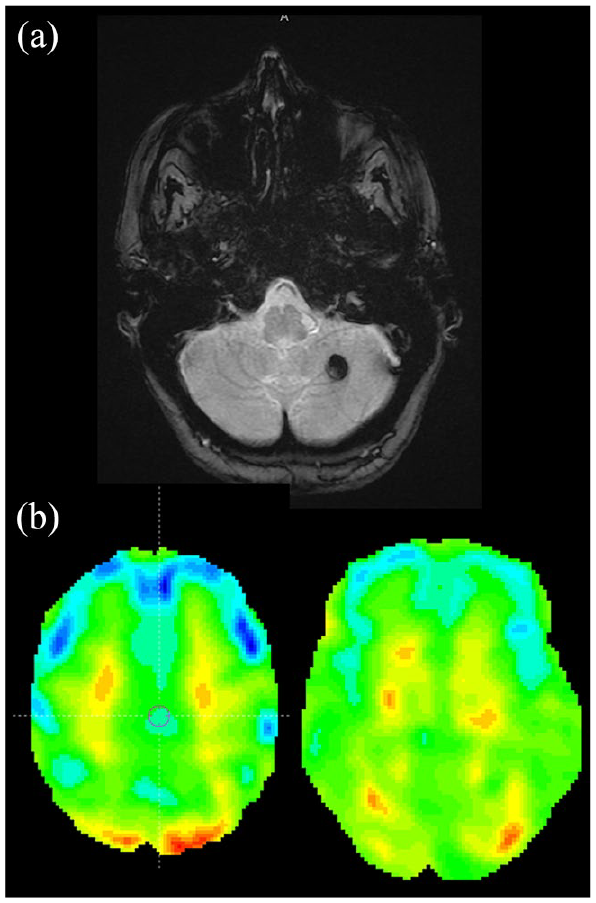
(a) Brain MRI with axial T2* sequence shows a hyposignal lesion in the left hemisphere suggestive of cavernoma (b) PET brain scan before (left) and after (right) 13 sessions of electroconvulsive therapy.
The antidepressants adverse effects and the central diabetes insipidus restricted pharmacological up-titration. Therefore, after a multidisciplinary decision (including psychiatrist, neurologist and neuroradiologist) and given the risk benefit balance, ECT was pursued.
After 13 sessions of bitemporal ECT, the patient described a significant mood improvement (MADRS = 7). No adverse effects throughout her course of treatment were noticed.
A PET scan was performed 3 months after ECT which showed an improvement of hypometabolism in prefrontal lobes (see Figure 1). Hypometabolisms in anterior cingulate and superficial parietal lobes remained identical.
We present here the first case report of successful ECT treatment in a patient with radiation-induced brain injuries. This case report also highlights that brain imaging can be crucial while treating severe and treatment-resistant mental illness, to identify patients who can benefit from targeted treatment such as a faster access to ECT (Peter et al., 2018). Finally, this case reaffirms that ECT is a safe treatment for patients with neuropsychiatric disorders after careful consideration of possible risks and benefits.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.