
Abstract
Objective:
To investigate the effectiveness of stimulants in patients with depression, by using naturalistic outcome measures, such as psychiatric admissions, psychiatric bed-days and incidents of intentional self-harm or suicide attempts.
Methods:
Via linkage of the Danish nationwide health registers, we identified all patients with a diagnosis of depression initiating stimulants, including methylphenidate, modafinil, amphetamine, dexamphetamine or lisdexamphetamine, from 1995 to 2012. We used a mirror-image model to test whether redemption of a stimulant prescription was associated with a reduction in psychiatric admissions, inpatient days and incidents of intentional self-harm or suicide attempts. Specifically, the number of these outcomes in the 2 years leading up to redemption of a stimulant prescription was compared to the two subsequent years. Similar outcomes were used in a reverse mirror-image model to investigate the effect of stimulant termination.
Results:
A total of 3354, 935 and 105 patients diagnosed with depression redeemed prescriptions for methylphenidate, modafinil or amphetamine/dexamphetamine/lisdexamphetamine, respectively. Initiation of methylphenidate was not associated with a significant change in psychiatric admissions (mean: −0.02 admissions, p = 0.11) or inpatient days (mean: 0.13 days, p = 0.74). Similar findings were made for modafinil and the amphetamines. In addition, no clinically relevant change in psychiatric admissions or inpatient days was found after termination of a stimulant. After initiation of methylphenidate, the incidents of self-harm or suicide attempts were reduced by 54%, from 68 to 31 events (p = 0.004). No significant change in incidents of self-harm or suicide attempts were found for modafinil or the amphetamines.
Conclusion:
This nationwide study, using naturalistic outcomes, does not support the use of stimulants in patients with depression. However, the use of methylphenidate was associated with a 54% reduction in incidents of self-harm or suicide attempts, indicating that methylphenidate may potentially be useful in patients with depression with suicidal- or self-harming behaviour. However, further studies are needed, before any firm conclusions can be made.
Introduction
Depression is a common, recurring and debilitating mental illness that often requires treatment (Otte et al., 2016). However, despite treatment with relevant antidepressants in adequate dosages, adjunctive psychotherapy and/or pharmacotherapy, remission rates for patients suffering from depression are quite modest, with 20–30% having treatment-resistant depression, emphasizing the need for alternative treatment strategies (Kohler-Forsberg et al., 2019; McIntyre et al., 2014; Nierenberg, 2013; Trevino et al., 2014; Trivedi et al., 2006).
Patients with attention-deficit hyperactivity disorder (ADHD) have an increased risk of developing depression and especially patients with severe or treatment-resistant depression have a high degree of ADHD-related symptoms compared to patients with remitted depression. This indicates that in patients with depression that fail to achieve remission on conventional pharmacotherapy, stimulants might be a therapeutic option (Bron et al., 2016; McIntyre et al., 2017; Meinzer et al., 2013).
Recently, studies have suggested that treatment with central nervous system stimulants, such as amphetamine, methylphenidate and modafinil, has antidepressant effect in patients with depression (Corp et al., 2014). Of particular interest, some randomized controlled trial (RCT) studies suggest that adding modafinil to established antidepressant treatment might improve overall depression rates and remission rates by reducing symptoms of fatigue/weariness (Abbasowa et al., 2013; Goss et al., 2013). Other studies have shown that augmentation with methylphenidate may reduce depressive symptoms in patients suffering from major depression, geriatric depression or terminal cancer (Kerr et al., 2012; Lavretsky et al., 2015; Ng et al., 2014). Finally, lisdexamphetamine has also shown promise in the treatment of depression (Trivedi et al., 2013). While promising, the studies investigating the effect of stimulants on depression have generally had short follow-up time and there are also RCT studies that do not support the use of stimulants in the treatment of depression (Malhi et al., 2016). Furthermore, the effect of stimulants has been suggested to be short-lived in patients with depression (Malhi et al., 2016).
Taken together, there is a need of studies evaluating the long-term and real-world effectiveness of this class of pharmaceuticals in the treatment of depression. Therefore, we aimed to evaluate the effectiveness of stimulants in patients with a diagnosis of depression, in a register study using naturalistic outcome measures, namely psychiatric admissions, psychiatric bed-days and incidents of intentional self-harm or suicide attempts.
Materials and methods
This study was based on linkage of data from the national Danish registers, which have been used for psychiatric research for decades (Munk-Jorgensen and Ostergaard, 2011).
Registers
The Danish Civil Registration System (DCRS) (Pedersen, 2011) contains information on all individuals with legal residence in Denmark from 1969 onwards. The DCRS includes information about date of birth, birthplace, vital status and so on, as well as a unique 10-digit personal identifier, which enables linkage of information – at the level of the individual – across all national Danish registers. The Danish Psychiatric Central Research Register (DPCRR) (Mors et al., 2011) contains information on all contacts to Danish psychiatric hospitals, including admissions, inpatient time and psychiatric diagnoses. From 1995, it was expanded to include the same information from outpatient contacts and emergency room visits as well. The Danish National Prescription Register (DNPreR) (Kildemoes et al., 2011) contains information on all redemptions of prescribed medicine since 1995. The Danish National Patient Register (DNPatR) contains information on every contact to the non-psychiatric hospital system in Denmark since 1977 (Lynge et al., 2011).
Study population
We used the DCRS, DPCRR and DNPreR to identify all Danish residents who received a diagnosis of depression (ICD-10 codes: F32, F33) in relation to inpatient, outpatient or emergency room assessment/treatment at a Danish psychiatric hospital in the period from 1 January 1995 to 1 September 2012, and who redeemed a prescription for a stimulant (methylphenidate, modafinil, amphetamine, dexamphetamine or lisdexamphetamine; Anatomical Therapeutic Chemical [ATC] codes: N06BA04, N06BA07, N06BA01, N06BA02, N06BA12). Subsequently, we used the DPCRR to identify individuals, who also received diagnoses of ADHD (ICD-10 code: F90). These patients were excluded, thus leaving a cohort of patients diagnosed with depression – without comorbid ADHD – receiving stimulants. In sensitivity analyses, we included the patients with ADHD and comorbid depression that were excluded from the main population.
Exposure and outcome
Exposure was defined as the first redemption of a prescription for a stimulant. Outcomes included psychiatric admissions, psychiatric bed-days and intentional self-harm or suicide attempts (ICD-10 codes: X60-84) identified through the DPCRR and DNPatR.
Statistical analyses
First, a traditional 2-year mirror-image model (Gault et al., 2016; Rohde et al., 2018a, 2018b) was used to assess whether psychiatric admissions and psychiatric bed-days changed after initiating treatment with a stimulant. This was done by comparing the post-mirror period, defined as the period spanning from the first redemption of a stimulant prescription and 2 years forward, to the pre-mirror period, defined as the 2 years prior to the first redemption of a stimulant prescription. If the patients died or stopped redeeming prescriptions for the stimulant, the post-mirror period was stopped at the date of death or 1 month after the last redemption, respectively – and the pre-mirror period was shortened equally, such that the pre-mirror and post-mirror periods had the exact same duration. If a patient did not receive a stimulant prescription within the period from 3 months before to 3 months after the end-date, the patients were considered to have stopped redeeming prescriptions for the stimulant at some point in the post-mirror period before the end-date. We then defined a new end-date, which was the date 1 month after the last redemption of a stimulant prescription in the post-mirror period (Figure 1).
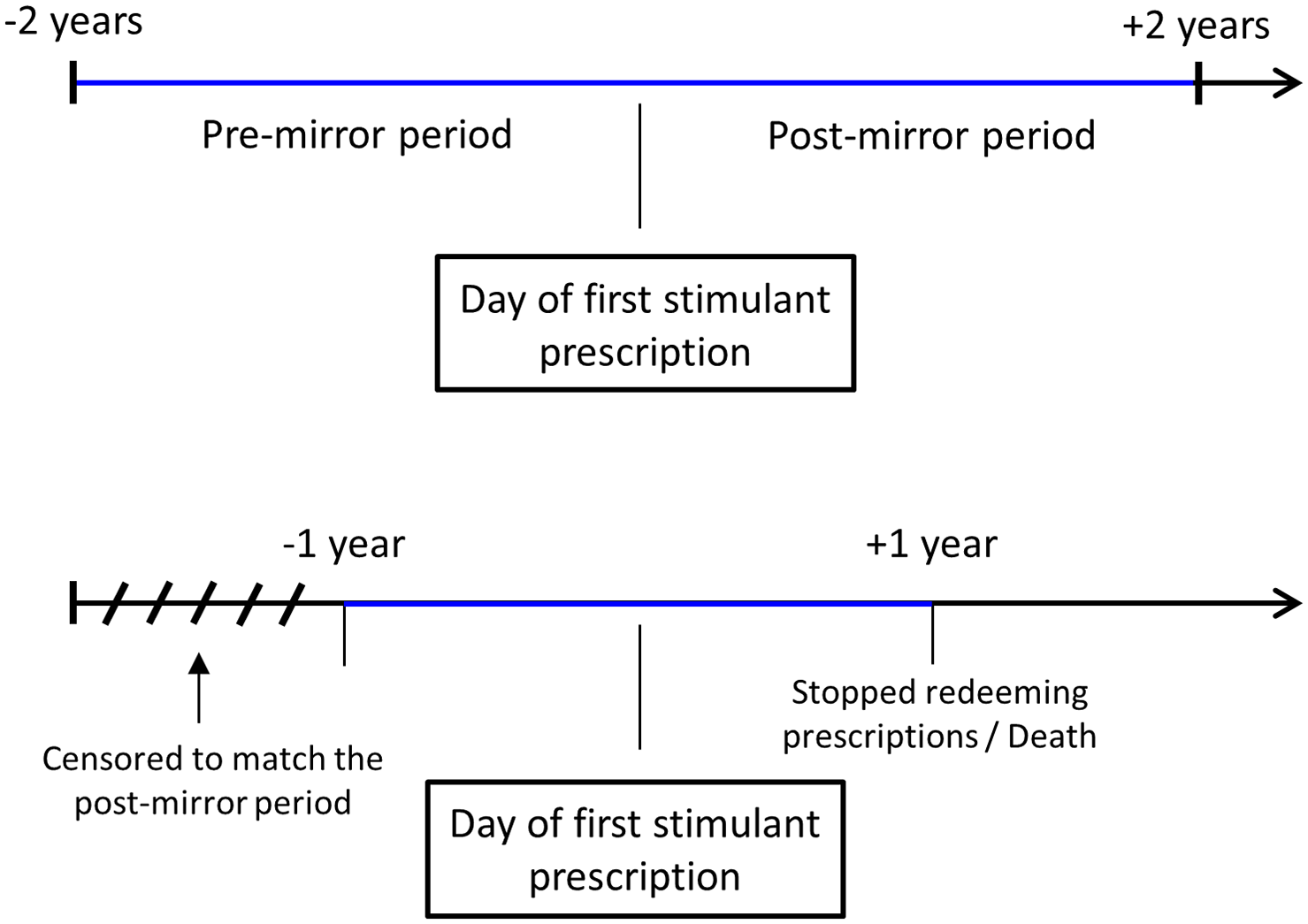
Illustration of the mirror-image design.
After having defined the mirror periods, the number of admissions, psychiatric bed-days and incidents of self-harm or suicide attempts were compared between the mirror periods using a paired t-test (assumptions for the paired t-tests were checked with Bland-Altman and QQ plots). If the first prescription of a stimulant occurred within 7 days after discharge from a psychiatric admission, this admission was excluded in the pre-mirror period, as it was likely that the stimulant was started during the admission (and the DNPreR does not contain data on drugs dispensed during admissions).
Subsequently, a reverse mirror-image model was used to assess whether psychiatric admissions, psychiatric bed-days and incidents of self-harm or suicide attempts changed after the patients stopped redeeming stimulant prescriptions. The post-mirror period was defined as from 1 month after the last prescription and 2 years forward. The pre-mirror period was mirrored around this 1 month after the last prescription date. The periods were again shortened equally if the patient died in the post-mirror period or if the patients had not received a stimulant for the full 2-year pre-mirror period.
In sensitivity analyses, patients were stratified on the severity of depression: mild (ICD-10 codes: F32.0, F33.0), moderate (ICD-10 codes: F32.1, F33.1) and severe depression (ICD-10 codes: F32.2, F32.3, F33.2, F33.3) and on concomitant treatment with antidepressants (selective serotonin reuptake inhibitors [SSRIs], serotonin and noradrenaline reuptake inhibitors [SNRIs] and tricyclic antidepressants [TCAs]), respectively.
As the mean number of psychiatric admissions and psychiatric bed-days has decreased in Denmark during the last years due to fewer psychiatric beds (Bauer et al., 2012), a linear regression for the overall decrease in psychiatric admissions and psychiatric bed-days for patients with depression was carried out, and all estimates in the analyses were adjusted for this estimate. Overall, the mean reduction in psychiatric admissions was 0.02 admission per year, and this was multiplied by the mean follow-up time in the post-mirror period and added to the mean number of psychiatric admissions in the post-mirror period. Similarly, this was done with psychiatric bed-days, where the overall mean reduction was 0.90 bed-days per year. For the sensitivity analyses, linear regressions for mild, moderate and severe depression were made, and the analyses were adjusted for these estimates.
Results
Cohort
We identified 7964 patients with depression receiving stimulants. After exclusion of patients with comorbid ADHD, 4394 patients with depression receiving stimulants remained and defined the main population (Figure 2).
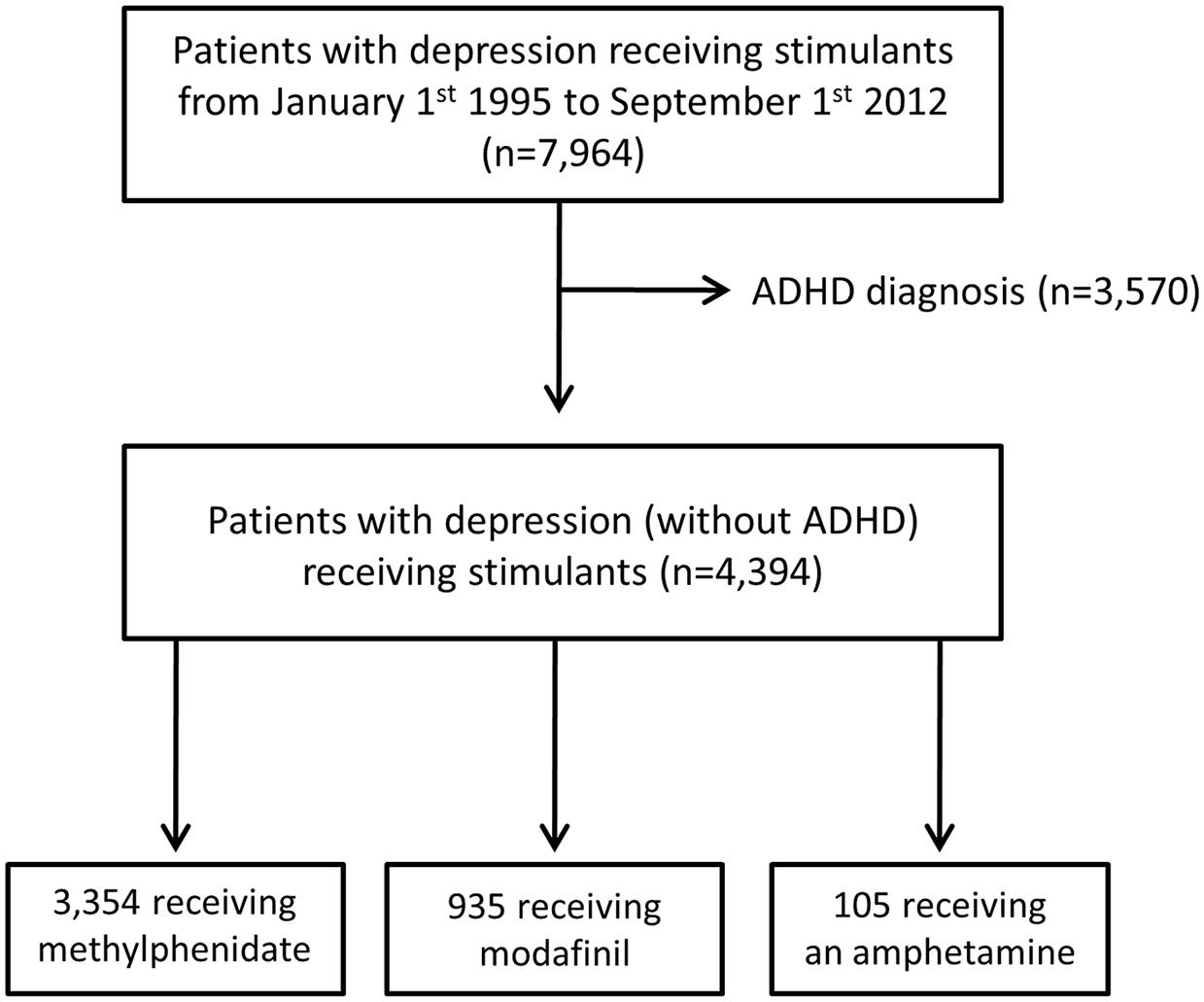
Flowchart illustrating the design of the study.
Methylphenidate and depression outcomes
A total of 3354 patients diagnosed with depression received methylphenidate. The mean age at first redemption of a methylphenidate prescription was 36.3 years (43.6% were men). The mean follow-up time was 429 days and 40.3% continued methylphenidate after the 2-year follow-up period (Table 1).
Patient characteristics.
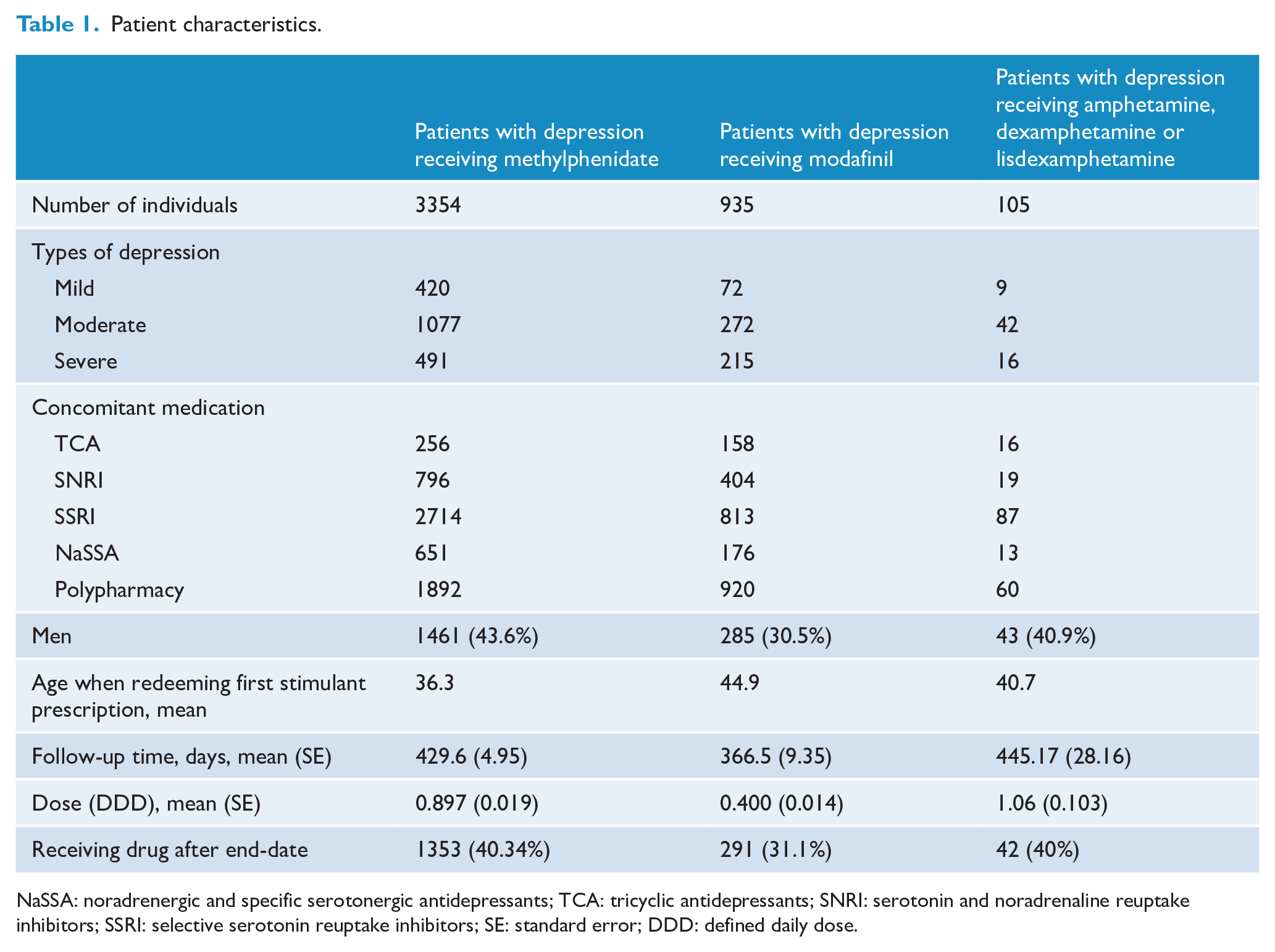
NaSSA: noradrenergic and specific serotonergic antidepressants; TCA: tricyclic antidepressants; SNRI: serotonin and noradrenaline reuptake inhibitors; SSRI: selective serotonin reuptake inhibitors; SE: standard error; DDD: defined daily dose.
After initiation of methylphenidate, the number of psychiatric admissions did not change for this group (mean: −0.02 admissions, p = 0.11). However, those suffering from moderate or severe depression had a significant reduction with 0.09 (p < 0.001) and 0.18 (p < 0.001) admissions, respectively. In addition, only patients treated with TCA had a significant reduction in psychiatric admission (−0.10 admissions, p = 0.014), whereas patients treated with SSRI or SNRI did not experience such a decrease. Similar findings were made regarding psychiatric bed-days, although a significant reduction was only found within the group of severely depressed patients (4.13 bed-days, p = 0.009) (Table 2). In addition, we found a significant reduction (p = 0.004) in attempts of suicide or self-harm after initiation of methylphenidate with 68 events in the pre-mirror period compared to 31 events in the post-mirror period for all patients with depression (Table 2). As a post hoc analysis, we stratified the analysis of suicide attempts/intentional self-harm on age and found that there was a significant change in this outcome for individuals aged ⩽30 (45 events in the pre-mirror period compared to 12 events in the post-mirror period; p < 0.01), but no significant change for individuals above the age of 30 (23 events in the pre-mirror period compared to 19 events in the post-mirror period; p = 0.61).
Mirror-image model comparing psychiatric admissions, inpatient days and self-harm or suicide attempts before and after initiation of treatment with stimulants.
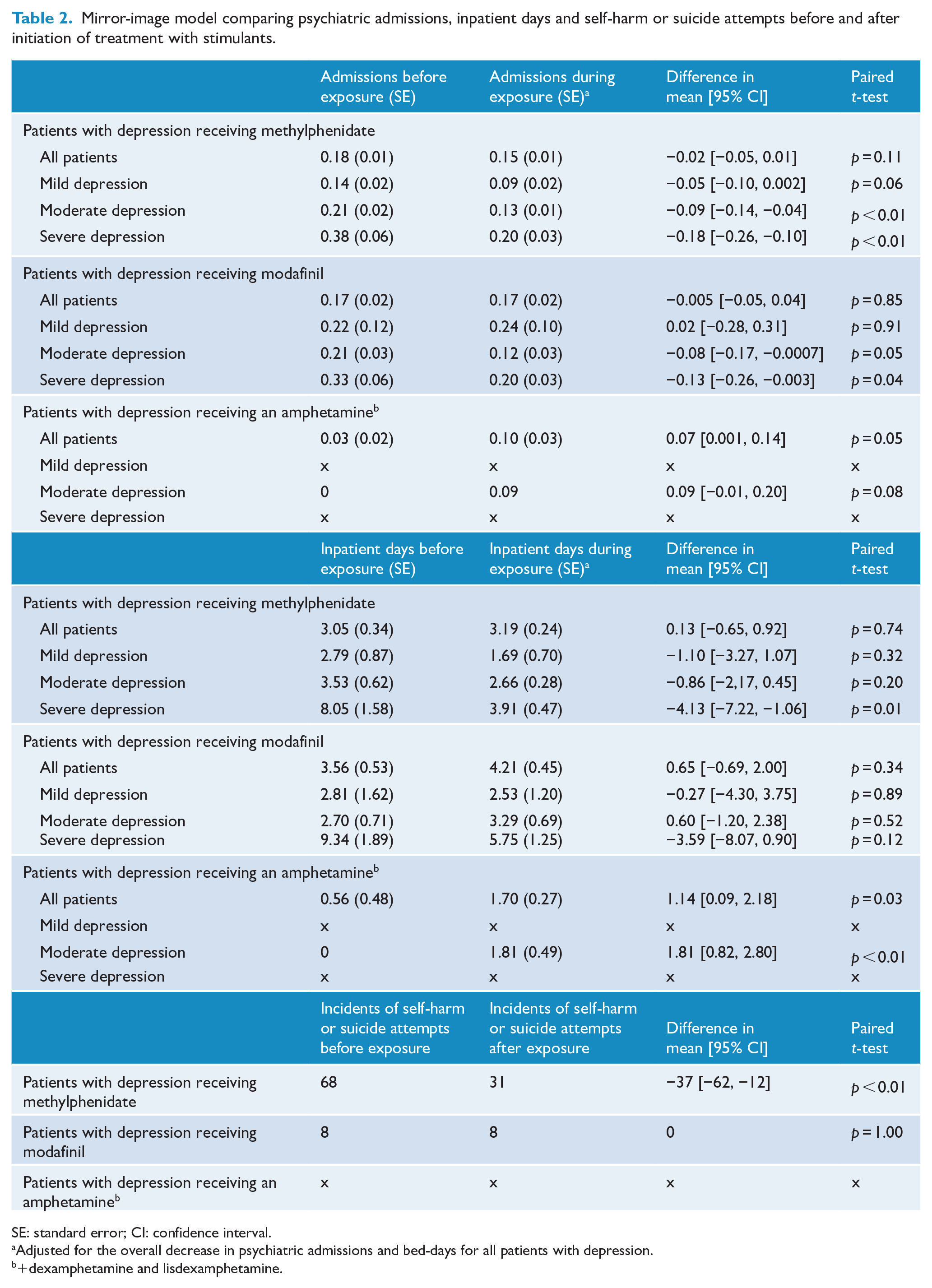
SE: standard error; CI: confidence interval.
Adjusted for the overall decrease in psychiatric admissions and bed-days for all patients with depression.
+dexamphetamine and lisdexamphetamine.
In the reverse mirror-image model, the number of psychiatric admissions or psychiatric bed-days did not change significantly after termination of methylphenidate (Table 3). There were 9 events of suicide attempt or self-harm in the pre-mirror period compared to 13 events after termination of methylphenidate in the post-mirror period (p = 0.66).
Reverse mirror-image model comparing psychiatric admissions and bed-days before and after termination of stimulant treatment.
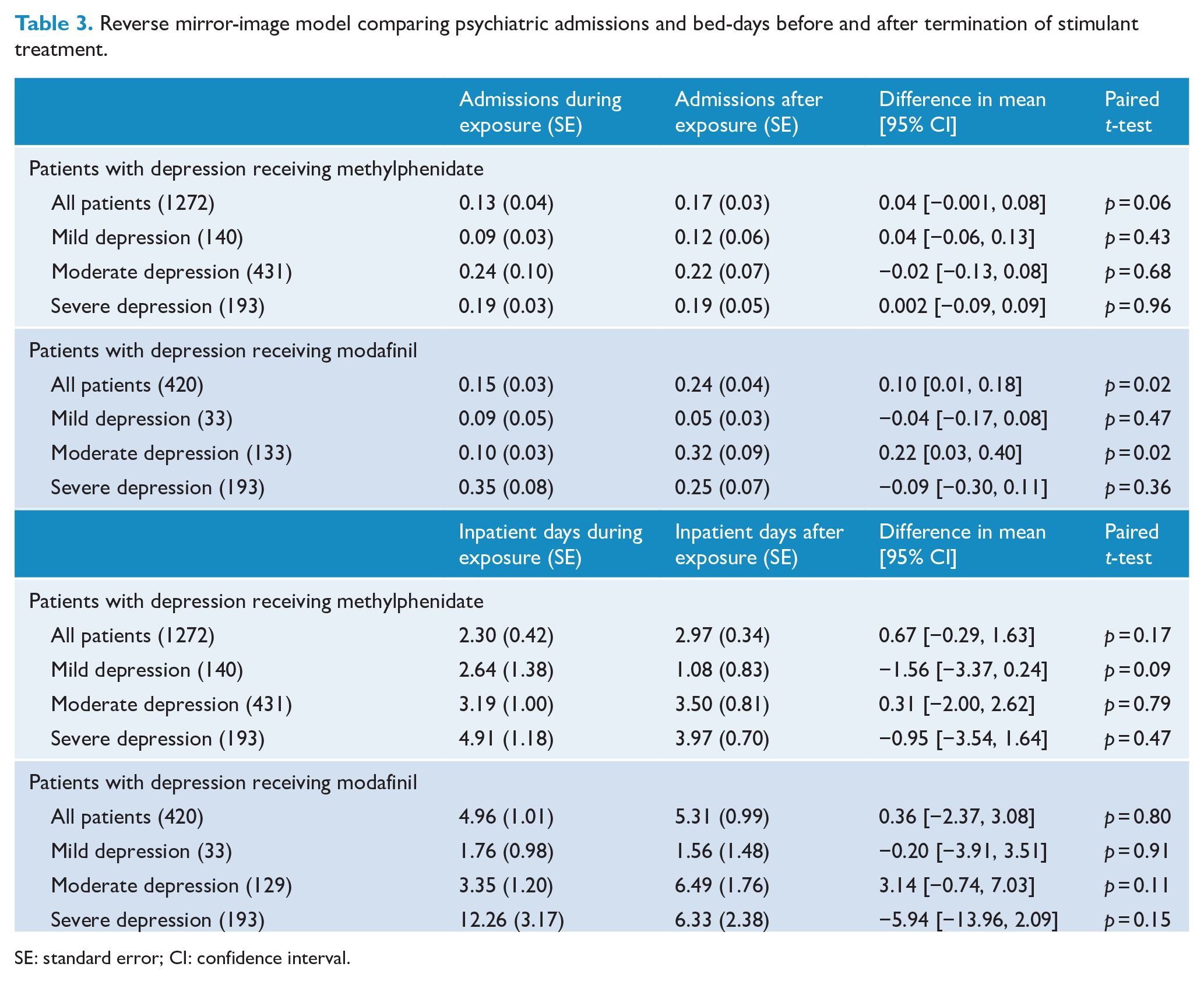
SE: standard error; CI: confidence interval.
Modafinil
A total of 935 patients with depression received modafinil. The mean age at first redemption of a modafinil prescription was 44.9 years (30.5% were men). Mean follow-up time was 366.5 days and 31.1% continued modafinil after the 2-year follow-up period (Table 1).
In the mirror-image model, the number of psychiatric admission or psychiatric bed-days did not change significantly after initiation of modafinil. However, a significant reduction in psychiatric admissions was found for patients diagnosed with moderate or severe depression, with a reduction on 0.08 (p = 0.048) and 0.13 (p = 0.044) admissions, respectively (Table 2). In addition, there was no change in the number of events of suicide attempt or self-harm, with eight events in the pre-mirror period compared to eight events after initiation of modafinil in the post-mirror period (Table 2).
In the reverse mirror-image model, there was a significant increase in psychiatric admissions with 0.10 (p = 0.02) admissions for the overall cohort and an increase of 0.22 (p = 0.02) admissions for patients with moderate depression. No change in psychiatric bed-days was found (Table 3). Neither did a change in events of suicide or self-harm occur with five events in both the pre-mirror period and after termination of modafinil in the post-mirror period.
Amphetamine, dexamphetamine and lisdexamphetamine
A total of 105 patients with depression received amphetamine, dexamphetamine or lisdexamphetamine. The mean age at first redemption of a stimulant prescription was 40.7 years (40.9% were men). Mean follow-up time was 445 days and 42% received an amphetamine after the 2-year follow-up period (Table 1).
After initiation of an amphetamine, the number of psychiatric admissions increased by 0.07 admission (p = 0.045) and the number of psychiatric bed-days increased with 1.14 bed-days (p = 0.03) (Table 2). There was not enough cases of self-harm or suicide attempts to do analyses.
It was not possible to assess the effect of amphetamine, dexamphetamine or lisdexamphetamine in the reverse mirror-image model due to a small number of outcomes.
Patients with ADHD and comorbid depression
In the sensitivity analyses (patients with ADHD and comorbid depression), we found results equivalent to those from the main analyses, that is, no significant changes in psychiatric admissions or bed-days upon initiation of treatment with stimulants. A significant reduction in attempts of suicide/intentional self-harm was found after initiation of methylphenidate with 163 events in the pre-mirror period compared to 108 events in the post-mirror period (p = 0.007). Modafinil did not change attempts of suicide or intentional self-harm, and there were too few cases receiving amphetamine, dexamphetamine or lisdexamphetamine to study this exposure.
Discussion
In this study, which, to our knowledge, is the first to investigate the real-world effectiveness of stimulants in patients suffering from depression, we did not find any clear evidence supporting the use of stimulants (methylphenidate, modafinil, amphetamine, dexamphetamine and lisdexamphetamine) as a supplement to the existing treatment. Although patients diagnosed with moderate and severe depression experienced a significant reduction in psychiatric admissions and bed-days after initiation of methylphenidate or modafinil, the effect sizes were very modest and unlikely to be clinically relevant, as they were ranging from 0.1 to 0.2 admissions over a 2-year period (approximately). Furthermore, we did not find any substantial changes in the number of psychiatric admissions or bed-days after termination of the stimulants. While there was apparently no clinically relevant effect of stimulants on the number of admissions or bed-days among patients with depression, we did find a 54% reduction in incidents of intentional self-harm or suicide attempts after initiation of methylphenidate, indicating that this particular drug may be a useful treatment in depressed patients with a tendency towards suicidal behaviour/self-harm.
Our findings of no apparent antidepressant effect of stimulants in the treatment of depression based on an observational and naturalistic study with long follow-up time are consistent with the conclusion by the recent paper by Hegerl and Hensch (2017). They looked at recent phase 3 multicentre studies and concluded that they all have failed to support any efficacy of stimulants in patients with depression.
An interesting secondary finding of our study was that incidents of intentional self-harm or suicide attempts were reduced after initiation of methylphenidate. These findings are rather interesting, as a recent study has suggested that stimulants might improve depressive symptoms in patients with low arousal, as seen in atypical depression (characterized by downregulated arousal regulation, hypersomnia and fatigue), and that this subgroup can be identified with an electroencephalography-based algorithm (Hegerl and Hensch, 2017; Schmidt et al., 2017). This particular patient group has also been found to be more likely to have suicidal ideations and to attempt suicide (Blanco et al., 2012; Xin et al., 2019). Therefore, while we could not stratify patients on typical/atypical depression in this study, future studies should ideally aim to determine whether methylphenidate could play a role in reducing self-harm and suicide attempts among patients with atypical depression in particular.
With regard to a potential mechanism, methylphenidate is in ADHD known to reduce emotional dysregulation, thereby increasing the patients’ ability to control and supervise their emotions, leading to less impulsivity (Suzer Gamli and Tahiroglu, 2018). We speculate that methylphenidate might also improve emotional regulation in patients with depression, increasing their ability to respond to negative emotions without succumbing to self-harm. This hypothesis is supported by the finding that the effect of methylphenidate on suicide attempts/intentional self-harm appeared to be restricted to younger individuals (aged ⩽ 30), as these individuals likely experience more difficulties with emotional regulation. Alternatively, the finding could reflect that methylphenidate increases arousal level in atypical depression, resulting in less self-harm. However, further clinical studies (ideally randomized placebo-controlled trials) are needed before any firm conclusions regarding the effect of stimulants (methylphenidate) upon the risk of suicide attempts/intentional self-harm in patients with depression can be made.
It can be argued that our finding of no increase in the incidents of self-harm or suicide attempts after termination of methylphenidate (the reverse-mirror model) points against a beneficial effect of this drug in relation to self-injurious behaviour. However, there are alternative explanations to this finding. Specifically, it may reflect that (1) patients with depression responding to methylphenidate are less likely to terminate treatment, meaning that only non-responders are terminated, which will not result in an increase in self-harm or suicide attempts in the reverse-mirror model; (2) patients continue methylphenidate until they have less tendency towards self-harm or suicide attempts, meaning that we will not see an increase after termination of methylphenidate; or (3) patients initiate methylphenidate treatment when they have reached a phase of their illness where they are already starting to get better, meaning that the results reflect regression to the mean. However, as the other stimulants did not seem to have equivalent effect, which would be expected if regression to the mean should explain our findings, and the number of psychiatric admissions and bed-days do not change after methylphenidate initiation, we find that the specificity of our results suggests that methylphenidate might be useful to reduce the more suicide attempts/intentional self-harm in patients with depression.
The following limitations should be borne in mind when interpreting our findings. First and foremost, as the study was based solely on register data, we did not have any detailed clinical information at our disposal, thereby making it impossible to characterize the patients who received stimulants clinically beyond their diagnosis – or to know on which indication treatment with stimulants was initiated. This is especially problematic in the modafinil group, as patients often receive modafinil due to sleep apnoea or narcolepsy. Second, when using a mirror-image model, independent events might affect outcome – for instance, an overall reduction in psychiatric facilities leading to fewer admissions in general. However, all estimates were adjusted for the overall decrease in psychiatric admissions and bed-days in Denmark, thus making this of minor importance. Third, mirror-image models might be affected by spontaneous remission of the disorder. Therefore, we employed a reverse mirror-image model as control. Fourth, we were not able to assess the compliance to the stimulants, but this is no different from RCTs without assessment of compliance via, for example, blood sampling. Fifth, the patients with depression in this study have been assigned a diagnosis in relation to assessment and treatment of mental disorders performed at psychiatric hospitals in Denmark. We do not have access to diagnoses from primary care settings, and our findings are therefore predominantly generalizable to relatively severe depression. Furthermore, not all diagnoses in the DPCRR have been validated, but the validity of those that have been tested (including depression) have been high (Bock et al., 2009; Uggerby et al., 2013). Sixth, in some of the stimulant groups we had small samples (modafinil and the amphetamines), so the results pertaining to these groups results should be interpreted with caution. Due to this limitation, we were also not able to conduct age-stratified analyses for modafinil and the amphetamines. Based on the finding that methylphenidate only seemed to reduce attempts of suicide and intentional self-harm in individuals aged ⩽30 or under, this limitation is an important one.
To our knowledge, this is the first study to investigate the effectiveness of using stimulants when treating patients diagnosed with depression, using naturalistic outcomes such as psychiatric admissions and bed-days, which may have more ecological validity compared to, for example, depression rating scales. Furthermore, the study was based on all patients in Denmark with hospital-based diagnoses of depression, who initiated treatment with stimulants. Due to this approach, the generalizability of our findings might exceed that of most RCTs, which only include patients meeting a long list of eligibility criteria. Finally, we used both a traditional model and a reverse mirror-image model. Similar conclusions were drawn from both models, thus minimizing most limitations normally known to appear in mirror-image models.
In conclusion, in this mirror-image study of 4394 patients with depression, we found no clinically relevant effect of stimulants on the number of psychiatric admissions and bed-days. However, after initiation of treatment with methylphenidate, the number of suicide attempts and intentional self-harm incidents decreased by 54%. This might indicate that methylphenidate can reduce the tendency towards suicide attempts/intentional self-harm in patients with depression, but at this point no firm conclusions can be made. Further studies – ideally randomized placebo-controlled trials – should investigate whether they can replicate our finding as intentional self-harm, suicide attempts and completed suicides remain key challenges for the psychiatric field.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.