
Abstract
Objective:
To assess changes in barriers to mental health care for children and adolescents over 16 years.
Methods:
We used data from two nationally representative surveys of Australian children and adolescents (4–17 years old), conducted in 1998 (N = 4509) and 2013–2014 (N = 6310). Barriers to care were assessed among parents who had reported a perceived partially met or unmet need for their child in the past 6 months in 1998, and the past 12 months in 2013–2014; barriers were similarly assessed among adolescents in relation to themselves. We addressed measurement inconsistencies between surveys by harmonising barriers to accommodate differences in wording and performing sensitivity analyses among those with a 1-month disorder to equalise the timeframes in which barriers were assessed. To assess change, we examined whether the rank order of the three most commonly endorsed barriers changed and whether the 95% confidence intervals (CI) around their estimates overlapped.
Results:
Similar proportions of parents reported a partially met or unmet need in 1998 (12.9%, 95% CI = [11.7, 14.0]) as in 2013–2014 (14.3%, 95% CI = [13.2, 15.3]), but the ratio of unmet to partially met need decreased from 3:1 in 1998 to 1:1 in 2013–2014. Top three parent-endorsed barriers (‘self-reliance’, ‘unsure where to get help’, and ‘cost’) were the same at both time points; ‘self-reliance’ decreased from 65.9% (95% CI = [61.1%, 70.7%]) to 34.9% (95% CI = [31.5%, 38.3%]). Top two adolescent-endorsed barriers (‘self-reliance’ and ‘concerned what others might think’) were the same at both time points, the third differed, but none of them decreased.
Conclusion:
Perceived unmet need for mental health care for children and adolescents may have decreased between 1998 and 2013–2014, but the gap in receiving sufficient care may have increased. Despite investments in community awareness and treatment during this period, key barriers seemed largely unchanged. For parents, the decrease in self-reliance may reflect a positive shift in beliefs about the potential benefits of treatment.
Background
Children and adolescents often underutilise potentially beneficial mental health care, even in countries where services are available and despite perceiving a need for care (Johnson et al., 2016, 2018; Merikangas et al., 2011; Sawyer et al., 2018). Underutilisation may result, at least in part, from barriers to mental health care. Structural barriers have included lack of available services and cost; attitudinal barriers have included lack of knowledge about mental health problems and the help-seeking process, preference for self-reliance and stigma (Gulliver et al., 2010; Reardon et al., 2017). Since the late 1990s, the Australian Government has adopted a population mental health approach, investing in large-scale promotion, prevention and treatment programmes designed to improve the mental health of Australians, including children and adolescents (Australian Government Department of Health and Ageing, 2013). This investment might have, at least indirectly, affected both attitudinal and structural barriers to mental health care for children and adolescents.
Since 2000, the Australian Government has sponsored a range of mental health promotion and prevention strategies including community awareness campaigns, youth engagement activities and school-based intervention programmes aimed at, for example, improving mental health literacy and reducing stigma. For example, beyondblue has undertaken social marketing campaigns to promote community mental health literacy about common disorders such as depression and anxiety (Yap et al., 2012); headspace has implemented campaigns to increase the number of young people accessing services, increase mental health literacy and reduce stigma among target populations such as young men (McGorry et al., 2013; Muir et al., 2009; Rickwood et al., 2019); Be You (incorporating the former MindMatters and KidsMatter initiatives), a whole-school initiative that involves children and adolescents, their teachers and parents, has provided a framework, an implementation process and key resources to promote social and emotional health and well-being across educational settings (Slee et al., 2009; Wyn et al., 2000). Evaluations of the impact of such programmes have been limited in scope and shown mixed results. For example, a general population survey of youth using a vignette-based approach portraying common mental disorders found that awareness of beyondblue mental health awareness campaigns was associated with a better recognition of some but not all examined disorders, and that the beliefs of youth regarding mental health first aid became more closely aligned with professional beliefs for all examined disorders (Yap et al., 2012). Evaluations of school-based or online programmes have shown that they might have improved mental health literacy and well-being, change stigma, and increased help-seeking behaviour, but study quality issues may have led to biased results making it difficult to draw firm conclusions (Clarke et al., 2014; Wei et al., 2013).
Over a similar period, there have been major changes in the provision of mental health treatment services (Bassilios et al., 2014; Rickwood et al., 2019). The Australian Government has introduced three major programmes designed to increase access to free or subsidised, evidence-based mental health treatment. The programmes were as follows: (1) the ‘Access to Allied Psychological Services’ (ATAPS) programme, introduced in 2001 and running until 2016; (2) the ‘Better Access to Psychiatrists, Psychologists and General Practitioners’ (Better Access) initiative, introduced in 2006; and (3) headspace, also introduced in 2006, specifically targeting youth health with emphasis on early intervention and improving access to care (McGorry et al., 2013, 2007). ATAPS and Better Access enable general practitioners to refer individuals to psychologists or other trained mental health care providers for treatment and is available to all children and adolescents with mental health or substance use problems. Headspace treatment services integrate youth-friendly healthcare focusing on well-being and early intervention, specifically targeted at young people aged 12–25 years with mental health and substance use issues (McGorry et al., 2013). Prior to the introduction of these programmes, Australian children and adolescents and their families usually had to cover the costs of mental health treatment themselves, either directly or through private health insurance, and services were scarce. Evaluation of these programmes has shown that they are reaching individuals who have not previously received psychological or other mental health care (Bassilios et al., 2014, 2017) and might reduce psychological distress and improve psychosocial functioning (Rickwood et al., 2015).
Whether outlined programmes have, at least indirectly, affected attitudinal or structural barriers to mental health care for Australian children and adolescents over time is currently unknown. Therefore, this study aimed to examine whether barriers to care changed over the 16-year period from 1998 to 2013–2014. We separately examined changes for parents and for adolescents. This is important because parents are usually the gatekeeper for their child’s mental health care. However, adolescents take an active part in their own help-seeking process and may even self-refer (Rickwood et al., 2007), and they often disagree with their parents regarding whether help is needed or experience different barriers to care (Boulter and Rickwood, 2013; Gulliver et al., 2010; Jorm et al., 2007; Reardon et al., 2017; Sayal et al., 2010; Schnyder et al., 2019; Yap et al., 2013). We also examined changes separately for children and adolescents with an unmet need (i.e. those who perceived a need for care but did not receive any help) and those with a partially met need (i.e. those who received some help but wanted more). It is possible that some of the reforms to mental health services may have facilitated the pathway into treatment but might not necessarily guarantee that perceived needs are fully met by treatment.
Methods
Two Australian nationally representative surveys of child and adolescent mental health and well-being – the only two of their kind to have repeatedly assessed perceived need for mental health care and barriers to care – provided a unique opportunity to examine barriers to care at the beginning or before major policy changes (in 1998) and many years into those changes (in 2013–2014). Importantly, both surveys assessed a range of structural and attitudinal barriers to care for those reporting a partially met or unmet need for care, but some of them differed. Where possible, we harmonised them to maximise comparability. Furthermore, the two surveys assessed barriers for different periods of time: past 6 months in 1998 and past 12 months in 2013–2014. To address this difference, we considered relative changes in barriers to care rather than absolute changes and we performed a sensitivity analysis restricting the sample to children and adolescents with a parent-reported 1-month mental disorder as this was common to both surveys and to equalise the denominator. Children and adolescents aged 4–17 years were randomly selected from Australia’s general population for both surveys (Hafekost et al., 2016; Sawyer et al., 2000). For this study, information on barriers to care for adolescents was collected from both parents and adolescents (aged 13–17 years), but for younger children (aged 4–12 years) it was only collected from parents.
Survey design and participants
The 1998 survey (Sawyer et al., 2019) was conducted between February and May 1998; see Sawyer et al. (2000) for details. Briefly, multistage probability sampling was used to identify households from which a representative sample of Australian children and adolescents (aged 4–17 years) was drawn. If more than one eligible child or adolescent lived in the household, the study participant with the birthday nearest to the interview date was selected. Trained interviewers conducted face-to-face interviews with one parent from each household; adolescents (aged 11–17 years) that agreed to participate in the self-report completed a pen-and-paper questionnaire. Children aged 4–10 years did not participate directly. Of eligible households, 4509 parents participated – a response rate of 70%. Of 1490 adolescents approached, 1284 (86%) completed the self-report. The Research Ethics Committee at the Women’s and Children’s Hospital, Adelaide, approved this survey.
The 2013–2014 (Zubrick et al., 2017) survey was conducted between June 2013 and April 2014; see Hafekost et al. (2016) for details. Briefly, multistage, area-based random sampling was used to identify households with at least one child or adolescent aged 4–17 years. If more than one eligible child or adolescent lived in the household, the study participant was selected randomly. Trained interviewers conducted face-to-face interviews with one parent or primary carer (hereafter, parent); adolescents (aged 11–17 years) completed a questionnaire on a tablet computer. Children aged 4–10 years did not participate directly. Of eligible households, 6310 parents participated – a response rate of 55%. Of 2604 adolescents approached, 2314 (89%) completed the self-report. The Ethics Committee of the Australian Government Department of Health approved this survey.
There were some differences in the designs of the two surveys with respect to sampling methods (see eTable 1, Online Appendix). However, the socio-demographic characteristics of participants in both surveys have been shown to reflect those of the Australian child and adolescent population (Hafekost et al., 2016; Sawyer et al., 2000).
The Human Ethics Research Office of The University of Queensland exempted the current study from ethics review due to negligible risk.
Defining the samples for analyses
For the current study, we defined the samples for analyses as parents who reported a partially met or unmet need for mental health care for their child or adolescent (aged 4–17 years) and adolescents aged 13–17 years who reported a partially met or unmet need for care for themselves. This was because only those who reported a partially met or unmet need were asked about barriers to care.
In the 1998 survey, parents were asked a series of questions about perceived need for mental health care. Parents who reported that their child had used any of four types of help (counselling, medicine or tablets, psychological testing, or ‘other type of help’) in the past 6 months for an emotional or behavioural problem were asked whether they felt that their child needed more help than was received. If they answered yes to any of them, they were considered to have a partially met need. Parents who reported that their child had not used any of the four types of help in the past 6 months were asked whether they felt that their child needed help for an emotional or behavioural problem from those same types of help. If these parents answered yes to any of them, they were considered to have an unmet need. The 2013–2014 survey used a similar approach, except that there were some differences in the four types of help (counselling, medication, information and skill-training) and the timeframe was the past 12 months.
In the 1998 survey, adolescents were asked two questions to assess their perceived need for care: (1) whether they thought that they needed professional help with an emotional or behavioural problem in the past 6 months (yes/no) and, if yes, (2) whether they got the help they needed (yes/no). We considered adolescents answering no to the second question as either having a partially met or an unmet need as they could have received some help but not enough or no help at all, but separate measures of partially met and unmet need could not be derived. In the 2013–2014 survey, the assessment of adolescent-reported perceived need for care was the same as for parents in 2013–2014. That is, partially met and unmet need were assessed in relation to four types of help (counselling, medication, information and skill-training) over the past 12 months, but were combined into a single group to enable comparison with 1998 survey data (for more details, see eTable 1, Online Appendix).
Measures
Parent-endorsed barriers to care
Parents who reported either a partially met or unmet need were presented with a list of barriers to care and answered yes or no to each one of them. In 1998, interviewers read out a list of barriers to parents; in 2013–2014, interviewers showed the list on a printed card. Some but not all barriers asked in each survey overlapped. Therefore, we created a harmonised set of barriers in which barriers were labelled as mapping: exactly if they assessed the same content; approximately if some but not all of the content overlapped; or not at all if they were only assessed in one of the two surveys (see eTable 2, Online Appendix).
Adolescent-endorsed main barriers to care
Adolescent-endorsed barriers to mental health care in both surveys were assessed in adolescents aged 13–17 years who reported a partially met or unmet need. At both time points, these adolescents read a list of barriers to care and were asked to identify the main barrier to care. In 2013–2014, the survey additionally allowed adolescents to endorse multiple barriers, but, to maximise comparability of the two surveys, we used only the main barriers. Rules for harmonising the barriers were the same as for parents (see eTable 3, Online Appendix).
Additional measures
In both surveys, parents completed the Diagnostic Interview Schedule for Children, Version IV (DISC-IV) modules for major depressive disorder (MDD), attention-deficit/hyperactivity disorder (ADHD) and conduct disorder (CD), which operationalises Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV) criteria for each these disorders. We used the 1 month disorder diagnoses.
Statistical analysis
For each survey, we applied survey weights to the data and analyses accounted for clustering to represent the estimated population of interest according to the 1996 and the 2011 Australian census, respectively. Statistical analyses were performed in R version 3.6.0 (R Core Team) using the package survey (Lumley, 2010). We excluded cases with missing data both on perceived need and on barriers to care (Figure 1, panel A).
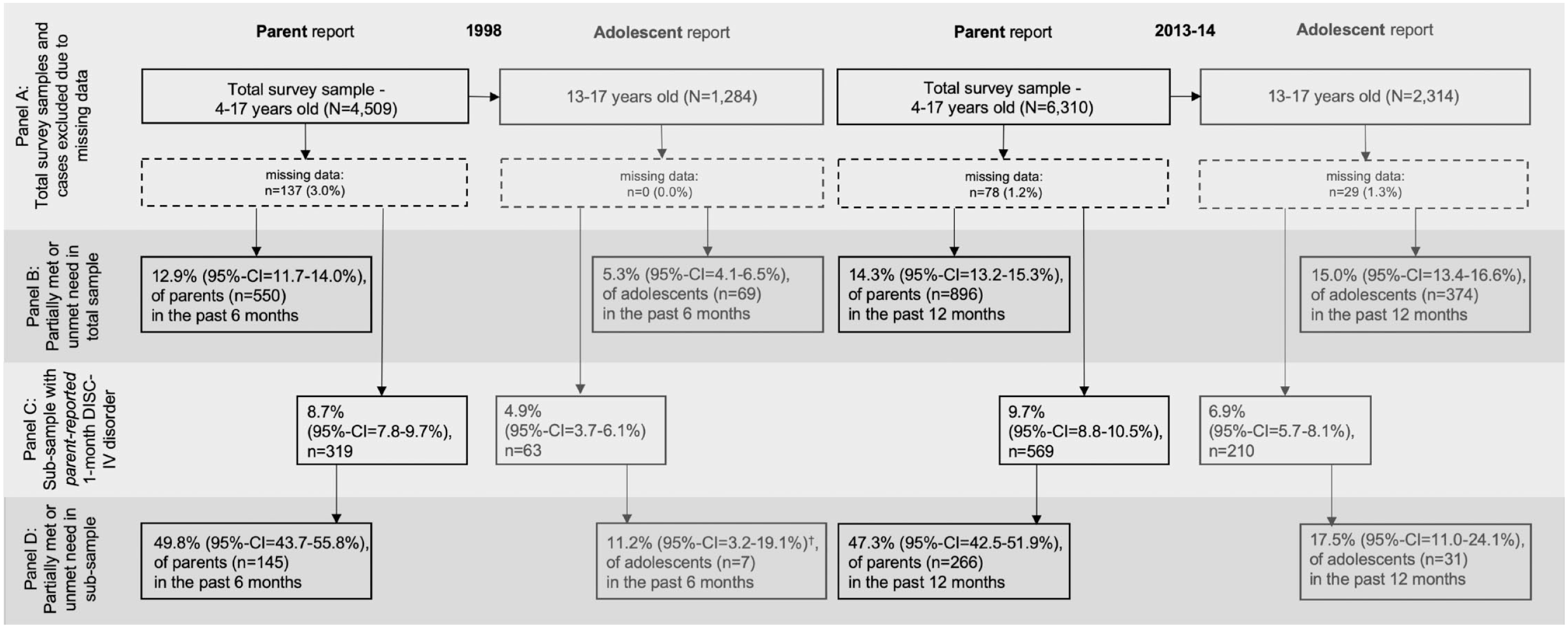
Frequencies of endorsed barriers to care in the two surveys – parent report (children and adolescents aged 4–17 years) and adolescent self-report (13–17 years) of total survey sample including sensitivity analysis for parent-reported 1-month DISC-IV disorder (MDD, ADHD, CD).
We examined change over time in parent-endorsed barriers for three groups: (1) the total child and adolescent sample (4–17 years old), (2) the total sample stratified by age (4–12 and 13–17 years old) and (3) the total sample stratified by level of perceived need (partially met and unmet need). In addition, we examined change over time in self-endorsed main barriers to care for adolescents (aged 13–17 years); we could not stratify the adolescent sample by level of perceived need because the 1998 survey did not allow us to distinguish between unmet and partially met need.
The different timeframes in which barriers were assessed in the two surveys (6 months in the 1998 survey vs 12 months in the 2013–2014 survey) may have accounted for some observed differences between the two surveys. To account for that, we conducted sensitivity analyses for parent-reported barriers for the total child and adolescent sample and for adolescent-reported barriers using only the sub-samples with a parent-reported 1-month mental disorder (MDD, ADHD and/or CD). This equalised the denominator of endorsed barriers for both surveys and we were able to examine them over the same period of time which was 1 month. We reasoned that, if patterns were similar to the ones found in the total samples, we could be more confident with the main findings.
For each analysis, we reported weighted percentages and 95% confidence intervals (CIs) for respondents endorsing each harmonised barrier. We analysed change over time of approximately or exactly mapping barriers in two ways. First, we ranked the top three barriers according to how frequently they were endorsed in each survey with barriers within ±2% of each other receiving the same rank and examining whether the top three barriers changed over time. Because of the differences in how barriers to care were assessed in the two surveys, the rank represents the relative importance of each barrier in that year among those with partially met or unmet need. Second, we examined overlap of 95% CIs of the 1998 and the 2013–2014 estimates, with no overlap indicating that estimates differed from each other. This is slightly more conservative than formal significance testing (Knol et al., 2011; Schenker and Gentleman, 2001). We followed Australian Bureau of Statistics (ABS) conventions for reporting; estimates with a relative standard error (RSE) between ⩾25% and ⩽50% should be interpreted with caution and those with an RSE >50% are considered too unreliable for use and so were not reported.
Results
Descriptives
Figure 1 shows how the samples for analysis were derived. For each survey year (1998 and 2013–2014), it shows the total number of participants for whom parent- and adolescent-report data were available (panel A) and, among those, the proportions reporting a partially met or unmet need (panel B). It also shows the number of participants with a parent-reported 1-month DISC-IV disorder (MDD, ADHD, CD) (panel C) and, among those, the proportions reporting a partially met or unmet need (panel D). The number of cases excluded from analysis due to missing data was small.
Similar proportions of parents reported a partially met or unmet need among the total sample and the sub-sample with a 1-month disorder in 1998, compared to 2013–2014. At each timepoint, the proportion of parents who reported partially met or unmet need was larger among the 1-month sub-sample than among the total survey sample.
A larger proportion of adolescents reported a partially met or unmet need in 1998 than in 2013–2014 in the total sample of adolescents, but among those with 1-month disorder there was potentially no difference.
Gender and age distributions of the samples for analysis were similar in 2013–2014 as in 1998. In 1998, 48.8% (95% CI = [47.2%, 50.3%]) of children and adolescents whose parents reported a partially met or unmet need in the past 6 months were female and the mean age was 10.5 (95% CI = [10.4, 10.6]); in 2013–2014, the corresponding figures were 48.7% (95% CI = [47.3%, 50.0%]) and 10.4 (95% CI = [10.3, 10.6]). In 1998, 49.6% (95% CI = [47.0%, 52.3%]) of adolescents who reported a partially met or unmet need were female and the mean age was 14.9 (95% CI = [14.9, 15.0]); in 2013–2014, the figures were 48.7% (95% CI = [46.5%, 51.0%]) and 15.0 (95% CI = [14.9, 15.1]).
Changes between 1998 and 2013–2014 in parent-endorsed barriers to mental health care for children and adolescents
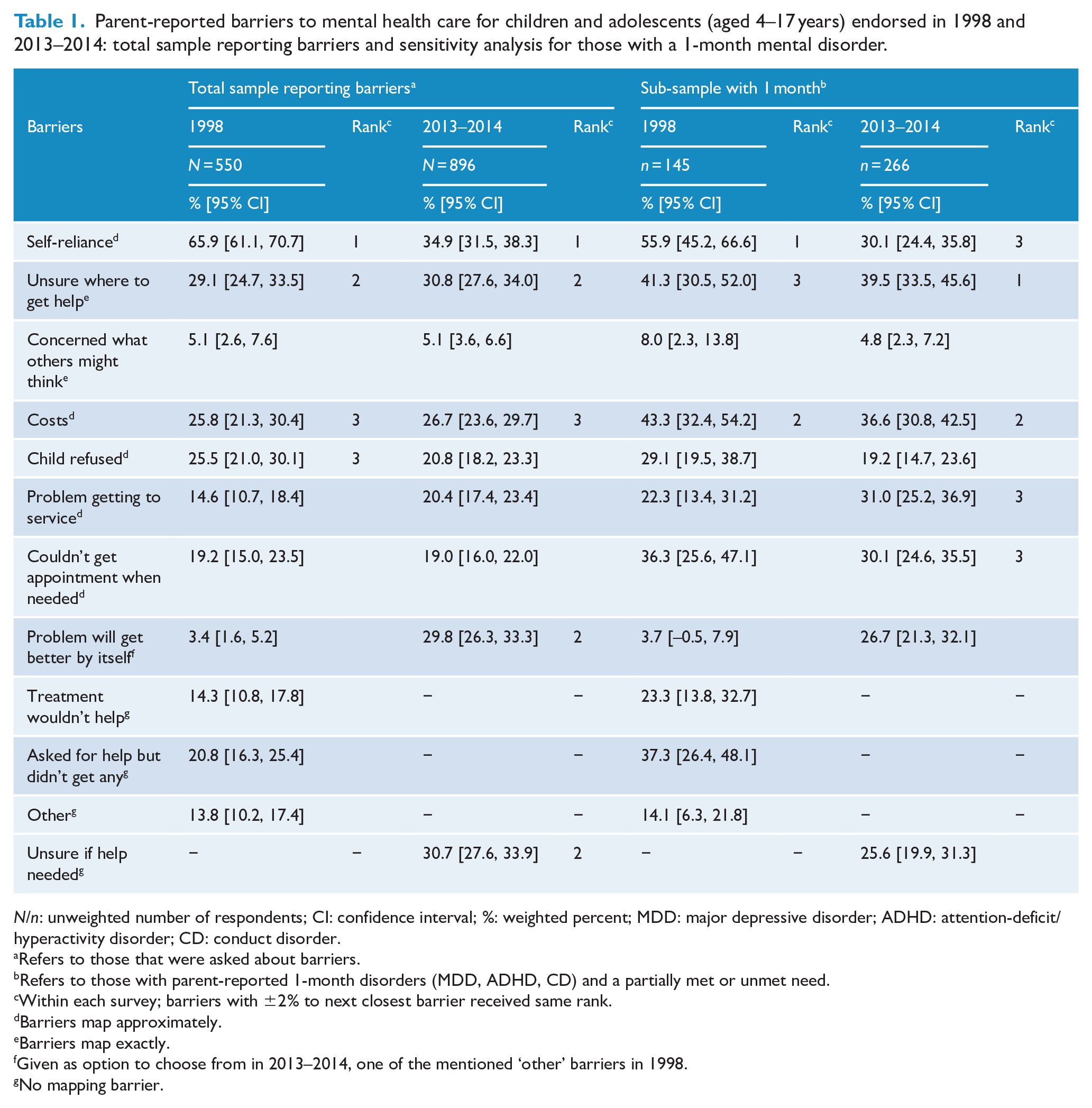
Table 1 shows changes in parent-endorsed barriers to mental health care for children and adolescents (aged 4–17 years). Only seven out of 12 barriers mapped exactly or approximately and were comparable between 1998 and 2013–2014. We found that the top three barriers – ‘self-reliance’, ‘unsure where to get help’ and ‘costs’ – had the same ranks at both time points. In contrast, ‘child refused’ was ranked third in 1998 but was unranked in 2013–2014. Using the criterion of non-overlapping CIs, only ‘self-reliance’ decreased between 1998 and 2013–2014. In 2013–2014, ‘problem will get better by itself’ and ‘unsure if help is needed’ were also ranked second, but they were not assessed in a comparable way in 1998.
Parent-reported barriers to mental health care for children and adolescents (aged 4–17 years) endorsed in 1998 and 2013–2014: total sample reporting barriers and sensitivity analysis for those with a 1-month mental disorder.
N/n: unweighted number of respondents; CI: confidence interval; %: weighted percent; MDD: major depressive disorder; ADHD: attention-deficit/hyperactivity disorder; CD: conduct disorder.
Refers to those that were asked about barriers.
Refers to those with parent-reported 1-month disorders (MDD, ADHD, CD) and a partially met or unmet need.
Within each survey; barriers with ±2% to next closest barrier received same rank.
Barriers map approximately.
Barriers map exactly.
Given as option to choose from in 2013–2014, one of the mentioned ‘other’ barriers in 1998.
No mapping barrier.
Similar patterns were found in the sub-sample of children and adolescents with a 1-month mental disorder. The top three barriers were the same as in the main analysis, albeit with a slightly different ranking order. Again, based on CIs, only ‘self-reliance’ decreased from 1998 to 2013–2014.
Changes between 1998 and 2013–2014 in parent-reported barriers to mental health care for 4- to 12-year-olds and 13- to 17-year-olds
Among the total survey samples, similar proportions of parents had reported a partially met or unmet need for 4- to 12-year-olds across surveys with 8.2% (95% CI = [7.4%, 9.1%]) reporting it in 1998 and 8.5% (95% CI = [7.7%, 9.3%]) in 2013–2014; this was also true for 13- to 17-year-olds with 4.7% (95% CI = [3.9%, 5.4%]) reporting it in 1998 and 5.8% (95% CI = [5.2%, 6.5%]) in 2013–2014.
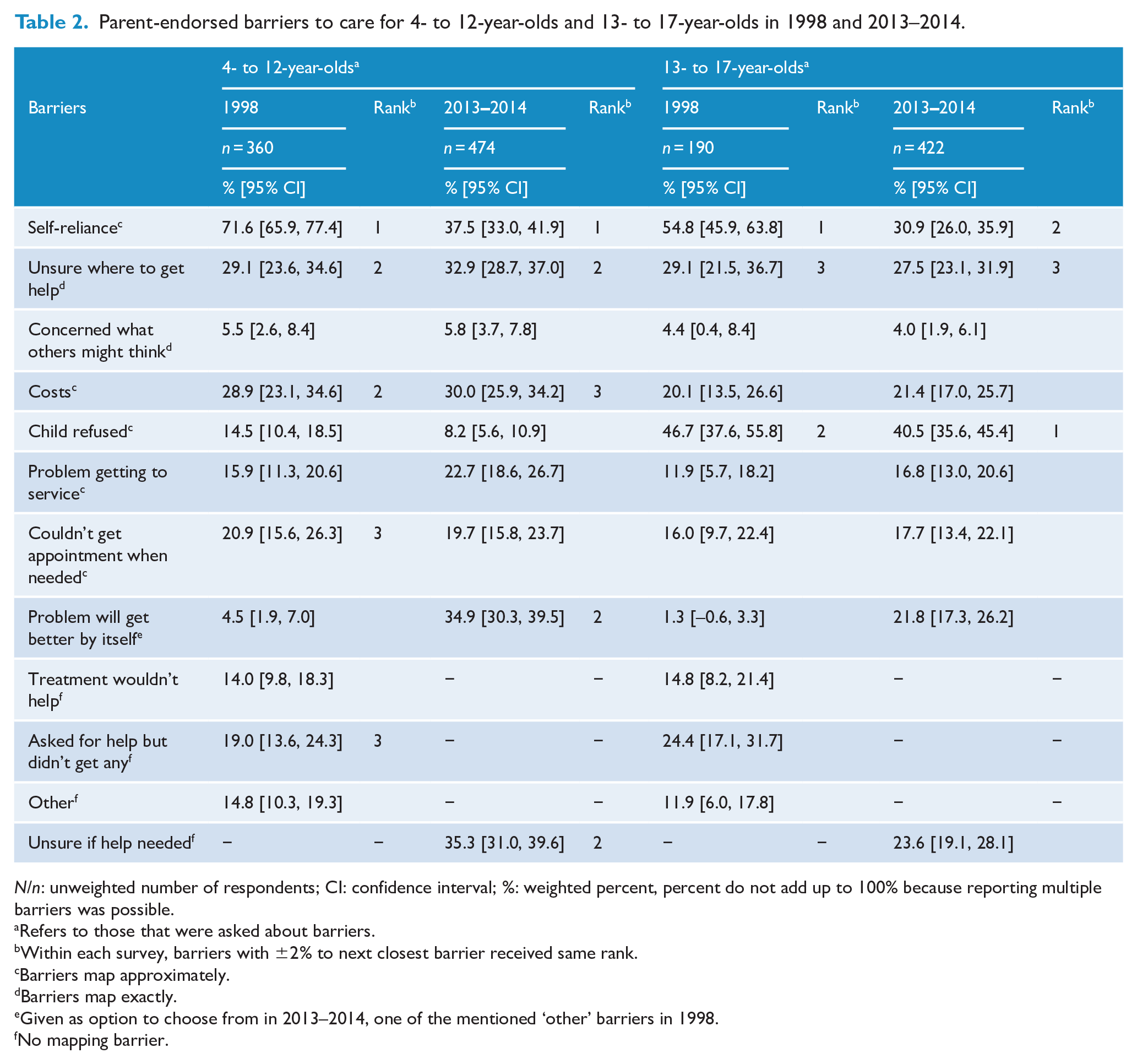
Among 4- to 12-year-olds, the top three barriers were generally similar at both time points with some slight differences in the ranking order (Table 2). This was also true among the 13- to 17-year-olds. Based on overlapping CIs, only ‘self-reliance’ decreased from 1998 to 2013–2014 for both 4- to 12-year-olds and 13- to 17-year-olds. In addition, for 4- to 12-year-olds, the following barriers were highly ranked at one of the time points but not assessed in an equivalent way at both time points: ‘asked for help but didn’t get any’, ‘problem will get better by itself’ and ‘being unsure if help was needed’.
Parent-endorsed barriers to care for 4- to 12-year-olds and 13- to 17-year-olds in 1998 and 2013–2014.
N/n: unweighted number of respondents; CI: confidence interval; %: weighted percent, percent do not add up to 100% because reporting multiple barriers was possible.
Refers to those that were asked about barriers.
Within each survey, barriers with ±2% to next closest barrier received same rank.
Barriers map approximately.
Barriers map exactly.
Given as option to choose from in 2013–2014, one of the mentioned ‘other’ barriers in 1998.
No mapping barrier.
We further noted that, at both time points, ‘child refused’ was an important barrier to care for 13- to 17 -year-olds but less for 4- to 12 -year-olds; ‘cost’ was important for 4- to 12 -year-olds but less for 13- to 17 -year-olds.
Changes between 1998 and 2013–2014 in adolescent-endorsed main barriers to mental health care
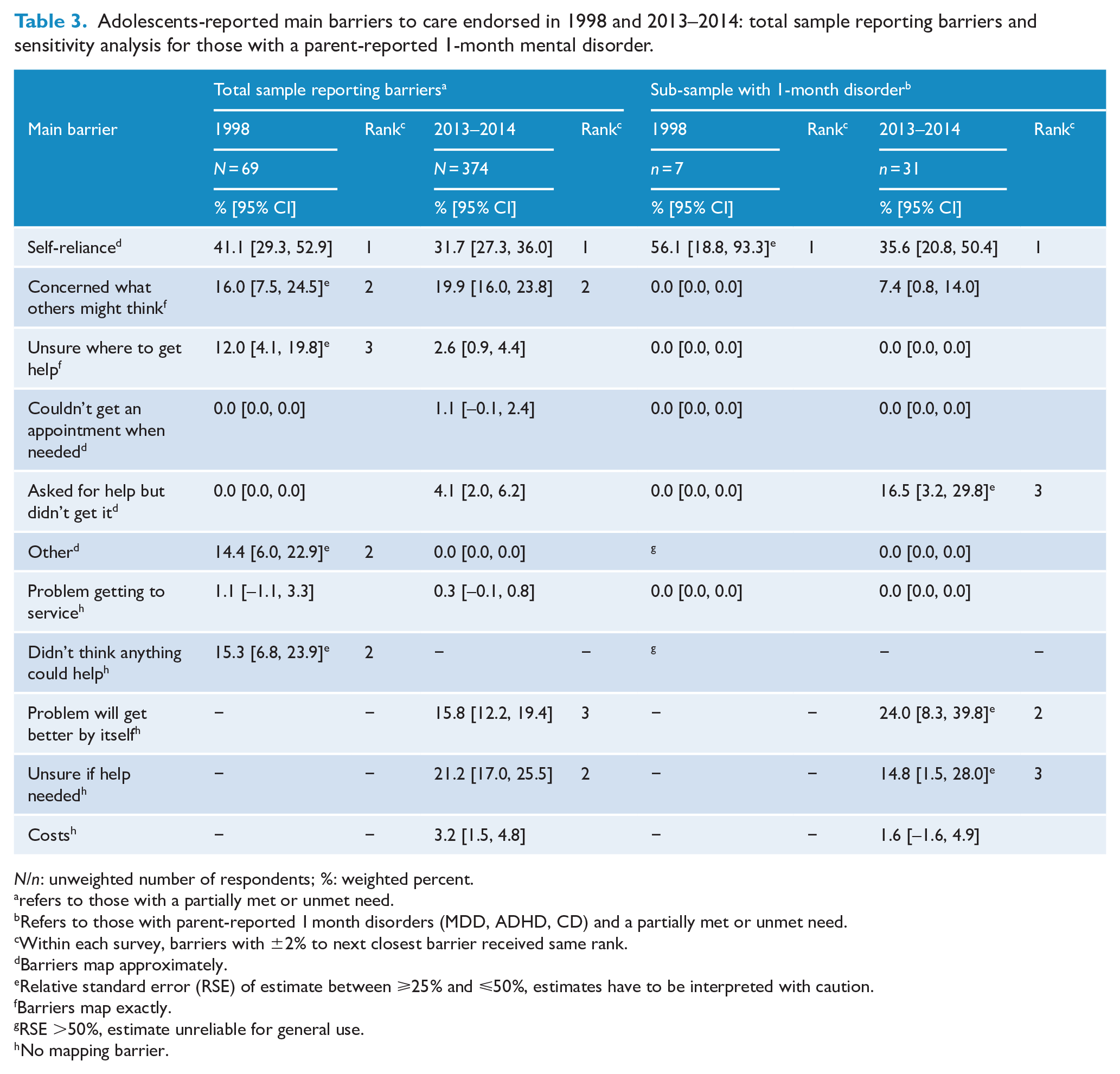
Estimates of adolescent-endorsed main barriers had large RSEs, with the exception of ‘self-reliance’. Six out of 11 main barriers endorsed by adolescents mapped exactly or approximately (Table 3). The top two barriers – ‘self-reliance’ and ‘concerned what others might think’ – had the same rank at both time points. In contrast, ‘unsure where to get help’ was ranked third in 1998 but was unranked in 2013–2014. Based on overlapping CIs, none of these top three main barriers changed over time. Other barriers were additionally ranked among the top three at one time point but were not assessed in a comparable way at the other time point: ‘problem will get better by itself’, ‘unsure if help is needed’ and ‘didn’t think anything could help’.
Adolescents-reported main barriers to care endorsed in 1998 and 2013–2014: total sample reporting barriers and sensitivity analysis for those with a parent-reported 1-month mental disorder.
N/n: unweighted number of respondents; %: weighted percent.
refers to those with a partially met or unmet need.
Refers to those with parent-reported 1 month disorders (MDD, ADHD, CD) and a partially met or unmet need.
Within each survey, barriers with ±2% to next closest barrier received same rank.
Barriers map approximately.
Relative standard error (RSE) of estimate between ⩾25% and ⩽50%, estimates have to be interpreted with caution.
Barriers map exactly.
RSE >50%, estimate unreliable for general use.
No mapping barrier.
In the sub-sample of adolescents with a parent-reported 1-month mental disorder, only the results for ‘self-reliance’ can be interpreted; the pattern was similar to that of the total sample.
Changes between 1998 and 2013–2014 in barriers to mental health care for children and adolescents among those with a perceived unmet or partially met need
Among the total survey samples, a smaller proportion of parents reported a partially met need in 1998 (3.2%, 95% CI = [2.7%, 3.8%]) than in 2013–2014 (6.8%, 95% CI = [6.0%, 7.5%]), and a larger proportion of parents had reported an unmet need in 1998 (9.6%, 95% CI = [8.7%, 10.6%]) than in 2013–2014 (7.5%, 95% CI = [6.7%, 8.3%]).
Among those with a partially met need the top three barriers were generally similar at both time points with some slight differences in the ranking order (Table 4). Based on overlapping CIs, none of these barriers changed over time. Among those with an unmet need, top three barriers differed somewhat, but only ‘self-reliance’ and ‘child refused’ decreased from 1998 to 2013–2014. ‘Couldn’t get an appointment when needed’ also decreased from 1998 to 2013–2014, despite not being among the top three barriers.
Parent-reported barriers to mental health care for children and adolescents endorsed in 1998 and 2013–2014: stratified by partially met and unmet need.
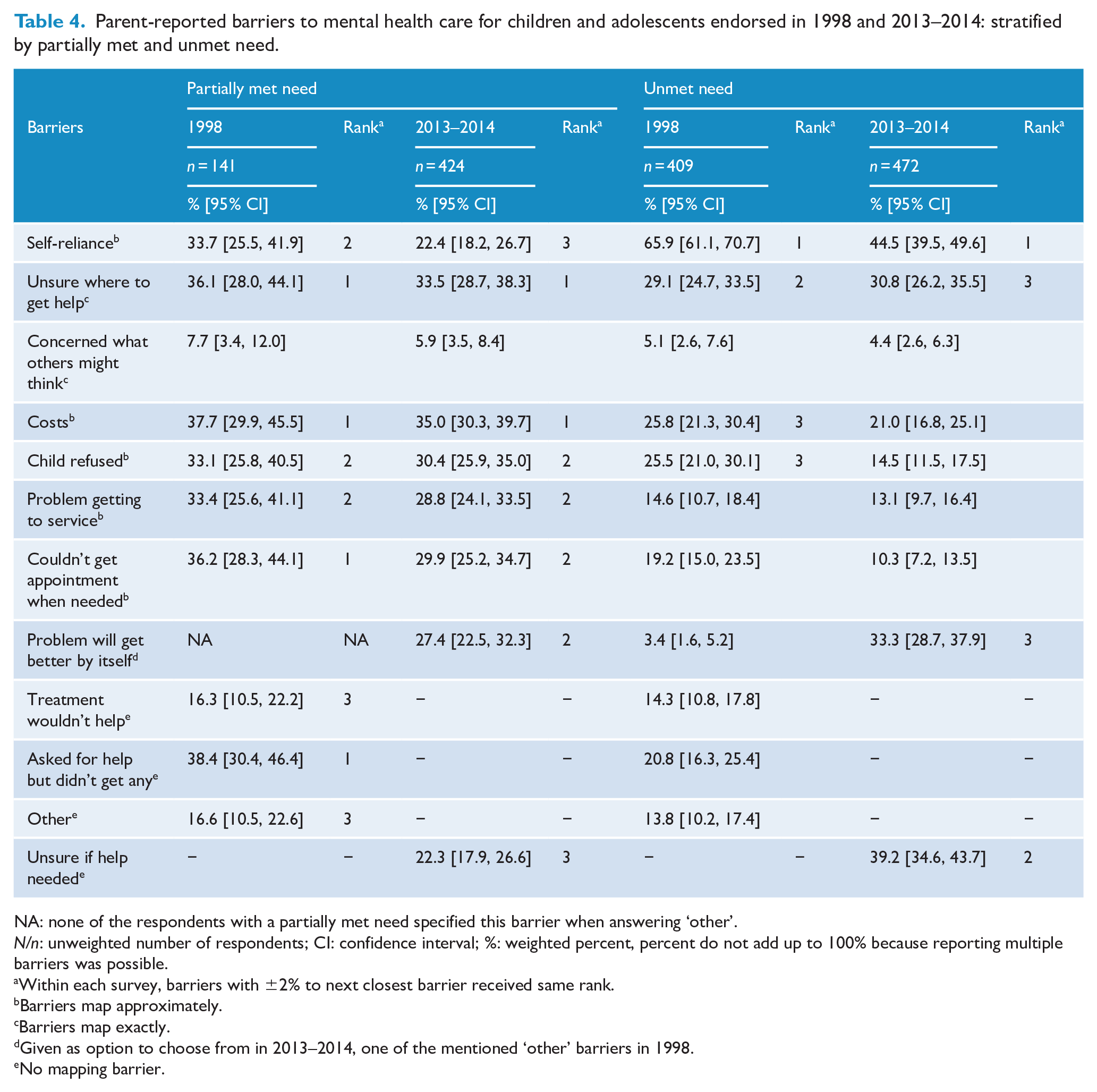
NA: none of the respondents with a partially met need specified this barrier when answering ‘other’.
N/n: unweighted number of respondents; CI: confidence interval; %: weighted percent, percent do not add up to 100% because reporting multiple barriers was possible.
Within each survey, barriers with ±2% to next closest barrier received same rank.
Barriers map approximately.
Barriers map exactly.
Given as option to choose from in 2013–2014, one of the mentioned ‘other’ barriers in 1998.
No mapping barrier.
In addition, at both time points, two of the comparable barriers seemed more important for those with a partially met need than those with an unmet need ( ‘problem getting to a service’ and ‘couldn’t get an appointment when needed’).
Discussion
Our study provides the first findings on changes over time in barriers to mental health care for children and adolescents. Findings suggest that, in Australia, between 1998 and 2013–2014, there has been a decrease in the ratio of unmet need to partially met need for child and adolescent mental health care, at least according to parents. There were also shifts in the relative importance of some barriers to care; notably, desire to ‘handle the problem on their own’ (‘self-reliance’) was less prevalent among parents in 2013–2014 than in 1998, but was unchanged among adolescents. Other barriers (e.g. ‘unsure where to get help’, ‘cost’ or ‘concerned what others might think’ (stigma)) did not decrease for parents nor adolescents, despite investments that might have been expected to reduce them. There were also shifts in the relative importance of some barriers (‘self-reliance’, ‘couldn’t get an appointment’ and ‘child refused help’) among those with unmet but not partially met need.
Our study had four key findings. First, the ratio of parent-reported unmet need to partially met need decreased over time, from 3:1 in 1998 to 1:1 in 2013–2014. This may indicate that, according to parents, fewer children and adolescents have perceived an unmet in 2013–2014 than they did in 1998, but they often did not receive sufficient care. This finding is consistent with an earlier analysis using the same two surveys which showed an increase in service use by Australian children and adolescents between 1998 and 2013–2014 (Johnson et al., 2016; Lawrence et al., 2015). It is also consistent with findings from a survey of Australian adults which showed a significant decrease in unmet but no change in partially or fully met need between 1997 and 2007 (Meadows and Bobevski, 2011). Efforts to address barriers to care should, therefore, be equally targeted at people who have used services, and those who have not.
Second, many attitudinal barriers to care seemed largely unchanged between 1998 and 2013–2014, despite investments in community awareness programmes. For example, in 1998 and 2013–2014, similar proportions of parents and adolescents seemed to be ‘unsure where to get help’, one aspect of mental health literacy, despite earlier general population surveys that reported improvements in other aspects of mental health literacy such as recognition of mental disorders or beliefs about treatment (Jorm et al., 2006a; Reavley and Jorm, 2012a). This might reflect underlying service-level problems such as challenges in navigating through a complex health care system or a lack of information about available services (Anderson et al., 2017). In another example, being ‘concerned what others might think’ seems to not have changed. Findings from an earlier population-based study indicated that certain aspects of stigmatising attitudes towards a person with a mental disorder (e.g. social distance) have decreased over the years while others have increased (e.g. beliefs about dangerousness or unpredictability) (Reavley and Jorm, 2012b). Taken together, these findings suggest that changes in one type of stigma might not translate into other types of stigma, particularly when reported as a barrier to care. In contrast, the desire to ‘handle the problem on their own’ (‘self-reliance’) decreased among parents, but not adolescents, between 1998 and 2013–2014. On one hand, this may be a potentially encouraging finding; it may reflect more positive beliefs among parents regarding the potential benefit of mental health interventions (Jorm et al., 2006b; Morgan et al., 2014; Reavley and Jorm, 2011) or towards health professionals (Jennings et al., 2015). On the other hand, despite this decrease, self-reliance remained (one of) the most important barriers to care for both parents and adolescents in 2013–2014.
Third, key parent-reported structural barriers relating to access and availability of mental health care for children and adolescents were largely unchanged between 1998 and 2013–2014, despite major policy changes intended to increase the availability of treatment services in Australia. ‘Cost’ of treatment was an important barrier in 1998, and remained so in 2013–2014, after the introduction of government-funded programmes that offered free or subsidised mental health care. This was particularly so for 4- to 12 -year-olds, suggesting an undersupply of specialised free or low-cost child mental health care relative to perceived need. Most of these programmes offer a limited amount of free or subsidised treatment sessions, which may not be sufficient for children and adolescents with more complex treatment needs; this might, in part, explain why cost for those with a partially met need remained one of the most important barriers at both time points. These findings may also support recent estimates that a fivefold increase in community-based state-funded child and adolescent services is needed to meet current clinical need in Australia (Segal et al., 2018).
Fourth, decreases in the relative importance of some barriers were observed in the unmet need group only, namely, ‘self-reliance’, ‘couldn’t get an appointment when needed’, and ‘child refused help’. Moreover, according to parents, some structural barriers (‘problem getting to a service’, and ‘couldn’t get an appointment when needed’) were more important for those who perceived a partially met need than an unmet need, both in 1998 and in 2013–2014. This finding might be in line with a recent systematic review that concluded that structural barriers such as waiting times and difficulties getting a referral are particularly important among families of service users (Reardon et al., 2017). Overall, these findings may suggest a need to focus on making services available at the right place and time, so that people who have started treatment will persist with it.
Important limitations should be acknowledged. First, our findings are based on two cross-sectional surveys; therefore, we cannot be sure whether the observed changes in population patterns regarding barriers to care occurred because of specific policy changes. For this, randomised controlled trials or similar study designs are needed (Sanson-Fisher et al., 2014). However, because the first survey assessed barriers before and the second after policy changes, we can consider whether it is plausible to interpret the findings in the context of these major policy changes, as has been done before (Meadows and Bobevski, 2011). Second, the assessment of perceived need among adolescents and, to a lesser extent, parents differed between surveys and may have affected the comparability of the samples included in the analysis. Third, the main outcome of this study, barriers to care, was not measured consistently across the two surveys (Schwarz, 1999). To address these differences, we (1) harmonised barriers to care to maximise comparability and have only interpreted results of those barriers that were exactly or approximately comparable; (2) conducted sensitivity analyses restricting reported perceived need and barriers to care to children and adolescents with a 1-month disorder in order to equalise the timeframe in which perceived need and barriers to care were assessed; (3) compared the relative rankings of the top three most frequently endorsed barriers (a narrative approach); and (4) refrained from formal significance testing, instead using a more conservative statistical method (overlap of 95% CIs) to test for changes over time. In the sensitivity analyses, particularly for the parent-report, the statistical analyses showed similar patterns of partially met or unmet need and barriers to care at both timepoints, and the narrative approach showed that the rankings of the most frequently endorsed barriers to care remained the same for all investigated groups. Furthermore, our study showed that there were few changes overall but where there were changes, they were quite large, therefore less likely to be due to methodological differences alone. Therefore, we were able to interpret key findings with confidence despite outlined limitations.
Recommendations for future surveys
For future surveys, it would be desirable to align the assessment of, for example, perceived need and barriers to care by retaining the same wording wherever possible and by retaining the same time frames in which these factors were assessed, to ensure comparability over time. However, it may also be useful to include barriers that our study found to be important in 1998 but were not assessed in 2013–2014 (e.g. ‘problem will get better by itself’ or ‘unsure if help needed’).
Conclusion
Barriers to mental health care for children and adolescents remain challenging. We found that, perceived unmet need for mental health care for children and adolescents may have decreased between 1998 and 2013–2014 but the gap in receiving sufficient care may have increased. Overall, most barriers to care seemed unchanged. Parents were less likely to endorse self-reliance as a barrier in 2013–2014; this may be the result of mental health awareness and promotion efforts to increase mental health literacy and reduce stigma. However, in 1998 and 2013–2014, both adolescents and parents were equally ‘unsure where to get help’ and adolescents in particular were ‘concerned what others might think’ if they sought help. Regarding structural barriers, there remains a need to increase the supply of free or low-cost treatment options. Given that partially met need was more common in 2013–2014 than in 1998, and that no barriers had decreased in relative importance in this group, future efforts should address barriers to receiving sufficient care among those who have used services.
Supplemental Material
online_appendix – Supplemental material for Barriers to mental health care for Australian children and adolescents in 1998 and 2013–2014
Supplemental material, online_appendix for Barriers to mental health care for Australian children and adolescents in 1998 and 2013–2014 by Nina Schnyder, Michael G Sawyer, David Lawrence, Radoslaw Panczak, Philip Burgess and Meredith G Harris in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would like to thank all the families that participated in the surveys; the survey teams and reference groups for implementing the surveys; the University of Adelaide and ACNielsen for conducting the first survey (Sawyer et al., 2019); and the University of Western Australia, the Telethon Kids Institute, Roy Morgan Research and the team of interviewers for conducting the second survey (Zubrick et al., 2017). We would also like thank Prof. Harvey A. Whiteford for his support.
Availability of Data and Materials
The Australian Data Archive (ADA) provided us with the data for both surveys. We are not able to directly share these data but researchers inside and outside of Australia can apply for the data with the ADA. The data application form, documentations and, once ADA granted access, the data itself can be accessed at https://dataverse.ada.edu.au/dataset.xhtml?persistentId=doi:10.4225/87/LCVEU3 and https://dataverse.ada.edu.au/dataset.xhtml?persistentId=doi:10.26193/QGXQ47. R scripts that were used for statistical analyses in this publication before (09_ChangeOverTime_191018.Rmd) and after revisions (10_ChangeOverTime_200104_Publication_AfterRevisions.Rmd) can be found at ![]() on the Open Science Framework.
on the Open Science Framework.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The research Ethics Committee at the Women’s and Children’s Hospital in South Australia (affiliated with the University of Adelaide’s Human Research Ethics Committee) approved the 1998 survey (REC768) and the Ethics Committee of the Australian Government Department of Health approved the 2013–2014 survey (reference no. 17/2012). The Human Ethics Research Office of the University of Queensland exempted the current study from ethics review due to negligible risk (Clearance Number: 2018001176).
Funding
The author(s) disclosed receipt of the following financial supportfor the research, authorship and/or publication of this article: N.S. was funded by the Swiss National Science Foundation (SNSF) Early Postdoc.Mobility fellowship (grant number: P2BEP3_181901). N.S.’s funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. This study used data from the two Australian surveys on child and adolescent mental health and well-being that were funded by the Australian Government Department of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.