
Abstract

There are significant public and political concerns about the lack of progress in reducing Australian suicide rates, despite numerous national mental health plans and suicide-prevention initiatives over the past three decades. Jorm (2019) has recently invited contributions to ‘please explain’ a graph showing the changes in the Australian suicide rate since 1991 that he annotated with mental health initiatives that might have reduced suicide rates, but these initiatives do not appear to have had sustained effects in preventing suicides.
Our apparent lack of success in suicide prevention could represent a frame reflection problem in which the underlying framing, that is, perceptions, beliefs and understanding of the problem might need to be re-examined (Schon and Rein, 1995). In this context, acknowledging that the framing of the problem might be awry, we turned away from a purely mental health perspective, back to Emile Durkheim’s (2006) seminal work on the sociology of suicide from 1897, where he concluded that each country has a more or less stable, that is, secular suicide rate, unless there are major sociological changes. Durkheim’s hypothesis might be a potential explanation for the rise and fall of Australia’s suicide rate since 1991: suicide rates could have fallen below the country’s long-term mean in the late 1990s and could now be returning to a sociologically determined ‘set point’. If Durkheim’s hypothesis did hold true, it might be the case that Australia’s long-term suicide rate is relatively stable, and not necessarily closely related to, or affected by particular mental health interventions, which are not designed to influence the underlying sociological, cultural and religious determinants of the national suicide rate.
Figure 1 shows the changes in Australia’s male, female and total suicide rates from 1921 to 2017, and the means for the male, female and total suicide rates. We found that between 1921 and 2017, the mean total suicide rate was 12.9 per 100,000 individuals (Australian Bureau of Statistics (ABS), 2018; Harrison and Henley, 2014), the mean male suicide rate was 19.8 per 100,000 individuals, and the mean female suicide rate was 6.2 per 100,000 individuals.

Australian suicide rates per 100,000 individuals by sex from 1921 to 2017.
Of note, there were three significantly discrepant periods with major variations from the long-term means: the increase in the male suicide rate during the Great Depression, peaking in 1930 with 30 suicides per 100,000 individuals; reduction in male suicides during World War II, down to 12 suicides per 100,000 individuals in 1944; and the rising female and male suicide rates, principally attributed to barbiturate access (Harrison and Henley, 2014) in the 1960s (with a female suicide rate of 12.9 per 100,000 individuals in 1965, and a male suicide rate of 25 per 100,000 individuals in 1963).
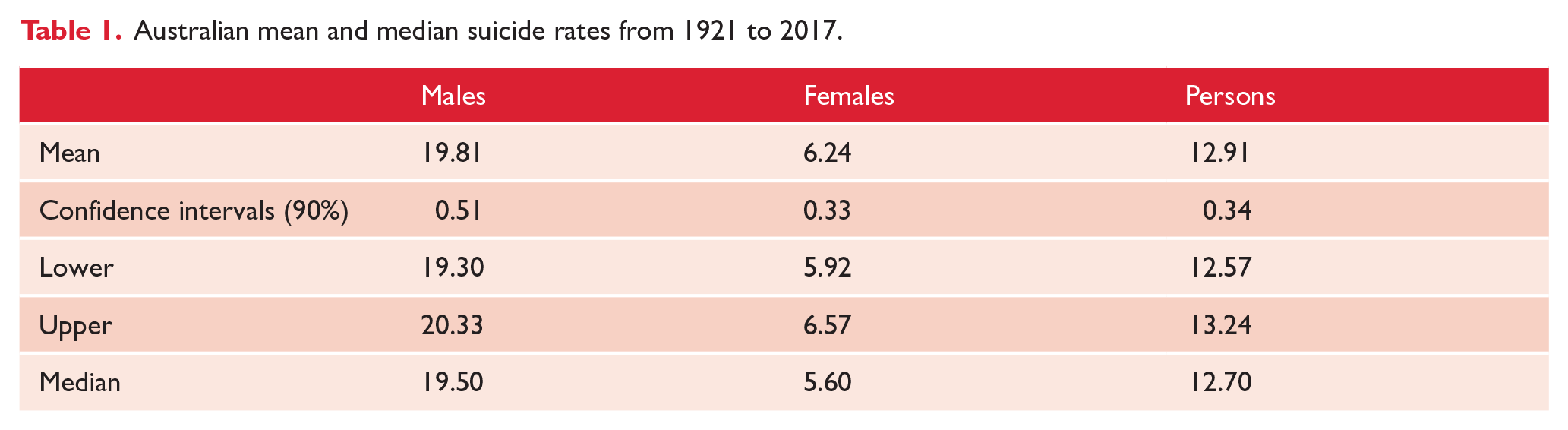
However, after nearly a century, the most recently reported Australian suicide rates (a total suicide rate of 12.6 per 100,000 individuals, male suicide rate of 19.1 per 100,000 individuals, and female suicide rate of 6.2 per 100,000 individuals in 2017) are close to the long-term mean suicide rates from 1921 to 2017 (Table 1). This is a remarkable finding, given the tumultuous history of the 20th century, Australia’s increasing prosperity and three decades of suicide-prevention efforts.
Australian mean and median suicide rates from 1921 to 2017.
Over the 96-year period, the Australian suicide rate was largely stable and predictable with the exception of three sociologically significant time periods (the Great Depression, World II, and the 1960s). This finding of the relative long-term stability of the Australian suicide rate could be somewhat surprising. It is especially notable how stable female suicide rates have been over the last 96 years.
However to Durkheim, the Australian suicide trend would have been entirely predictable, including the findings that the suicide rate increased during the Great Depression and declined during World War II. Durkheim comprehensively studied suicide data across Europe from 1841 to 1872. Durkheim’s general hypothesis was that ‘suicide varies inversely with the degree of integration of the social groups of which the individuals form a part’. He also identified that within a given society, the suicide rate remains largely constant over time. Durkheim specifically stated that ‘each society has a particular disposition towards suicide at any moment in its history’ and that ‘every society is predisposed to supply a given number of voluntary deaths’.
Durkheim, however, noted that there were exceptions to the stability of national suicide rates. Durkheim identified that periods of significant economic, social, or political change might result in ‘anomic suicide’, due to a lack of social integration, and a rise in egoism, as people’s material and social circumstances fall below what they had expected, such as the Great Depression period. In addition, he identified that during major wars, suicide rates actually declined because ‘great popular wars arouse collective sentiments, stimulate partisan spirit and patriotism, political and national faith alike, and … Cause a greater integration of society’.
However, it is important to note that the Australian causes of death data during World War II were significantly affected by the fact that more than half a million men were absent from Australia serving in the armed forces (Harrison and Henley, 2014). Deaths of army personnel from any cause while overseas were not included in Australian death registrations, and population estimates for the period were not adjusted to allow for their absence, leading to an age- and gender-specific dip in the calculated rates of suicide (Harrison and Henley, 2014).
The large increase in Australian suicides related to barbiturate access in the 1960s (Harrison and Henley, 2014) highlights the particular importance of reducing access to lethal means, in order to reduce population levels of suicide.
Conclusion
Preceding Durkheim, suicide was largely thought of as a product of individual despair, and to a large extent, this remains the dominant view in individualistic Westernised cultures such as Australia. However, an examination of Australia’s suicide rates over the last century tends to support Durkheim’s view: only major social upheavals like the Great Depression and World War II changed Australian suicide rates, and even then, they have tended to return to the mean. As Jorm (2019) has highlighted, more recent suicide-prevention efforts have not had a sustained effect on Australian suicide rates, possibly because they were not designed to influence the underlying sociological factors that Durkheim described as determining national rates of suicide.
Australia’s suicide rates since 1921 align with Durkheim’s original theories, and accordingly, we might need to consciously reframe the problem of suicide by moving towards a broader sociological perspective in order to better understand and address this vital issue. This perspective of sociologically determined suicide rates would mean that there are unlikely to be any quick fixes, and that expectations might need to be moderated. Therefore, we suggest that psychiatric researchers focus on the sociological factors affecting Australian suicide rates, in order to inform the development of future suicide-prevention policies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.