
Abstract

Pre–disruptive mood dysregulation disorder
Prior to the publication of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) in 2013, it was difficult to diagnose and suitably treat a child presenting with significant impairment and dysfunction because of persistent irritability, angry mood and frequent temper outbursts. This is because in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV), none of the defined childhood disorders fully captured the central symptom of persistent irritability. And although some of these symptoms could be roughly mapped onto oppositional defiant disorder (ODD), attention-deficit/hyperactivity disorder (ADHD) or conduct disorder (CD), many key diagnostic criteria would not be fulfilled. Therefore, in practice, to formulate these symptoms diagnostically, clinicians working with children had to extrapolate from the diagnostic criteria of adult disorders. For example, the DSM diagnosis of bipolar disorder (BD; in adults) makes explicit mention of irritability within its principal criteria for a manic episode. Additionally, in childhood, it is thought that the presentation of BD is not episodic and therefore persistent irritability can be regarded as a symptom of paediatric BD.
However, irritability is not exclusive to mania, and in adolescence and childhood, irritability is also a symptom of depression. In other words, irritability in this age group can reflect mania, depression or both. However, notably, after the age of 18 years, for the purposes of diagnosis in the context of mood disorders, irritability can only signify mania. Because of this confusion, persistent irritability in youth has often led to the diagnosis of BD in children and adolescents.
At the beginning of the new millennium, this diagnostic extrapolation of BD to explain chronic irritability in youth resulted in the rates of paediatric BD diagnoses increasing by approximately 500% in less than a decade (Blader and Carlson, 2007; Moreno et al., 2007). And, understandably, in the face of this apparent ‘epidemic of BD’ among children and adolescents, researchers argued that thorough investigations into the accuracy of a paediatric bipolar diagnosis must be undertaken. This was important because broadening of the diagnosis also meant more widespread prescription of medications – a particularly grave concern because of the risks the use of antipsychotics and antidepressants pose when used in populations in which they have not been properly tested.
Therefore, to counter the increasing rates of paediatric bipolar diagnoses, a totally new diagnosis of disruptive mood dysregulation disorder (DMDD) was suddenly introduced in DSM-5. In this, DMDD is diagnosed in children and adolescents on the basis of chronic and persistent irritability – distinguishing it from the episodic and recurrent pattern of mood episodes observed in adults. However, more than half a decade later, the ‘creation’ of this new diagnostic entity has not provided any novel insights or greater understanding and is yet to demonstrate any tangible clinical benefits. Instead, DMDD has added to existing diagnostic confusion and likely distracted researchers and clinicians from more meaningful exploration of the mechanisms underlying irritability in children and adolescents.
DMDD
Irritability
Irritability is a principal symptom of DMDD and it is common to the phenomenology of several externalising disorders. Hence, there is significant diagnostic overlap between DMDD and a number of other disorders. In addition to the overlap of irritability, some symptoms and behaviours of DMDD may be a consequence of irritability and these are also found in a range of childhood disorders (see Figure 1). For example, behavioural symptoms such as destruction of property, physical/verbal aggression and being argumentative may arise because of ongoing irritability, but these are also the diagnostic criteria for externalising disorders such as ODD. Similarly, psychomotor agitation is an important feature of mania that overlaps clinically with DMDD irritability. The contiguity and imbrication of symptoms that constitute the clinical profile of DMDD with those of other disorders suggests that it possesses no distinctive features, and as such, its criteria are inextricably enmeshed with those used to define a whole range of externalising disorders.
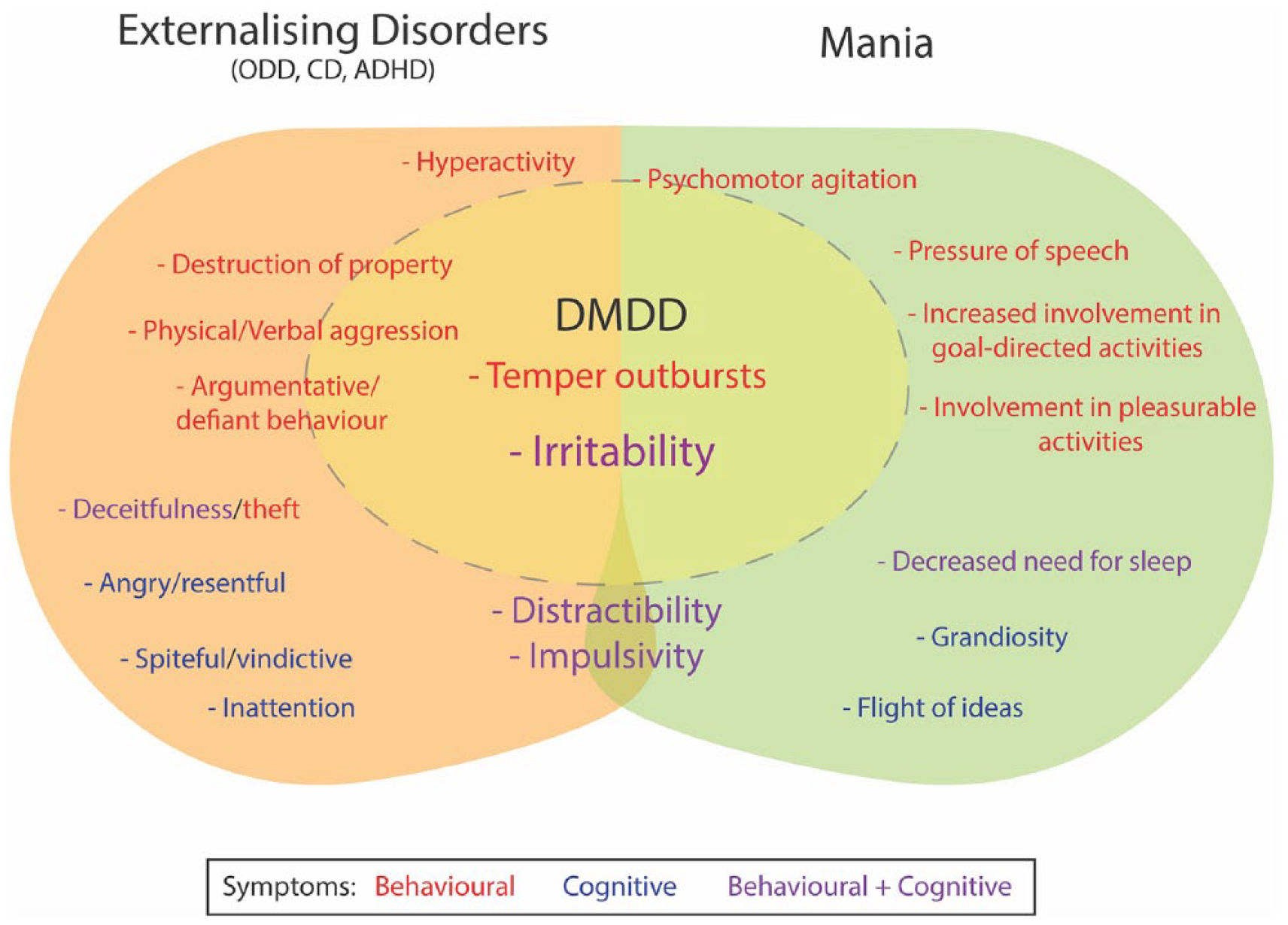
DMDD lacks diagnostic distinction phenomenologically. Figure shows overlap of symptoms between DSM-5 externalising disorders, DMDD and mania. Symptoms/signs that straddle a ‘boundary’ between two disorders may be secondary and arise as a result of primary symptoms, for example, destruction of property as a result of temper outbursts. Broadly speaking the symptoms/signs can also be categorised as being largely cognitive or behavioural or indeed both. It is notable that irritability (a prominent feature of DMDD) is common to many disorders.
Diagnosis
At first pass the diagnostic criteria for DMDD seem to be straightforward and include behavioural outbursts (temper outbursts) set against a background of irritable mood (see Figure 2). But closer examination of the criteria reveals that they are complicated and difficult to understand and apply in practice. For example, it is unclear how ‘temper outbursts’ differ from ‘losing one’s temper’ – a criterion for ODD angry/irritable mood. The nature of temper outbursts that should be considered as being consistent with a particular developmental level is also not specified. Furthermore, throughout the diagnostic decision-making tree (see Figure 2), the empirical basis for each criterion is not made clear, and although the cut-offs are explicit, the determination of duration, severity and context is left to the clinician to interpret and apply.
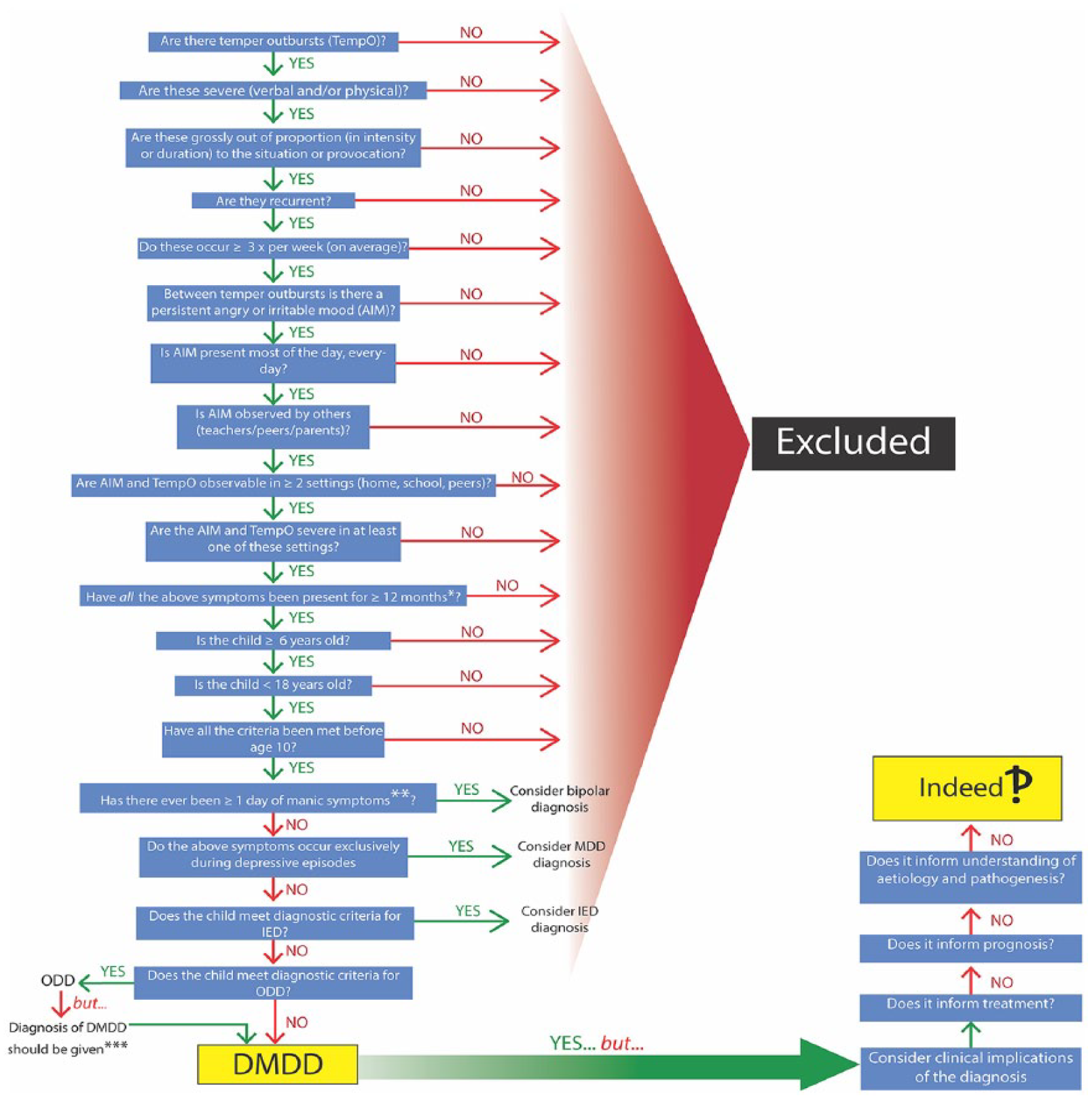
Step-wise diagnosis of DMDD. The decision tree shows the questions that need to be considered in order to arrive at a diagnosis of DMDD as per DSM-5 criteria. It illustrates the complexity of the process and highlights the futility of the experience given that the diagnosis does not inform prognosis or treatment and does not provide any meaningful understanding of the individual’s behaviour and distress.
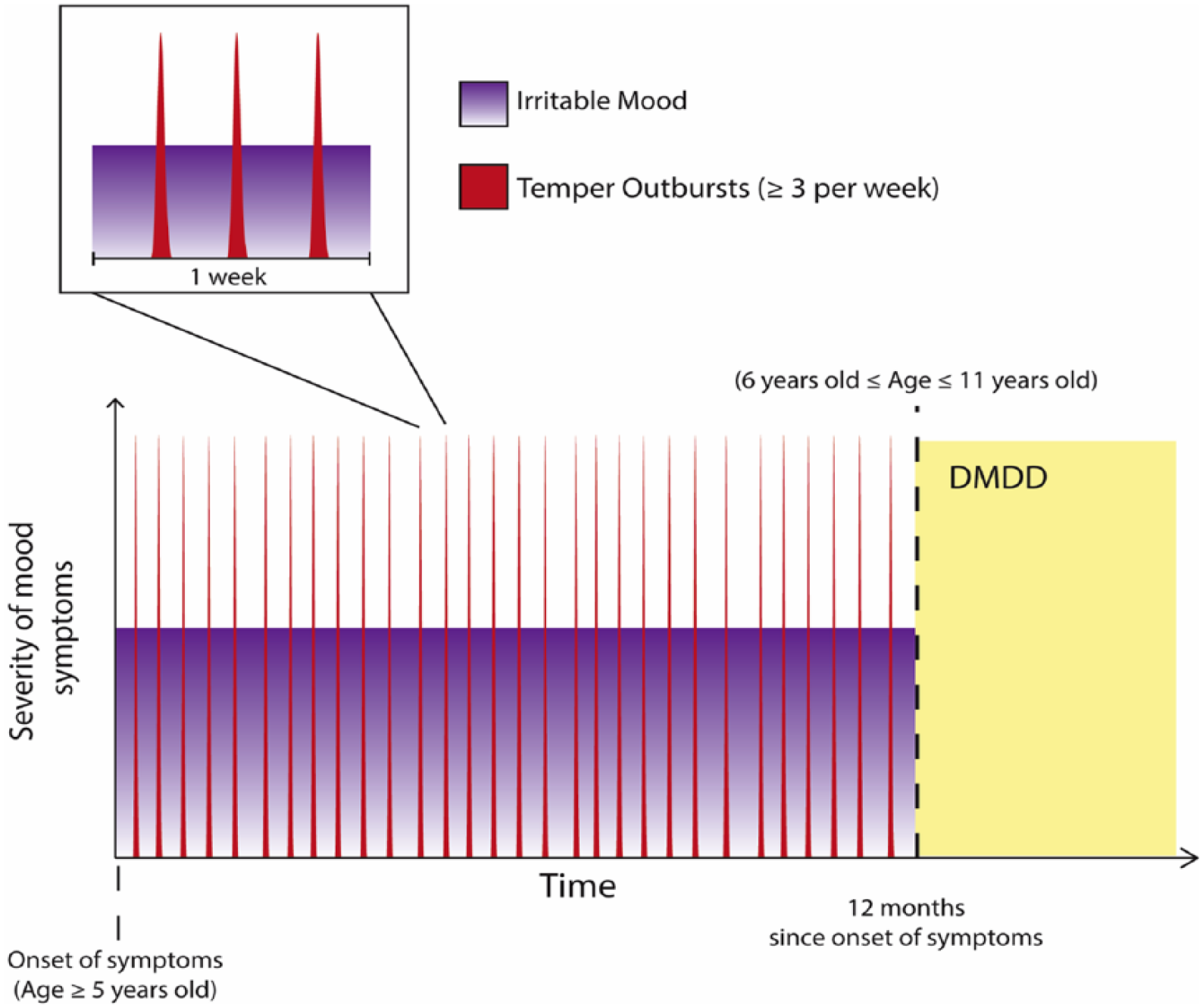
Schematic of diagnostic criteria (A–E) for DSM-5 DMDD. Peaks represent temper outbursts (TempO), which punctuate a persistent state of irritability. Once symptoms have been present for 12 months, a diagnosis of DMDD can be considered, provided these symptoms first appeared between the ages of 5 and 10 years.
As shown in Figure 3, in order to qualify for DMDD, a child must have experienced persistent angry or irritable mood coupled with frequent verbal and/or physical temper outbursts (criteria A and D). Furthermore, the latter must be inconsistent with the developmental level and must occur ⩾3 times per week (criteria B and C). In addition, criterion E stipulates that the aforementioned criteria must have been present for at least 9 of the past 12 months and that there should not have been a period lasting 3 or more consecutive months without all of the symptoms in criteria A–D. This means that there may be many periods of less than this duration when the symptoms are not present – and overall, this may amount to a large proportion of time where there are no symptoms whatsoever. Nevertheless, once this pattern of symptoms has been established, the child’s age also needs to be factored into diagnostic considerations. For instance, the diagnosis cannot be made before the age of 6 years or after the age of 18 years (criterion G); however, at the same time, the above symptoms must have first occurred (onset) before the age of 10 years (criterion H). In other words, these symptoms have to be identified after close observation within a specific window of 5–11 years of age. However, what is not explicated is how this should be achieved. But this is not all that is required.
In order to formulate a diagnosis of DMDD, irritability must be retrospectively reported by at least two sources over a period of at least 12 months. This is problematic because it is not specified how irritability should be measured, and clearly attempting to marry the historical accounts of two people is necessarily difficult. Consequently, the clinical assessment undertaken by a psychiatrist is most likely to rely on forming an impression, which is itself at best drawn from the impressions of others.
Once the aforementioned criteria have been established, criterion F stipulates that both temper outbursts and irritable mood must be present in at least two of the following settings and be occurring at a severe level in at least one of these environments: home, school, or with peers. This criterion therefore requires the corroboration of symptoms from either teachers or peers (in addition to parents) to validate their pervasive and impactful nature. Not surprisingly, in the majority of clinical real-world settings, this is likely to be a formidable challenge for all concerned.
But, still this is insufficient information to make a diagnosis of DMDD. On top of this exhaustive analysis, DMDD then has to be differentiated from other disorders. For instance, the child cannot have had a manic or hypomanic episode (which in itself is difficult to diagnose), but curiously a single day of mania or hypomania is permitted (criterion I). The symptoms also cannot be present only in the context of a major depressive episode and cannot coexist with BD, ODD or intermittent explosive disorder (criterion J). This comorbidity constraint also highlights a diagnostic hierarchy, wherein one disorder takes precedence over another. For example, a child or adolescent that satisfies criteria for both ODD and DMDD should only be given the diagnosis of (DMDD), whereas a diagnosis of DMDD can coexist with any one of CD, ADHD or major depression. This somewhat arbitrary hierarchy likely reflects the fact that disorders such as ODD and DMDD have significant shared phenomenology and that in many instances the diagnoses are subsumed by each other. Hence, why greater diagnostic specificity provides no additional information with regard to treatment.
In sum, the diagnostic criteria for DMDD require the caregiver of the child in question to recollect accurately the frequency, age of onset and duration of both any persistent irritability and temper outbursts the child may be experiencing and then to corroborate this information with another relevant second source such as a teacher. A clinician must then ascertain whether these symptoms are not better explained by a mood episode or other psychiatric disorder that has a significant overlap in symptomatology. This convoluted process – many aspects of which are clearly unrealistic – would at least be theoretically acceptable were it not for the fact that successfully making a diagnosis of DMDD, does not inform management. In other words, the diagnosis offers no insight as regards treatment, and therefore, the process of diagnosing DMDD is redundant. This is also why, in practice, clinicians have to manage DMDD by extrapolating from the treatment of other psychiatric disorders. For example, many children diagnosed with DMDD are medicated with stimulants and/or antipsychotics.
International Classification of Diseases (11th revision)
Clinically, DMDD has failed to distinguish itself from other similar childhood disorders such as ODD (Mayes et al., 2016). This lack of phenomenological distinction means that the diagnosis has failed to achieve its primary goal, namely, to inform treatment. This is perhaps why the World Health Organization (WHO) has not included a diagnosis of DMDD in International Classification of Diseases (11th revision; ICD-11), but instead added a ‘with chronic irritability-anger’ subtype in the criteria for ODD (De Rosa, 2018). Given that DMDD was created by DSM to address the over-diagnosis of BD in youth, amending the criteria of an existing disorder based on empirical evidence of the construct that will encourage accurate scientific investigation of this syndrome is undoubtedly better than generating a new diagnosis altogether.
Post-DMDD
As DMDD lists no distinct criteria of its own and shares significant symptomatic overlap with already defined disorders, it is important to question its conceptualisation as a separate entity. The arbitrary distinction of DMDD risks distorting and skewing our perspective on the inception of adult psychiatric disorders and is likely to generate research that will misinform and mislead clinical practice.
DSM should follow ICD-11 and insert a chronic irritability specifier or subtype within the diagnostic criteria for ODD. This would reflect empirical evidence and also provide a more meaningful framework on which to develop appropriate treatments and further examine the mechanisms underlying paediatric irritability.
Conclusion
DMDD has failed to fulfil the primary role of any diagnostic entity, that is, to inform treatment. Furthermore, the over-diagnosis of paediatric BD, the issue which led to the development of DMDD in the first place, has not been resolved by the introduction of this new diagnostic category. Hence, because of these fundamental flaws that are likely to have dire consequences if left unchecked, urgent consideration should be given to expunging DMDD from DSM.
Fake Views
In an age where everything is seemingly fake, this series examines contentious ideas and concepts in psychiatry in search of the truth.
Footnotes
Declaration of Conflicting Interests
G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. E.B. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.