
Abstract

Introduction
More than a century ago, Karl Ludwig Kahlbaum and Ewald Hecker coined the descriptor cyclothymia (Angst and Marneros, 2001), which is used interchangeably with cyclothymic disorder. The definition of cyclothymic disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM) has remained virtually the same over the past four decades, and it has been classified as part of mood disorders (Perugi et al., 2015). However, its definition and classificatory home have been questioned, with suggestions that it is better regarded as a temperament, trait or personality disorder as opposed to being a subtype of bipolar disorder.
Criteria
DSM
Criterion A
Duration
Among the criteria for cyclothymic disorder, the most salient is its duration. Criterion A stipulates that symptoms have to be present for ‘at least 2 years’ (American Psychiatric Association, 2013). This is vastly different from bipolar disorder, in which episodes of mania and depression are required to satisfy significantly shorter duration criteria (1 week and 2 weeks, respectively).
Periods of mood symptoms
In addition, criterion A requires that while there are discernible periods of mood symptoms (PoMS; that are presumably different from the normal vicissitudes of mood), none of these (periods) meet criteria for an episode of hypomania/mania or depression at any time.
A direct comparison of criterion A of cyclothymic disorder and typical features of bipolar disorder highlights the differences in time frame between the two presentations (see Figure 1). However, in practice, the distinction is less apparent and more difficult to define – especially when the additional stipulations within DSM are taken into consideration.
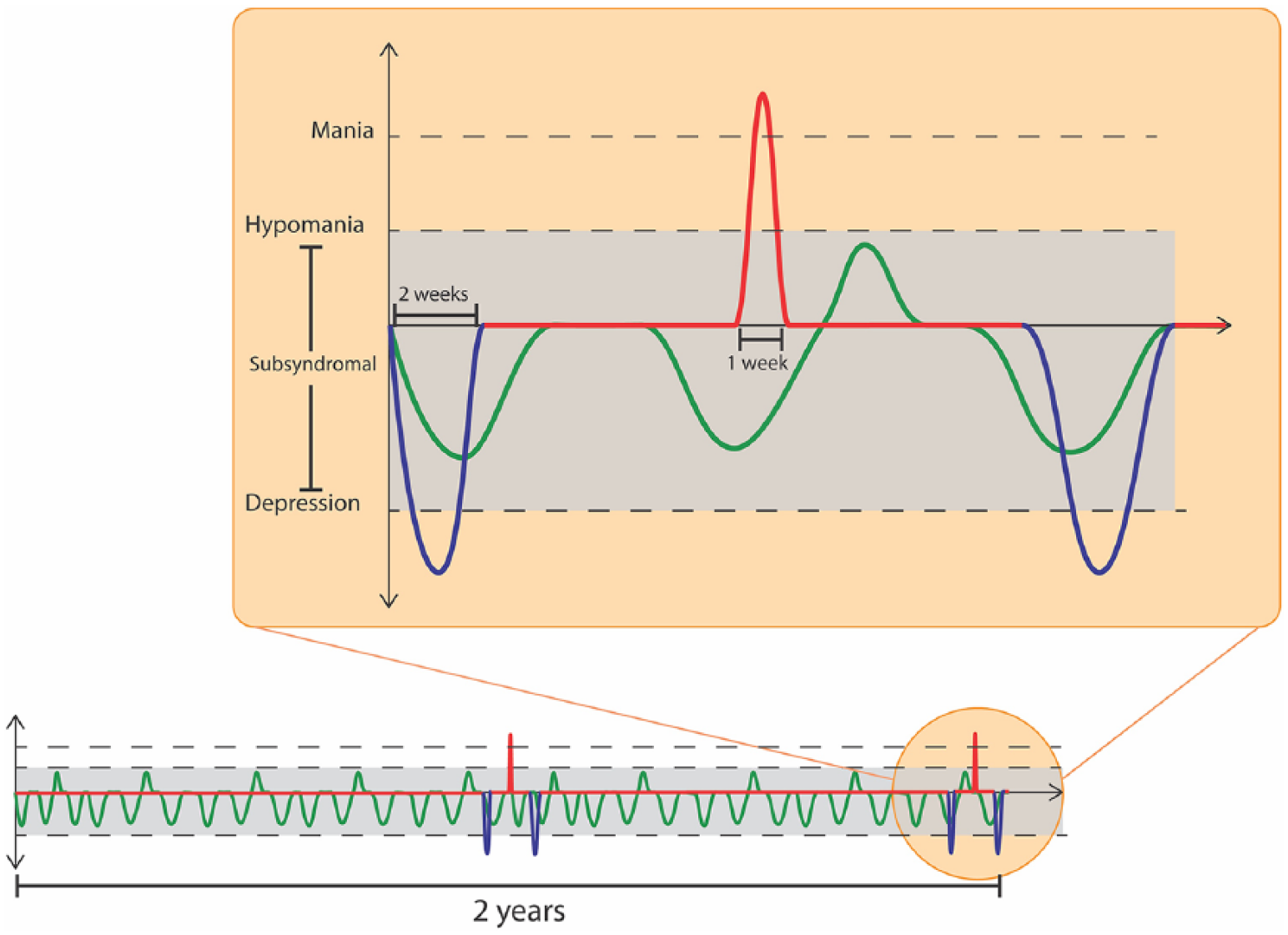
Comparison of duration and severity criteria for cyclothymic disorder (green) and bipolar disorder (red and blue). The schematic representation shows that in comparison with episodes (mania/depression) of bipolar disorder, the symptoms of cyclothymic disorder are less severe but last much longer.
Criterion B
Criterion B adds further duration stipulations, specifying that PoMS must have been present for at least half of the time, and that (during the specified 2 years) there has not been any period of more than 2 months duration during which there have been no symptoms. Clinically, this convoluted definition is extremely impractical.
For instance, the arbitrary stipulation of symptoms occurring for ‘at least half of the time’ – in other words, the majority of the time – provides no information as regards symptom pattern and attaches no importance to whether symptoms are ongoing or recent (Malhi and Bell, 2019). It also means that specific symptom patterns cannot be captured even though they are present for significant periods of time. For example, three PoMS of 6 months each, separated by two periods of 3 months of euthymia (no significant symptoms), fail to qualify as cyclothymic disorder, even though overall the person has been symptomatic for 75% of the time (see Figure 2). Similarly, extended periods of symptoms can be discounted if a period of more than 2 months can be identified during which there are no PoMS. In other words, the person can have symptoms for almost 90% of the time and yet not qualify for the diagnosis. The accuracy with which criterion B can be determined is further compromised by the fact that in real-world clinical practice, information concerning the duration of symptoms is largely reliant on the recall abilities of the patient.
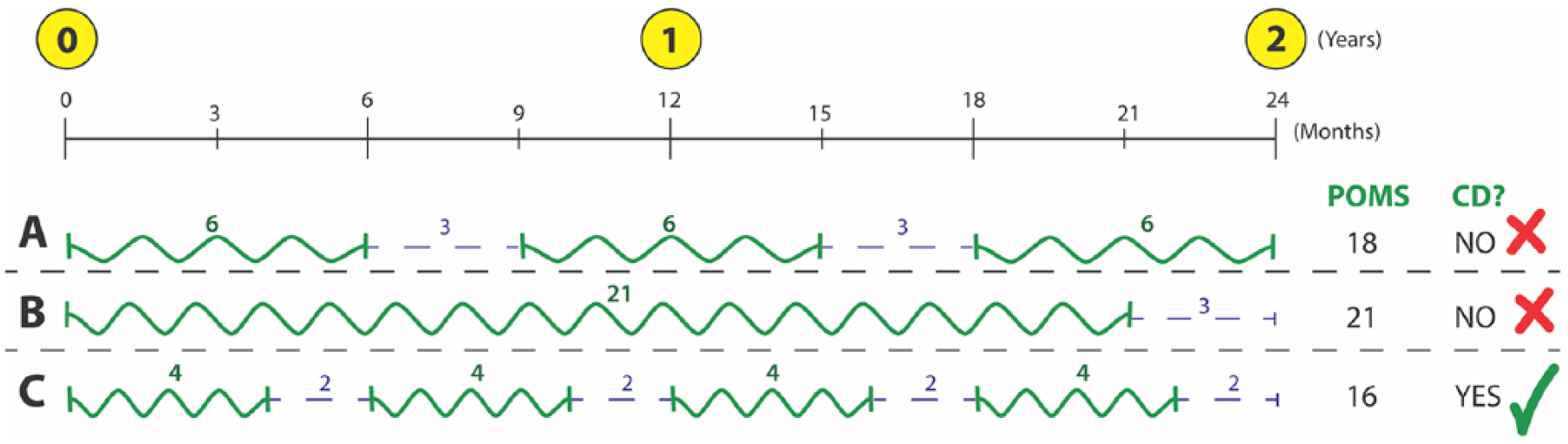
Longitudinal mood symptom patterns. The schematic representation shows how some patterns of symptoms may not satisfy the diagnosis of cyclothymic disorder (CD) on the basis of criterion B. For example, individual A has experienced periods of mood symptoms (PoMS) (green) for a total of 18 months; however, the two periods of euthymia (blue) each lasting 3 months each means that this pattern does not meet criteria for CD. Similarly, individual B experienced 21 consecutive months of PoMS but would also not qualify for diagnosis because of a consecutive 3-month period of euthymia occurring at the end of 2 years. In contrast, individual C who has experienced only 16 months of PoMS (out of the 24) does satisfy cyclothymic disorder criteria, because the periods of euthymia in between only lasted 2 months each.
Criterion C
Criterion C maintains that a depressive, hypomanic or manic episode has never occurred and essentially reiterates what has already been said in criterion A. However, notably, in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5), this criterion does not mention periods of mixed symptoms, even though its predecessor, the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV), included mixed episodes. Presumably, these are not mentioned because these are no longer codable in DSM-5. However, rather than not mentioning mixed presentations whatsoever, mixed episodes should have been replaced by mixed features. This is critical, because clin-ically mixed symptoms are common – especially at the milder end of the bipolar spectrum. Furthermore, from a practical perspective, criterion C is problematic because it does not specify which components of mood episode criteria need to be met, that is, symptom numbers or impairment.
Criteria D, E and F
Subtle variants of criteria D and E appear throughout DSM and reflect its hierarchical nature – in which more ‘serious’ and ‘severe’ mental illnesses and physical/organic illnesses trump milder psychiatric conditions. However, criterion F is worth noting because it stipulates the ‘symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning’. Interestingly, distress can be further emphasised by adding a ‘with anxious distress specifier’.
The key problem is that cyclothymia is meant to be subsyndromal. That is to say, it does not meet criteria for a syndrome. Indeed, a fundamental feature at the cusp of symptom severity is the impact symptoms have on functioning – and it is this transition (whether symptoms cause distress or functional impairment) that determines the designation of a syndrome and thereby a disorder. However, in this instance, DSM specifies that the symptoms of cyclothymic disorder should not meet criteria for an episode (depression, mania, hypomania), but at the same time, they must cause impairment and/or distress. This is a very fine distinction and one which is extremely difficult to gauge.
The second problem is that in order to use the anxious distress specifier, the symptoms need to be present ‘during the majority of days of the current or most recent
International Classification of Diseases–11th Revision
The definition of cyclothymic disorder in the 11th edition of the International Classification of Diseases (ICD-11) is different to that of DSM-5. It specifies that an individual must have experienced ‘persistent instability of mood’ over a period of 2 years (World Health Organization [WHO], 2018). It excludes those who have experienced a depressive episode (stating ‘never been sufficiently severe or prolonged’) but intriguingly allows ‘hypomanic symptomatology may or may not be sufficiently severe or prolonged to meet full definitional requirements of a hypomanic episode’. This is a tacit admission that the margins of hypomania are indistinct – and reflects the clinical difficulty of discerning subsyndromal symptoms of mania. Like DSM-5, the proportion of time the individual has mood symptoms is essentially the majority, but this is captured rather abstrusely as ‘more of the time than not’. However, unlike DSM-5, the ICD-11 definition of cyclothymic disorder does not spell out the nature of any periods during which there is an absence of mood symptoms. Perhaps, because of this, the description of mood instability in ICD-11 probably approximates more closely to the clinical experiences reported by patients, and these criteria may prove more useful for empirical research than those posed by DSM-5.
Short-duration cyclothymia?
Remarkably, despite chronicity being the foundation of the diagnosis and it being common across the two diagnostic manuals (DSM and ICD), DSM has decided to also tamper with this criterion. To this end, within the Other Specified Bipolar and Related Disorders category, DSM-5 has introduced ‘short-duration cyclothymia’ (SDC) as an additional qualifier to capture presentations that do not meet criteria for any specific disorder.
The ‘creation’ of SDC suggests that the key defining feature of cyclothymic disorder, namely its duration, is not essential and that the overall time period of 2 years is somewhat arbitrary. In other words, even though one of the main reasons for having the diagnosis of cyclothymic disorder is that it captures those individuals who fail to qualify for more significant disorders – despite having long-standing symptoms, the introduction of SDC suggests that the enduring nature of symptoms is not that critical. Moreover, not only does SDC state that it can be applied to individuals who have a cyclothymic pattern of symptoms for less than 24 months (less than 12 months in children and adolescents), crucially it does not have a minimal duration criterion. In effect, this means SDC can be applied to any instance in which an individual has periods of subsyndromal mood symptoms (both depressive and manic) – and the overall period over which the diagnosis can be made only needs to be long enough to accommodate multiple mood periods. In theory, this can be as short as a week or even a few days.
Another variation in duration of symptoms that undermines the importance of this criterion occurs when considering cyclothymic disorder in young people. In children and adolescents, the duration criterion for cyclothymic disorder in DSM-5 is half that of adults. Specifically, the diagnosis can be made once children and adolescents have demonstrated the relevant symptom pattern for 12 months (as opposed to 24 months). Again there is no reasonable explanation for this and no indication of whether this shortening of duration also applies to the intervals without mood symptoms.
Conclusion
Mood disorder symptoms differ from normal vicissitudes of mood both qualitatively and by virtue of being more severe and sustained. But when these symptoms occur in a very mild form, they can be difficult to differentiate from normal mood experiences. In such cases, the duration of symptoms, and the fact that they persist, is the feature that is most likely to result in impairment. Given that this is the case, duration is a critical criterion, and one that should not be compromised. Developmentally, it is logical to suppose that a milder form of bipolar disorder precedes the illness, and in some cases, this may be so. But to detect such cases, especially with the aim of attaching prognostic significance, specific criteria are necessary. In this regard, severity is an important differentiating feature, but because cyclothymia is essentially defined by a lack of severity, it means that distinguishing cyclothymia from normalcy on this basis alone is difficult, and therefore duration must remain sacrosanct.
Clinically, cyclothymia is seldom used. And this is most likely because it is difficult to define in writing and almost impossible to discern in practice. To make use of this category and have purpose to its inclusion in classificatory systems, we need to stop dithering and define the diagnosis clearly.
Fake Views
In an age where everything is seemingly fake, this series examines contentious ideas and concepts in psychiatry in search of the truth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. E.B. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.