
Abstract

A great deal of intelligence can be invested in ignorance when the need for an illusion is deep.
Pareidolia is a sensory deception and largely a normal phenomenon. But the term is rarely used as a clinical descriptor of phenomenology these days, and hence this brief exploration of its meaning and putative use in an attempt to bring it back into our psychiatric vernacular.
Sensory deceptions are divided into illusions and hallucinations. Illusions are misinterpretations of existing stimuli, whereas hallucinations occur in the absence of a stimulus. Sims (2003) described three types of illusions. Complete illusions usually arise because of inattention such as misreading a word that is then replaced in one’s mind by a word from prior experience. Affect illusions arise in the context of a particular mood state, for example, visually perceiving a deceased person during bereavement or interpreting an innocent gesture as threatening in depression or anxiety. And similarly, Pareidolia is an illusion because it develops as a consequence of attending to an actual stimulus, usually an image or a sound, such that a familiar pattern is perceived despite none existing.
The word pareidolia derives from the Greek para (παρά, ‘beside, alongside, instead [of]’ – in this context meaning something faulty or wrong) and the noun eidolon (εἴδωλον ‘image, form, shape’ – the diminutive of eidos). The illusion leads to the interpretation of random images, or patterns of light and shadow, as known objects. Common examples are perceived images of animals, faces or objects formed within flames of a fire, or clouds in the sky. Also, hearing indistinct voices against background noise such as that produced by air conditioners or fans are pareidolia illusions.
An inherent bias towards the perception of faces is logical given that newborn babies preferentially look at faces and face-like patterns, suggesting a predisposition to detect and attend to stimuli that most likely form a face. This exquisite sensitivity to face recognition might also explain why the mere perception of a face can produce the same subconscious reactions we have when we look at a real person. Interestingly, Takahashi and Watanabe (2015) found that we track the gaze of phantom faces (for example, see Figure 1) in the same manner as that employed to track the eyes of a person in front of us.
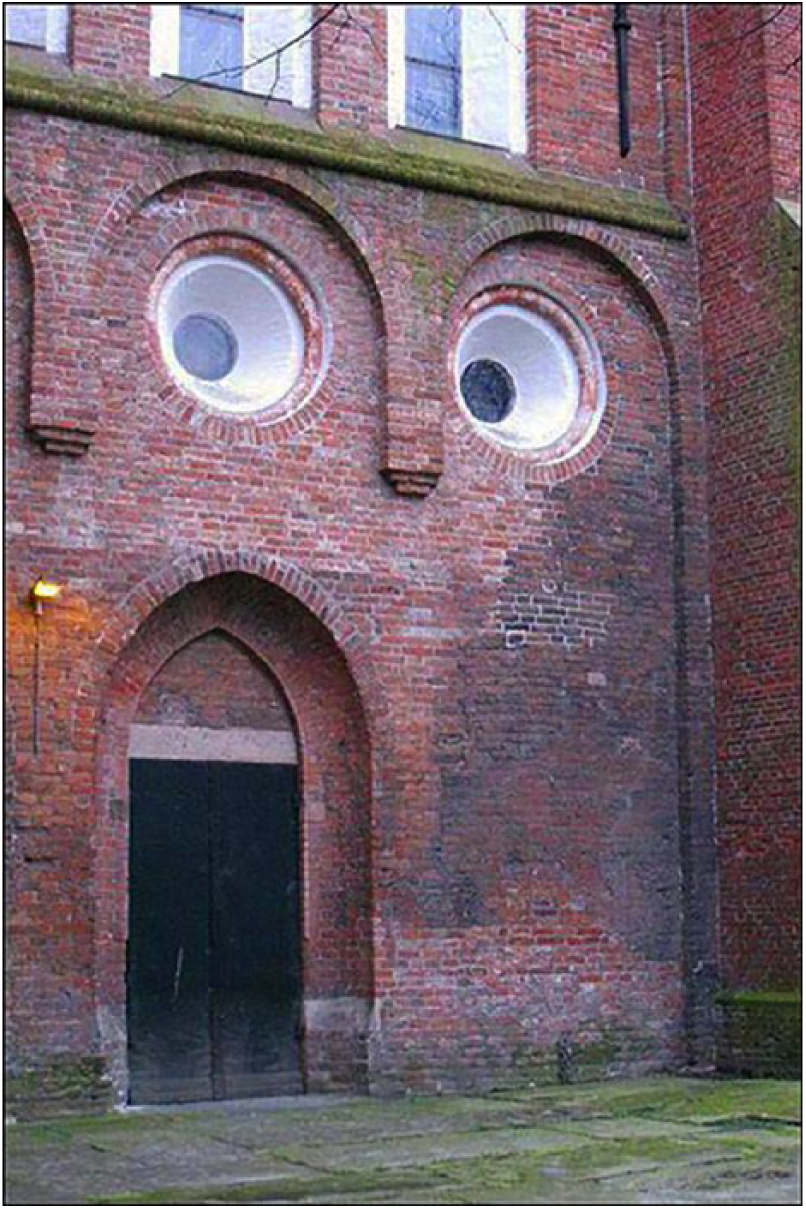
Pareidolia in everyday life. An image of a building providing the illusion of a face. When you see this perplexed building giving a sideways glance you might have an urge to see what’s making it gawp. From: http://www.bbc.com/future/story/20140730-why-do-we-see-faces-in-objects. Creative Commons Licence Wout Mager CC BY-NC-SA 2.0.
Recently, several studies have investigated the phenomena of pareidolia using functional magnetic resonance imaging (fMRI) and have found that objects perceived as faces evoke an activation within the fusiform face area (FFA), which is located in the inferior temporal cortex, whereas perceiving other common objects does not evoke such activation. The FFA is responsible for facial recognition and it responds in a speedy 165 ms in response to face-like objects, while the activation is faster still (occurring in 130 ms) for images of real faces (Voss et al., 2012). Voss et al. (2012) have suggested that face perception evoked by face-like objects is a relatively early process, and not a late cognitive reinterpretation phenomenon. These results indicate that the interpretation of ambiguous stimuli depends upon processes similar to those elicited by real objects (Voss et al., 2012). In a later study, Liu et al. (2014) examined neural responses of participants to pure-noise images – akin to analogue TV static – when they were led to believe that 50% of those images contained faces or letters. In all, 34% of participants ‘saw’ faces in these images, and in these participants the FFA showed greater activity when participants reported ‘seeing’ faces as opposed to letters. This suggests that the FFA plays a role not only in processing real faces but also in illusory face perception. Taking these findings together, face pareidolia is not wholly imaginary; rather, it also has an organic basis.
Pareidolias are also used in medical diagnostic processes; for instance, in MRI the discovery of the ‘hummingbird sign’ in progressive supranuclear palsy and the ‘panda sign’ in Wilson’s disease. Evidently, our brains are hard-wired to find familiar patterns in contrasts and this leads to increased sensitivity and specificity when the gradients between normal and abnormal are increasingly difficult to perceive.
The perception of any object requires the synthesis of the current experience of the object (i.e. ‘it’s a dog’) with other aspects not immediately available but related to experience and memory (i.e. ‘can bite, can be dangerous.’…). A coherent synthesis does not develop if the object is only seen in terms of one of those aspects. The organisation of the various aspects of a perceived object into a coherent meaning occurs before conscious perception takes place. Therefore, the perception of an object is relative to the experience and standpoint of the observer and thus not necessarily ‘objective’ (Uhlhaas and Mishara, 2007).
Intriguingly, these findings suggest that the brain is able to make predictions about what we will see, based on our past experience, and projects these expectations onto what we actually see. In this manner the brain pieces together a picture, erroneously or not, even if the image is not clear. It also makes our vision more subjective than we often assume, suggesting that perhaps we really do see what our brain ‘wants’ to see!
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.