
Abstract
To the Editor
Logopenic variant primary progressive aphasia (lvPPA) is the most common nonamnestic phenotypic variant of young-onset Alzheimer’s disease (Mendez, 2019). LvPPA patients exhibit deficits in naming and repetition in the context of spared semantic, syntactic and motor speech abilities. The neuropsychiatric symptoms are relatively infrequently early (Modirrousta et al., 2013). On the contrary, patients with behavior variant frontotemporal dementia (bvFTD) have prominent behavior symptoms, but less language deficits than patients with primary progressive aphasia (PPA) (Liu et al., 2019). It is challenging to differentiate lvPPA from bvFTD in patients with prominent behavioral symptoms with subtle language deficit at the beginning of the illness, and an accurate diagnosis could potentially alter treatment strategy.
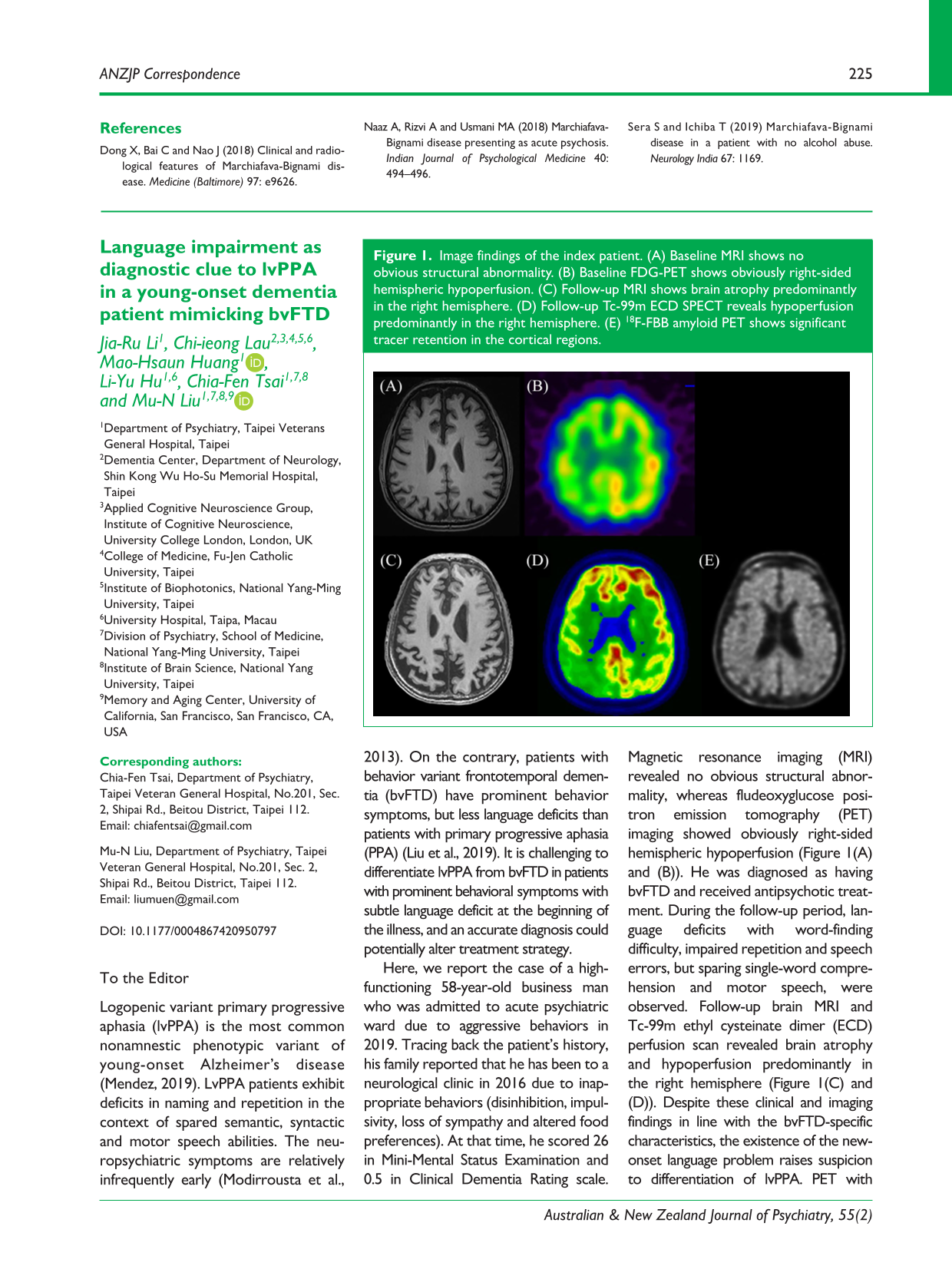
Here, we report the case of a high-functioning 58-year-old business man who was admitted to acute psychiatric ward due to aggressive behaviors in 2019. Tracing back the patient’s history, his family reported that he has been to a neurological clinic in 2016 due to inappropriate behaviors (disinhibition, impulsivity, loss of sympathy and altered food preferences). At that time, he scored 26 in Mini-Mental Status Examination and 0.5 in Clinical Dementia Rating scale. Magnetic resonance imaging (MRI) revealed no obvious structural abnormality, whereas fludeoxyglucose positron emission tomography (PET) imaging showed obviously right-sided hemispheric hypoperfusion (Figure 1(A) and (B)). He was diagnosed as having bvFTD and received antipsychotic treatment. During the follow-up period, language deficits with word-finding difficulty, impaired repetition and speech errors, but sparing single-word comprehension and motor speech, were observed. Follow-up brain MRI and Tc-99m ethyl cysteinate dimer (ECD) perfusion scan revealed brain atrophy and hypoperfusion predominantly in the right hemisphere (Figure 1(C) and (D)). Despite these clinical and imaging findings in line with the bvFTD-specific characteristics, the existence of the new-onset language problem raises suspicion to differentiation of lvPPA. PET with 18F-florbetaben was arranged, which showed radioligand binding in the cortical regions, indicative of high amyloid burden (Figure 1(E)). A diagnosis of lvPPA was established and cognitive enhancer was added as the patient’s main treatment strategy soon.
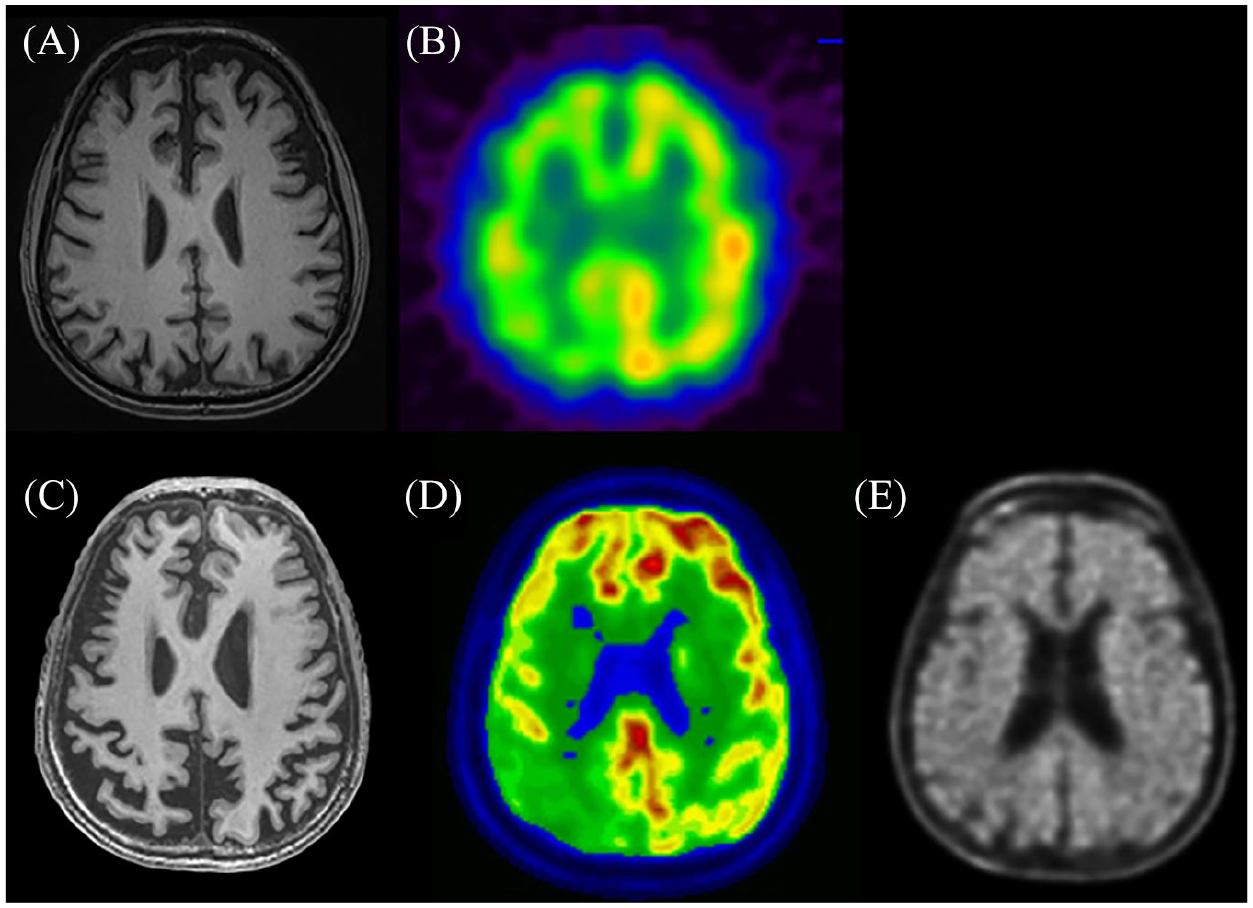
Image findings of the index patient. (A) Baseline MRI shows no obvious structural abnormality. (B) Baseline FDG-PET shows obviously right-sided hemispheric hypoperfusion. (C) Follow-up MRI shows brain atrophy predominantly in the right hemisphere. (D) Follow-up Tc-99m ECD SPECT reveals hypoperfusion predominantly in the right hemisphere. (E) 18F-FBB amyloid PET shows significant tracer retention in the cortical regions.
This case illustrates the complexity of the differential diagnostic processes in young-onset dementia, suggesting that language profile should be taken into account when differentiating lvPPA from bvFTD in patients with behavior symptoms. We also highlight that lvPPA patients could present with neuropsychiatric symptoms and obviously right-sided hemispheric hypoperfusion at the beginning of the illness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.