
Abstract
Objective:
To review a clinical practice improvement approach to statewide implementation of smoking care in adult acute mental health inpatient units across public mental health services in Queensland.
Method:
Queensland public mental health services, with adult acute inpatient units, joined a statewide collaborative to work together to increase the routine screening of smoking and delivery of a Smoking Cessation Clinical Pathway brief intervention to identified smokers.
Results:
Over a 2-year period, statewide improvements were demonstrated in the recording of smoking status (88–97%) and in the provision of a brief smoking cessation intervention to smokers (38–73%). In addition, all individual mental health services increased the delivery of a brief intervention to identified smokers and the recording of smoking status either improved or remained at high levels.
Conclusion:
Smoking remains an ongoing challenge for mental health services and one of the most important physical health issues for people living with a mental illness. The ability to implement statewide smoking care in public mental health services is an important step in shifting poor health outcomes. The clinical practice change approach adopted in Queensland has demonstrated encouraging outcomes in improving the delivery of smoking care that has been sustained over a 2-year period.
It is of great concern that people with serious mental illness (SMI) are in frequent contact with healthcare professionals, yet remain less likely to be offered support to stop smoking (Le Cook et al., 2014). Cigarette smoking is a leading contributor to premature death for smokers with SMI (Tam et al., 2016). While smoking rates in the general population have declined, rates for people with an SMI remain unchanged (Dickerson et al., 2018; Morgan et al., 2012). Smoking prevalence in mental health inpatient units is substantially higher than in the general population, with more than two-thirds of Australian public mental health inpatients reported to be smokers (Morgan et al., 2012). The introduction of smoking bans and smokefree policy in psychiatric services represents a significant step towards addressing health inequalities, but achieving practice change requires more than writing policy. Hospitals are considered opportune settings for initiating smoking cessation with the treatment of tobacco dependence shown to be feasible and effective in general (Freund et al., 2009) and psychiatric inpatient settings (Iyer et al., 2018; Prochaska et al., 2014; Slattery et al., 2016; Wye et al., 2010). But concerns remain regarding the number of inpatients missing out on receiving smoking care and challenges around variable staff support for policy (Campion et al., 2010; Huddlestone et al., 2018).
In 2015, Queensland public hospitals intensified efforts to implement smokefree healthcare in acute inpatient services statewide including the implementation of a Smoking Cessation Clinical Pathway (SCCP; Queensland Statewide Respiratory Clinical Network, 2017) and a Quality Improvement Payment for Hospital and Health Services. Mental health services (MHS) contributed data towards this initiative but were not well engaged. However, in January 2015, Queensland smokefree legislation prohibited smoking at all public and private Queensland hospitals and healthcare facilities. This change meant that for the first time MHS could not seek exemptions for designated smoking areas and needed to consider how to implement statewide smokefree healthcare. The Queensland Mental Health Clinical Collaborative (MHCC) was considered a method to support the embedding of smoking care into routine clinical practice with demonstrated success in statewide practice change (Plever et al., 2010, 2012, 2016). The methodology underpinning the MHCC is based on the Institute for Healthcare Improvement Model (Ovretveit et al., 2002) that has been adapted to meet the needs of Queensland MHS. Essentially, the MHCC is a statewide service improvement initiative that brings clinicians together to identify topic areas for improvement in clinical practice in adult MHS. The MHCC team develops clinical indicators utilising existing data systems and provide clinician-friendly reports to services. Clinicians are supported to share local service improvement strategies, engage in educational activities and review progress through 6-monthly statewide forums.
The following provides an analysis of the first 2 years of implementation of statewide smoking cessation, during inpatient admission, in mental health inpatient units in public MHS across Queensland. More than 50 adult acute inpatient units across Queensland, located in 16 diverse MHS governed by different Health and Hospital Services, took part. It was hypothesised that this initiative would support statewide and individual services to increase reporting of smoking status and delivery of the SCCP to identified smokers.
Method
Sixteen adult MHS with inpatient acute units engaged in service improvement initiatives to increase reporting of smoking and delivery of SCCP to identified smokers. In-scope inpatients included all patients discharged from acute MHS (extended care facilities were not included), 18 years or over, with a length of stay of two or more consecutive nights, during the reference period (October 2015–September 2017).
For every admission to the inpatient ward, clinicians were asked to determine if eligible inpatients were smokers. A smoker was defined as an inpatient who self-identified as having smoked tobacco in the past 30 days or asked for support to quit smoking. This information was recorded in the medical record. For inpatients identified as a smoker, the SCCP was completed and filed in the medical record, with a minimum number of fields required to be considered completed. The SCCP depicted in Figure 1 is an evidence-based decision support tool for clinicians to use at point of care that enables the assessment of nicotine dependence, nicotine replacement therapy (NRT) prescription and follow-up (Queensland Statewide Respiratory Clinical Network, 2017). It utilises the 5As to guide clinicians to provide consistent assessment, intervention and referral for follow-up support, to hospitalised smokers as part of routine care (Gupta and Yeung, 2016).
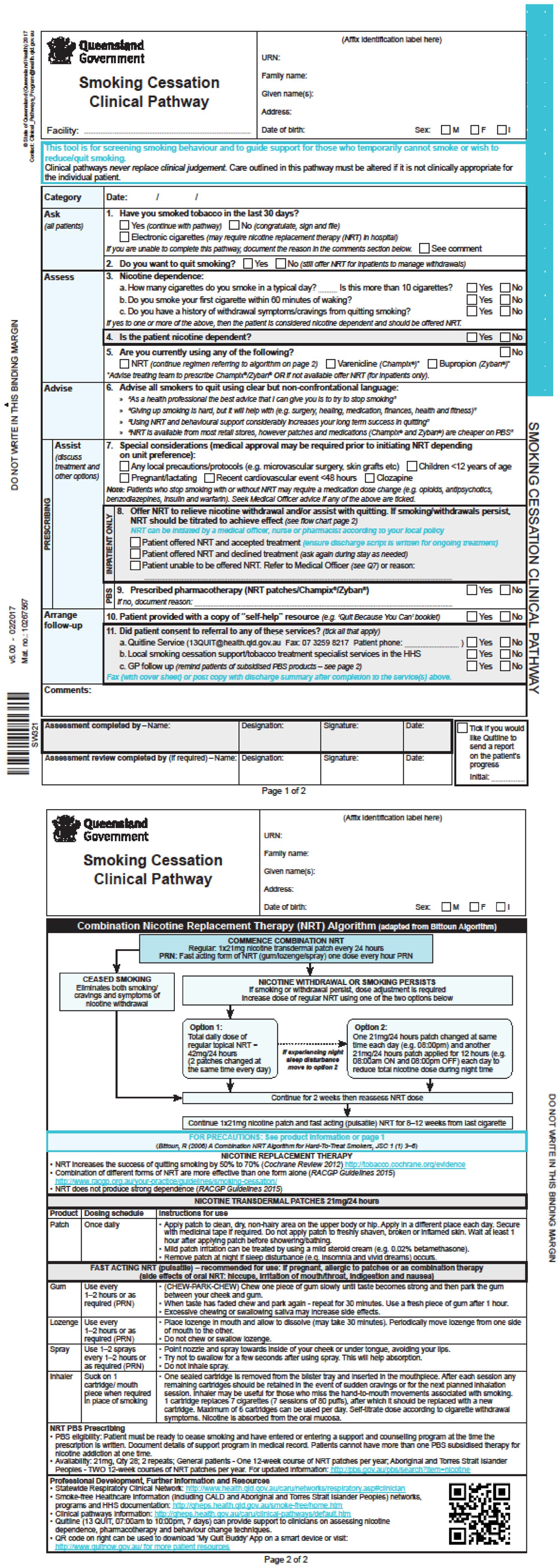
Queensland Smoking Cessation Clinical Pathway – version 5.
Hospital coders entered all information on smoking status and SCCP in the hospitals’ system for admitted patients, which was uploaded to the Queensland Health Admitted Patient Data Collection (QHAPDC), a statewide repository for inpatient data. As smoking status was asked for every admission, an individual inpatient may be counted more than once during the reference period.
The smoking status indicator was calculated as the proportion of inpatient mental health separations where an inpatient had a smoking status recorded during the reference period. The SCCP indicator was calculated as the proportion of inpatient mental health separations where identified smokers had a completed SCCP within the reference period. Services were provided monthly progress reports, opportunity for staff to attend four statewide forums focused on physical health and smoking cessation and access to MHCC staff for support on request.
Data extracted from QHAPDC were used to determine statewide percentages for each indicator and graphically depict monthly changes over time. Smoking status and SCCP indicators were derived by MHS and quarter. The score test for trend was used to assess whether there were significant trends over time in the proportion of separations in which status was recorded and the proportion of known-smoker separations for which a brief intervention (SCCP) was completed. Analyses were performed using the Stata statistical software package, version 15 (StataCorp, 2017).
Results
During the 24-month period, a total of 33,269 separations occurred across the 16 MHS with smoking status documented for 93% (31,041 separations). Of the 31,041 separations with known smoking status, 17,539 (57%) were identified as current smokers. The mean age for identified smoker separations was 37.6 years and 61% of smokers were male (Table 1). Thirteen percent of smokers identified as being Aboriginal and/or Torres Strait Islander. The most prevalent diagnosis among smokers was schizophrenia. A total of 10,495 SCCPs, comprising 60% of known-smoker separations, were completed over the 2-year period.
Demographic characteristics for consumer separations during October 2015–September 2017.
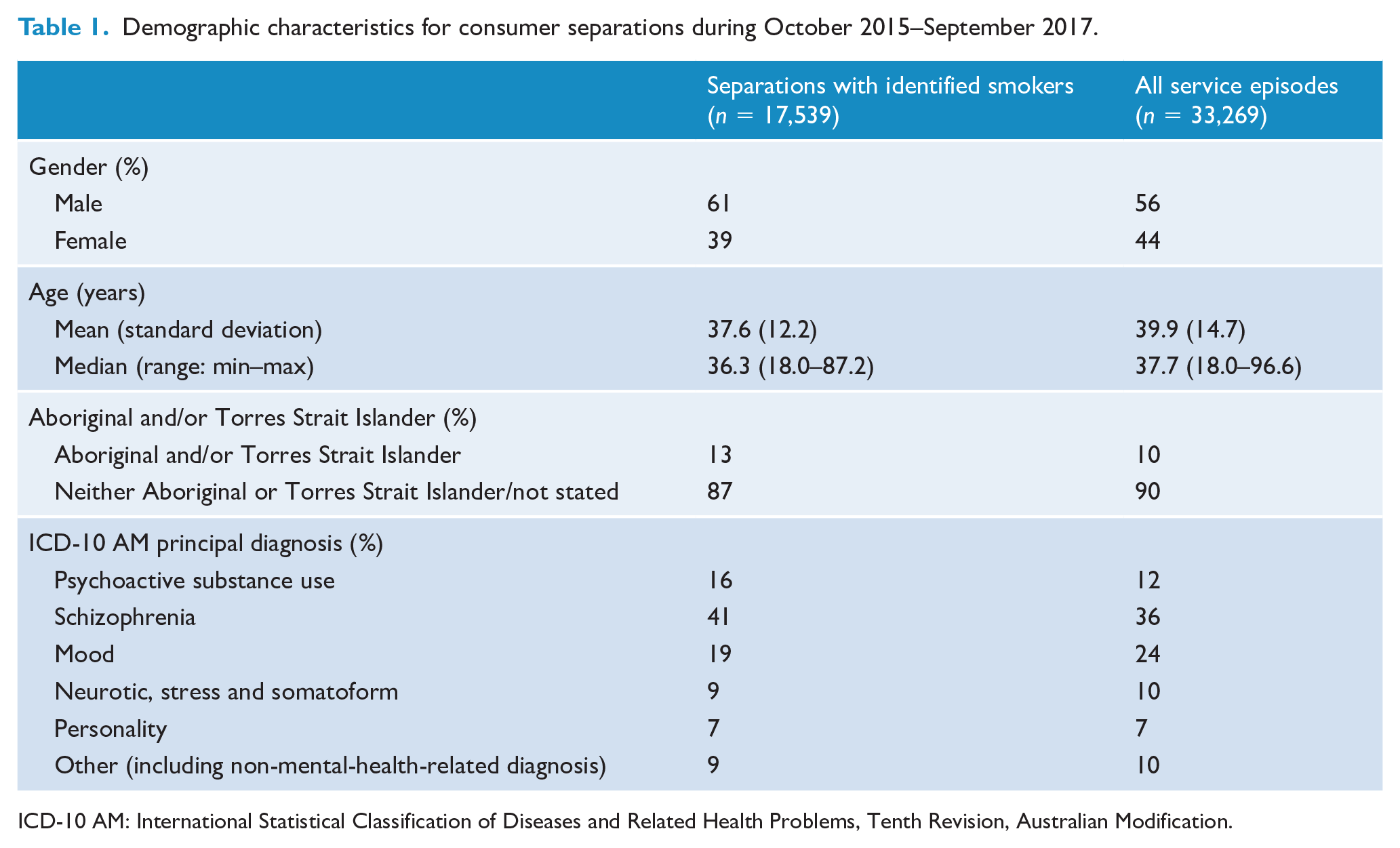
ICD-10 AM: International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification.
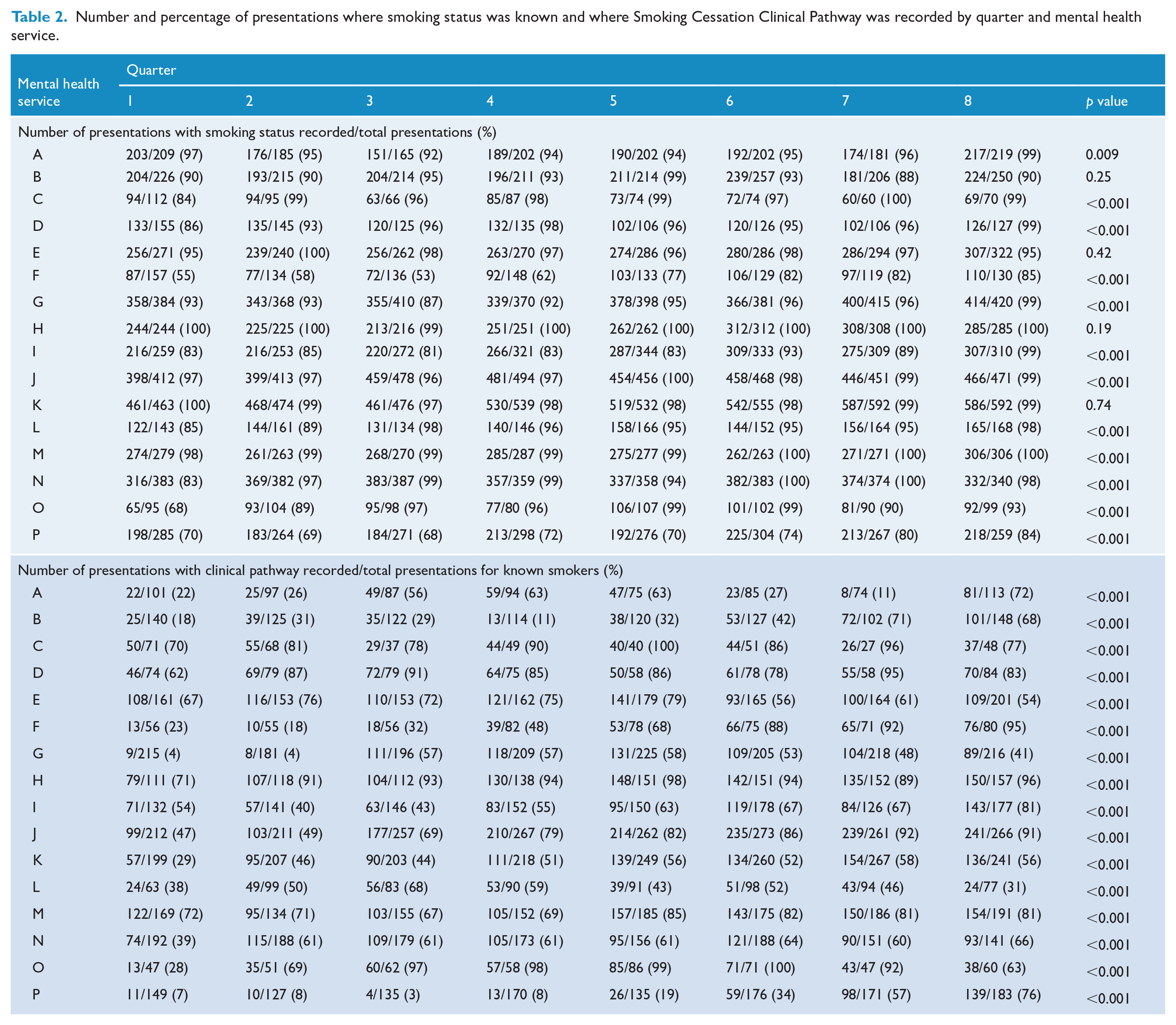
Statewide results for changes in documentation of smoking status over time and results for changes in the percentage of mental health inpatient separations for which identified smokers had an SCCP are shown graphically in Figure 2. Aggregated summary statistics for each indicator by MHS and quarter are presented in Table 2, with p values derived from score tests for trend.
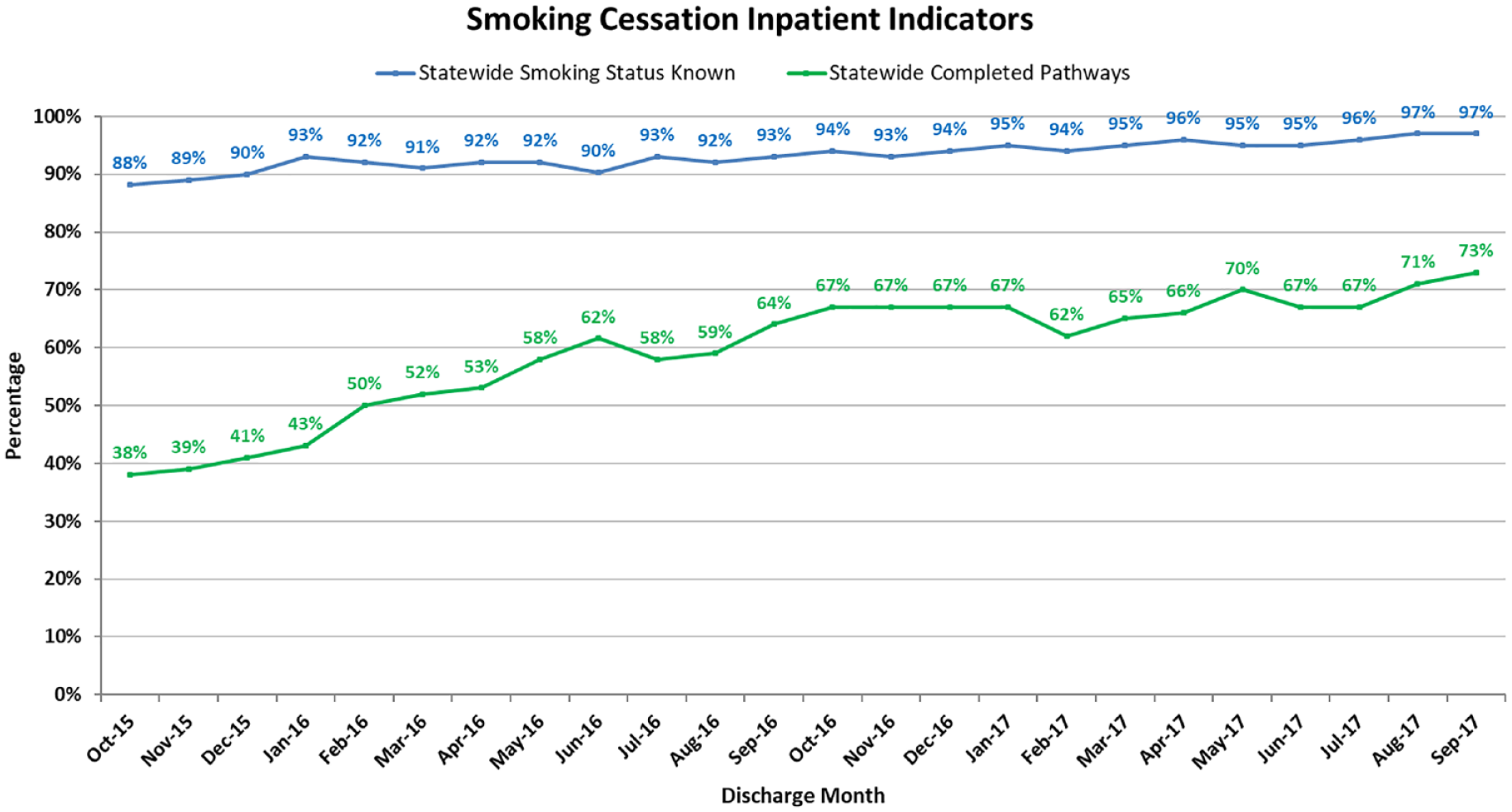
Statewide results for smoking status and completion of Smoking Cessation Clinical Pathway from October 2015 to September 2017.
Number and percentage of presentations where smoking status was known and where Smoking Cessation Clinical Pathway was recorded by quarter and mental health service.
Over the 2-year period, the statewide smoking status indicator increased from 88% in the first month to 97% in the final month (Figure 2). Within MHS, the quarterly percentage ranged from 53% to 100%. Consistent with the statewide pattern, 12 of 16 MHS exhibited a significant increasing linear trend over time in the percentage of separations with documentation of smoking status. The four remaining MHS started with very high documentation rates, which remained high throughout the 2 years, with average rates over 90%. The percentage of identified smokers per quarter per MHS ranged from 39.5% to 89%.
The overall percentage of SCCPs completed increased from 38% to 73% for separations involving a documented smoker (Figure 1). All MHS exhibited significant improvement over time. There was considerable variability within and between MHS, with percentages ranging from 3% to 100% (Table 2).
Discussion
This work supports a service improvement approach to improving the recording of smoking and the delivery of a brief smoking intervention across multiple diverse mental health inpatient services simultaneously. While individual service variability was evident, over the 2-year period all services demonstrated improvement, or maintenance of high levels, for recording smoking status and improvement in SCCP delivery to smokers. This result extends the evidence base supporting service improvement approaches to changing clinical practice in the implementation of smoking care in mental health.
The smoking rate for Queensland mental health adult inpatient acute separations across the period was 57%. Despite methodological differences, this is in keeping with reported rates for inpatient psychiatric populations (Huddlestone et al., 2018; Metse et al., 2017; Stockings et al., 2013). Accurate identification of smoking status is vital to the appropriate management of nicotine dependence in inpatient settings. Other service improvement initiatives in psychiatric settings have shown improvements in recording smoking status from 36% to 52% (Wye et al., 2017). In our data, the identification of smoking status remained consistently high and an improvement in the delivery of the SCCP was also demonstrated. While individual service variability was evident, more smoking care was provided to smokers across all services. The endurance of these improvements throughout the period implies practice change being embedded into practice.
While many staff support smoking bans and believe that they have a role in providing smoking care, apprehension around the potential for increased violence, doubts about patient ability/motivation to quit and concerns regarding competence to deliver smoking cessation interventions still exist and impede the delivery of smoking support. Literature suggests that successful drivers of smokefree policy implementation in mental health include the consistent support for policy at all levels of the organisation (Ratschen et al., 2011; Sheals et al., 2016). The MHCC approach consistently brought staff at all levels in each MHS together to focus on this issue. This initiative also attempted to address staff concerns through ongoing education, forums supportive of discussion around these concerns and provision of training opportunities. However, individual service methods of implementation of smokefree healthcare care were not controlled and differential application of smoking cessation care was likely contributing to individual service variability in performance. Despite these challenges, all services demonstrated improvement.
Researchers have highlighted the high proportion of patients who, despite implementation of evidence-based practice change strategies, still do not receive smoking cessation support (Metse et al., 2017). By the conclusion of our review period, 27% of smokers statewide did not receive the SCCP. While this is an improvement on other reported rates closer to 50% (Slattery et al., 2016; Wye et al., 2017), it still leaves an unacceptable number of smokers not being treated. Lack of systematic application, challenges in administrative burden and ongoing staff resistance to providing smoking care have been implicated in patients not receiving smoking care (Huddlestone et al., 2018; Koplan et al., 2008; Metse et al., 2018; Wye et al., 2017). The current initiative used an existing hospital clinical pathway to minimise additional administrative effort but also support staff with varying capability levels. Despite the brevity of the pathway, anecdotal reports suggested that even this was considered burdensome for some clinical staff. Future efforts to improve service systems and reduce administrative burden may help reduce this practice gap and better support clinicians to provide smoking care.
The results achieved here are encouraging and suggest that a service-improvement-based model can be effective in achieving clinical practice change for smoking cessation in multiple inpatient MHS located in different hospitals simultaneously. Interpretation of the results should be conducted with consideration to limitations including potential confounding influence of sex, age and diagnosis to these results and to the real-world implementation necessary for the initiative to have occurred. To achieve widespread reach and rapid implementation, local practices were accommodated. This meant that smoking cessation delivery, staff training, information and support were variable from site to site. This limits the identification of components that may be of more importance to delivery of smoking care. Another consideration is that the improvement has occurred during a time of heightened focus for smoking. As service priorities change, challenges to sustaining results will emerge. To mitigate this, the Queensland Mental Health Alcohol and Other Drugs Branch has incorporated these smoking clinical indicators into statewide Key Performance Indicators for MHS. This strategy has proved successful in sustaining improvements in other clinical practice change interventions supported by the MHCC (Plever et al., 2012). This review did not examine the impact of the Quality Improvement Payment to MHS results. While MHS contributed to hospital-wide data for the Quality Improvement Payment, MHS engagement with the scheme was nominal. Finally, while the focus of this review was on clinical practice change, the real question is whether this translated to supporting smokers to cut down, quit or attempt to quit. The implementation of a systematic process for recording smoking cessation support in Queensland inpatient acute MHS will enable us to begin tracking these outcomes. Building on the success of this initiative, we are now extending this approach to Queensland Health community MHS to strengthen smoking cessation across the continuum of care.
Footnotes
Acknowledgements
The authors would like to acknowledge the work of individual mental health services and clinicians that have participated in this initiative and the Queensland Health Respiratory Clinical Network for development of the Smoking Cessation Clinical Pathway.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.