
Abstract
Objective:
To determine the efficacy, safety and acceptability as well as the patient demographics of three newly developed emergency department–embedded Psychiatric Assessment and Planning Units located in Metropolitan Melbourne at Austin, Peninsula and Eastern Health Services.
Methods:
The evaluation reviewed a 12-month period of service activity from 1 September 2017 to 31 August 2018, when all three Psychiatric Assessment and Planning Units services were operational. A 12-month period from 1 September 2014 to 31 August 2015 was compared as the pre-Psychiatric Assessment and Planning Units period. Mixed qualitative and quantitative methods were used. This included semi-structured interviews of 30 Psychiatric Assessment and Planning Units patients and 30 emergency department staff (10 of each for all 3 sites), patient survey, statistical analysis of Client Management Interface data for the emergency department and related Psychiatric Assessment and Planning Units as well as audit of RISKMAN registers.
Results:
There were 365 Austin, 567 Eastern and 791 Peninsula Psychiatric Assessment and Planning Units admissions. Psychiatric Assessment and Planning Units were generally well accepted by patients and emergency department staff, relatively safe, operating within the Key Performance Indicators with mixed effect on emergency department flow. Austin emergency department processing times improved post-Psychiatric Assessment and Planning Units (4 hours 57 minutes to 4 hours 19 minutes; p < 0.001) while deteriorating at Eastern and Peninsula. Adjustment Disorder and Depression and Borderline Personality Disorder were the most common admission diagnoses. While the Psychiatric Assessment and Planning Units had mixed utility on emergency department processing times, they appear to serve a demographic not previously accommodated in traditional emergency department psychiatry models.
Conclusion:
The emergency department–embedded Psychiatric Assessment and Planning Unit model of care appears effective on some measures, safe and acceptable to patients and staff. The Psychiatric Assessment and Planning Units seem to service a group not previously accommodated in traditional emergency psychiatry models.
Keywords
Introduction
Mental health patients make up a significant proportion of emergency department (ED) presentations, endure on average longer stays in ED and represent a large allocation of health resources (Australasian College for Emergency Medicine, 2018; Barratt et al., 2016; Weiss and et al, 2016). Psychiatric Short Stay Units have been part of the redesign of many hospitals to help deal with this (Birmingham and Solihull Mental Health, 2017; Brakoulias et al., 2010; Johns Hopkins Medicine, 2017; NSW Health, 2015; Seymour et al., 2018). Psychiatric Assessment and Planning Units (PAPUs) are another version of this care model. They aim to assess and manage patients in acute crisis. There are other PAPUs in Australia, generally located in either Inpatient Psychiatric Units or ED (Victorian Department of Health, 2013). In ED, they have direct utility to the emergency setting, potentially offering a differentiated specialist model of care, improved system efficiency, reduced ED mental health wait times and overall improved quality of care for patients presenting in crisis.
The policy framework for the PAPUs (Victorian Department of Health, 2013), aims they provide timely short-term inpatient care (less than 72 hours), reduce the demands on ED by actively seeking patients from the ED and be adult focus with allowance for potentially more vulnerable people aged 16–18 years and those over 65 years if appropriate.
There are three new PAPU services in Melbourne that are within close proximity of their services ED: Austin Health, Eastern Health and Peninsula Health. Each service comprises 4–6 beds and aims to provide recovery-orientated, person-centred care (Victorian Department of Health, 2013). Interventions include comprehensive psychiatric assessment, medication, brief psychological support such as psychoeducation and safety planning, access to carer, consumer and family support, social worker input and liaison with community linkages. The model of co-locating PAPUs in an emergency environment has given us scope to reflect on this arrangement and consider their efficacy, safety and acceptability as well as determine their patient population defined by demographics and diagnostic related groups (DRGs). Analysing the performance of the PAPUs in their first few months of operation is essential to understanding their utility and to progressing the model.
Objectives
The study included four key objectives: (1) An evaluation of the experience of PAPU consumers and staff associated with the PAPU. (2) A review of service safety. (3) An analysis of the patient demographics, the performance for each PAPU measured by Key Performance Indicators (KPIs) and the impact of the PAPUs on the consumer waiting times in ED including a comparison of ED performance pre- and post-PAPU. (4) A review of the clinical diagnoses of those using the PAPUs.
Material and methods
Study design
To achieve objective 1, semi-structured interviews were completed on 30 PAPU patients and 30 ED staff (10 of each from all sites, total 60). Quota sampling was used. The interviewer visited each site on a 3-week rotation. Patients were randomly selected on the day for interviewing. Patients completed a consent for review. If the patient refused, another patient was approached. This process continued until the quota was achieved. The same process was applied to ED staff with the interviewer visiting each site on a 3-week rotation until completion. For consistency, there was one interviewer who was a social work student, specialising in mental health. The interviewer completed six practice interviews with a qualified psychiatrist, so interview techniques such as rapport building, openness and empathetic listening were mastered. These interviews aimed to discern the experience and attitudes of the patients and staff towards the PAPU. Interview transcripts were reviewed using thematic inductive analysis by two independent analysts. The process included familiarisation with data, generation of initial codes and interpretation into overriding common themes. In addition, we reviewed identical patient surveys distributed to each PAPU.
To achieve objective 2, there was a retrospective review of the RISKMAN data base for each site. This register logs incidents concerning safety breaches.
To achieve objective 3, a retrospective study of the PAPU patients was completed, using the Client Management Interface (CMI) data base for each PAPU and associated ED. We reviewed the patient’s demographics, including age, sex as well as leading diagnoses. We analysed the functioning of the PAPU as per KPIs, including length of stay, bed occupancy and readmissions. The percentage of mental health ED presentations transferring to PAPU and a comparison of wait times for mental health presentations in ED pre- and post-PAPU were analysed. This was to understand the PAPUs effect on ED bed flow.
To achieve objective 4, we retrospectively analysed the CMI data to establish in addition to demographics the primary presenting diagnoses for PAPU patients.
Time frames
Data at each service were collected from 1 September 2017 to 31 August 2018. In this 12 months, all three PAPUs were operational. For ED waiting times, we compared these data with 1 September 2014 to 31 August 2015, a period where no services had PAPUs. Semi-structured interviews of PAPU consumers and ED staff were conducted between 1 May 2018 and 1 September 2018.
Subjects
Subjects interviewed were either inpatients or ED staff associated with the PAPUs. The PAPUs inclusion criteria were 18–65 years of age with scope to admit outside this age range. Patients required an acute mental health issue to be able to be treated safely in the PAPU and likely to improve within 72 hours. To consent to the semi-structured interviews, PAPU patients needed to be over 18 years. Patients aged younger than 18 years were excluded. Semi-structured interview of ED staff required individuals employed in work associated with the ED. This included any ED Health profession.
Statistics
Results were analysed using Microsoft Excel 2010. Comparisons in mean were analysed with T-tests and proportions with Chi-square tests. Continuous data were expressed with means, standard deviation (SD) and 95% confidence intervals. Categorical data were expressed as a proportion or percentage.
Power calculations and sample size were calculated for the comparison of ED processing times: Mean Length of Stay in ED (before and after PAPU). In order to power the study at 80%, we required 1006 ED patients in the pre-PAPU sample and 1006 ED patients in the post-PAPU sample (total of 2012). Sample estimations were calculated using SampleSize (version 1.1.3; Computer Software, Sheffield, UK) by epiGenesys (2012), calculating for superiority between the two samples and assuming normal distribution.
Results
Objective 1-PAPU consumer and ED staff experience of PAPU
PAPU consumers
A total of 30 semi-structured interviews were completed (10 at each site); 21 interviewees were females (70%) and mean age was 35.3 years. All interviewees were PAPU inpatients. Following thematic analysis of the data, several concepts emerged with both reviewers in agreement of these themes.
An idea of sanctuary
PAPU was perceived as respite or a sanctuary from the busy ED or adult psychiatric units. Many interviewees had previous admissions to either child or adult psychiatric units. Their PAPU admission was viewed as comparatively favourable. This was for a variety of reasons that included the perception of PAPU as a relatively quieter environment, the mix of seemingly less aggressive co-patients and feeling safer in a small contained environment.
A feeling of staff being caring and receptive
Across all three sites, patients consistently commented that staff were kind and caring with many expressing being respected. Responses that related to this included staff being accessible, the large amount of time spent by staff engaging with patients as well as feeling comfortable approaching staff about their needs and having those needs met.
In addition, all those interviewed had seen a psychiatrist and nurse with additional services such as social work, drug and alcohol counsellors, dietician and other allied supports.
In all, 99 patient surveys were collected. The majority were from Austin Health whom had designed the survey and were possibly more proactive in promoting this (66 from Austin Health, 22 from Peninsula Health and 11 from Eastern Health; see Table 1). The majority of completed surveys rated the services as excellent in most domains. Freeform comments provided by PAPU patients highlighted consumers expressing that staff were caring and approachable and feeling respected.
Collated patient feedback surveys (N [%]).
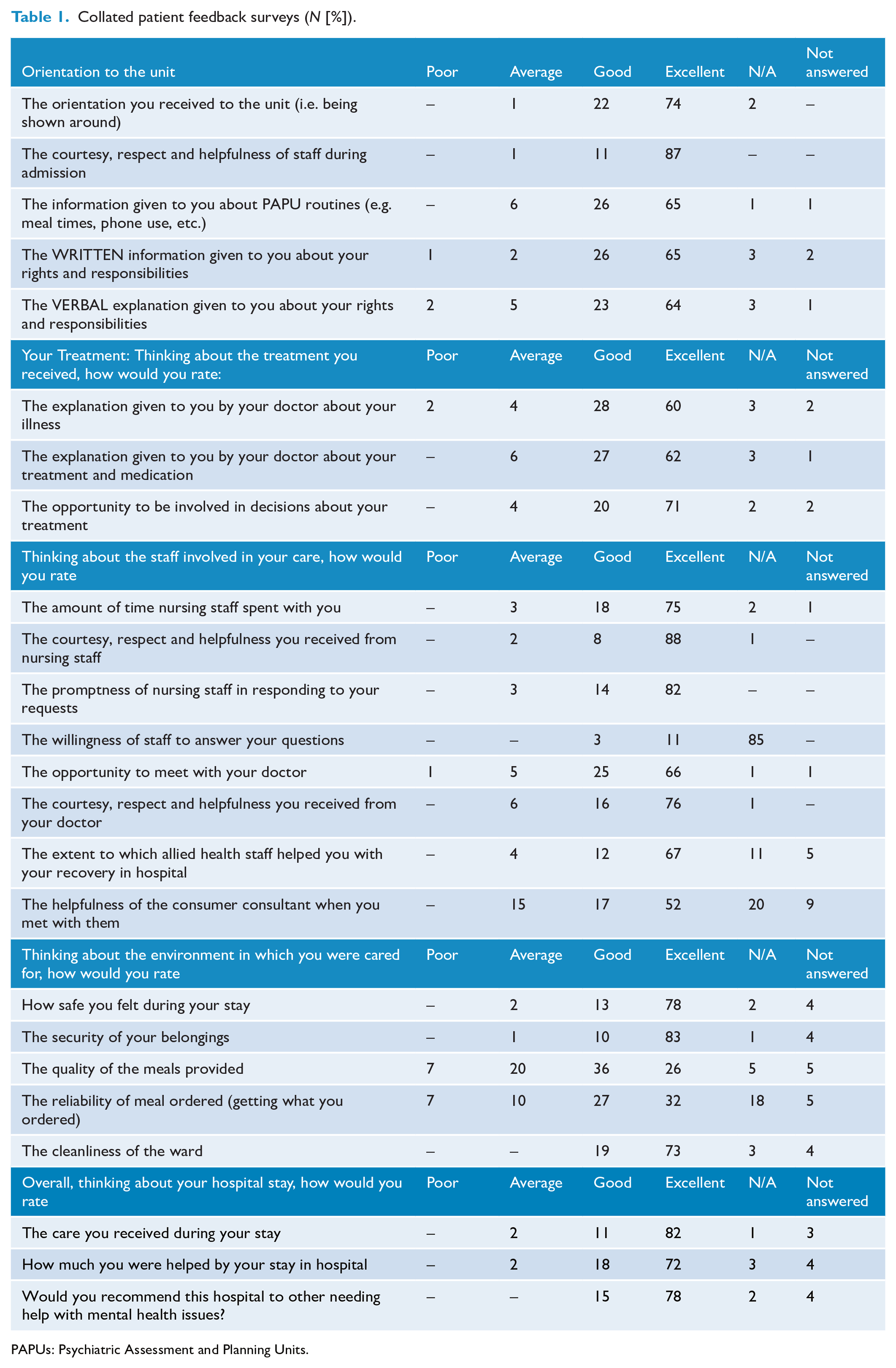
PAPUs: Psychiatric Assessment and Planning Units.
ED staff
A total of 30 semi-structured interviews were completed with ED staff (10 occurring at each site). Interviewees included 20 nurses, 6 Emergency Consultants, 2 Emergency Psychiatric Service Clinicians and 1 Ward Clerk. These themes emerged.
Positive experience of PAPU linked to familiarity
PAPU was viewed as positive when the staff member was familiar with the service and had multiple experiences of dealing with the PAPUs. Staff whom responded positively described feeling assisted by PAPU with mental health patients in ED and patients not having to stay in ED as long. Conversely, those that were not familiar with PAPU were more likely to be either negative in their response or were not confident to comment.
PAPU being selective about patient admissions
Another theme was of PAPU being selective in regards to patient admissions. Some staff reflected that because PAPU was not admitting certain high-risk or aggressive patients, these patients typically remained in ED with bed flow and management issues unresolved.
Objective 2 safety
All three PAPU sites were relatively safe with no major incidents occurring in the 12-month period studied.
Objective 3 PAPU consumer demographics, KPIs and effect on ED
In the 12-month period from 1 September 2017 to 31 August 2018, there was total of 1723 PAPU admissions for all three services. Table 2 summarises the services’ consumer demographics, readmission rates and ED flow. Due to differences in service characteristics, it is generally more valid to review the services individually. However, the three services demonstrated a similar mean age (approximately 36 years old). This was despite the broad age group being 18–65 years with the capacity to admit those aged 16–18 and over 65 years. The services also had similar sex distributions (approximately 60% female, 40% male and <1% identifying as neither male or female) and bed occupancy rates (>74%).
Summary of key findings for objective 3 (1 September 2017 to 31 August 2018).
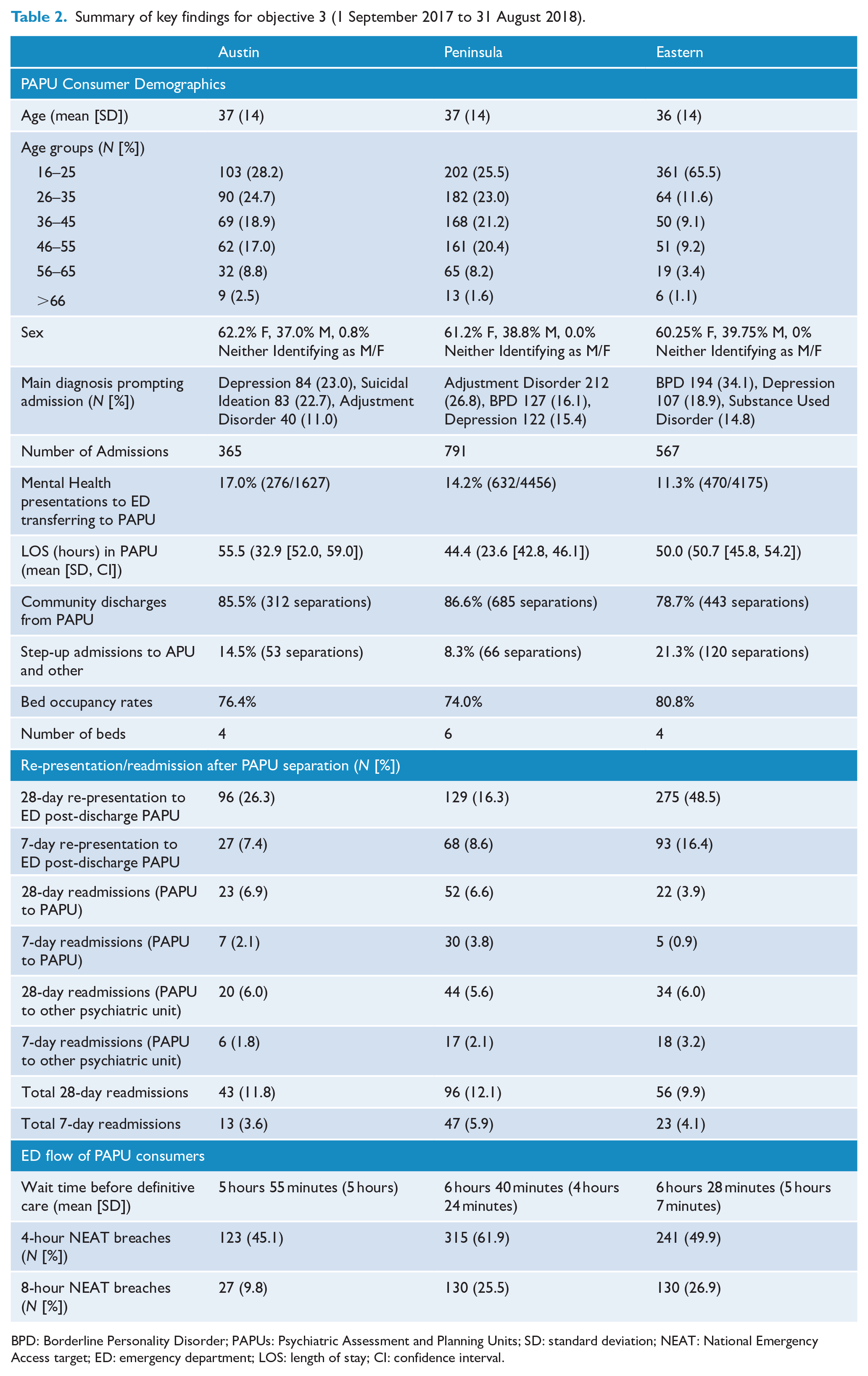
BPD: Borderline Personality Disorder; PAPUs: Psychiatric Assessment and Planning Units; SD: standard deviation; NEAT: National Emergency Access target; ED: emergency department; LOS: length of stay; CI: confidence interval.
Austin Health PAPU had the lowest total admissions. This was concurrent with total ED mental health presentations for each service, with Austin having substantially fewer mental health presentations, compared to Peninsula and Eastern. This possibly allowed Austin Health to accept a higher proportion of their ED mental health presentation into their PAPU as well as have a longer admission length.
The proportion of patients who were unable to be discharged directly from PAPU and required a ‘step-up’ to an Adult Inpatient Unit, Adolescent Inpatient Unit or equivalent differed between the PAPUs. Furthermore, this variance did not correlate with the total number of admissions or ‘bed-pressures’. Peninsula had the lowest number of step-up admissions followed by Austin and Eastern. Overwhelmingly, patients were managed within PAPU and discharge into community care.
The functioning of the PAPUs with ED and readmission rates also varied between the services. Re-presentations to EDs after discharge from PAPU must be contextualised. A single patient may represent to an ED multiple times, thus inflating the re-presentation for that service. This partially explains the significant number of ED re-presentations from Eastern PAPU. ED re-presentation figures at the other two services were superior. In contrast, Eastern PAPU had the lowest proportion of PAPU to PAPU readmissions, followed by Austin and then Peninsula. Readmissions from PAPU to other psychiatric units overall were similar.
The average wait time in ED prior to PAPU breached the National Emergency Access target (NEAT) of 4 hours in all services. Austin Health had the shortest average times to PAPU admission, followed by Peninsula and finally Eastern Health. For proportion of NEAT breaches, Austin was most favourable followed by Eastern and Peninsula Health.
A comparison of ED wait times of mental health consumers is summarised in Table 3. Between the two 12-month periods of the 1 September 2014 to 31 August 2015 and the 1 September 2017 to 31 August 2018, all services had an increase in mental health–related ED presentations. Austin in particular experienced a significant increase in presentations. Despite this increase, Austin Health was the only service that had a statistically significant decrease in wait time and NEAT breaches, with the other services demonstrating significant increases in these statistics (p < 0.05). The increase in ED presentations appeared to have a variable effect on proportion of ED mental health–related presentations being admitted. Austin demonstrated no significant difference in proportion admitted and Eastern saw a significant decrease, whereas Peninsula saw a large increase in proportion admitted, leading to this being reflected in the combined admission rate.
ED flow of mental health consumers pre- and post-implementation of PAPU (χ2 test for % and T-test for means significance).
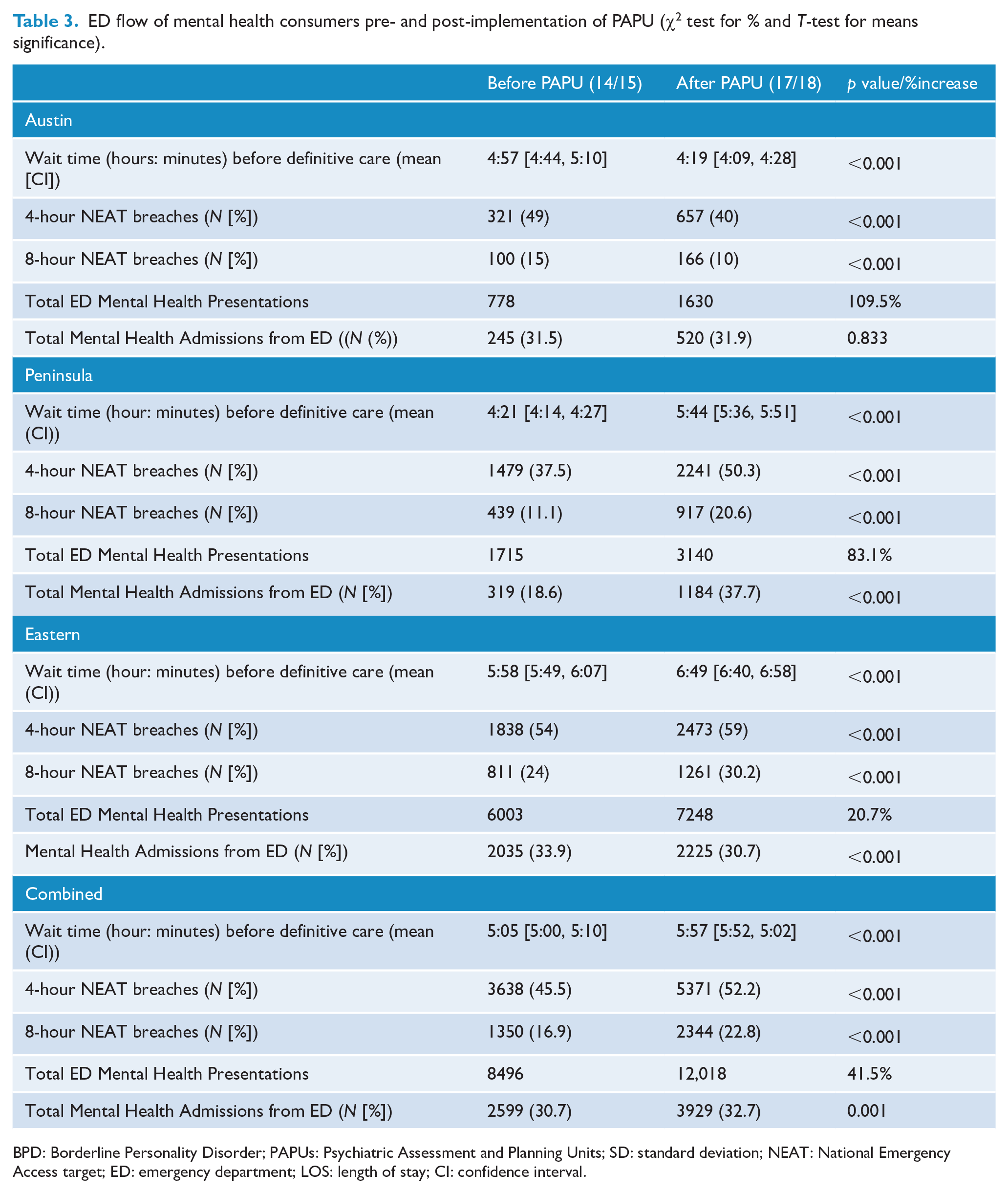
BPD: Borderline Personality Disorder; PAPUs: Psychiatric Assessment and Planning Units; SD: standard deviation; NEAT: National Emergency Access target; ED: emergency department; LOS: length of stay; CI: confidence interval.
Objective 4 diagnoses
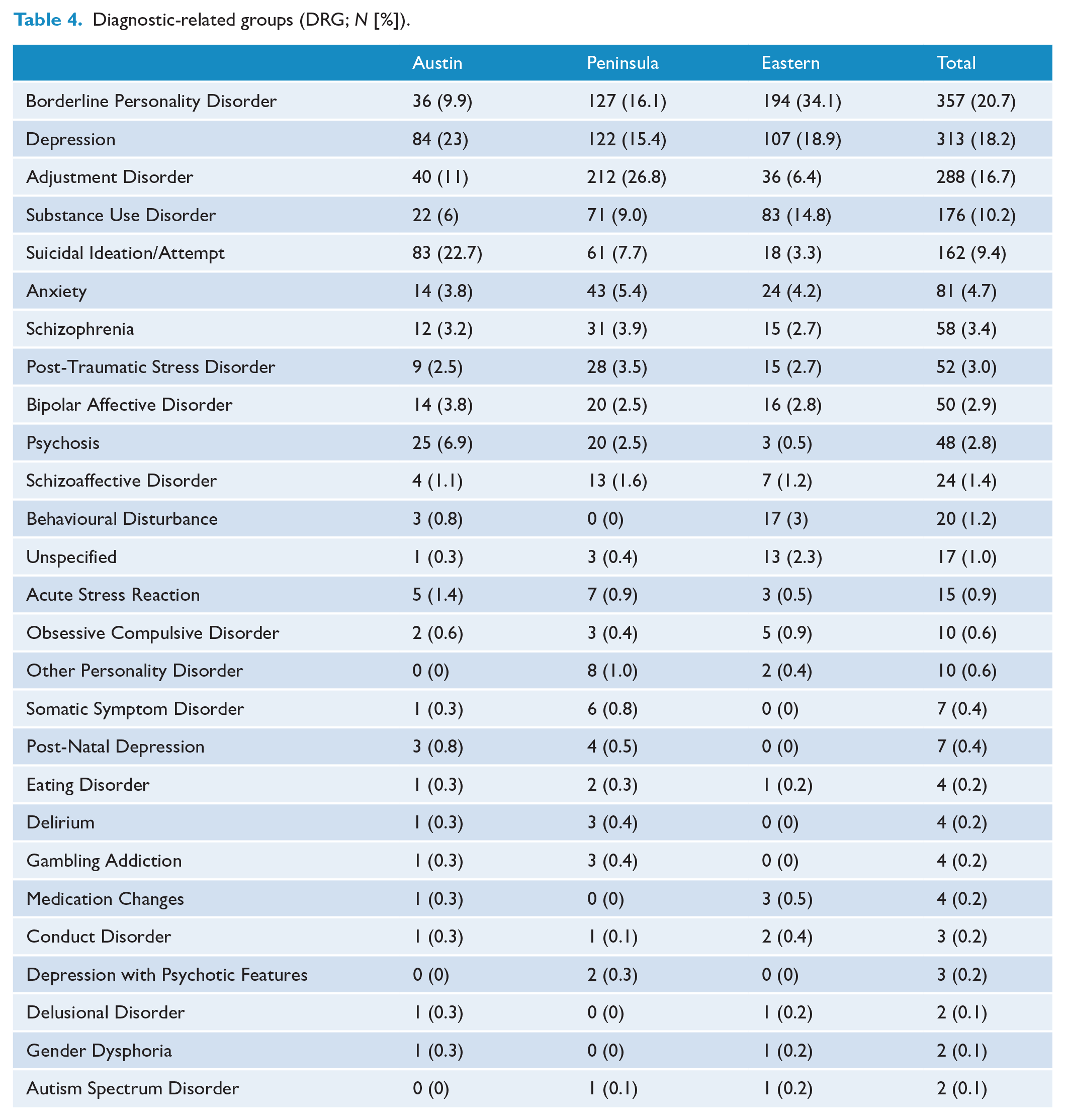
The DRG utilising PAPU are summarised in Table 4, with Figure 1 demonstrating the proportions of the main admission diagnoses. Collectively, the most common admission diagnosis was Borderline Personality Disorder, Depression, Adjustment Disorder, Substance Use Disorder and Suicidal Ideation/Attempt.
Diagnostic-related groups (DRG; N [%]).
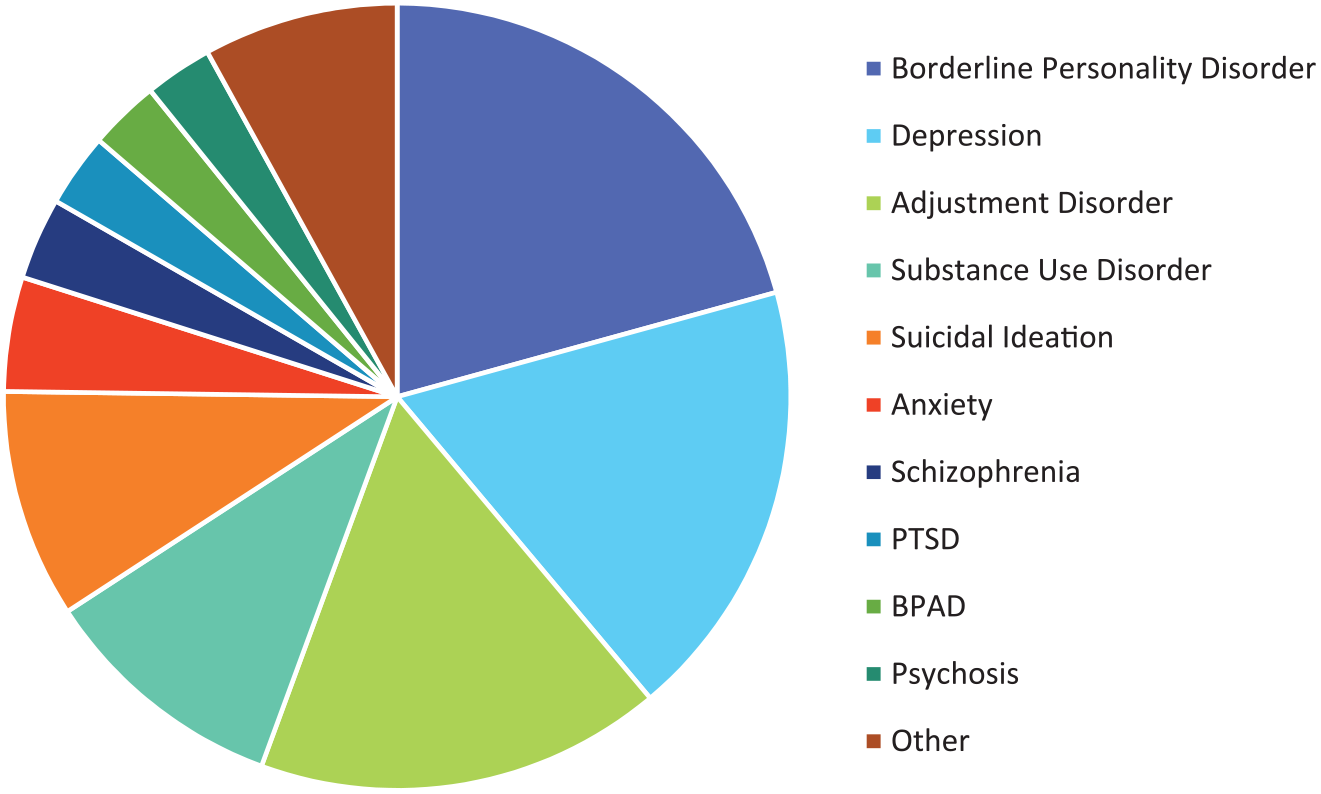
Main diagnosis and issues prompting admission proportionally.
Discussions
If Emergency Psychiatry is a burgeoning sub-specialty (Cammell, 2017), ED-embedded PAPUs can become an integral part of this. Thus, an imperative to evaluate them. While there is literature pertaining to the efficacy of medical short stay units (Damiani and et al, 2011; Juan and et al, 2006) and similar short stay psychiatric units (Brakoulias et al., 2010; Frank et al., 2005; Seymour et al., 2018), there is little on PAPUs.
The evaluation provided several insights. First, the ED-embedded PAPU model of care appeared well accepted by consumers. For many individuals, it was preferable to other inpatient models. Feedback from consumers at all sites, via semi-structured interviews and consumer surveys, was overwhelmingly positive. Feedback from ED staff was mixed. The main issue for ED staff was a lack of understanding of the PAPU model or inability to relate how the service impacted upon the ED. There is clearly scope for improved communication between psychiatry and EDs. Conversely, it is worth considering that the separation of mental health and physical health within an ED is a privileged position in which many metropolitan Melbourne services now operate. Hence, psychiatry presentations to the ED are often triaged and referred directly to Emergency Psychiatry Services without significant input from ED staff. In such a paradigm, ED staff may not have much interaction with psychiatry presentations or mental health services like PAPU. Regardless, the concerns that PAPUs were not receiving the more aggressive patients warrant reflection. This is partially addressed through the introduction of Behavioural Assessment Rooms (BAR; Victorian Department of Health, 2017a) where potentially aggressive patients can be assessed, managed and harm mitigated in collaboration between the ED and Emergency Psychiatry Services.
Safety in any hospital setting is paramount (Victorian Department of Health, 2013, 2016, 2017b). The PAPU model appeared to be safe for both consumers using the service and staff. In all three sites, no serious harm came to inpatients, staff or persons in proximity of the PAPU. While a favourable outcome, this can be somewhat attributed to risk screening and patient selection which mitigates risk. The disadvantage being that the PAPUs might lack utility to manage more aggressive or disturbed consumers that ED are often keen to expedite from the department.
In terms of the effect of the PAPUs on ED, the results of each PAPU varied slightly. The Austin PAPU had a discernible decrease in ED wait times post-PAPU that was statistically significant on all measures. Mean time in ED for mental health contact reduced by 38 minutes. Also, the breaches of the 4- and 8-hour targets in ED for mental health contacts were both reduced (4-hour breaches: 49–40% and 8-hour breaches: 15–10%) post-PAPU. This was not the case at Eastern Health or Peninsula, where ED wait times increased in the same period. The mixed results not only create further scope for enquiry but demonstrate the complexities of objectively discerning a services effect on dynamic systems issues such as ED flow. The policy frame work for PAPUs (Victorian Department of Health, 2013) aims to provide short timely care, reduce the demands on ED and be adult focussed with the scope to care for those patients who aged above 18–65 years. PAPUs appear to be meeting these aims with the exception of ED flow. In some regards, the current model has conflicting aims. Supporting seemingly more vulnerable demographics, like those younger and older clients, may limit the PAPUs ability to handle higher risk aggressive patients. If this is the case, there needs to be policy considerations to change the PAPU model or adapt support systems, such as the BAR, to improve patient flow. Otherwise, policy must adopt PAPUs other utilities and accept their limitations.
Each PAPU site functioned within the parameters of many KPIs. Of note, 28-day readmissions to any mental health service at each site were less than 14%, the state-wide target (Victorian State Government, 2018). Given PAPUs’ focus on community linkages post discharge, this was a positive finding.
Finally, the demographics and Diagnostic-Related Groups (DRG) utilising PAPU tell us much about the model. Generally speaking, PAPU consumers were young (mean ages: Austin 37 years, Peninsula 36 years and Maroondah 36 years) and proportionally more likely to be female. One could speculate that the perception of PAPU as a safe and contained environment lends itself to groups perceived as more vulnerable selected for admission.
Overall, the PAPU services appeared to be definitively general adult services. The PAPUs managed a wide range of psychiatric illnesses. In an age of medicine where the prevailing paradigm can be silos of sub-specialisation, the diversity of presentations the PAPU services provides is distinguishing.
In terms of main DRGs, the differences between the services can be partially accounted by whether the service preferences a symptom-based or diagnostic approach. For example, Austin Health PAPU had a smaller proportion classified as Borderline Personality Disorder compared to Eastern Health, but had a higher proportion of a common presenting symptom of patients with Borderline Personality Disorder (Suicidal Ideation). The main DRG variation between services was Substance Use Disorders. This was the third most common presentation to Eastern (14.8%), but was not in the main DRG of the other services. This likely reflected Eastern Health’s policy of co-managing medical complications like alcohol detoxification in PAPU. This would be managed in the Short Stay Units in the other services.
Otherwise, all serviced a similar spectrum of mental health presentations. Borderline Personality Disorder and Depression were the leading admissions, diagnoses and highlight areas where the services need to be skilled, but the third most common complaint was adjustment disorders. PAPU represented an intermediate option for patients with less severe illness. In these situations, admission to an adult inpatient unit was probably inappropriate, and prior to PAPU, there was no equivalent option. The admission of these presentations to PAPU highlights that within our public mental health services, there is a need to service such presentations, just as there is a need for the provision of care to higher acuity mental health illness.
Limitations
There are limitations to the scope of this evaluation project. Any evaluation that is conducted over multiple sites and uses multiple methods of data gathering (both qualitative and quantitative) leads to complexity and in turn distorts results.
While we have tried to discern a general utility from the three ED Embedded PAPU sites at Austin, Peninsula and Eastern Health, we are faced with issues trying to deduce an overall result from three PAPUs attached to three independent health services, each with their own directorship and cultures.
In analysing the changes to the ED pre- and post-PAPU, because of the lag between each site opening (Eastern PAPU in May 2016, Austin in February 2017 and Peninsula in June 2017), we were compelled to review a period of time prior to all three PAPU operating and a time period in which all three sites were operational. Hence, our decision is to review with mirror methodology the pre-PAPU period 1 September 2014 to 31 August 2015 and the post-PAPU period 1 September 2017 to 31 August 2018. While this has facilitated the allowance of all three services having a simultaneous period of review, it has also meant we have not reviewed a period that is immediately pre- and post-PAPU for each site. We therefore cannot rule out that the gap between the 14/15 and 17/18 periods included any number of changes that may have equally influenced the ED environment and that were separate confounding influences. Why ED presentations increased in these three sites at a slightly higher rate than the state average could be influenced by many factors that are beyond the scope of this paper and yet may have exerted a profound influence.
This evaluation has been the study of a complex health system in the process of continuous operation. There may be a myriad of factors beyond PAPU that influenced the ED flow and indeed the PAPU and associated mental health services. We cannot say for certain that any improvement or regression in ED wait times was completely or directly attributable to the associated PAPU, when the true influence may have been a change in governance, better ED liaison or changes in service demand over time.
Also, reviewing a host of objectives with multiple methods, both benefitted and hindered. Arguably, we benefit from a range of tools to evaluate the services but are hindered by an inability to truly integrate our multiple results.
The challenges of reviewing three sites, with varying degrees of understanding of each site and variations in the level of cooperation, effects the prism through which we viewed the results. The proportion of completed patient surveys at each site is an example of this variation. Similarly, the difference in diagnostic categorisation between the services reflected practice variability. To better understand the diagnostic variations between sites, we could have analysed the case notes of each admission to better authenticate the diagnoses.
Conclusion
The ED-embedded PAPUs appear effective, safe and acceptable to their patients and the ED staff. The services included proportionally more females and younger persons. The main diagnoses included mood, adjustment and borderline personality disorder. The ED-embedded PAPUs are not designed to manage patients who are with extreme behavioural disturbances or who are at high risk. This probably limits their ability to contribute to traditional patient flow. It, however, adds additional resources for a previously under serviced clinical group of lower severity illness. Further research into PAPUs’ effect on ED is warranted. Policy needs to consider the PAPU models’ benefit and limitations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.