
Abstract
Objective:
The International Classification of Diseases, 11th Revision classification of personality disorder removes all categories of disorder in favour of a single diagnostic spectrum extending from no personality dysfunction to severe personality disorder. Following concerns from some clinicians and Personality Disorder Societies, it was subsequently agreed to include a borderline pattern descriptor as a qualifier of the main diagnosis. We explore the value of this additional descriptor by examining personality data in patients with major depression.
Method:
We examined personality data obtained using the Structured Clinical Interview for Personality Disorder-II in 606 patients enrolled in five randomised controlled trials of depression. The Structured Clinical Interview for Personality Disorder-II uses the Diagnostic and Statistical Manual of Mental Disorders categorical system, which includes borderline personality disorder. The International Classification of Diseases, 11th Revision classification has five domain traits. Each of the Diagnostic and Statistical Manual of Mental Disorders personality disorder symptoms or behaviours from Structured Clinical Interview for Personality Disorder-II was reordered into the five domains independently by two assessors. The relationship between the two systems was examined by tabular and correlational analysis.
Results:
The findings showed that the symptoms of borderline personality disorder were associated with greater severity of personality disturbance in the International Classification of Diseases, 11th Revision classification (p < 0.0001) and were associated primarily with the Negative Affective, Dissocial and Disinhibited domains. There was only a weak association with the other two domains, Anankastia and Detachment.
Conclusion:
The addition of a borderline pattern descriptor is likely to add little to the International Classification of Diseases, 11th Revision classification of personality disorder. Its features are well represented within the severity/domain structure, which allows for more fine-grained description of the personality features that constitute the borderline concept.
Keywords
Introduction
The International Classification of Diseases, 11th Revision (ICD-11) classification of personality disorders (PDs) represents a radical change from the International Classification of Diseases, 10th Revision (ICD-10) classification. Individual PD categories have been removed and replaced by a core diagnosis of PD which can be specified as mild, moderate or severe. Clinicians can then choose to describe PD features by specifying one or more trait domains: Negative Affectivity, Detachment, Disinhibition, Dissociability and Anankastia. However, one feature of the ICD-10 classification remains; the borderline pattern qualifier which essentially lists the symptoms of Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) borderline personality disorder (BPD) and ICD-10 Emotionally Unstable (borderline) diagnosis (see Supplemental Appendix 1 for the World Health Organization [WHO] description of the Borderline Specifier).
The retention of a borderline pattern descriptor remains contentious. Its presence is a pragmatic compromise to assuage the concern of some clinicians and researchers, as well as the International, European and North American Societies for the study of PDs. Their concerns focused on the magnitude of change in the classification of PDs and the loss of BPD which has been the most studied PD with regard to aetiology and treatment (Herpertz et al., 2017; Reed, 2018). However, the new ICD-11 borderline pattern qualifier has also been questioned since it was proposed (Hopwood et al., 2019). Some have argued that there is no scientific basis for its inclusion (Watts, 2019; Irwin and Malhi, 2019; Livesley, 2019).
There remains a lack of evidence that BPD is a unified syndrome. On the contrary, there is a well-established problem of excessive co-occurrence with other forms of personality pathology (Tyrer, 2009). A recent meta-analytic study of the DSM-5 Alternative Model for Personality Disorder personality facet criteria reported that while six of the seven trait facets proposed for BPD reached a meaningful level of association, so did 11 of the 18 nonproposed facets, highlighting this problem of excessive co-occurrences (Watters et al., 2019). Similarly, Sharp et al. (2015), when analysing PD criteria, found strong support for a latent factor underlying the nine BPD criteria. However, when the analysis included the other PD criteria, including a general factor, the BPD items loaded virtually entirely on the general PD factor and there was no specific BPD factor. In other words, BPD symptoms ‘hung together’ when examined in isolation, but ‘disappeared’ into a general trait when modelled alongside other PDs (Sharp et al., 2015). One interpretation of this is that BPD criteria may capture a general impairment in personality functioning, particularly around self/interpersonal problems (Sharp, 2016).
The aim of this paper is to study the relationship of the borderline pattern qualifier to the five ICD-11 domains in a sample of depressed patients. To do this, we have used the DSM-IV BPD symptoms to derive the borderline pattern qualifier and then looked at the qualifier’s relationship to total personality symptoms across all domains, and within each of the five ICD-11 domains. The ICD-11 domains were derived via confirmatory factor analysis in an exploratory framework in a previous study (Mulder et al., 2016). We wished to test whether the borderline qualifier symptoms correlate strongly with overall severity of PD, and whether they add any descriptive value to the existing ICD-11 domains.
Method
Sample
The Structured Clinical Interview for Personality Disorder-II (SCID II) data were obtained from outpatients who were enrolled in one of four randomised controlled trials (RCTs) for the treatment of depression (combined sample N = 606). Two studies were drug trials, while the other two were psychotherapy studies. Details of each study are reported elsewhere (Carter et al., 2013; Joyce et al., 1994, 2002; Mulder et al., 2017).
The participants had all received a diagnosis of major depression and consented to participate in an RCT examining the efficacy of treatment for their depression. They were recruited from the community, the emergency psychiatric services, general practitioners and community mental health teams. Exclusion criteria were a diagnosis of schizophrenia, mania, severe substance use disorder (mild to moderate was acceptable) and significant physical illness. Two trials also excluded those who had not benefitted from psychotherapy over the prior year (Carter et al., 2013; Mulder et al., 2017). Participants were all recruited from the same geographic area, Canterbury, New Zealand, and were similar with regard to demographic and diagnostic variables.
Personality assessment
All subjects were administered the SCID II in a face-to-face interview. The SCID II is a clinician administered semi-structured interview for diagnosing the 10 Axis II PDs in DSM-IV (and now DSM-5). Consistent with SCID II instructions, patients filled out a self-report questionnaire that enabled clinicians to focus on items corresponding to positively endorsed personality questions. Because all patients were depressed when entering the studies, the SCID II was administered at 4 to 6 weeks after enrolment. Patients and clinicians were instructed to try and rate PD symptoms when patients were not depressed.
ICD-11 personality domains
Two authors (R.T.M. and P.T.) independently assigned each DSM PD symptom into one of the five proposed ICD-11 domains. Symptoms judged to not fit into any domains were categorised as not addressed. When the raters disagreed, this was resolved by review and discussion. The SCID II contains a total of 79 symptoms; 57 symptom criteria were selected for inclusion in the study, with a further 22 classified as not addressed (Mulder et al., 2016). Confirmatory factor analysis of the item data showed that the 57 items could be scaled on five factors that corresponded broadly to the ICD-11 PD domains, with some items loading on more than one factor. The number of items (out of 57) classified into each of the five ICD-11 PD domains were, respectively: Disinhibition (18 items); Dissociality (9 items); Negative Affectivity (16 items); Detachment (10 items); and Anankastia (10 items). See Supplementary Table S1 for the full list of selected symptoms loading on each domain.
Statistical modelling
Symptom score counts were constructed by summing the symptoms assigned to each of the five ICD-11 PD symptom domains and combined across all domains. Associations between DSM-IV BPD symptoms, diagnosis and ICD-11 symptom scores were tested using the Mantel–Haenszel chi-square test for linear trend (for individual BPD symptoms, diagnosis), or linear regression (for total BPD symptom score count). The strength of each association was summarised by the correlation (r) between the DSM-IV BPD symptom measure and the ICD-11 PD symptom count. Point biserial correlations were used for individual BPD symptoms and BPD diagnosis, and the product moment correlation for the BPD symptom count.
Results
Table 1 shows the profile of borderline symptoms and BPD diagnosis cross-classified against the total PD symptom score created from the sum of all 57 PD symptoms assigned to the five ICD-11 domains. For ease of data display, the total PD symptom count has been classified into a series of class intervals ranging from those in the lowest quartile of symptom scores (0–2 symptoms) to those whose scores placed them in the highest decile of the distribution (16+ symptoms). For each association, the table also reports a test of linear trend and the correlation (r) between the BPD symptom measure and the total PD symptom score.
Profile of borderline symptomatology against total PD symptoms score.
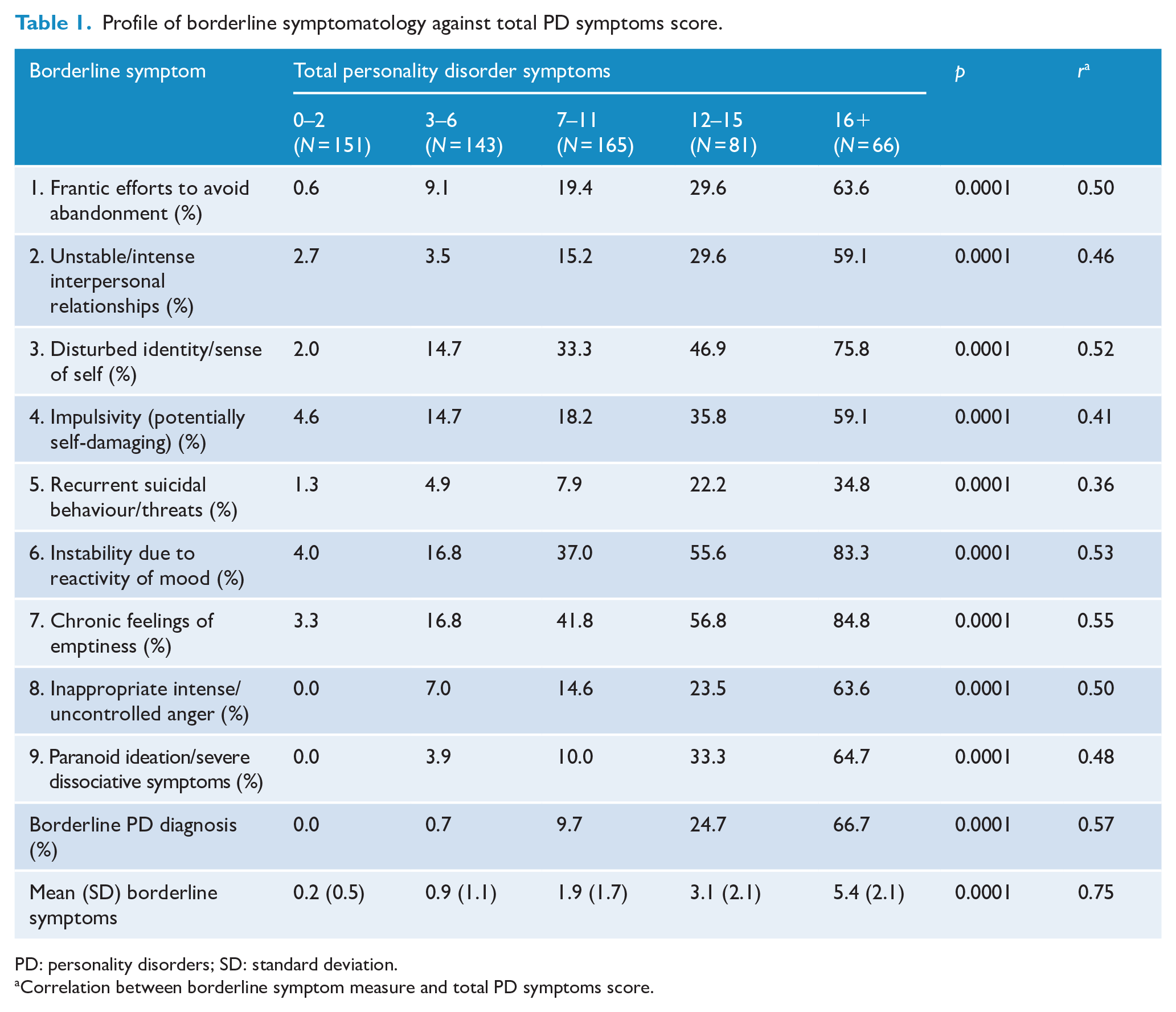
PD: personality disorders; SD: standard deviation.
Correlation between borderline symptom measure and total PD symptoms score.
Examination of the table shows a pervasive pattern of strong and statistically significant (p < 0.0001) associations reflecting increasing prevalence of BPD symptoms with increasing severity of overall PD symptomatology. Those in the highest decile of overall PD symptoms typically had very high rates of BPD symptoms (range 35%–85%) compared to those in the lowest quartile of PD symptomatology (range 0%–5%). Overall, 13.3% of the sample met criteria for a BPD diagnosis, and of these more nearly three quarters (72%) fell into the top two levels (highest quartile) of overall PD symptoms. The correlations of the various BPD symptom measures with total PD symptom score were uniformly strong (r = 0.36–0.55), and even stronger for the BPD diagnosis, total BPD symptom measures (r = 0.57, 0.75).
The clear impression conveyed by these results is that, in general, severity of overall PD symptomatology was strongly reflected in severity of BPD symptoms and vice versa.
Table 2 shows the correlations of BPD symptoms/diagnosis with total symptom scores calculated for each of the five ICD-11 domains. The full symptom profiles for each domain are given in Supplement Tables S2–S6. Examination of the tables suggests some variation in the strength of associations across the different domains. For Disinhibition and Dissociality, the pattern of associations was very strong and similar to that observed for the total PD symptom score in Table 1. Correlations with individual BPD symptoms ranged from r = 0.47–0.65 (Disinhibition) and r = 0.33–0.76 (Dissociality); correlations with BPD diagnosis and total BPD symptoms were respectively r = 0.73, 0.91 (Disinhibition) and r = 0.63, 0.72 (Dissociality).
Correlations (r) between DSM-IV BPD symptoms, diagnosis and ICD-11 PD symptom domain scores.
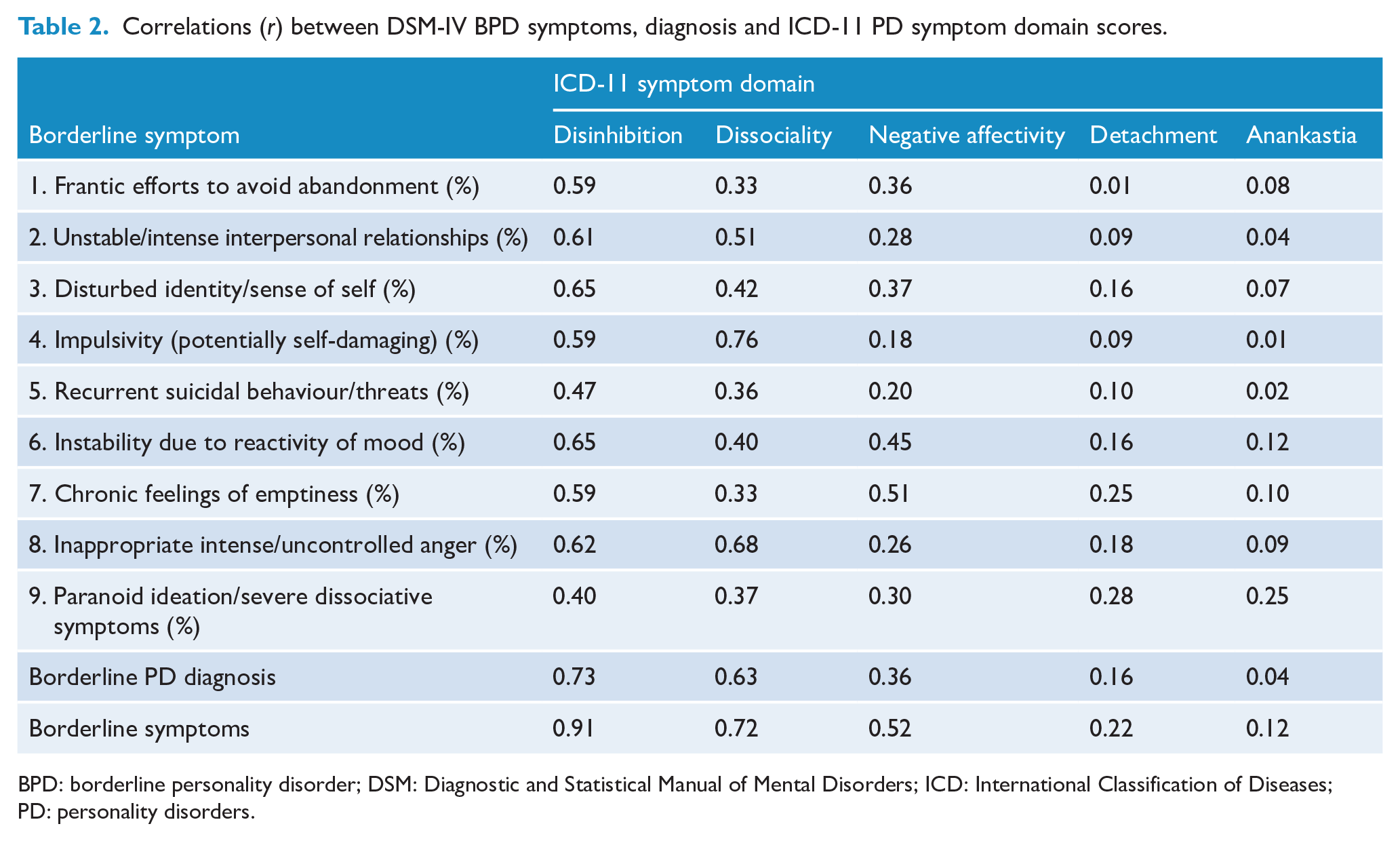
BPD: borderline personality disorder; DSM: Diagnostic and Statistical Manual of Mental Disorders; ICD: International Classification of Diseases; PD: personality disorders.
The Negative Affectivity domain exhibited a more moderate pattern of associations (r = 0.18–0.51 for symptoms, r = 0.36, 0.52 for diagnosis, total BPD symptoms); while the associations with Detachment (r = 0.01–0.28 for symptoms, r = 0.16, 0.22 for diagnosis and total BPD symptoms) and Anankastia (r = 0.01–0.25 for symptoms, r = 0.04, 0.12 for diagnosis, total BPD symptoms) were generally in the range from weak to non-existent.
A potential limitation of the above analysis is that the PD symptom criteria selected for inclusion in the ICD-11 PD domains included a total of seven of the BPD symptom criteria (see Supplementary Table S1), spread across the Disinhibition, Dissociality and Negative Affectivity domains. This raises the possibility that the observed associations above may simply reflect the inclusion of these BPD symptoms in calculating the PD domain scores. To examine this possibility, a sensitivity analysis was conducted in which all BPD symptom criteria were excluded from the relevant ICD-11 domain symptom scores and the total PD symptom count. The results of this analysis are summarised in Table 3 which shows the correlations between BPD symptoms and the relevant ICD-11 PD domain scores calculated excluding all BPD symptoms. The table shows that while there was some attenuation in the strength of associations (compared to those in Tables 1 and 2) when BPD symptoms were excluded, nevertheless there remained a consistent pattern reflecting moderate to strong associations between BPD symptoms and the relevant PD domain scores.
Correlations (r) between DSM-IV BPD symptoms, diagnosis and relevant ICD-11 PD symptom domain scores (excluding BPD symptoms).
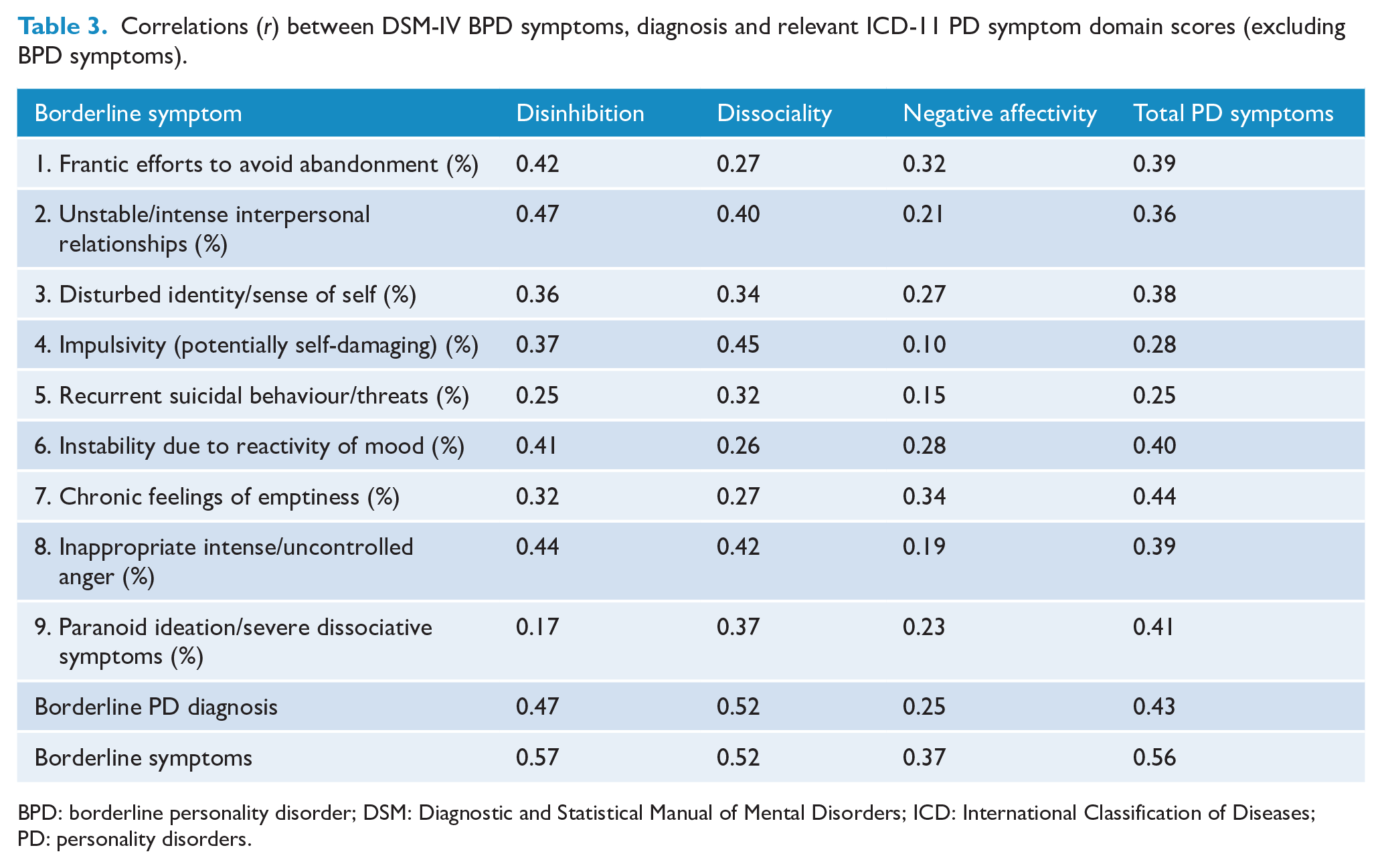
BPD: borderline personality disorder; DSM: Diagnostic and Statistical Manual of Mental Disorders; ICD: International Classification of Diseases; PD: personality disorders.
Discussion
The results show that there is a very strong relationship between the borderline pattern qualifier symptoms and the overall severity of personality pathology (r = 0.75 mean borderline pattern symptoms). In addition, borderline pattern symptoms are highly correlated with the Disinhibition (r = 0.91) and Dissociality domain (r = 0.72) symptoms, moderately to strongly correlated with the Negative Affectivity domain (r = 0.51), and weakly related to the Detached (r = 0.22) and Anankastia (r = 0.12) domains.
These results are consistent with studies that have explored the relationship between BPD symptoms and other PD symptoms. As noted above, Sharp et al. (2015) and Watters et al. (2019) reported excessive overlap with other PD symptoms and a strong association with general PD severity. This has led to suggestions that BPD criteria and the borderline pattern qualifier may actually capture the impairment in personality functioning as defined by the general description of PD in ICD-11. In other words, fulfilling the borderline pattern may be little more specific than qualifying for having a moderate or severe PD.
It is also clear that, as expected, borderline qualifier symptoms were strongly correlated with two domains; Disinhibition and Dissociality, and moderately to strongly correlated with Negative Affectivity. Whether adding the borderline qualifier to a description using these domains has any advantages is unclear. It may be that describing the PD features using the domains results in a more nuanced and complex description of individuals we would currently see as having BPD. It may also lead to the potential of trying different treatments with heterogeneous groups of patients now called BPD. For example, an individual with more Dissociality domain features might require a lengthier and more complex psychotherapy than one with predominantly Negative Affectivity. Bateman et al. (2016) reported that individuals with co-morbid antisocial and BPD needed a more complex and intense psychotherapy – in this case Mentalization-based Therapy – than those without antisocial features.
It should also be noted that the borderline qualifier is not a diagnosis but an alternative offered to those who do not feel the domain structure captures the elements of borderline pathology. The diagnosis of PD in ICD-11 remains on a single spectrum ranging from normal function to severe PD. It is possible, therefore, for those with the subsyndromal disorder of personality difficulty, as well as mild PD, to qualify for the borderline qualifier. It will be a matter of research interest to find out how many might fulfil criteria for the qualifier at lower levels of pathology, not least as there tends to be an increase in domains identified in those with greater severity of disorder (Tyrer et al., 2019).
Limitations
A major potential limitation is that the PD domain symptom scores include BPD symptoms. This means that there is obvious tautology in some of our findings. This is primarily an issue for the Disinhibition domain (7 out of 18 symptoms were BPD), but to a lesser degree, also for the Dissociality and Negative Affective domains (see Supplementary Table S1). The moderate to strong associations observed for these domains reflect this relationship to some extent. The tautology is largely unavoidable since the borderline qualifier was added to domain description late in the classification. The domain descriptions already included content such as emotional liability, separation insecurity and impulsivity which overlap with the borderline descriptor. Sensitivity analysis showed that a similar but mildly attenuated pattern of findings persisted even when BPD symptoms were excluded from the PD domain symptom scores. This clearly suggests that borderline symptoms are relevant to the elaboration of broader PD symptomatology, but still begs the question of what the borderline descriptor adds to the PD diagnosis.
A second limitation relates to the nature of the analysis sample, which combined participant data from a series of five RCTs for treatment of depression. The studies were not designed for the purpose of examining PD diagnostic models. However, because exclusion criteria were minimal, more than 40% fulfilled criteria for a PD diagnosis. In this sample, the most common PD symptoms were those in the Negative Affectivity and Anankastia domains, with symptoms in other ICD domains typically being of lower prevalence. It is possible that findings would be different in other clinical contexts where different patterns of PD symptomatology may occur.
Conclusion
The borderline pattern qualifier was an attempt to retain some continuity between ICD-10 and the paradigm shift in ICD-11 PD diagnosis. BPD is the most studied of all PDs, particularly with regard to treatment, and its retention may have reassured some clinicians. However, the fundamental problem that factor analytic studies over the past 20 years have failed to support a categorically defined BPD analysis (Sharp, 2016) has not gone away. From our data, the borderline pattern descriptor appears to be correlated with overall personality pathology and a mixture of Disinhibited, Dissociality and Negative Affectivity domain symptoms. Whether using the qualifier adds anything to describing PD severity and domains remains to be seen. Hopefully, clinicians will try both models to test which is more clinically useful.
Supplemental Material
Supplementary_Material – Supplemental material for The borderline pattern descriptor in the International Classification of Diseases, 11th Revision: A redundant addition to classification
Supplemental material, Supplementary_Material for The borderline pattern descriptor in the International Classification of Diseases, 11th Revision: A redundant addition to classification by Roger T Mulder, L John Horwood and Peter Tyrer in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: P.T. and R.T.M. are members of the ICD-11 Personality Disorder Classification Committee.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.