
Abstract
Objective:
To conduct a meta-analysis of Theory of Mind studies exclusively in euthymic patients with bipolar disorder.
Method:
After the exclusion of studies evaluating symptomatic patients during acute episodes, we performed a meta-analysis including a total of 30 studies, comparing 1294 euthymic bipolar disorder patients and 1116 healthy controls.
Results:
Patients with bipolar disorder presented a significant impairment in Theory of Mind performance when compared to controls (Hedge’s g = −0.589, 95% confidence interval: −0.764 to −0.414, Z = −6.594, p < 0.001). When compared to controls, Theory of Mind was impaired in patients with both bipolar disorder I (Hedge’s g = −0.663, 95% confidence interval: −0.954 to −0.372, Z = −4.462, p < 0.001) and bipolar disorder II (Hedge’s g = −1.165, 95% confidence interval: −1.915 to −0.415, Z = −3.044, p = 0.002). Theory of Mind impairments were also significantly more severe in verbal tasks (Hedge’s g = −1.077, 95% confidence interval: −1.610 to −0.544, Z = −3.961 p < 0.001) than visual tasks (Hedge’s g =−0.614, 95% confidence interval: −0.844 to −0.384, Z = −5.231, p < 0.001) when compared to controls.
Conclusion:
The results obtained confirm that Theory of Mind is impaired in remitted bipolar disorder patients, being a potential endophenotype for bipolar disorder. Moreover, we found higher deficits in verbal Theory of Mind, compared with visual Theory of Mind. Since most studies were cross-sectional, there is a need for longitudinal studies to evaluate whether the deficits detected in Theory of Mind are progressive over the course of the illness.
Introduction
Bipolar disorder (BD) is a chronic and disabling mental illness characterized by recurrent mood episodes, with periods of depressive symptomatology, as well as periods of remission of mood symptoms (Vieta et al., 2018). People with a BD diagnosis often suffer from lasting functional impairments and low quality of life, with subsyndromal symptoms and neurocognitive impairments being aspects that appear to increase the risk of low functioning and disability in BD patients (Sanchez-Moreno et al., 2009).
Data from various studies reveal that most BD patients exhibit neurocognitive dysfunction, present even during remission, with more pronounced effects in those with a more severe or chronic presentation (Bourne et al., 2013; Carvalho et al., 2015; Cullen et al., 2016; Robinson et al., 2006). Among these findings, the deficits concentrate in executive functions, attention, verbal learning, while premorbid intelligence appears to be preserved (Kurtz and Gerraty, 2009). Specific cognitive deficits are observed in euthymic BD patients such as verbal memory and speed of information processing, suggesting that deficits in such domains may actually be a useful cognitive endophenotype for BD (Balanzá-Martínez et al., 2008; Srivastava et al., 2019), being reported even during euthymia (Robinson et al., 2006). In contrast, moderate deficits found in relatives of patients with BD suggest that these cognitive deficits in BD patients might also indicate a consequence of disease-associated factors such as chronicity, multiple episodes, medication side effects and/or psychiatric comorbidities (Kapczinski et al., 2008). Evidence suggests that cognitive dysfunction is a pivotal mediator of negative psychosocial outcomes in BD and a predictor of adverse employment outcome (Baune and Mahli, 2015).
Social cognition (SC) is a field that aims to comprehend how brain function supports the cognitive processes of underlying social behavior and encompasses a complex set of processes which allow for adaptive social interaction. These involve the representation of internal somatic states, knowledge about oneself and others, interpersonal motivations and appropriate response to socioemotional information (Amodio and Frith, 2006). The National Institute of Mental Health (NIMH) has identified five core domains within this construct: Theory of Mind (ToM), Social Perception, Social Knowledge, Attribution Bias and Emotion Processing (EP) (Green et al., 2008). Despite the recent developments in research on the topic, studies lack a further investigation regarding association between SC domains and BD, such as ToM. There is evidence indicating that SC deficits are present in patients with BD even in remission (Samamé et al., 2012; Varo et al., 2019), although it is still not known if the deficits precede illness onset or are a consequence of the disorder. It is worth mentioning that SC evaluation involves a considerable number of tasks that vary in degrees of complexity. Also, the effects of neurocognitive deficits on SC can be considered an influence factor, meaning an impairment in one domain can have consequences in another (Samamé, 2013). SC performance may moderately influence neurocognitive functioning and seems to be a predictor of psychosocial outcome (Caletti et al., 2013); therefore, a better understanding of SC in BD should help us further understand the illness cognitive deficits mechanisms and develop new interventions.
ToM, an SC construct, and referred to as mentalizing, is the cognitive ability to infer mental states to others and oneself with respect to thought, emotion and intention. Hence, it is an essential skill for successful social interactions (Premack and Woodruff, 1978). ToM is essential for social development and interactions. It underlies the capacity to cooperate, empathize and accurately anticipate the behavior of others.
Impairment in ToM function has been identified in a variety of psychiatric disorders, including autism (Happé, 1994) and schizophrenia (Frith and Corcoran, 1996). The first study on ToM in BD was conducted by Doody and colleagues (1998), although only 2 of the 12 participants had a BD diagnosis and were psychotic during the testing. In 2003, Kerr and colleagues (2003) conducted the first study including only remitted BD patients. One study (Lee et al., 2013) indicated that BD patients did not differ statistically to HCs on SC, whereas other studies have reported impaired SC performances in BD, especially regarding the domains of ToM and Emotion Recognition (Bora et al., 2016; Cusi et al., 2012; Samamé, 2013). Regarding ToM and psychosocial functioning, studies vary in results, with some studies (Dalkner et al., 2019; Lahera et al., 2013) finding no change in psychosocial outcome in relation to ToM, and other authors reporting a significant relationship between ToM and Psychosocial Functioning (Caletti et al., 2013; Montag et al., 2010). Furthermore, some authors have suggested that cognitive ToM is more likely to be impaired than affective ToM in BD patients (Montag et al., 2010; Shamay-Tsoory et al., 2009). However, further studies are needed in order to explore the extension of social-cognitive impairments, differentiating cognitive vs affective ToM and, thus, being able to detect which is more impaired in BD.
ToM studies in BD patients have been previously reviewed in one major systematic review (Cusi et al., 2012) and two meta-analyses in the past decade (Bora et al., 2016; Samamé et al., 2012). Cusi et al. (2012) conducted a broad systematic review of the neural basis of SC in patients with mood disorders (BD and major depressive disorder), focusing on two domains: ToM and Emotion Comprehension, in neuroimaging studies, and including a total of 65 studies. However, studies that did not include control tasks or a comparator group were not included in this review. The results revealed that three studies showed that ToM deficits appear to persist into euthymic states in patients with BD, with one (McKinnon et al., 2010) finding ToM correlation with the neurocognitive domains of executive function and working memory. Samamé and colleagues (2012) conducted a meta-analysis with literature review exploring SC in euthymic adults with BD, including 46 studies exploring emotion recognition and ToM. The authors found that deficits in ToM and EP occur in euthymic BD patients, whereas decision-making appears to be preserved in this population. Bora and colleagues (2016) published a meta-analysis of ToM impairment in BD, which included remitted/subsyndromal and acute (depressive and manic) patients, albeit only 19 out of the 34 studies included in this meta-analysis had a euthymic BD sample. As a result, the authors concluded that ToM dysfunction is more pronounced during acute episodes, but deficits are also present during remission periods, suggesting that ToM impairment might be a trait-marker of BD. Finally, the authors suggest the need for future studies, with a larger sample size, and a more inquisitive investigation of a possible association between neurocognitive subdomains and ToM performance.
To date, no systematic review or meta-analysis had investigated the presence of ToM deficits in solely euthymic BD patients, although previous studies had conducted sub-analysis with euthymic sub-samples Bora and colleagues (2016) and Samamé and colleagues (2012). Also, since the previous meta-analysis, the updated literature has 14 new studies and demands a new analysis of its findings. The relevance of our meta-analysis relays on (1) the new studies that had been published since 2016, (2) the investigation of ToM deficits in studies that included only euthymic bipolar subjects and (3) a rigorous methodology that included only theses and full paper and peer-reviewed articles.
The aim of this article is to provide an updated comprehensive systematic review of controlled studies that investigated the ToM functioning in euthymic BD subjects and verify, via a meta-analysis, whether euthymic patients with BD present deficits in SC, more specifically in ToM. We chose to include tests that had appeared consistently in the studies conducted in this topic and for which data were available for the majority of patient samples.
Methods
Search strategy and eligibility criteria
The studies for this review were compiled by searching PubMed, Google Scholar, ResearchGate, Web of Science and PsychINFO databases and by examining reference/bibliography lists of relevant papers to locate additional studies that were not identified through the database searches. Databases were scanned from January 2000 until January 2019. To our knowledge, before January 2000, no full papers or theses were published with euthymic BD patients and ToM tasks. The first full paper that published with euthymic BD patients and ToM tasks was Kerr et al. (2003).
A systematic search of trials using the terms ‘Bipolar Disorder’ AND ‘Social Cognition’ OR ‘Theory of Mind’ OR ‘Mentalizing’ OR ‘Mind Reading’ was completed. Specific inclusion criteria for the studies included the following: (1) being published in English; (2) being a controlled study, with the inclusion of a psychiatrically healthy comparison group; (3) having at least 10 subjects in each arm (patient and comparison groups); (4) including only euthymic BD patients; (5) comparing ToM performance of BD patients with that of healthy controls.
Studies that include observational reports and case series were not included. All studies including patients having depressive, manic or hypomanic and/or subsyndromal episodes were excluded. Studies that only included an abstract were also excluded. Studies that included euthymic and non-euthymic BD patients but failed to provide separate data for each group were excluded. Finally, studies that did not provide information about the patients’ mood states and lack of specific data on BD’s ToM performance were excluded from the analysis. We also contacted seven authors for incomplete information and/or further clarification but received answer from only two authors with the requested data (Marotta et al., 2018; Ospina et al., 2018). The first and second authors (L.d.S.R. and G.H.B.) screened the full texts of these studies and any discrepancies were discussed between the authors until a consensus was reached. The authors also screened the references listed by each article selected.
Search results
A total of 30 studies (27 full papers and 3 theses) meeting the selection criteria were identified and thus considered for the present review (Table 1). The flow diagram summarizes the selection of the reviewed papers (Figure 1).
Characteristics of the studies included in the meta-analysis.
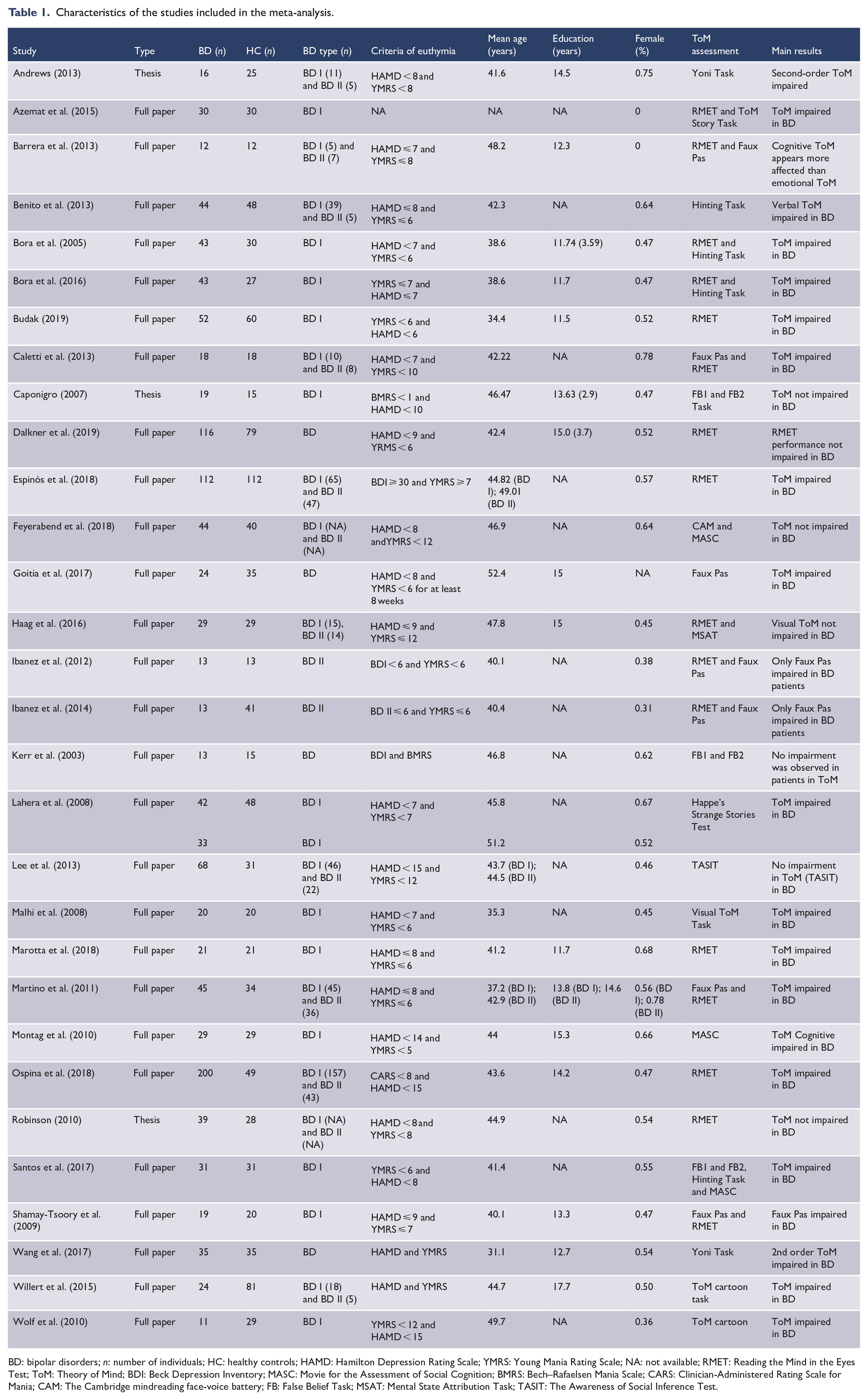
BD: bipolar disorders; n: number of individuals; HC: healthy controls; HAMD: Hamilton Depression Rating Scale; YMRS: Young Mania Rating Scale; NA: not available; RMET: Reading the Mind in the Eyes Test; ToM: Theory of Mind; BDI: Beck Depression Inventory; MASC: Movie for the Assessment of Social Cognition; BMRS: Bech–Rafaelsen Mania Scale; CARS: Clinician-Administered Rating Scale for Mania; CAM: The Cambridge mindreading face-voice battery; FB: False Belief Task; MSAT: Mental State Attribution Task; TASIT: The Awareness of Social Inference Test.
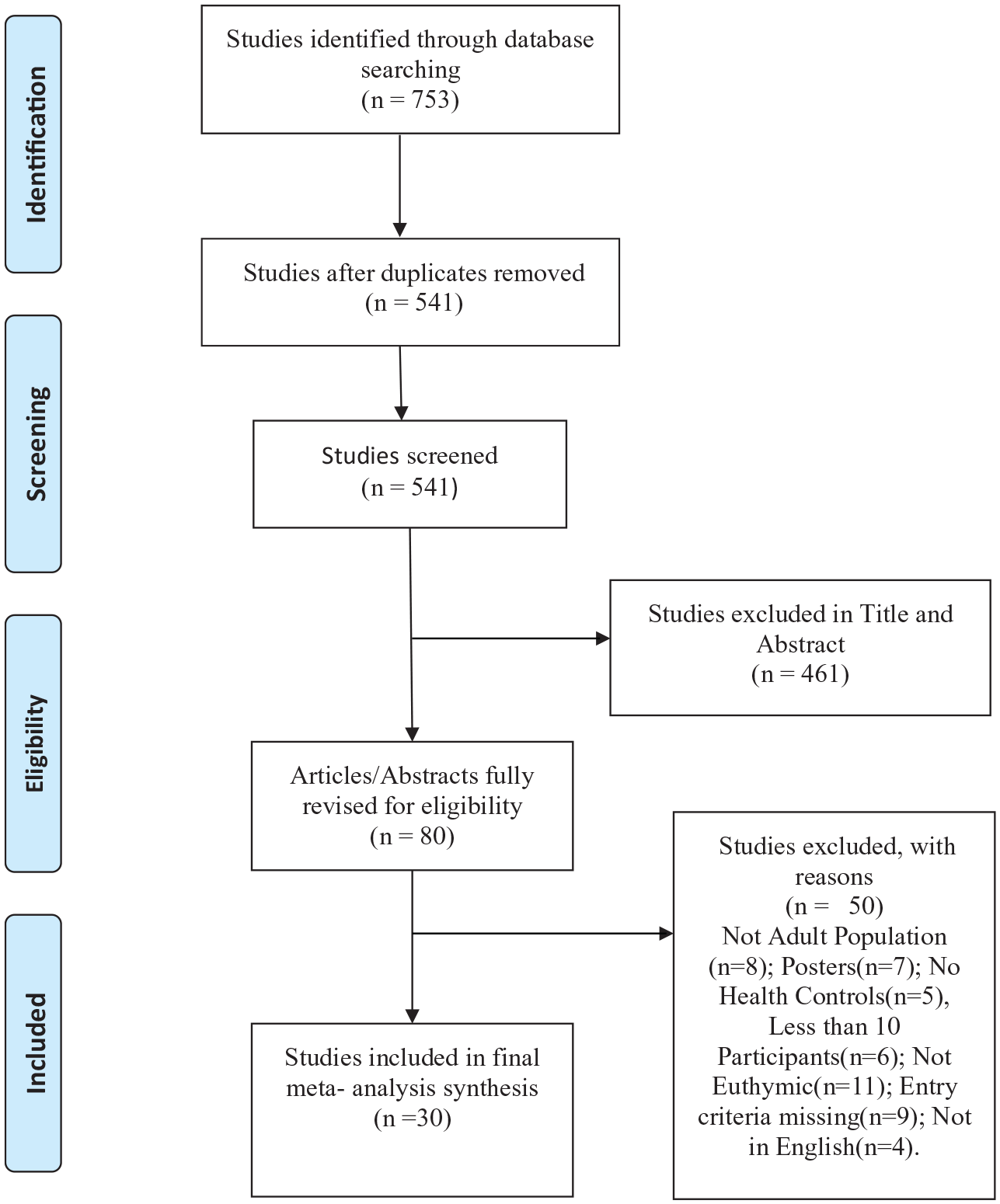
Flow diagram.
ToM measures
ToM can be measured by different instruments and diverse degrees of complexity. To understand the results, it is important to elucidate each instrument and its function. In this review, we examined in more depth the most commonly used ToM instruments that appeared in the selected studies (Reading the Mind in the Eyes Task [RMET], Faux Pas and Hinting Task).
RMET
One of the most used ToM tasks assesses the capacity to evaluate other mental states by watching the ocular region of faces (Baron-Cohen et al., 2001). This task consists in 36 pictures of the ocular region of varying unknown people and the subject must choose one out of four options that best describes the mental state observed. The task involves describing the emotional/mental state of a person based on only an image of their eyes, in a fixed-choice paradigm. The eye gaze is a non-verbal information about another person’s intentional state.
Faux Pas Recognition Task (adult version)
The name of the task can be roughly translated as False Step, and it assesses the subject’s ability to perceive when a social indiscretion occurs (Stone et al., 2002). A total of 20 short stories containing incidents of Faux Pas (someone mistakenly saying something they should not have) are read to the individual, who is then asked questions to determine whether or not they recognized the Faux Pas.
The Hinting Task
This task required the individual to be able to differentiate between literal and intended meaning (Corcoran et al., 1995). This task consists in 10 brief stories, all have two characters and at the end of each story, one of the characters drops a clear hint. The subjects are asked what the character in the story really wanted to say with the comment she or he made. Successful performance thus requires attribution of mental states such as desires, beliefs or intentions and sometimes higher order mental states such as one character’s belief about what another character knows.
Statistical analysis
The aim of the study was to verify, via a meta-analysis, whether euthymic patients with BD present deficits in SC, more specifically in ToM and compare the results verbal and non-verbal domain. The studies were analyzed in a meta-analysis using a random effects model. This model was chosen in the study design based on the putative heterogeneity contained in these studies, once different tasks and samples were assessed. The main outcomes were the scores obtained in the different ToM tasks.
The analysis was conducted with all individuals with BD, individuals with BD I or BD II separately and for three ToM tasks (RMET, Faux Paus Task and Hinting Task). These tasks were chosen once they were the most frequently used in the selected studies. The majority of the studies reported results from more than one ToM task. Each task was considered in the meta-analyses. Differently from Bora and colleagues (2016), we decided to analyze individual ToM tasks, rather than polled effect sizes from all ToM tasks, once we believe that polling data may lose statistical power.
Hedge’s g and its 95% confidence interval (95% CI) were used to calculate the summary effect sizes (Figures 2–4). Heterogeneity was assessed through Q test and I2 statistics. Publication bias was calculated by Egger’s test. Studies with a statistically significant publication bias were detected using such test; a funnel plot was performed (see Figure 5), and outlier studies were identified. Meta-regression was conducted to examine the effects of age, gender, illness onset, illness duration and education level in the meta-analyses results.
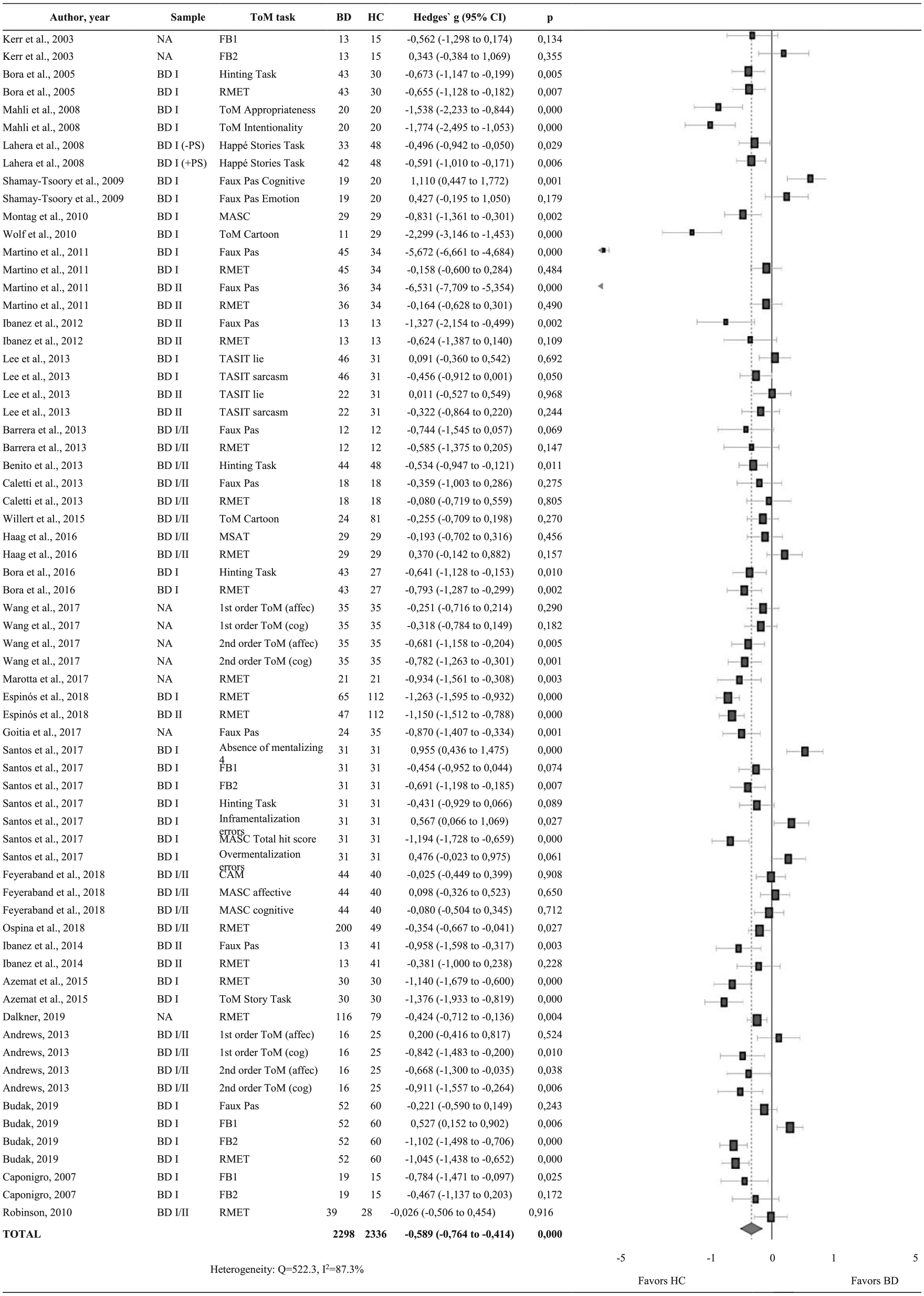
Summary of results and forest plots of meta-analyses comparing Theory of Mind (ToM) between individuals with bipolar disorders (BD) and healthy controls (HC).
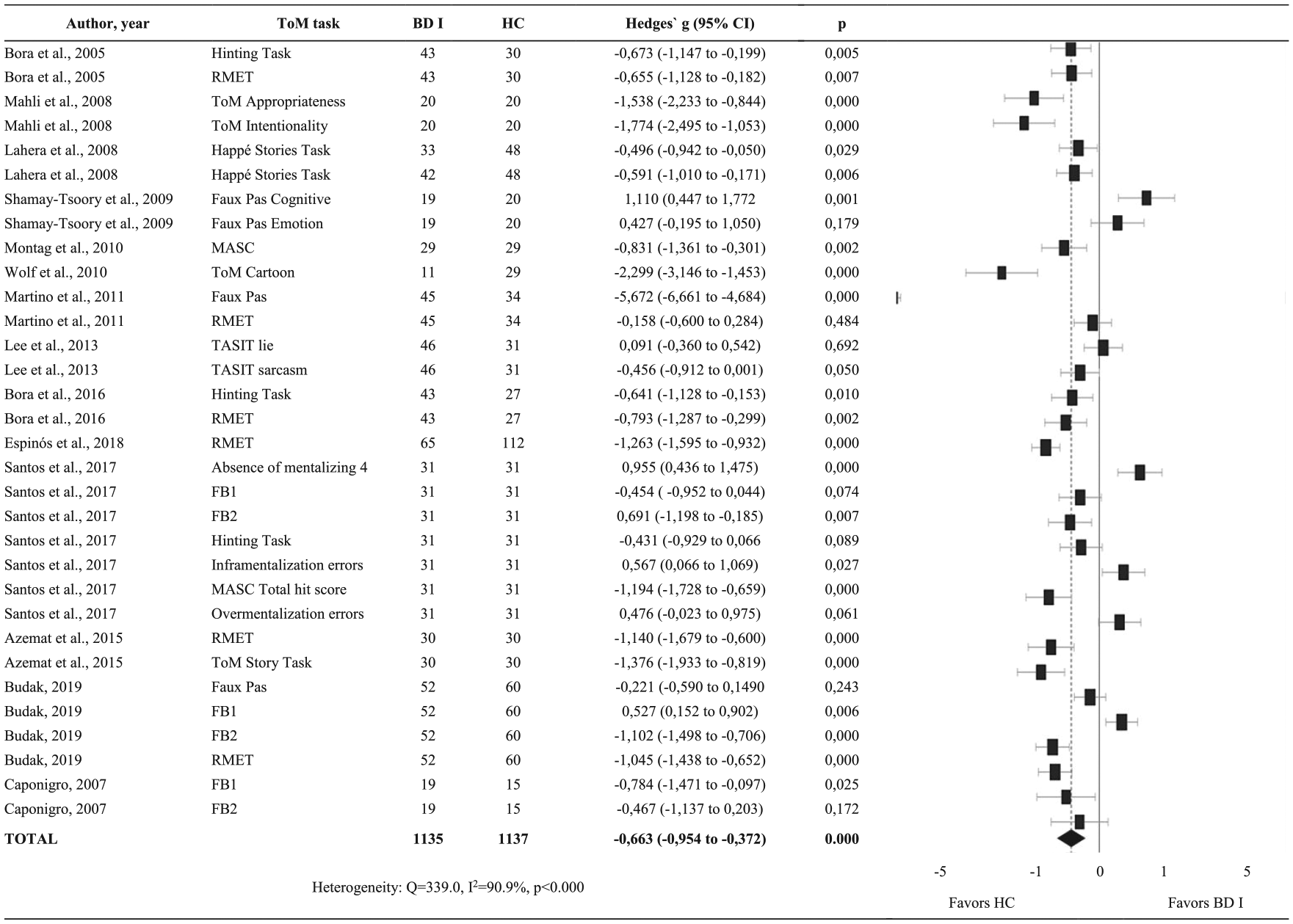
Summary of results and forest plots of meta-analyses comparing Theory of Mind (ToM) between individuals with type I bipolar disorders (BD I) and healthy controls (HC).
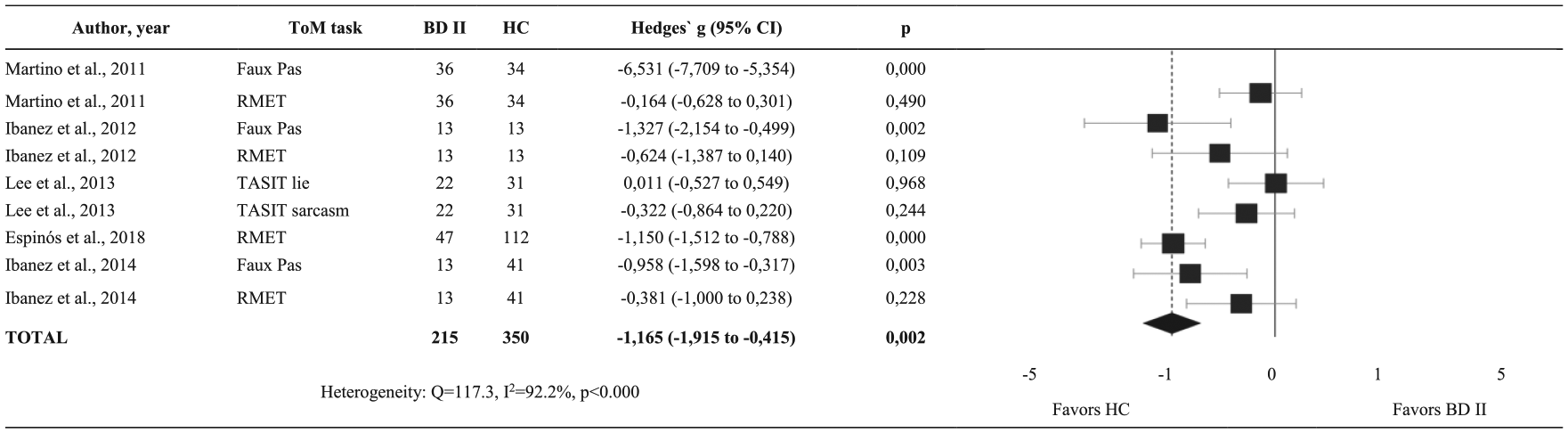
Summary of results and forest plots of meta-analyses comparing Theory of Mind (ToM) between individuals with type II bipolar disorders (BD II) and healthy controls (HC).
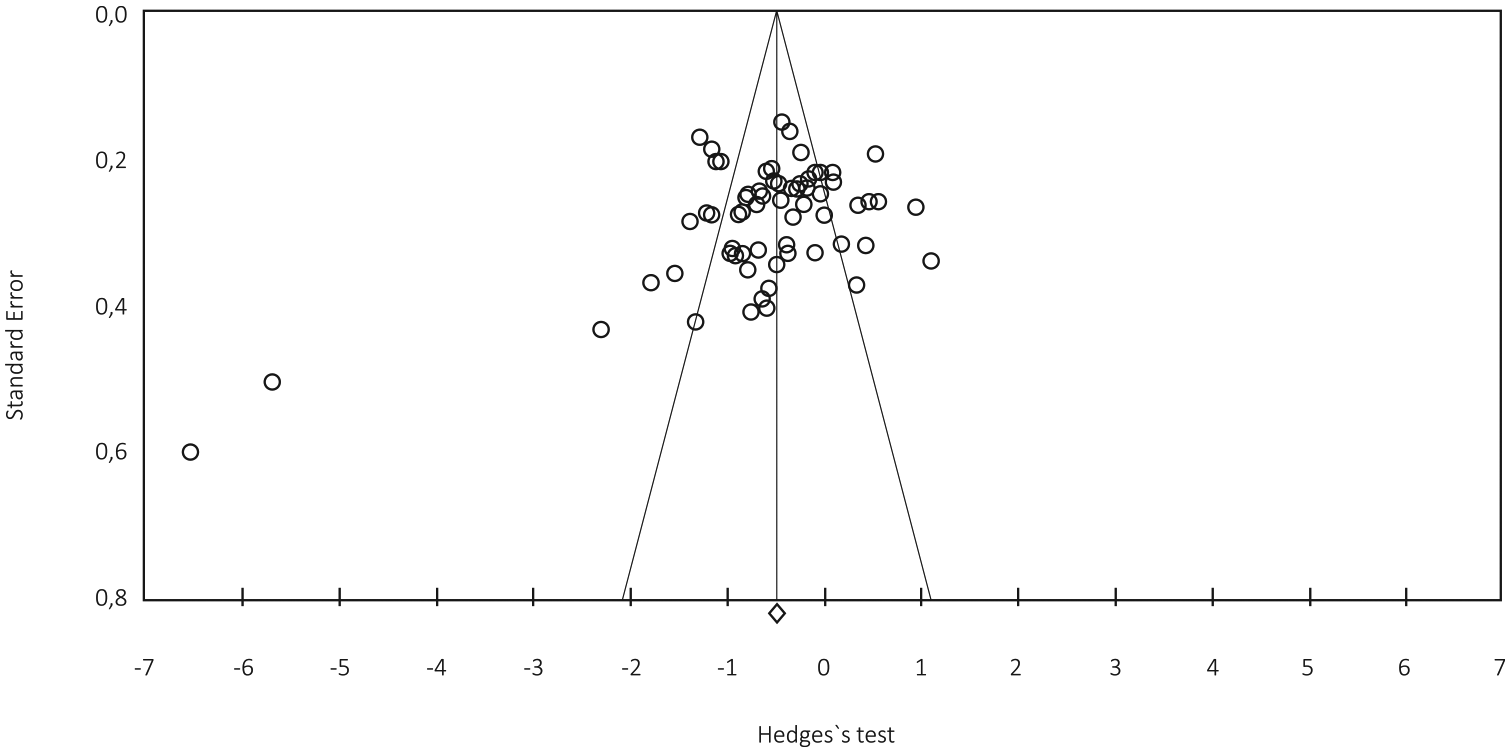
Funnel plot.
Results
Characteristics of the studies
A total of 30 studies were included (27 full paper and 3 theses) in this meta-analysis. The sample was heterogeneous regarding BD type, 12 studies included only BD I patients, 2 studies included only BD II patients (Ibanez et al., 2012, 2014), 12 studies included both types (BD I and II) and 4 studies did not mention type of BD in their sample (Dalkner et al., 2019; Goitia et al., 2017; Kerr et al., 2003; Wang et al., 2017). For more information, see Table 1.
ToM in BD compared to controls
Patients with BD presented a significant impairment in ToM performance when compared to controls (Hedge’s g = −0.589, 95% CI: −0.764 to −0.414, Z = −6.594, p < 0.001). The distribution of effect sizes was heterogeneous (I2 = 87.36%, p < 0.001). The variance of the true effects on the same scale as the effects was τ2 = 0.453. No publication bias was detected (Egger’s test = 0.015).
ToM in BD I and BD II compared to controls
When compared to controls, ToM was impaired in patients with both BD I (Hedge’s g =−0.663, 95% CI: −0.954 to −0.372, Z = −4.462, p < 0.001) and BD II (Hedge’s g =−1.165, 95% CI: −1.915 to −0.415, Z = −3.044, p = 0.002, τ2 = 1.198). In this case, these results may suggest that individuals with BD II were slightly more compromised than BD I when compared to controls. However, no direct comparison of BD I vs BD II was carried out.
Individual task analyses
RMET
A total of 13 studies used RMET to assess ToM. Patients with BD showed a significant impairment in RMET task (Hedge’s g = −0.555, 95% CI: −0.749 to −0.361, Z = −5.608, p < 0.001). When compared to controls, these results suggest that patients with BD I showed a greater impairment (Hedge’s g = −0.850, 95% CI: −1.188 to −0.512, Z = −4.932, p < 0.001) than individuals with BD II (Hedge’s g = −0.598, 95% CI: −1.126 to −0.069, Z = −2.216 p = 0.027).
Faux Pas Task
A total of six studies used Faux Pas to assess ToM. Faux Pas scores were significantly impaired in BD patients when compared to controls (Hedge’s g = −1.452, 95% CI: −2.524 to −0.381, Z = −2.657, p = 0.008). In this task, patients with BD II present a greater impairment when compared to controls (Hedge’s g =−2.899, 95% CI: −5.804 to 0.006, Z = −1.956, p = 0.051) than individuals with BD I (Hedge’s g =−1.048, 95% CI: −3.098 to 1.002, Z = −1.002, p = 0.316).
The Hinting Task
A total of four studies used the Hinting Task to assess ToM. In individual task analyses, Hinting Task scores were significantly impaired in BD patients (Hedge’s g = −0.575, 95% CI: −0.810 to −0.341, Z = −4.806, p < 0.001). It was not possible to compare BD I and BD II with controls, given that only BD I patients performed the Hinting Task in the analyzed studies.
ToM visual vs ToM verbal
ToM impairments were found in BD patients, compared to controls, on verbal (Hedge’s g = −1.077, 95% CI: −1.610 to −0.544, Z = −3.961 p < 0.001) and visual (Hedge’s g =−0.614, 95% CI: −0.844 to −0.384, Z = −5.231, p < 0.001) tasks, suggesting a more significant impairment in verbal tasks.
In verbal tasks, BD I patients showed significant differences in ToM when compared to controls (Hedge’s g = −0.794, 95% CI: −1.450 to −0.137, Z = −2.369, p = 0.018), while BD II patients showed non-significant differences when compared to controls (Hedge’s g =−2.899, 95% CI: −5.804 to 0.006, Z = −1.956, p = 0.051). In visual tasks, BD I patients showed significant differences in ToM when compared to controls (Hedge’s g = −1.034, 95% CI: −1.386 to −0.682, Z = −5.763 p < 0.001), as well as BD II patients showed a significant difference in ToM when compared to controls (Hedge’s g = −0.598, 95% CI: −1.126 to −0.069, Z = −2.216, p = 0.027). Although both BD types showed a significant difference, BD I results suggest a poorer performance when compared to controls.
Meta-regression
There was no significant effect of gender (Z = 0.16, p = 0.87), age (Z = 0.59, p = 0.55), education (Z = −0.3, p = 0.74), illness duration (Z = 0.76, p = 0.44) and age of onset of illness (Z = −1.3, p = 0.19) in the results of ToM in BD patients.
Discussion
To our knowledge, this is the first meta-analysis to investigate ToM performance in a well-characterized euthymic sample of BD patients, in comparison with healthy controls. We found a relationship between BD and deficits in ToM performance, indicating impaired ToM in BD patients even during remission periods. The effect size of ToM (g = 0.58) deficit in euthymic patients suggests a medium effect size impairment and is comparable with the previous meta-analysis’ effect size (d = 0.50) of a subset for euthymic patients (Bora et al., 2016). Recent studies indicate that ToM performance was also found to be impaired in relatives of BD patients, indicating that ToM may be a potential endophenotypic marker of BD (Berecz and Tényi, 2016; Bora and Özerdem, 2017). It is possible to hypothesize, regarding our findings, that ToM deficits might be trait markers of BD; however, further longitudinal studies in this area are needed in order to test this hypothesis. This is necessary since in order to be considered endophenotypes, markers should be more frequent in unaffected relatives of patients compared to the general population, and therefore, heritable (Samamé, 2013).
Although we did not directly compare results obtained from BD I vs BD II, our findings may suggest a slightly more compromised ToM impairment in BD II (g = 1.16) when compared to BD I (g = 0.66). However, of the 14 studies that included BD II patients, only 6 offered task results, indicating that BD II is a less commonly studied subtype, making it more difficult to compared to BD I. Taking this into account, our results must be cautiously interpreted, given the small sample of BD II patients included in this meta-analysis.
In agreement with the prior meta-analysis, conducted by Bora and colleagues (2016), we found a significant worse performance in verbal tasks in comparison with visual tasks in euthymic BD patients, such as the Faux Pas and the Hinting Task. Verbal tasks demand an accurate interpretation of the semantic meaning of a social situation, as well as a correct knowledge of social cues and executive functioning. Therefore, our results indicate that ToM tasks that demand verbal function are more impaired in euthymic BD patients. This is in accordance with previous findings that indicated ToM deficits in Verbal ToM tasks, but not in Visual ToM Tasks (Haag et al., 2016; Olley et al., 2005).
ToM must not be viewed as a homogeneous construct, but a set of various inter-dependent processes that may be distinctly affected in BD patients. Affective and Cognitive aspects of ToM are evaluated in tasks and are behaviorally distinct and supported by diverse networks, as shown in imaging studies and psychophysiological findings in HC subjects (Abu-Akel and Shamay-Tsoory, 2011; Amodio and Frith, 2006); thus, ToM cannot be referred as an all-or-nothing capacity, but as a spectrum of degrees (Abu-Akel and Shamay-Tsoory, 2011). RMET and Faux Pas are considered as a ToM Affective Task and a ToM Cognitive Task, respectively, being different in the complexity of ToM processing. Unlike a previous meta-analysis (Bora et al., 2016), we found in our individual task analyses a more significant impairment in RMET in BD I (g =−0.85) than to BD II (g = −0.59), although it must be empathized that we did not compare directly results obtained from BD I vs BD II. The RMET (Baron-Cohen et al., 2001) is one of the most used ToM tasks to assess the capacity to evaluate others mental states by watching the ocular region of faces. The task involves describing the emotional/mental state of a person based only on an image of their eyes, in a fixed-choice paradigm. Even though automatic processes are important in the RMET task, it also requires a perception of complex visual materials like faces and basic emotion recognition (RMET; Baron-Cohen et al., 2001). Therefore, other functions, like basic emotion recognition, may be partially responsible for the ToM impairments found in euthymic sample. Hence, RMET requires a more implicit social-perceptual process (Peterson and Miller, 2012). A recent study has shown to overlap between impaired verbal memory function and poor RMET performance, especially in male BD patients (Dalkner et al., 2019). Certain emotional deficiencies in affective ToM in euthymic BD patients have been described in other studies (Espinós et al., 2018; Marotta et al., 2018; Martino et al., 2011; Wolf et al., 2010). These findings are in contrast with previous studies that stated that BD patients only showed Cognitive ToM deficits (Montag et al., 2010; Shamay-Tsoory et al., 2009). It is important to mention that, in some studies, some tasks may not have been challenging for the euthymic BD sample, given that the eye stimuli used had only one distractor (Shamay-Tsoory et al., 2009), whereas others had three distractors (Baron-Cohen et al., 2001). These divergent results may depend on the samples’ characteristics. Nonetheless, the results of the current meta-analysis indicate that euthymic BD patients do not adequately identify the emotional states of other people, which might lead to impairments in the relationships with others and a deficient comprehension of other people’s emotional intentions.
Alternatively, regarding the Faux Pas Task, our findings may suggest that euthymic BD II patients (g = 2.89) present a more expressive dysfunction when compared to euthymic BD I patients (g = 1.04). The name of the task can be roughly translated as ‘False Step’, and it assesses the subject’s ability to perceive when a social indiscretion occurs. According to Torrent et al. (2006), executive dysfunctions are likely to constitute good predictors of social and occupational difficulties in patients with BD II, whereas problems in retaining and recovering information may be more relevant in BD I. The differences in ToM performances might be influenced by these predictors, given that the RMET task requires attentional functions and the Faux Pas Task constitutes a more elaborate deduction of perspectives, rendering to executive functions. Considering the findings in this current meta-analysis, we can speculate that BD I euthymic patients present a poor functioning in implicit social-perceptual processes, an automatic decoding ability (Samamé, 2013), whereas euthymic BD II patients appear to have a more expressive deficit in the reasoning about emotional mental states.
A second explanation for the differences found in distinct tasks of ToM may be related to ToM reasoning vs decoding. While ToM reasoning requires a higher demand of general cognitive domains, such as executive function and working memory, ToM decoding is similar to the perception of mental states cues (Mitchell and Young, 2016). RMET is a measure of decoding emotional states based on perceptual visual information and Faux Pas, in contrast, is a more complex task that requires the patient to reason whether the other person said something appropriate. Thus, the findings in this current study may indicate that BD I euthymic patients have task-related impairments in decoding ToM, whereas BD II euthymic patients present more complex delays in ToM reasoning.
Finally, studies investigating social cognition training (SCT) show a potential for improving ToM function. Kurtz and Richardson (2011) conducted a meta-analytic investigation of controlled researches in SCT for schizophrenia, finding positive effects of social-cognitive training programs on ToM performance in all seven studies. This finding, although only focused in schizophrenia, is significant in demonstrating that advanced ToM functions can be reversed through structured training programs. According to the meta-analysis, patients with a longer history of living with the illness are better equipped to partake in SCT (Kurtz and Richardson, 2011). In another study, conducted by Santiesteban and colleagues (2012), ToM function was improved using imitation–inhibition training in healthy adults. This finding suggests that training in general inhibitory control enhances self-other distinction, which in turn helps to ameliorate egocentric bias in perspective training (Santiesteban et al., 2012). A recent study (Lahera et al., 2013) implemented a social cognition and interaction training (SCIT) for outpatients with BD, finding a small increase in ToM Task performance. More studies are needed in order to provide preliminary evidence of successful ToM rehabilitation programs for bipolar populations, since it is extremely important to identify methods that can effectively remediate impaired ToM, as well as provide early interventions to improve ToM.
SC and, thus, ToM, have a significant number of complex and hierarchical subdomains, as well as different kinds of stimuli, that make the task of comparing results between studies very difficult. Due to the heterogeneity of ToM tasks, we recommend that future studies use standardized tasks, in order to maintain homogeneity and better assess this domain. In addition, it has been discussed that certain ToM tasks, such as First- and Second-Order False Belief Stories, may not be sensitive enough to analyze subtle ToM impairments in adults (Bora et al., 2005). More advanced tasks are required in order to detect more subtle ToM constructs such as irony, white lies, sarcasm and jokes. Furthermore, tasks should adopt more ecological ToM tasks such as video-based material in more naturalistic settings. Some studies have used novel tasks aimed at assessing more specific ToM deficits (Feyerabend et al., 2018; Montag et al., 2010). It is necessary to adapt assessments making them more applicable and specific for BD patients, given that the impairments in BD tend to be more subtle when compared to other populations, such as schizophrenia (Lee et al., 2013; Wang et al., 2017). Finally, further studies should include, in parallel to ToM tasks, a comprehensive neuropsychological battery, making it possible to investigate the relation between cognitive function and ToM performance.
An important limitation to be considered with regard to some studies included in this meta-analysis is the use of antipsychotics not controlled for in these studies. This might have an important influence in the results due to the differential use of medication within samples. Similarly, another limitation is the wide variety of different measures used to measure ToM and Cognitive domains, each with its own limitations indicating a need for clear consensus in what tasks to use. Furthermore, an important limitation that needs to be considered is that comorbid conditions have not been discussed to much extent in many of the studies included in this review. Similarly, to previous analyses (Bora et al., 2016; Samamé et al., 2012), our attempt to link demographic and clinical information with ToM failed. At present, no significant associations were found between ToM and age, gender, illness onset, illness duration and education. Wolf, Brüne and Assion (2010), however, established a positive finding between performance of ToM and illness duration. More research between these variables is required in other to determine whether ToM is progressive, as this study. An important limitation to be considered with regard to this meta-analysis is that we were not able to assess the possible effect of cognitive subdomains on the observed ToM effect sizes due to the lack of enough studies that included a complete and similar neurocognitive assessment. Bora et al. (2016), in their meta-analysis, present findings that suggest that neurocognitive deficits may importantly contribute to ToM deficits. A recent study found a significant relationship between the ToM task RMET and verbal memory in BD euthymic patients (Dalkner et al., 2019). For both therapeutic and academic purposes, it is crucial to establish whether ToM impairment in euthymic BD is primary in origin or simply secondary to a more general cognitive impairment (Mitchell and Young, 2016). Future studies should focus on longitudinal and cross-sectional data to examine cause and effect on specific cognitive domains and their relationship with ToM. Although we followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, one limitation of this study was the non-registration of the PROSPERO protocol, as suggested by the National Institute for Health Research (NIHR). Moreover, another limitation is the small number of studies that included BD II patients; of the 14 studies that included BD II patients, only 6 offered task results.
Finally, the studies that included euthymic BD patients were heterogeneous in their definitions of euthymia and the choice of scales for such measure. Some studies required participants to present a score below 6–8 for the Young Mania Rating Scale (YMRS) and 6–8 for the Hamilton Depression Rating Scale (HDRS), whereas others used other scales such as CARS-M, PANSS, HDRS and Beck Depression Inventory–II (BDI-II). Future studies in this topic should use the same scale for determining the patient’s mood status and be able to have a more homogeneous group of euthymic patients.
Conclusion
This study suggests that euthymic patients with BD have impairment in ToM function, presenting a more significant deficit in verbal ToM. With regard to ToM ability in BD patients, impairment has been broadly observed during acute phases of the illness (Bazin et al., 2009; Kerr et al., 2003), while evidence of the presence of deficits in remission samples has been less conclusive. Sociocognitive impairment in euthymic states is of great interest in the field, since such deficits may be a defining interference for social reintegration and rehabilitation (Mitchell and Young, 2016). Given the importance and impact of ToM performance on quality of life, social perception and social behavior, further investigations into the psychological and neurobiological mechanisms of these impairments are essential in order to establish specific targets for the development of personalized SC training for this population.
Research Data
Excel_Data_Research for Impaired social cognition in bipolar disorder: A meta-analysis of Theory of Mind in euthymic patients
Excel_Data_Research for Impaired social cognition in bipolar disorder: A meta-analysis of Theory of Mind in euthymic patients by Luisa de Siqueira Rotenberg, Gabriel Henrique Beraldi, Gabriel Okawa Belizario and Beny Lafer in Australian & New Zealand Journal of Psychiatry
Research Data
Final_Results_Excel for Impaired social cognition in bipolar disorder: A meta-analysis of Theory of Mind in euthymic patients
Final_Results_Excel for Impaired social cognition in bipolar disorder: A meta-analysis of Theory of Mind in euthymic patients by Luisa de Siqueira Rotenberg, Gabriel Henrique Beraldi, Gabriel Okawa Belizario and Beny Lafer in Australian & New Zealand Journal of Psychiatry
Footnotes
Author Contributions
L.d.S.R. participated in the conception and design of the study, reviewed studies, extracted data, performed the analysis and wrote the manuscript. G.H.B. participated in the design of the study, reviewed studies, performed the analysis and reviewed the manuscript. G.O.B. reviewed studies, extracted data and reviewed manuscript. B.L. supervised the study design, data collection and analysis and reviewed the manuscript. All authors revised the article critically and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was partly supported by a generous private donation from Suzana and Carlos Melzer to the USP Bipolar Disorder Research Program (PROMAN).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.