
Abstract
Irritable mood is a seemingly common symptom that features prominently in several the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) psychiatric diagnoses (Toohey and DiGiuseppe, 2017). It is sometimes used interchangeably with irritability, but such imprecision, apart from lacking accuracy, is simply unhelpful. In DSM-5, irritable mood is qualified as ‘often the predominant mood is irritable’, and this elaboration provides a clue to its conceptualisation (Malhi et al., 2019a). The insinuation is that irritable mood is principally a ‘mood’, but that it has an ‘irritable expression’ (see Figure 1(a)). And so, DSM essentially considers irritable mood to be a ‘manifestation’ of mood. In other words – it is a kind of mood, notwithstanding the fact that clinically and experientially irritable mood is often quite different to mood without irritability. However, if irritable mood is conceptualised as a facet of mood, then it remains a type of mood regardless of how it appears. It is important to note that assigning primacy to mood does not exclude the role of other factors such as anxiety and personality that can contribute to irritability – it simply emphasises the core nature of irritable mood as having emanated from mood itself.
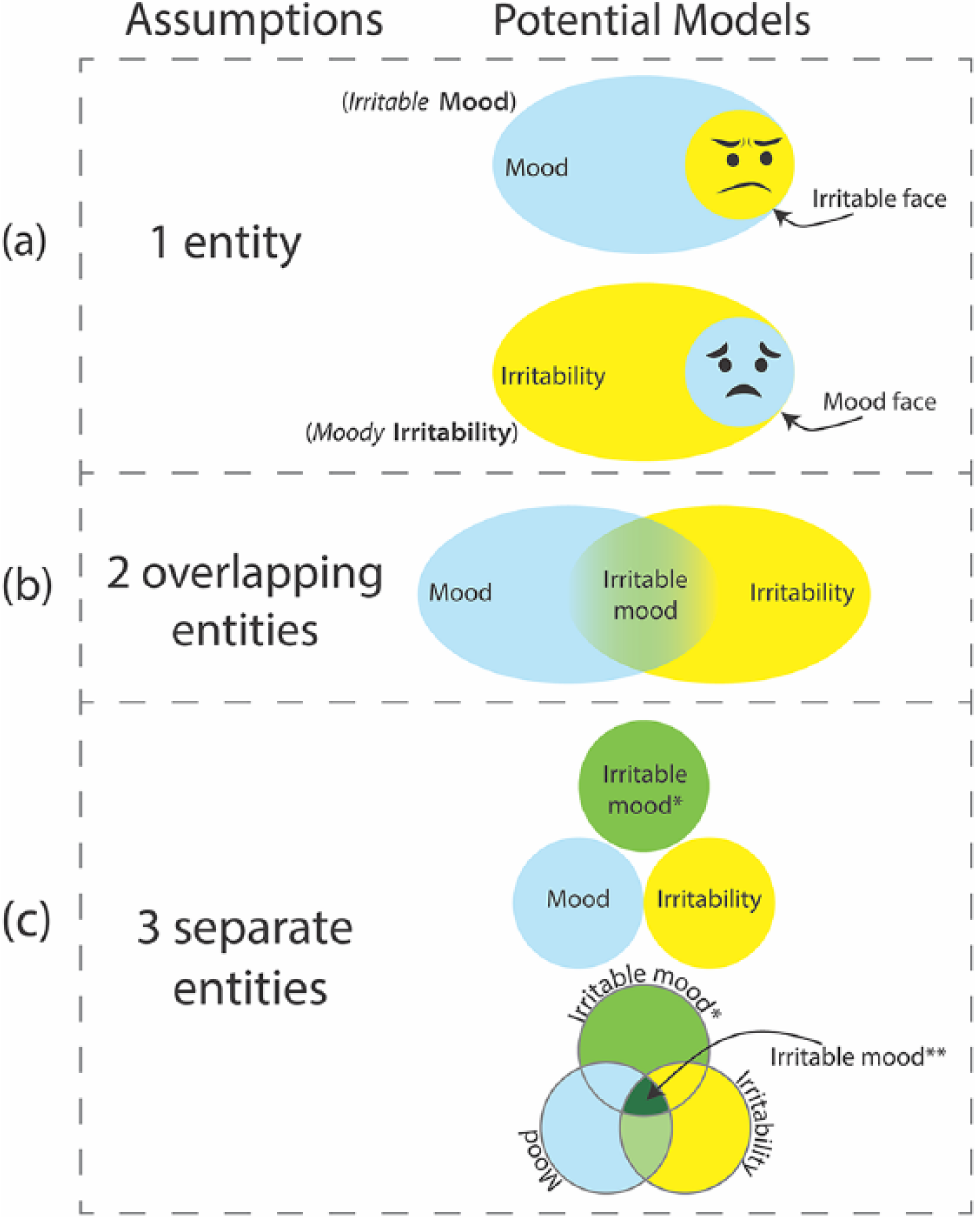
Schematic outlining of conceptual assumptions and corresponding possible models for irritable mood. (a) The first assumption is that irritable mood is a single entity, either mood or irritability, and that it manifests with either an irritable or moody ‘face’. (b) The second possibility is that irritable mood is an admixture that arises as a consequence of two (purer) entities, namely mood and irritability, overlapping in certain circumstances, and it is this overlap that produces irritable mood. (c) The third assumption is that irritable mood is a separate entity unto itself and that it is distinct from irritability and mood (*). However, these three entities may still overlap at times – creating a more pronounced irritable mood (**).
Understanding the substance of irritable mood and having a clear and consistent concept of its construction is important, not only for classification and clinical usage but also for researching the phenomenon and obtaining a deeper understanding of how it (and by extension irritability) arises in the first place (Malhi et al., 2019b). However, in addition to the DSM-5 ‘definition’ of irritable mood (a mood with an irritable ‘face’), there are other ways in which it can be conceptualised. The first is a simple reversal of the two constructs, that is to say irritable mood may be a form of irritability that manifests with symptoms of mood (see Figure 1(a)). This possibility is important because it positions irritability as a totally separate entity that can be confused with mood when it has an affective expression. In other words, because one of the ‘faces’ of irritability is mood, it can appear to be an aberration primarily of mood even though its quintessence is that of a separate phenomenon (irritability) and mood is only a facet. To reflect this and differentiate it from irritable mood, it can be called ‘moody irritability’. It is important to note that these considerations are not purely theoretical as they have significant treatment implications. For instance, depending on which of these two conceptualizations (irritable mood versus moody irritability) is correct, it follows that treatments targeting mood alone are likely to be less effective if irritable mood is in fact moody irritability, that is, a form of irritability that is simply ‘disguised’ as mood.
A third possibility is that mood and irritability are quite separate entities that occasionally overlap and in doing so create an admixture that is irritable mood. The margins of this overlap are likely to be fuzzy and difficult to delineate clinically, and hence, at an individual level it may be difficult to distinguish ‘overlapping irritable mood’ from its separate underlying components (i.e. pure irritability and pure mood; see Figure 1(b)). With respect to treatment in this model, the clinical scenario is then quite different and the treatment of either mood or irritability will alleviate irritable mood to some extent and should have some discernible impact, but effective treatment and the complete amelioration of irritable mood will require therapy that successfully addresses both irritability and mood.
Thus far, we have considered irritable mood as a single entity (an outcrop of either irritability or mood) or the result of two entities that intersect/overlap. But there is a further possibility, namely that irritable mood is a separate entity altogether. That is to say, it has a unique identity of its own that it is distinct from both irritability and mood. Explicating further, although irritable mood has elements that appear the same as irritability and mood, at its core it is neither. This does not mean that irritable mood does not or cannot overlap with either or both of these constructs (irritability and mood), but it does mean that with respect to management the treatment of irritable mood (the separate entity) might require therapies distinct to those used to treat either mood or irritability alone (see Figure 1(c)).
Consideration of these various possibilities and the development of a more granular perspective on irritable mood is important as it will assist in driving more focused research and achieving a deeper understanding of all of these constructs. To facilitate this, and to inform the development of more targeted treatment, we have recently posited a novel model for the phenomenology of mood disorders that reintroduces additional domains and adds activity and cognition alongside emotion. Termed the Activity, Cognition and Emotion (ACE) model, this emphasises the dimensional aspect of symptoms – a point that is especially apposite when conceptualising irritable mood.
Conceptualising irritability dimensionally
In our recently proposed ACE model, which attempts to broaden the emphasis within the clinical phenomenology of mood disorders from a single dimension of mood to that of three domains namely activity, cognition and emotion, we have argued that this more sophisticated approach yields a more accurate reflection of reality that also offers a better explanation of mixed mood states (Malhi et al., 2018). In a similar vein, irritability may be more accurately captured if modelled dimensionally – spanning both depression and mania but remaining a separate entity. Therefore, within each of the models depicted in Figure 1, irritability can be considered to be a dimensional construct – similar to the activity, cognition and emotion components of ‘mood’. This model is essential for better understanding of mixed mood states, which are characterised by irritability and can occur in both mania and depression and overlap with anxiety. This is because DSM-5 does not classify mixed mood states as codable episodes – equivalent to depression and mania; instead it uses a specifier to denote their existence. Thus, once again, akin to DSM’s somewhat constricted view of irritable mood, the classificatory system as a whole assigns mood states to categories (e.g. depression and mania) as opposed to placing them on a continuum. In relation to irritable mood, this compartmentalised view is especially evident when considering its diagnostic significance at different ages.
The changing significance of irritable mood with respect to mood state and age
Logically, depressed mood is a key feature of major depression in DSM-5, and in adults, either depressed mood or anhedonia are needed to diagnose major depressive disorder (American Psychiat-ric Association, 2013). However, in adolescents and children, this key feature (depressed mood) – arguably one of the most fundamental symptoms of depression, can be substituted with irritable mood. In other words, to define depression in children and adolescents, irritable mood is on par with depressed mood and anhedonia as a principal defining feature of the syndrome.
There are several possible reasons as to why the diagnostic criteria of depression have been relaxed in relation to age. For instance, it may allow depression to subsume a greater proportion of concurrent anxiety, which is a more prevalent comorbidity in younger populations. Alternatively, it may be that the expression of depression (low mood/sadness) in the developing brain is intrinsically different, and in order to satisfactorily capture it, a broader symptom set is needed. However, it may also be a tacit acknowledgement of the fact that some symptoms are ‘transpolar’, that is, they occur in both depression and mania and reflect the mixed nature of mood disorders, which exist on a spectrum.
As a consequence, the diagnostic significance of irritable mood in DSM-5 changes quite dramatically according to age (see Figure 2(a)). For example, in childhood and adolescence, irritable mood is a key feature of depression (see also Table 1), but in adults it becomes a defining feature of mania. This diagnostic transition from one ‘pole’ of the spectrum of mood to the other as a function of age is confusing because it means that similar symptoms (e.g. irritable mood, agitation, diminished ability to concentrate and suicidal ideation) can be used to loosely define depression when an individual is an adolescent, but then be indicative of mania once they become an adult. In the context of a mixed mood state, this means that an individual defined as having depression with mixed features in adolescence may meet criteria for mania with mixed features once they become an adult. Apart from causing clinical confusion, this diagnostic fluidity has significant implications for treatment within the current frame of bipolar management in which the treatment of mixed mood states is essentially symptomatic and determined by the dominant mood state.
Abridged DSM-5 criteria for both a major depressive and manic episode.
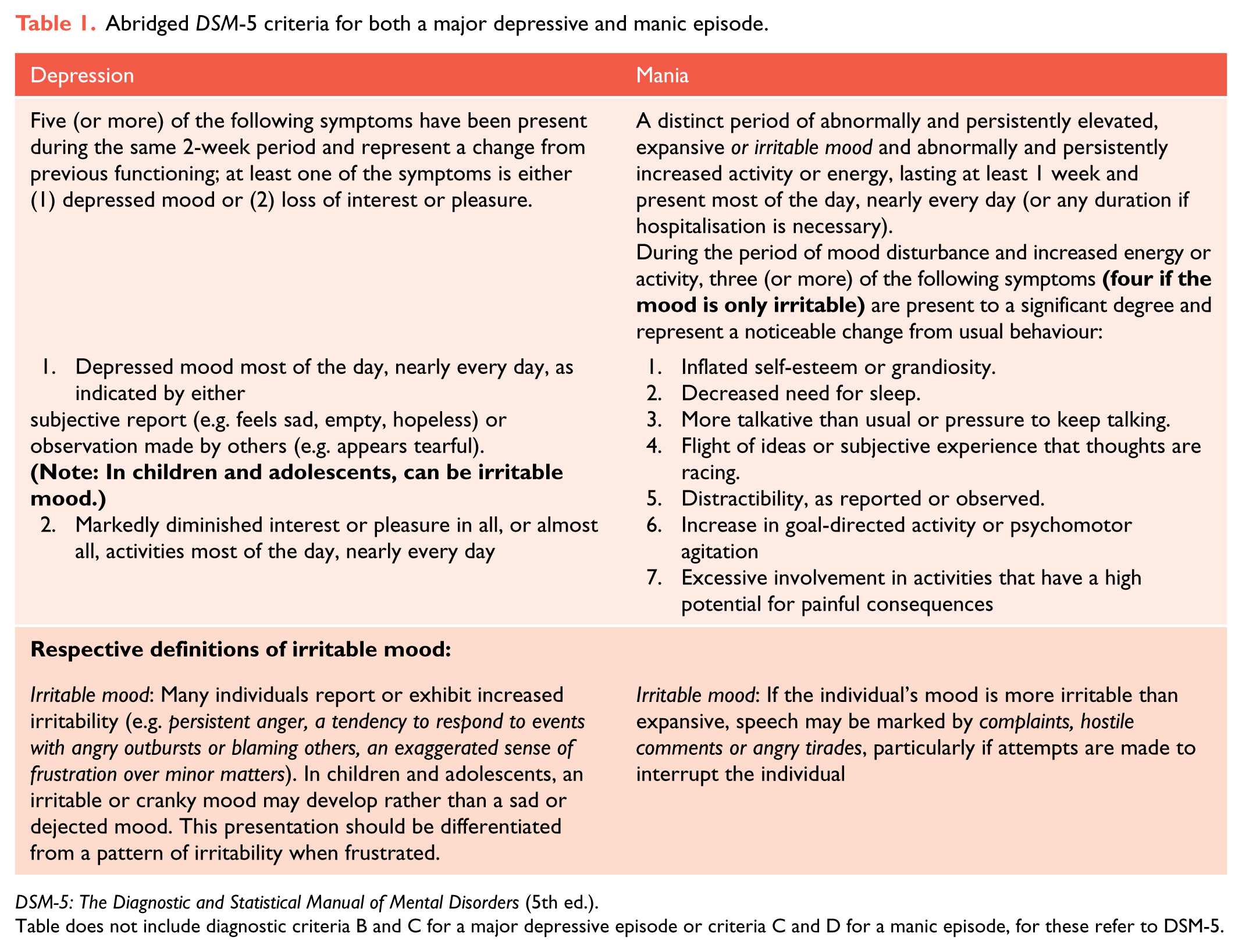
DSM-5: The Diagnostic and Statistical Manual of Mental Disorders (5th ed.).
Table does not include diagnostic criteria B and C for a major depressive episode or criteria C and D for a manic episode, for these refer to DSM-5.
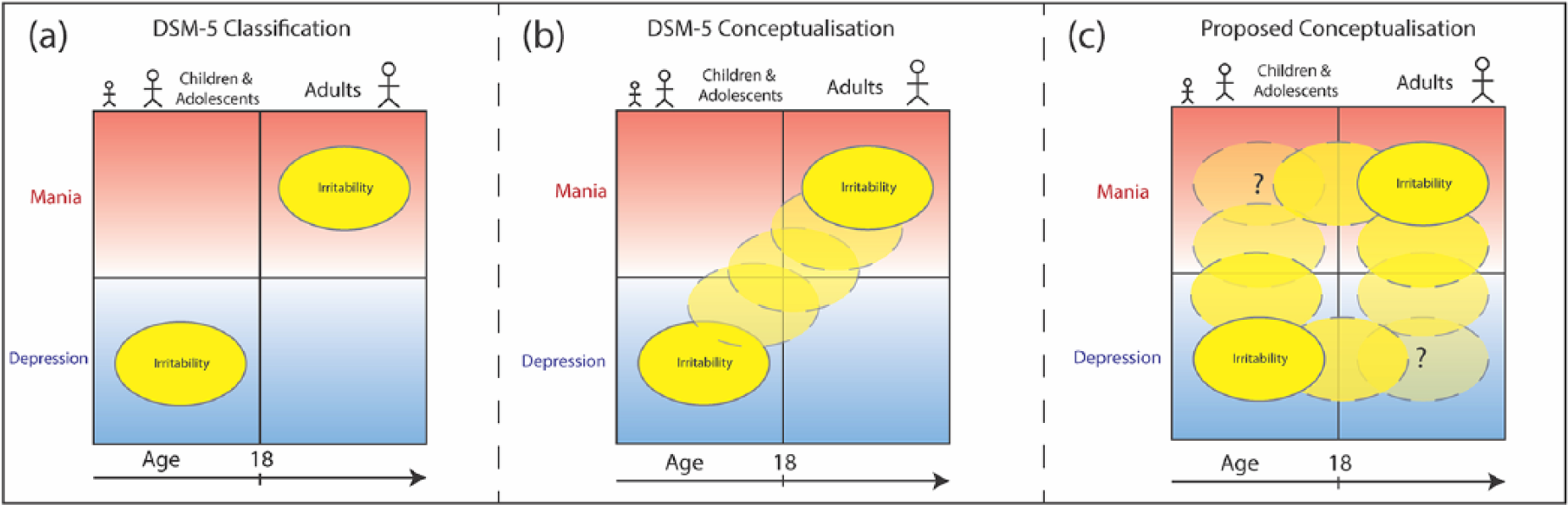
Schematic illustrating both DSM-5 and proposed conceptualisation of irritability from childhood to adulthood. (a) The current DSM-5 criteria regard irritability in childhood as predominantly a symptom of depression and irritability in adulthood as an expression of mania. (b) Temporally, this conceptualisation suggests that irritability transmutes from depressive to manic symptomatology as an individual transitions from childhood and adolescence into adulthood. (c) However, a new proposed conceptualisation regards irritability as a symptom of both mania and depression and is present in both throughout the lifespan. This new conceptualisation captures expressions of irritability such as mixed states and agitated depression, which are currently not accommodated in existing criteria within DSM-5.
Furthermore, the conceptualisation (and compartmentalisation) of irritability (and in particular irritable mood) in DSM-5 (see Figure 2(a) and (b)) is inaccurate because in practice, irritability is thought to reflect mania-like presentations in adolescents and children. However, this is still somewhat contentious, and in recent years, this issue has been the focus of extensive research seeking to define paediatric bipolar disorder. Nevertheless, whether irritability defines bipolar disorder or depression, it is clear that it is very prevalent in these younger populations. At the same time, irritability is also a common feature of depression in the elderly – where it often overlaps with anxiety and agitation and is usually diagnosed as agitated depression.
It is therefore inaccurate and unhelpful to limit irritability/irritable mood to depression and mania in adolescents/children and adults, respectively. Instead we suggest that irritability and indeed irritable mood be conceptualised as a much broader construct that occurs at all ages and in conjunction with the full spectrum of mood. Only then will it be possible to determine its true nature and deduce which of the various models best explains its clinical characteristics.
Conclusion
Currently, the descriptor ‘irritable mood’ permeates both formal and colloquial lexicons and yet lacks a clear definition and fails to provide any meaningful insights as regards diagnosis or treatment. By prematurely compartmentalising irritability according to both age and mood polarity, DSM has hampered research that may have yielded important insights into the relationship between irritability and psychopathology such as that related to mood disorders. To facilitate accurate classification and effective treatment of mood disorders a more sophisticated understanding of irritability is needed, but this can only be achieved by examining irritability both transdiagnostically and across the lifespan and by regarding it as a dimensional construct that is fundamentally distinct from mood.
Fake Views
In an age where everything is seemingly fake, this series examines contentious ideas and concepts in psychiatry in search of the truth.
Footnotes
Declaration of Conflicting Interests
G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. The author E.B. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.