
Abstract

Introduction
The term ‘resilience’ is used widely across many domains of human endeavour, including sports, personal development and education. However, it has also become a familiar term in the management of mental illness as the fourth ‘R’ – beyond response, remission and recovery – providing a focus for many therapeutic approaches, including, for example, psychological interventions. But what is resilience? Is it an intrinsic quality, an attribute derived largely from our genetic makeup – or is it an acquired property – something that is created? Our language would seem to suggest that resilience is both, an innate trait and an attribute that we develop. For example, we often speak of being ‘naturally’ resilient but, at the same time, refer to the process of ‘building’ resilience. In this brief Make News article, we examine this important property more closely, and proffer a model that links adversity and resilience.
In common with others, our model of resilience retains both intrinsic and built components, but we introduce some additional concepts that we believe will advance our understanding of the construct – as one that evolves and is dynamic in nature. We hypothesise that to cultivate resilience properly and to its full extent, it has to be moulded to our circumstances and facilitated to grow, akin to the processes entrained within neuroplastic development, which increases markedly during adolescence. We thus consider resilience to be a skill, that invariably needs impetus but equally, if not more importantly, needs training and honing that only adversity can provide. Hence, we propose the term adversity-predicated resilience.
Conceptualising resilience
It is well established that stress is harmful and that it damages many systems within the body, both acutely and over the longer term, but it is important to note that not all stress is damaging per se. Nocent stress is the source of many mental and physical health problems and maladaptive behaviours that decrease overall well-being. This kind of stress is often threat related (e.g. various forms of abuse) or deprivation related (e.g. neglect), and collectively, these are broadly referred to as adversity. However, not everyone exposed to these adverse experiences, even when they are severe and protracted, necessarily goes on to develop problems. Individuals who manage to stave off such difficulties and endure are usually those who have been able to cope and retain some degree of functioning, despite adversity. This is the quality that is generally described as ‘resilience’.
There are many different perspectives on the nature of resilience. Some consider it to be a ‘trait’ – that you either possess from the outset of life or lack altogether. Others regard it merely as the absence of psychopathology. The diametrically opposed views seem to suggest that if you do not have innate resilience, you cannot develop it at any time, or that if you have psychopathology, you cannot be regarded as resilient. Empirically, the extremes of these perspectives do not appear to hold, and theoretically, the explanations offer few insights.
It is these limitations that have led to a paradigm shift in the conceptualisation of resilience, and therefore, increasingly, it is viewed as a multifaceted dynamic process, that involves the acquisition and application of new skills. It is also dependent on individual factors and subject to environmental influences and hence why it is variable in its manifestations. However, one consistent association is the context within which resilience invariably emerges, namely, adversity.
The emergence of resilience
Although we may be able to describe a person overall as showing resilience and having or being resilient, we are unable to say precisely when this happens or indeed how. Specifically, we are unable to give an account of the driving factors and the steps involved. All we can say is that the process is likely to be variable and complicated. We have an appreciation of this partly because the context which forges resilience – i.e. adversity – is itself highly diverse and multifaceted. For example, there are many kinds of stressors and they all can vary in intensity/severity and duration, and they each modify the stress–response systems within the body to different extents. This inherent variability and complexity in the nature of adversity that is thought to produce, or least mould resilience, has made it difficult to gain a deep understanding of resilience. It is to this end, to assist our future research endeavours, that we have developed an integrated resilience model (Malhi et al., 2019) that can perhaps capture its evolution and provide us with essential insights.
Our model (Malhi et al., 2019) is composed of three key components (see Figure 1); the most basic of which consists of intrinsic factors such as personality and plasticity genes, which we refer to as intrinsic resilience (Ri). These intrinsic factors are present from the beginning and are found both in the context of adversity and outside of it. It is these intrinsic factors that are susceptible to change in response to adversity, as may Ri, and it is this component of resilience that is commonly assessed using various resilience scales.
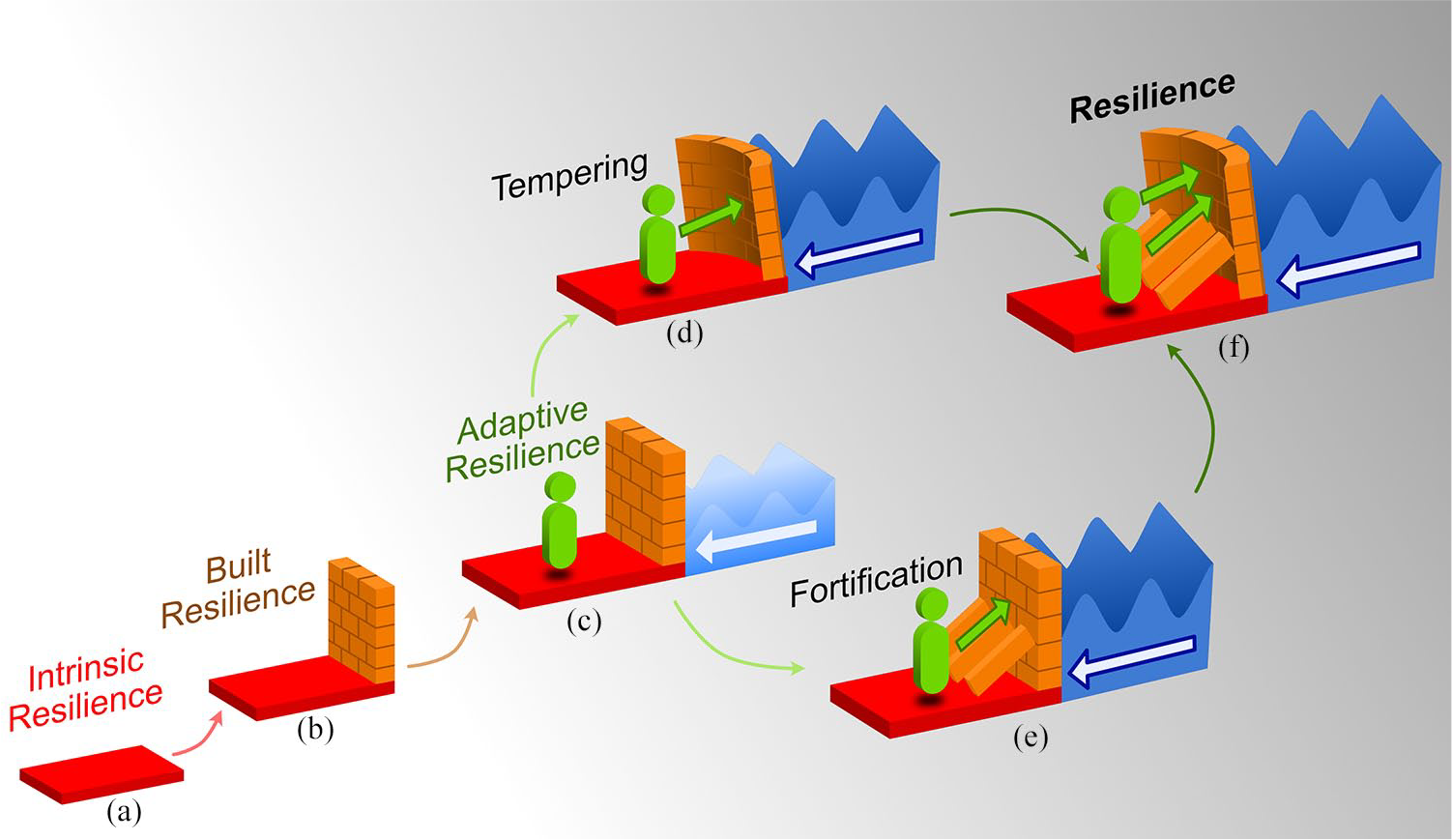
Schematic of the components of resilience comprising intrinsic, built and adaptive resilience linked by the coloured arrows. (a) Intrinsic resilience is based on personality and genetic factors (represented by the red base), while built resilience (b; represented by the orange wall superimposed on the red base) develops over time, from childhood to adulthood, with nurturing and supportive environments or in response to mild stressors. Adversity is not a required prerequisite for both intrinsic and built resilience to emerge, but it is necessary for adaptive resilience (c). This is because adversity exerts variable pressure (represented by light to dark blue waveforms) on stress-responsive systems (neurobiological and psychosocial) that pre-existing intrinsic and built resilience cannot withstand. Therefore, the pressure eventually weakens and damages stress-responsive systems. However, the two processes that can withstand increasing pressure or allostatic load (represented by blue/white arrows showing the direction of applied pressure) are tempering (d) and fortification (e). The ability to withstand increasing pressure requires active engagement (represented by forward green arrows) to either deploy pre-existing skills for use in new contexts (tempering, depicted by curvature of the wall) or acquire additional skills to strengthen stress-responsive structures (fortification, depicted by bracing on the wall). Tempering can be fast and immediate but may be unstable, while fortification may be stable, but it is slow and takes time to develop. To enhance stability, flexibility and durability of stress-responsive systems, tempering and fortification have to be well coordinated (f; depicted by the tempered and fortified wall). Ultimately, tempering and fortification repair, modify and strengthen the integrity of stress-responsive systems to produce resilience.
In addition to Ri, our model also identifies the component of resilience that is built over time through neurophysiological and psychosocial development, from childhood to adolescence and beyond. We refer to this resilience as built resilience (Rb). We posit, that Rb emerges either from mild or positive stressors that are not sufficient to destabilise stress-responsive systems or from promotive psychosocial factors such as engagement in healthy lifestyles and supportive environments that harness positive emotions in daily life and provide a sense of security and self-worth. Importantly, and similar to Ri, this component of resilience (Rb) gradually builds independently of adversity. In other words, it is not reliant on adversity to take shape and form. However, as a consequence, it is likely to be somewhat fragile, and therefore, along with Ri, it remains vulnerable to adverse and uncontrollable situations.
By its nature, adversity is unpredictable in its intensity, severity and duration. At times, it can exert excessive ‘pressure’ (stress) on systems within the body that are designed to counter stress (stress-responsive systems). The pressure is a consequence of cumulative wear and tear of the body and brain that is sometimes referred to as ‘allostatic load’. In normal circumstances, the ‘damage’ caused by adversity-induced allostatic load (McEwen, 2005) undergoes active repair, and this leads to strengthening of stress-responsive systems. The mechanisms by which this occurs require the use of specific strategies that we have described as tempering and fortification (see Figure 1). And it is these strategies that form the adaptive component of resilience (Ra).
Tempering and fortification
Tempering involves the deployment of pre-existing but dormant skills for use in new contexts in response to increasing allostatic load. As tempering strengthens stress-responsive systems, it also introduces potential fragilities as the systems become more rigid – reflected as inflexibility or ‘brittleness’. This is the point at which fortification comes into play. Fortification is able to bolster any brittleness that may have been produced by the tempering process, and it does so by cultivating the acquisition of new skills. The development of these skills naturally takes time, but the investment is worthwhile as it is more likely to instil stability to systems that is ultimately more enduring. To achieve the most robust resilience, both processes are necessary. Tempering, on its own for instance, is more immediate – a quick fix – but it is not as enduring as having additional fortification. We hypothesise that all these processes are activated by adversity to operate in a coordinated and seamless manner to repair failing, compromised or impaired systems, while strengthening weakened ones, and this eventuates in adaptive resilience (Ra). However, it is important to note that not everyone with adversity will necessarily achieve Ra by virtue of simply having experienced adversity because the process requires active participation.
An integrated model of resilience
Our integrated resilience model proposes that stress-responsive systems have to be ‘tested’ by adversity for resilience to fully form. It features intrinsic (Ri) and built (Rb) resilience as building blocks without which Ra (see Figure 1) would not be fully achieved. This means that certain capabilities (innate or built) are necessary for the deployment of old capabilities and acquisition of new ones.
Developmental mechanisms
Stress-responsive systems are multifaceted and consist of both neurobiological and psychosocial components. Importantly, they are systems that are adaptive by nature and are designed to flourish in optimal conditions and environments. Examples of such systems include the hypothalamic–pituitary–adrenal (HPA) axis, the autonomic nervous system (ANS) and the immune system, which cooperatively effect changes in the neurocircuitry of emotion regulation (ER), cognitive processing and social behaviour. Together, they make us adaptive beings.
While Ri is related to intrinsic factors that interact with the environment to exert effects on the underlying neurocircuitry of the brain and its functions, it is, nonetheless, a largely ineffective component of resilience in the context of severe and novel adversity – especially when deployed alone. Similarly, Rb, which manifests in stress-responsive systems predominantly prior to adversity, is also insufficient to counter mounting adversity. It is therefore at this point that tempering and fortification assume the responsibility of repairing stress-responsive systems and strengthening them by enhancing and modifying weaknesses within the neurocircuitry and functioning of the brain – that has been caused by adversity-induced allostatic load.
How these systems respond to adversity also depends on the individual’s overall development. For instance, in childhood, the prefrontal cortex (PFC) is not yet fully equipped to cultivate necessary connections and has only rudimentary capabilities as regards functions such as adaptive ER and decision-making, which only begin to undergo sophisticated development and consolidation upon entering adolescence. Importantly, as the brain develops in adolescence and significant neuroplasticity occurs, an opportunity to assess the changes that are related to normal, aberrant and adaptive development (indicative of Ra) emerges. At the same time, adolescence typically features an increase in environmental demands accompanied by heightened sensitivity to social cues, and this provides a potential window for the nuanced investigation of adverse events and their consequences.
Implications for research and clinical practice
Fostering resilience is critical to the reduction of maladaptive behaviours, the promotion of health and the prevention and treatment of mental and physical health problems (Galatzer-Levy et al., 2018). However, a better understanding of its evolution from a developmental perspective necessitates a framework for research programmes with salience for clinical practice. For instance, augmentation of the amygdala–PFC coupling has been identified as a neural mechanism of adaptation (Ra), countering amygdala hyper-reactivity to adversity in adolescents (Herringa et al., 2016). Likewise, stronger connectivity between the hippocampus and the ventromedial PFC (vmPFC) during aversive learning prospectively predicted improvements in anxiety symptoms as an index of recovery (Ra) from a significant form of early adversity in adolescents (Silvers et al., 2016). However, the evolution of these factors in response to adversity cannot be determined with confidence from cross-sectional studies alone, and therefore, prospective longitudinal studies are needed.
Conclusion
Resilience is increasingly considered a dynamic construct, and in our proposed model, it is a skill that confers adaptation. At its core, we define resilience as the adaptation of neural systems and their elaborate physiological, cognitive and behavioural manifestations in response to adversity-induced allostatic load. The evolution of resilience involves a number of key processes that build resilience on the foundation of intrinsic factors. Subsequent tempering and fortification in response to adversity leads to Ra that enables stress-responsive systems to counter allostatic load. Our adaptive model that is adversity predicated is promising because it affords opportunities for the development of preventive interventions and treatments. Thus, given adolescence is a critical period of brain maturation and the time during which Ra forms, this is where research efforts into understanding resilience need to be focussed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. G.W.M. is a consultant for Akili, Alkermes, Allergan, Axsome, Ironshore, Intracellular, Janssen, Lundbeck, Otsuka, Neos Therapeutics, Purdue, Rhodes, Sage, Sunovion, Takeda and Teva; has received research grants from Akili, Alkermes, Allergan, Axsome, Boehringer, Janssen, Lundbeck, Medgenics, NLS-1 Pharma AG, Otsuka, Reckitt Benckiser, Roche, Sage, Sunovion, Supernus, Takeda and Teva; and received speaker/promotional honoraria from Alkermes, Allergan, Ironshore, Janssen, Lundbeck, Otsuka, Sunovion and Takeda. The authors P.D., E.B. and Z.M. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.