
Abstract
Objectives:
Retrospective recall of dissociative symptoms has been found to mediate the association between childhood abuse and deliberate self-harm (DSH) in later life. To disentangle the effect of recall bias, we tested whether dissociation symptoms ascertained during an acute DSH presentation mediates this link.
Method:
All participants with DSH were recruited during emergency presentation. Seventy-one individuals aged 11–17 years with overdose (OD) and/or self-injury (SI) participated in semi-structured interviews and psychiatric assessment to measure abuse and dissociation. An age- and gender-matched comparison group of 42 non-psychiatric patients admitted to the same service were also assessed.
Results:
The DSH groups reported significantly higher levels of abuse and dissociation compared to comparison group. Dissociation significantly mediated the association between abuse and DSH. Of the four dissociation subtypes, ‘depersonalisation’ was the primary mediator. Adolescents with chronic patterns of DSH and the ‘OD + SI’ self-harm type reported more severe dissociation.
Conclusion:
Exposure to abuse significantly increased the risk of DSH in adolescence. This association was mediated by dissociation. Our findings suggest a possible dose–response relationship between dissociation with DSH chronicity and the ‘OD + SI’ self-harm type, implicating the importance of evaluating dissociation and depersonalisation symptoms as well as abuse exposure in DSH management.
Introduction
Deliberate self-harm (DSH) is common among adolescents: one school survey reported a prevalence rate of 7%, of whom only 12.6% accessed acute health services (Hawton et al., 2002). The health care needs of self-harming adolescents thereby represent a significant economic burden. A greater understanding of the factors that contribute to DSH in adolescents is therefore essential in developing effective treatment strategies.
Clinical practice guidelines for psychiatrists in Australia and New Zealand have identified several risk factors associated with DSH (Carter et al., 2016). Exposure to childhood neglect and physical or sexual abuse are recognised predictors of DSH (Van der Kolk et al., 1991; Yates et al., 2008). In particular, sexual abuse predicts enduring patterns of DSH (Yates et al., 2008). Up to 79% of those who engage in DSH report a history of childhood maltreatment (Yates et al., 2008), with an estimated fourfold increased risk of later DSH behaviours compared to their non-abused counterparts (Noll et al., 2003). Childhood sexual abuse is commonly found to be most strongly associated with DSH chronicity and severity (including suicidality), though physical abuse is also a significant predictive factor (Brown et al., 1999; Low et al., 2000; Swannell et al., 2012; Yates et al., 2008). Chronicity of DSH has also been highlighted as an important predictor of future DSH risks in a sample of Australian adolescents (Hu et al., 2016). Despite an overrepresentation of those exposed to childhood abuse among those who engage in DSH, prior abuse exposure does not predict DSH behaviour in a deterministic manner. A meta-analysis found only a partial relationship between childhood sexual abuse and later self-injurious behaviours (Klonsky, 2007). Furthermore, a prospective study by Yates et al. (2008) found that 67% of young adults exposed to childhood sexual abuse did not engage in DSH, suggesting that only a third develop DSH as sequelae. Such findings support the hypothesis that the trajectory from abuse to DSH is mediated by other factors (Bolen et al., 2013; Gordon et al., 2016). Dissociation is one factor posited to elevate the risk of DSH among individuals exposed to abuse (Low et al., 2000).
Indeed in adults, dissociation is implicated as a partial mediator between childhood maltreatment/sexual abuse and subsequent DSH (Low et al., 2000; Yates et al., 2008). Similarly, a study of adolescents reported that dissociation mediates the link between sexual abuse, psychiatric symptoms and risk-taking behaviours (including suicidality and self-mutilation) (Kisiel and Lyons, 2001), and this mediating relationship was also reported in adolescents with different psychiatric diagnoses (Kılıç et al., 2017). In other words, exposure to abuse per se may not lead to DSH deterministically and is unlikely to represent a direct or sufficient risk for DSH. Rather, it is the expression of dissociation that instantiates the risk. Despite these findings, dissociation has not been a major focus of DSH nosology to date, nor a target for intervention. For instance, the criteria for ‘Nonsuicidal Self-Injury’ and ‘Suicidal Behaviour Disorder’ in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) under ‘Conditions for Further Study’ do not include dissociation as an associated, relevant or risk factor (American Psychiatric Association [APA], 2013).
Dissociation is defined as a psychological phenomenon that ‘involves disruptions of usually integrated functions of consciousness, perception, memory, identity and affect’ (Krause-Utz et al., 2017). Dissociation symptoms are common in those exposed to childhood abuse, hypothesised to represent a helpless response for defending themselves or ‘mentally escaping’ the negative affect elicited by the trauma (Noll et al., 2003). This view is analogous to the freezing response observed in animals under inescapable threat, contrasting with the active defence mechanism (fight or flight reaction; Krause-Utz et al., 2017). Dissociation in humans is typically conceptualised as a unitary construct, comprising four correlated components: amnesia, depersonalisation, passive influence and absorption (Armstrong et al., 1997). Empirical findings have yielded mixed support for dissociation as a singular or multifactorial construct given moderate to strong correlations observed between these components (Schimmenti, 2016). For these reasons, it remains important to explore the mediating roles of dissociation both as a unitary construct and as separate subcomponents.
Zetterqvist et al. (2014) also found that dissociation mediated the association between childhood maltreatment and DSH in a sample of 816 adolescents. However, childhood maltreatment included a broad variety of events (e.g. parental adversity, bullying). Furthermore, dissociation symptoms and DSH events were ascertained retrospectively (after the DSH events) in all three studies on adolescents (Kılıç et al., 2017; Kisiel and Lyons, 2001; Zetterqvist et al., 2014). Consequently, the findings may be confounded by recall bias. The aim of this study was to evaluate the specific association between childhood abuse and DSH and test specifically the mediating role of dissociation in a child and adolescent sample. To address the recall bias, information on the DSH events and dissociation symptoms were captured concurrently during the acute presentation to emergency service.
For this study, a clinical sample of adolescents was recruited from individuals attending acute hospital child and adolescent services. The relationship between dissociative experiences and DSH was examined, explicitly testing whether dissociation mediates the link between prior abuse and DSH. This study tested a series of four hypotheses in a child and adolescent sample. The first three hypotheses evaluated the relationships between dissociation, abuse and DSH; the fourth hypothesis evaluated a possible ‘dose–response relationship’ between dissociation and DSH, for an association of dissociation severity with DSH chronicity:
Dissociation, abuse and DSH are significantly associated (H1).
Dissociation will mediate the relationship between abuse and DSH (H2).
Dissociation subtypes will each differentially contribute to the mediated relationship between abuse and DSH (H3).
Dissociative symptoms are more severe among those with recurrent chronic patterns of DSH (defined as three or more episodes of DSH attempts in the preceding six months) (H4).
Method
Sample
The study was approved by the local ethics committee in accordance with national protocols for clinical research governance. Seventy-one secondary school-age children and adolescents (between 11 and 17 years) who presented to Emergency Assessment Service in Princess Alexandra Hospital in Harlow, Essex (United Kingdom) with DSH were recruited. DSH was defined as deliberate overdose (OD) or/and deliberate self-injury (SI). Staff from the Accident and Emergency (A&E) department and paediatric medical wards referred DSH cases to the first author (C.H.), who then approached the patients to obtain informed consent and collect information within 48 hours of DSH presentation. Parents and patients were informed in detail about the nature of the research, given a study information sheet and the confidentiality policy and asked for written consent. To ascertain exposure to abuse, semi-structured interviews were conducted with either the child/adolescent alone or, if preferred, with parent(s) present. Information from a standard clinical psychiatric assessment and Self-Injury Schedule (SIS) was used to yield caseness and subtype of DSH. OD was defined as deliberate self-poisoning with medication. SI was defined as a deliberate injury to the skin producing bleeding, bruises or burns – including cutting, stabbing, bruising and banging. Three broad patterns of DSH were identified: ‘OD-only’, ‘SI-only’ and ‘OD + SI’. Patients who undertook both forms of DSH within 48 hours were designated as ‘OD + SI’ subtype.
A comparison group of 42 non-psychiatric patients was recruited by approaching adolescents from the same referral sources. These control patients were either inpatients on the same paediatric ward or outpatients awaiting medical or surgical treatment in the A&E department and were being seen for reasons other than psychiatric consultation. They were matched for the age range and gender distribution of the DSH sample. Exclusion criteria included severe mental impairment and psychotic disorders. No inpatients were recruited from psychiatric wards to avoid potential confounds and inherent referral bias.
Research instruments
The Adolescent Dissociative Experiences Scale (A-DES; version 1.0; Armstrong et al., 1997) was developed as a screening tool of serious dissociative and post-traumatic disorders among adolescents and consists of 30 self-administered items. The psychometric properties of A-DES are validated, with Cronbach’s alpha reported as 0.93 and split-half reliability as 0.92 (Armstrong et al., 1997). Four subscales capture separate constructs of dissociation, notably (1) amnesia, (2) absorption and imaginative over-involvement, (3) passive influence and (4) depersonalisation. Each patient was asked to rate specific dissociative experiences on a Likert-type Scale from 0 to 10 (with ‘0’ representing ‘never’ and ‘10’ as ‘always’). A mean score of 4 or more indicated pathologically significant dissociation.
The SIS (Zlotnick et al., 1997) is a semi-structured interview version of the Self-Injury Inventory (SII; Zlotnick et al., 1997) to record self-harming, self-mutilation, impulsive behaviours and assess a broad spectrum of self-injurious behaviours, including frequency, duration and subtypes of self-injurious acts.
The Child Maltreatment Interview Schedule (CMIS; Vizzard, 1991) is a semi-structured interview to ascertain recall of exposure to maltreatment and collect categorical data on Parental Availability, Parental Neglect, Emotional Abuse, Physical Abuse and Sexual Abuse. In this study, to increase statistical power, ‘physical’ and ‘sexual abuse’ exposures were combined to yield a binary variable designated ‘abuse’.
Statistical analyses
All analyses were performed using version 25.0 of SPSS. Levels of dissociation symptoms for different groups (i.e. abuse subtypes and DSH subtypes) were compared using a series of one-way ANOVAs. Mediation analyses were performed using the PROCESS macro (Hayes, 2017). Fisher’s Least Significant Difference (LSD) was used to correct for the increased family-wise error rate.
Results
Sample characteristics
The total sample consisted of 71 participants with DSH attempts and 42 matched controls. There was no significant difference in male/female ratio between the DSH group (male: n = 11 of 71) and the comparison group (male: n = 12 of 42), χ2(1) = 2.78; p = 0.095. There was also no significant age difference between the comparison group and DSH group, t(111) = −0.76, p = 0.450, or across the three DSH subtype groups (p = 0.837). Descriptive statistics for the sample are presented in Table 1, demonstrating appropriate matching of the comparison group.
Descriptive statistics for DSH group with subtypes and comparison group (N = 113).
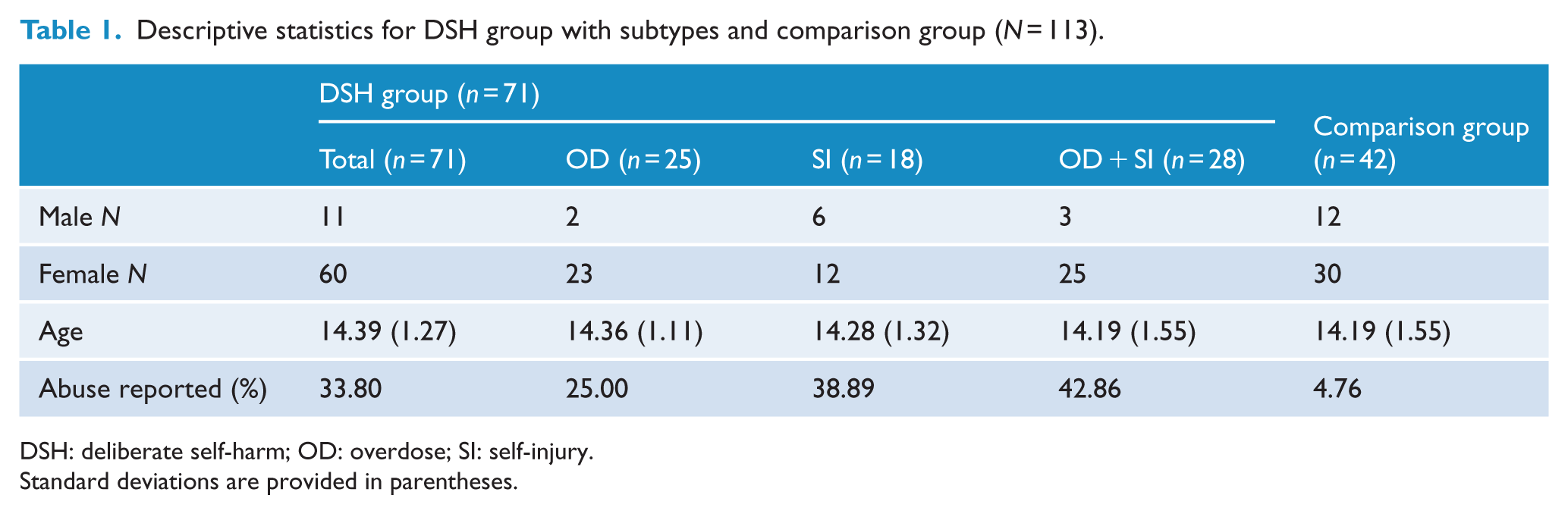
DSH: deliberate self-harm; OD: overdose; SI: self-injury.
Standard deviations are provided in parentheses.
Point bi-serial correlations between abuse, total and subtype scores of the A-DES and any form of DSH are presented in Table 2, showing significant associations of relevant parameters.
Pearson correlation coefficients between prior exposure to abuse, A-DES total and subscale scores and any form of deliberate self-harm (N = 113).
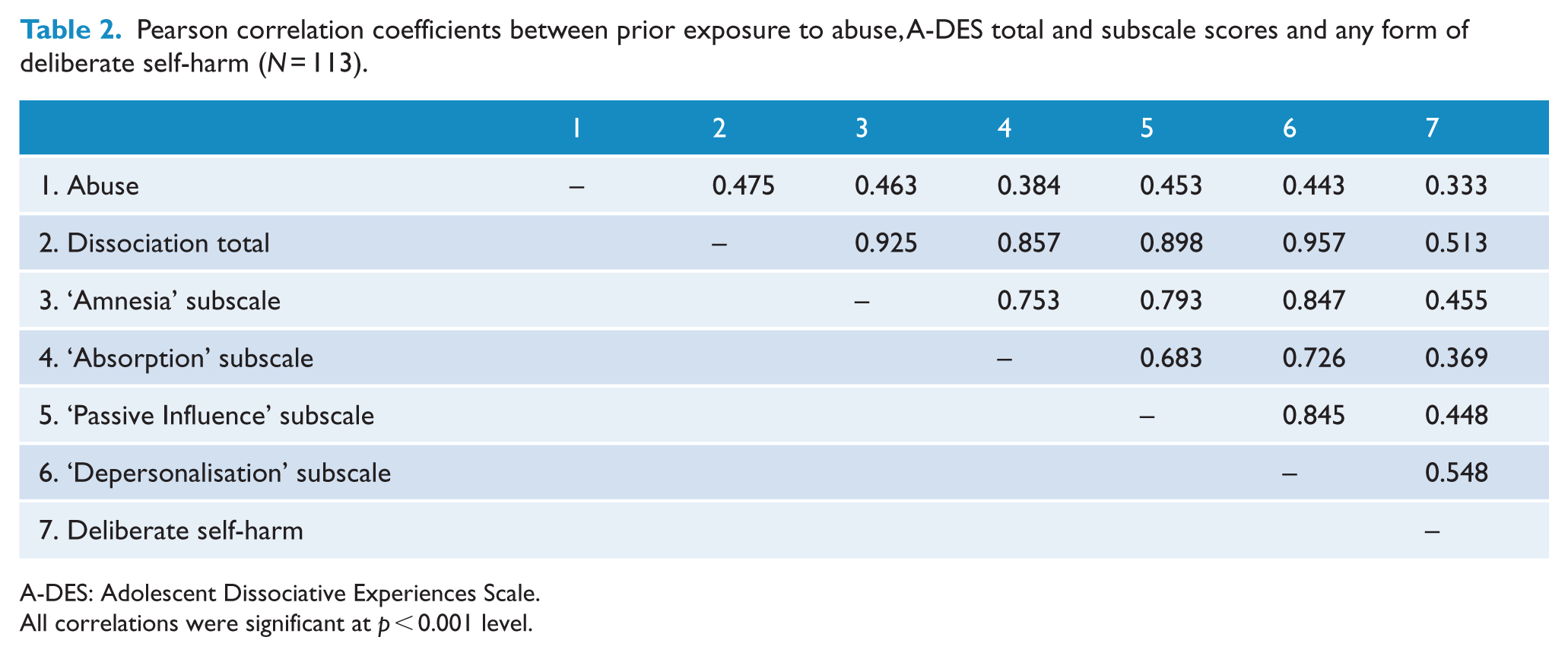
A-DES: Adolescent Dissociative Experiences Scale.
All correlations were significant at p < 0.001 level.
Dissociative symptoms, abuse exposure and DSH patterns
First, dissociation scores of ‘OD + SI’ patients (A-DES total score mean = 4.49) were significantly higher than those of ‘SI-only’ (A-DES mean = 2.84) and those of ‘OD-only’ (A-DES mean = 2.02). Dissociation scores of ‘OD + SI’ and ‘SI-only’ groups were significantly higher than that of the control comparison group (A-DES mean = 0.87; Table 3).
Differences on A-DES total and subscale scores across groups of DSH subtypes and exposures to abuse.
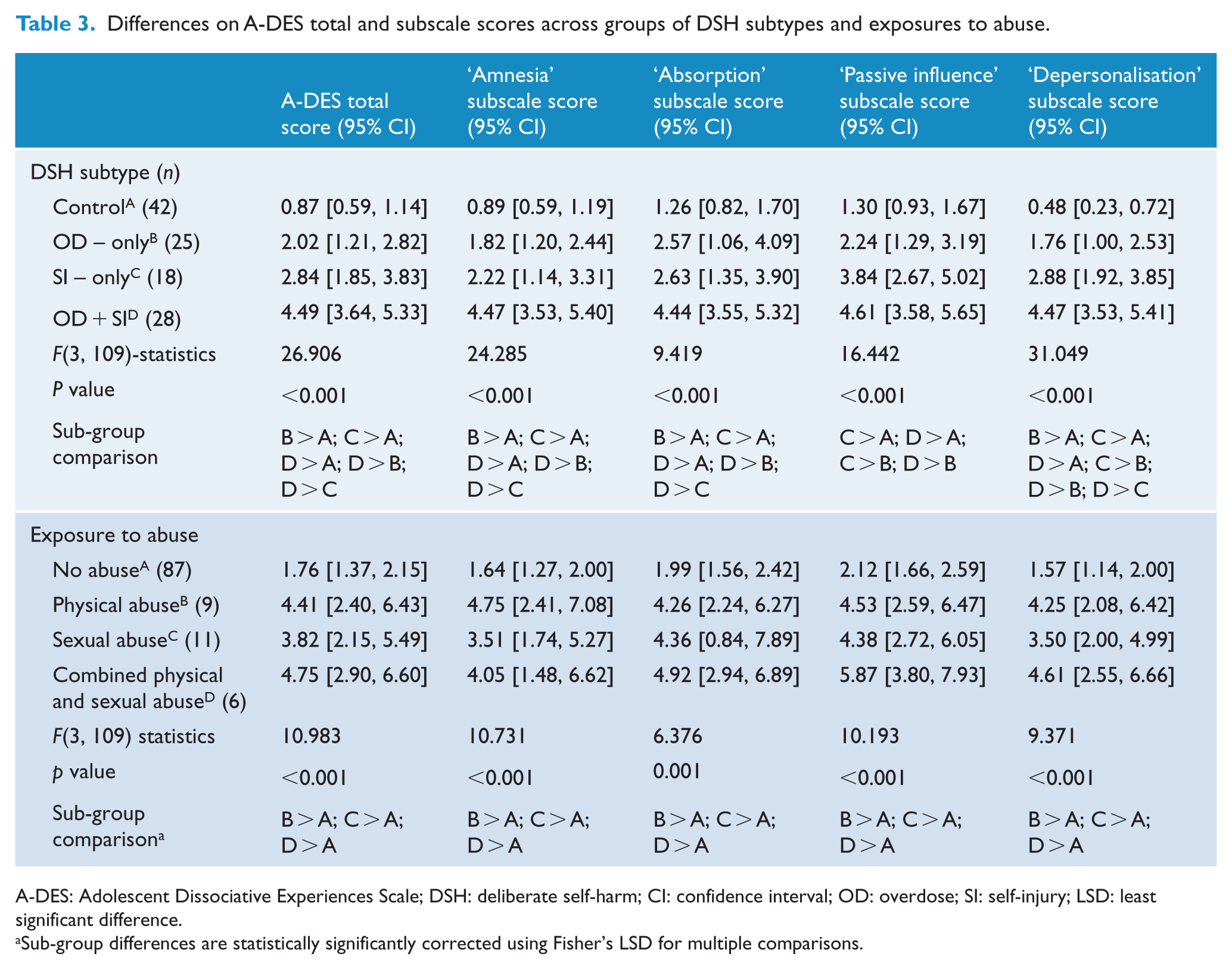
A-DES: Adolescent Dissociative Experiences Scale; DSH: deliberate self-harm; CI: confidence interval; OD: overdose; SI: self-injury; LSD: least significant difference.
Sub-group differences are statistically significantly corrected using Fisher’s LSD for multiple comparisons.
Second, depersonalisation symptom scores were significantly higher for patients who committed any form of DSH (i.e. ‘OD-only’, ‘SI-only’ or ‘OD + SI’) than the controls. Moreover, symptom scores for experiences of depersonalisation and amnesia were significantly higher in the ‘OD + SI’ group compared to control, ‘OD-only’ and ‘SI-only’ groups. This uniquely distinguished the ‘OD + SI’ group.
Third, dissociation was significantly associated with exposure to abuse, F(2, 110) = 16.56, p < 0.001. However, there was no significant difference between those exposed to physical abuse (A-DES total score mean = 3.82) and to sexual abuse (A-DES total score mean = 4.55). Thus, to increase statistical power, we combined these two subtypes into a single binary variable (i.e. ‘abuse’) for subsequent regression analyses.
DSH and abuse
Chi-squares test of contingencies identified that exposure to any form of abuse significantly increased the odds of presenting to hospital with any form of DSH above the comparison group: χ2 = 12.56, p < 0.001, odds ratio (OR) = 10.21, 95% confidence interval (CI) = [2.27, 45.90].
The mediating effect of dissociative experiences
Binary logistic mediation analysis using the PROCESS macro (Hayes, 2012) was used to evaluate whether the association between prior abuse (IV) and DSH (DV) was mediated by dissociation (M).
In the first ordinary least squares regression model, abuse was positively associated with dissociation, b = 2.48, standard error (SE) = 0.44, p < 0.001, 95% CI = [1.61, 3.34]. In the second logistic regression model, which included abuse and dissociation as predictors of DSH, abuse (b = 1.12, SE = 0.86, OR = 3.06, 95% CI = [–0.56, 2.80], p = 0.191) was not independently associated with DSH at criterion significance. However, dissociation was significantly associated with DSH (b = .92, SE = 2.33, OR = 2.51, p < 0.001, 95% CI = [0.47, 1.34]). This suggests that for each unit increase in dissociation, the odds of DSH increased 2.51 fold and abuse no longer significantly predicted DSH independent of dissociation (see Figure 1).
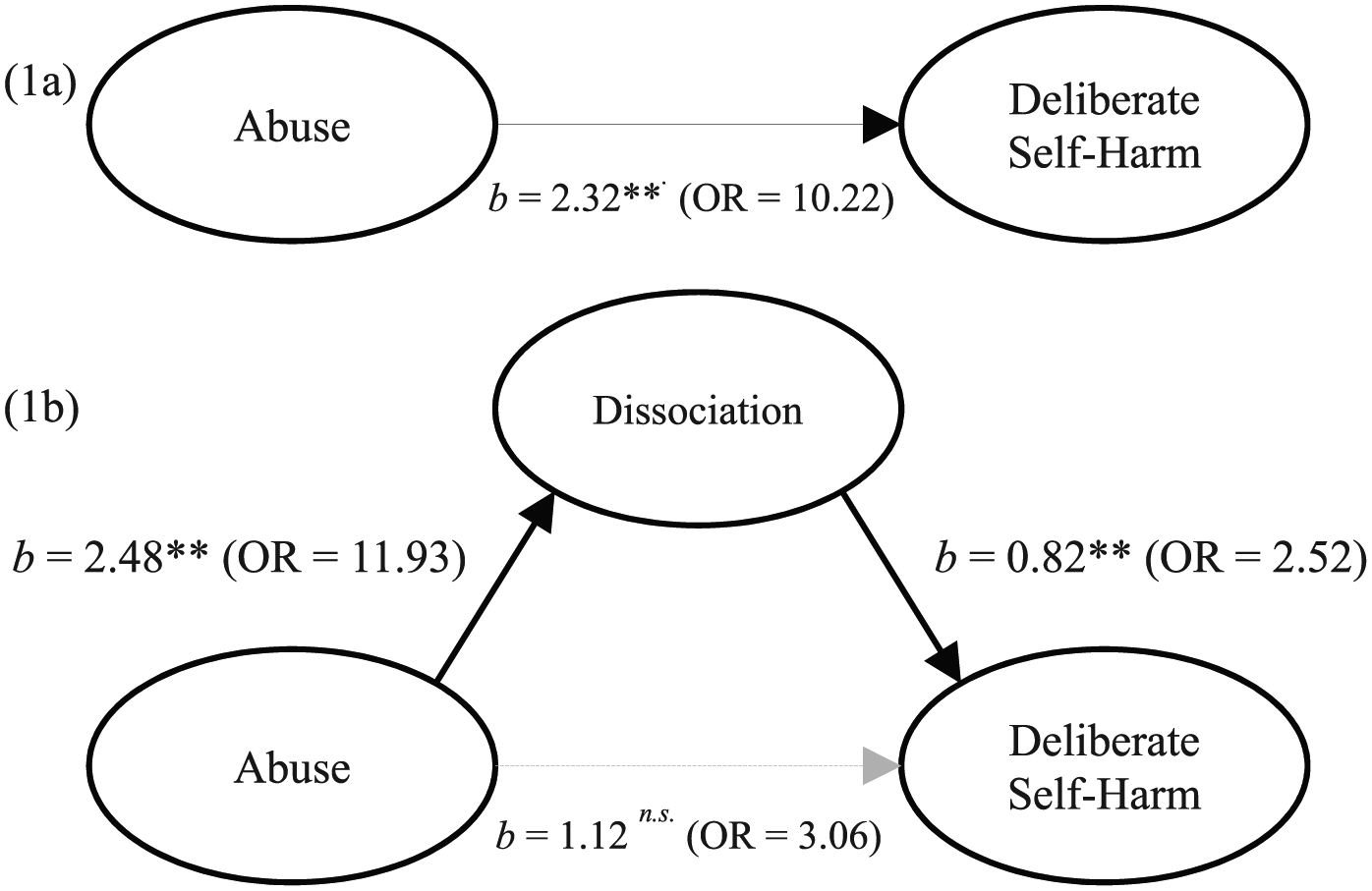
Logistic mediation model demonstrating that the association between abuse and deliberate self-harm (DSH) is mediated by dissociation as measured by the Adolescent Dissociative Experience Scale (A-DES) score. Significant pathways are depicted with solid line (**p < 0.001). The first model (1a) depicts the significant association between abuse and deliberate self-harm prior to the inclusion of dissociation as a mediator variable. The second model (1b) depicts the non-significant association between abuse and deliberate self-harm after the inclusion of dissociation as a mediator variable.
The bootstrapped and bias-corrected CI derived from 10,000 samples indicated that the indirect effect coefficient was statistically significant (b = 2.29, SE = 0.92, 95% Bayesian credible intervals (BCI) = [1.15, 4.71]). The Sobel test statistic (Z = 3.26) was statistically significant, with Baron and Kenny’s Percentage (Proportion) of Effect Mediated calculated as 78.37%. In other words, 78.37% of the observed direct effect of abuse on DSH was mediated by dissociation. This supports the hypothesis that the association between abuse and DSH is mediated by dissociation (see Figure 1).
Dissociation subtypes
A follow-up logistic mediation analysis using the PROCESS macro (Hayes, 2017) evaluated a multiple mediator model whereby the association between abuse (IV) and DSH (DV) was mediated by each of A-DES subtypes of dissociation: namely, amnesia (M1), absorption (M2), passive influence (M3) and depersonalisation (M4).
In the first of a series of ordinary least squares regression models between abuse and four subtypes of dissociation, abuse was positively associated with each of the four subtypes of dissociation (b ranging from 2.43 to 2.65) at the p < 0.001 level.
In the second logistic regression mediation model, which included abuse and the four subtypes of dissociation as predictors of DSH, abuse (b = 1.10, SE = 0.84, OR = 3.01, 95% CI = [−0.75 to 2.94], p = 0.242) was not independently associated with DSH, consistent with previous finding demonstrating the mediating pathway via dissociation. Of the four subtypes entered in the mediation model, only the depersonalisation subtype was significantly associated with DSH (b = 2.11, SE = 0.59, OR = 8.25, p < 0.001, 95% CI = [0.95, 3.28]; see Figure 2). The Sobel test statistic (Z = 3.28) was statistically significant, with Baron and Kenny’s Percentage (Proportion) of Effect Mediated calculated as 85.72%, indicative of a strong mediation effect. Thus, these findings do not support the hypothesis that all dissociation subtypes mediate the association between abuse and DSH.
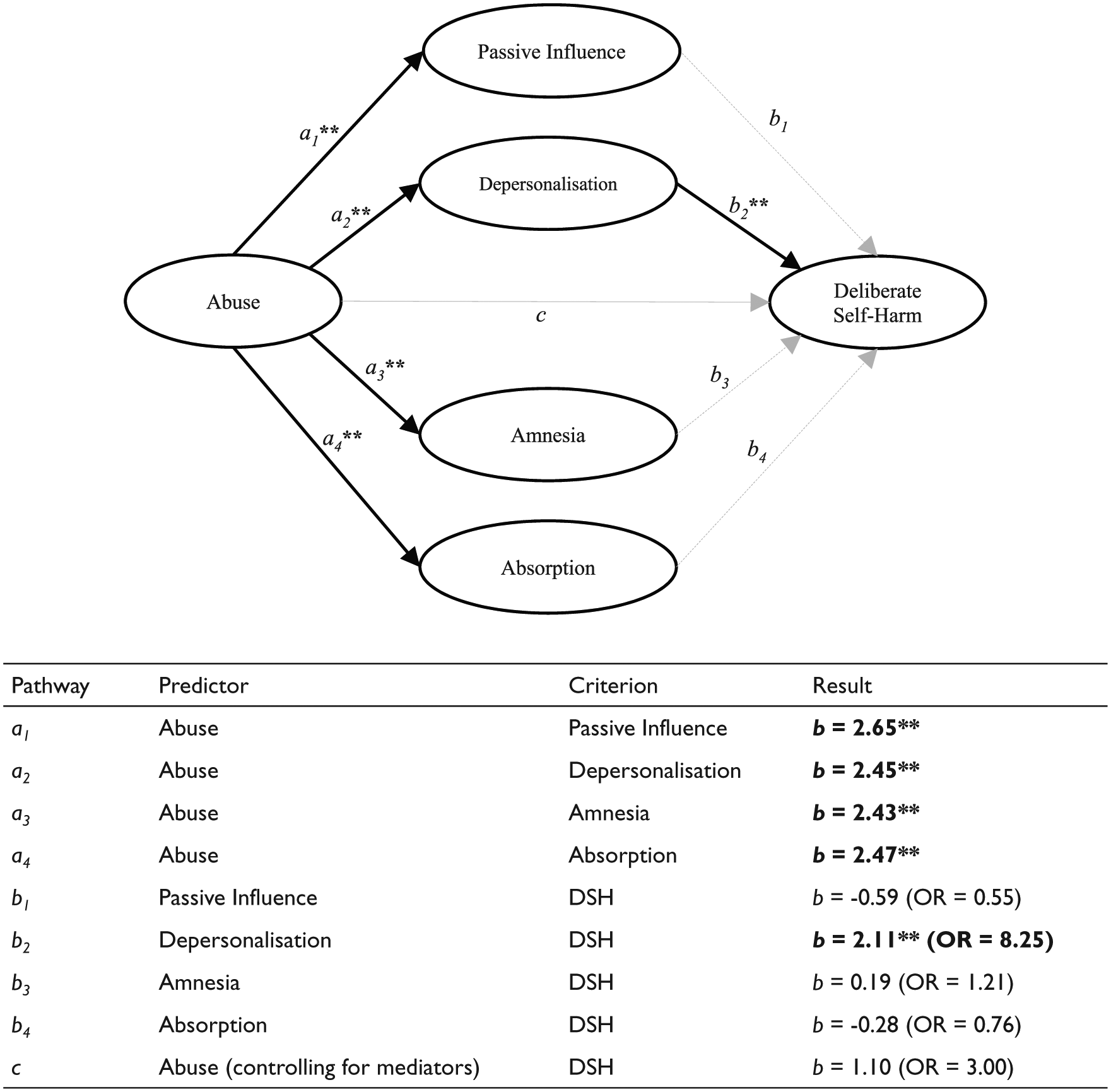
Logistic mediation model demonstrating that the association between abuse and deliberate self-harm (DSH) is mediated by only the ‘Depersonalisation’ subtype of dissociation as measured by the Adolescent Dissociative Experience Scale (A-DES) score. Significant pathways are depicted with solid line. Pathway coefficients are provided in the table below the figure (OR = odds ratio; **p < 0.001).
Chronicity of DSH
Each patient’s history of DSH of repeated patterns of DSH behaviours was also ascertained. To maximise statistical power, the inter-subject variation in DSH patterns was condensed into a dichotomous variable of ‘DSH chronicity’, defined as three or more episodes of DSH attempts occurring over a period of 6 months before the current presentation. Forty-one patients were classified as ‘chronic’ as compared with 30 patients ‘without chronic DSH’.
Abuse was significantly associated with ‘Chronic DSH’; patients exposed to abuse were found to be 3.13 times more likely to engage in ‘Chronic DSH’ compared to without abuse exposure (OR = 3.13, 95% CI = [1.06, 9.28], p = 0.04).
Analysis of variance (ANOVA) corrected using Fisher’s LSD was used to compare the total and subtype scores on the A-DES between individuals with a history of ‘Chronic DSH’ to those without chronic DSH. Those with ‘Chronic DSH’ reported significantly higher A-DES total scores, in addition to the amnesia, passive influence and depersonalisation subtypes, with large effect sizes observed. No significant difference was observed on the absorption subtype, though the size of the effect was medium (see Table 4). These findings are mostly consistent with the hypothesis that dissociative symptoms are more severe among those individuals with recurrent patterns of DSH.
Comparison of score means for children and adolescents with and without chronic deliberate self-harm (N = 71).
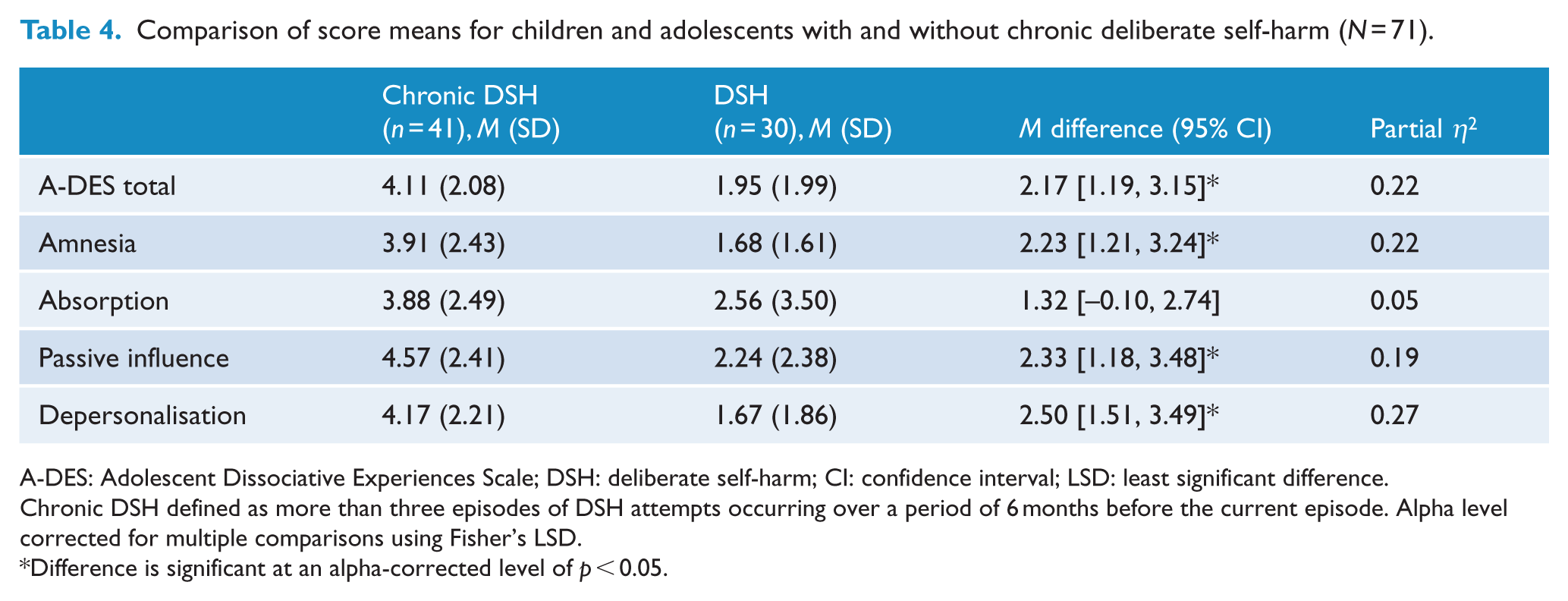
A-DES: Adolescent Dissociative Experiences Scale; DSH: deliberate self-harm; CI: confidence interval; LSD: least significant difference.
Chronic DSH defined as more than three episodes of DSH attempts occurring over a period of 6 months before the current episode. Alpha level corrected for multiple comparisons using Fisher’s LSD.
Difference is significant at an alpha-corrected level of p < 0.05.
Discussion
There are four key findings. First, there is a three-way association between dissociation, abuse and hospital attendance for DSH. Second, the effect of abuse on DSH is mediated by dissociation. In other words, exposure to abuse per se does not necessarily predict DSH: it is the expression of dissociation in the context of abuse exposure that predicts DSH. Third, within subscales of dissociation, depersonalisation exerted the strongest mediating influence. Fourth, severe dissociation is associated with DSH chronicity. In other words, our finding suggests that abuse and dissociation are likely pathoetiological in the development of recurrent DSH. If replicated and causality established, this finding will enhance the conceptualisation, clinical recognition and targeted treatment of chronic DSH behaviours.
Overall, our findings provide informative and novel evidence that dissociation – particularly depersonalisation – mediates the relationship between DSH and maltreatment. In other words, our analyses isolated depersonalisation as a candidate symptom that related to exposure within the context of DSH as well as its chronicity. This finding is in line with recent evidence indicating that depersonalisation contributes to the pathway linking sexual abuse and non-suicidal SI within an adult sample (Gómez, 2018).
Our observations extend previous findings within the DSH literature on the relative contribution of dissociation to DSH (Foote et al., 2008; Kaplan et al., 1995; Shearer, 1994; Van der Kolk et al., 1991; Zlotnick et al., 1999) and its mediating role in linking childhood maltreatment to recurrent DSH in adults (Low et al., 2000; Yates et al., 2008). We show that such models are valid in an adolescent population, providing convergent evidence with adult studies, independent of differences in study design, size and patient type. Previous studies typically use self-reported retrospective recall of abuse exposure. One exception is a prospective study of a high-risk birth cohort that recorded abuse exposure using multiple source information including direct observations, care-giver interviews, reviews of child protection and medical records and teacher interviews (Yates et al., 2008). In this cohort, dissociative symptoms were also measured at the age of 17 and 26 years, prior to self-harm behaviours assessed at the age of 26 years. This rigorously designed study provides arguably the most compelling evidence in adults that dissociation mediated the link between DSH and abuse exposure.
There are five relevant studies reporting associations between dissociation, abuse exposure and self-harm in adolescents (Kisiel and Lyons, 2001; Matsumoto et al., 2004, 2005; Tolmunen et al., 2008; Zoroglu et al., 2003). These cross-sectional studies include two community samples recruited from high schools (Tolmunen et al., 2008; Zoroglu et al., 2003); psychiatric clinic sample spanning a wide age range (15–30 years; Matsumoto et al., 2004) and a forensic sample of self-cutters among male juvenile inmates (Matsumoto et al., 2005). Among these, Kisiel and Lyons (2001) conducted a mediation analysis, implicating dissociation in mediating the link between abuse and DSH; Zoroglu et al. (2003) examined a community sample of high-school students and found trauma and dissociation contributed to suicidal attempts and self-mutilation, with dissociation as the strongest predictor (Zoroglu et al., 2003). However, recall of abuse exposure, dissociation and DSH measures were not ascertained simultaneously in all these studies, thus the confounding interaction of recall and response bias in reporting self-harm outcome in particular could not be ruled out. An advantage of our study is the immediate ascertainment of DSH data with independent medical verification during the acute episodes while patients attended the acute hospital service, thereby minimising the effect of recall and response bias on DSH status. Furthermore, dissociation symptoms were also captured during the acute presentation. Our data ascertainment, within an acute hospital setting, further compliment and strengthen the existing convergent evidence.
The UK National Institute of Clinical Excellence (NICE) guidelines on self-harm acknowledges the influences of childhood abuse and dissociation. It notes that in those who were abused as children, acts of self-harm occur seemingly out of the person’s control or even awareness, during ‘trance-like’, or dissociative states; that there is a strong association between childhood sexual abuse and the development of childhood post-traumatic stress disorder (PTSD) and that the later emergence of self-harming behaviours may well be a response to this. The argument here is the personalised sense of detachment may be critical, as also suggested by the prominent role of depersonalisation subscale of dissociation in our findings.
However, the phenomenology of depersonalisation is complex, encompassing a range of qualitative alterations in subjective experience beyond detachment (Medford et al., 2005; Sierra, 2009). Depersonalisation may represent a distinct symptomatic cluster as suggested by large studies of patients with primary depersonalisation disorder (DPD; Sierra et al., 2005; Simeon et al., 2008). Typically, there is dampening of emotional experience, a sense of disembodiment or lack of body ownership and anomalies in subjective recall with an alteration in the quality of personal memories: Factual recall of past events may be broadly intact but memories seem to lack a personal quality. One patient quoted, ‘I can remember things, but it seems as if what I remember did not really happen to me’ (Sierra, 2009: 33).
Psychological models of depersonalisation (Medford et al., 2005; Reutens et al., 2010) construe it as a response to threat; a coping mechanism that places distressing events and consequent negative affect at an experiential distance. This study suggests that depersonalisation phenomena in adolescents merit special clinical attention, both to better characterise the phenomenology of mental states predisposing to DSH and also as an avenue targeted for therapeutic intervention. Functional magnetic resonance imaging (MRI) studies of patients with primary DPD suggest that underactivity of the anterior insula may be the key neurobiological correlate of the alteration of subjective experience that is central to the depersonalised state (Medford et al., 2016). The anterior insula is thought to play a crucial role in the integration of bodily feedback into awareness, so insula hypoactivity is a plausible substrate for the reduced emotional responsivity and sense of estrangement from the body that characterise depersonalisation.
Gene–environment interaction in the pathogenesis of dissociation is reported as exerting an indirect effect of maltreatment on dissociation, via ‘limbic irritability’ as moderated by FKBP5 gene variants. The FKBP5 gene is found to be involved in regulating the sensitivity and binding affinity of the glucocorticoid receptor, with implicated roles in the functioning of the limbic system (Dackis et al., 2012). A significant interactive effect of the timing and chronicity of childhood maltreatment exposure with FKBP5 risk haplotype is also reported on the expression of dissociative symptoms in adolescents, indexing an interaction between genotype and childhood maltreatment in predicting trauma-related psychopathology (Yaylaci et al., 2017). However, these studies have not examined DSH as a distal outcome. Therefore, future studies examining the mediating effect of dissociation in the link between DSH and maltreatment exposure could usefully include genetic markers. Genetic vulnerability in response to maltreatment exposure leading to dissociation and self-harm presents a novel and potentially fruitful avenue for research and therapeutic innovation.
These psychological and genotypic risk factors for dissociation in adolescents are likely moderated by the severity of trauma experienced. Trauma severity has been previously shown to predict the severity of dissociation, suggesting this is an independent pathogenic process of dissociation that manifest during traumatisation (Maercker et al., 2000). This association is pivotal, as dissociation severity was shown to be predictive of DSH frequency in a review by Černis et al. (2019). This review also highlighted a smaller number of studies that documented a mediating relationship between childhood trauma and DSH similar to that identified in this study. These findings highlight the potential importance of measuring trauma severity to better understand the associations between dissociation and DSH. The measurement of trauma (i.e. abuse) in this study was dichotomous, rather than dimensional, precluding the exploration of trauma severity effect as an independent variable, thereby reducing the statistical power of our model. Nevertheless, evidence of a mediating relationship was still identified. However, ‘trauma severity’ per se is likely a complex multifaceted construct rather than a unidimensional representation of ‘dosage’. ‘Trauma severity’ is most likely influenced by a number of factors, such as the age at which the trauma occurred, the victim’s relationship to their abuser (or abusers), the degree of control the victim experience, victim’s temperament and resilience traits, the extent and duration of the abuse, the response of significant adults to any disclosure and number of incidents. The impacts of these parameters may also vary within different contexts. We therefore postulate that these relationships should be evaluated in greater and more nuanced details in future research in adolescents whereby additional measures of trauma severity can be ascertained and explored.
Limitations to our study include a theoretical possibility that dissociative symptoms are the consequence of the DSH behaviours (Kisiel and Lyons, 2001) wherein reports obtained during the acute episodes may represent epiphenomena of DSH acts per se. However, this is unlikely as similar conclusions are reached by a study using retrospective recall data, when the subjects were not actively self-harming or in the immediate aftermath of DSH behaviours. Taken together, our own study, along with the retrospective study, supports the notion that trait dissociation mediates the association between DSH and abuse; and does not support the alternative view that abuse gives rise to DSH, which in turn induces the dissociative state. Second, our measure of chronicity still ultimately depends on the recall by an adolescent during an acute DSH episode. There is a need for further replication of these findings since recall bias and suggestibility, possibly further confounded by the presence of dissociative symptoms, cannot be excluded. Furthermore, our definition of chronicity may also be confounded with the frequency of DSH within the preceding time window, rather than longer term chronicity. Future studies using either hospital or general family practitioner prospective records or preferably both can potentially overcome this weakness.
The A-DES (Armstrong et al., 1997) was used to measure dissociation in our study, as this measure is one of the few reliable measures validated for use in the adolescent population. Albeit an older measure of dissociation, the items in the A-DES still capture many of the experiences identified in the DSM-5 operational definition: ‘disruption of and/or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, and behavior’ (p. 291). Nevertheless, it is important to note that new measures (such as Dissociative Experiences Measure, Oxford [DEMO]; Černis et al., 2018) have been developed to reflect the more contemporary conceptualisation of dissociation; however, these new measures have not been validated in research for adolescents. Overall, dissociative experiences are now considered to be broader and more complex than the symptoms specified in older measures of dissociation, such as the A-DES (Černis et al., 2018, 2019). The Dissociative Experiences Measure, Oxford (DEMO) by Černiset al. (2018) capture five dimensions, reflecting the contemporary operationalisation of dissociation (‘Unreality’, ‘Numb and Disconnected’, ‘Memory Blanks’, ‘Zoned Out’ and ‘Vivid Internal World’). Validation of this scale for an adolescent population could facilitate replication of this study with an updated measure of dissociation.
Conclusion
The relatively low importance accorded to dissociation within DSH literature is mirrored in management guidelines issued by the APA (2004; Jacobs et al., 2010) and American Academy of Child and Adolescent Psychiatry (AACAP; Shaffer and Pfeffer, 2001). Preliminary evidence from studies of dialectical behavioural therapy supports the targeting of dissociative symptoms in DSH care (Linehan, 1993). Our findings underline the importance of recognising, understanding and treating such symptoms, as their presence indexes risks in terms of repetition, severity and exposure to abuse. These findings are also relevant to future taxonomic revision.
Overall, our results show that exposure to abuse is strongly associated with DSH and that dissociation symptoms, especially depersonalisation, mediate this association. Dissociation further influences the chronicity symptoms supporting its central importance in the etiology and maintenance of DSH behaviour. Our findings potentially have practical clinical implications. First, clinical identification of the recurrent variant of DSH among adolescents appears essential. Here, an ‘at risk’ adolescent may only disclose exposure to maltreatment or sexual abuse during an unhurried and sympathetic clinical interview conducted with sensitivity and informed knowledge. Second, dissociative symptoms need to be elicited accurately and explicitly during clinical evaluation, as this is not yet routine practice. Finally, while 70% of recurrent self-injurers report a history of childhood sexual abuse, it is also important to note that 67% of those exposed to sexual abuse do not progress clinically to DSH (Yates et al., 2008). Therefore, abuse exposure does not predict self-harm in a deterministic manner. Historical exposure to abuse cannot be reversed, yet treatment can be tailored to attenuate dissociative symptoms. Our findings argue for further research on the role of dissociation. This future work may formulate new ways of treating and preventing repeat DSH behaviours that can complement existing Australian and New Zealand clinical practice guidelines for the management of deliberate self-harm (Carter et al., 2016).
Footnotes
Acknowledgements
The authors also thank the participants and families of this study, North East Essex Mental Health Trust and Professor David Baldwin for reading the manuscript and his comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The data collection of this study was funded by C-MENT Trust awarded to the first author (C.H.).