
Abstract

A recent Australasian College for Emergency Medicine (ACEM) study of 72 Australian and New Zealand hospitals revealed that people with severe mental illness often face long stays in emergency departments (EDs) while waiting for a hospital psychiatric bed (https://acem.org.au/News/Feb-2018/ACEM-mental-health-care-access-block.aspx). While only 4% of all ED presentations were for mental-health-related diagnoses, these patients accounted for 19% of those waiting for a bed and constituted 28% of those who experienced ‘access block’ (an ED length of stay [LOS] over 8 hours). Patients waited for up to 6 days in busy EDs, before being admitted.
Supply and demand
In 2014, the Organisation for Economic Co-operation and Development (OECD) warned policymakers that Australia’s relatively low number of hospital psychiatric beds increased the risks for people with severe mental illness of ‘worsening symptoms, more stays in emergency departments and more hospital readmissions’ (www.oecd.org/els/health-systems/MMHC-Country-Press-Note-Australia.pdf). In 2017, Australia remains near the bottom of the OECD rankings, being 27th of 36 OECD countries for hospital psychiatric beds.
ED access block represents a mismatch between the ‘demand’ for a bed and the ‘supply’ of beds (La et al., 2016). From the 1960s to the 1990s, Australia’s supply of hospital psychiatric beds was dramatically reduced from 280 to 40 beds per 100,000 population (Whiteford, 2017), which is below the required minimum for people with severe mental illness (50 public sector beds per 100,000 population), according to an expert consensus statement (Allison et al., 2018b).
More recently, state and territory governments restricted bed supplies during a period when hospital psychiatric admissions were rising faster than population growth (Figure 1): admissions doubled from 2005 to 2017, while the population grew by only 20%. Over the period, public sector adult beds were tightened by 5.5% (from 31 to 29 beds per 100,000 population), due to a reduction in older adult beds. Restricting the supply of beds when admissions were rising, increased the pressures on the EDs and inpatient LOS (Allison et al., 2018a, 2018b; Benjamin et al., 2018). Meanwhile, private sector hospital beds grew by 34% from 8 to 12 per 100,000 population. The substitution of private for public sector beds increased Australia’s socioeconomic disparities in accessing inpatient care.
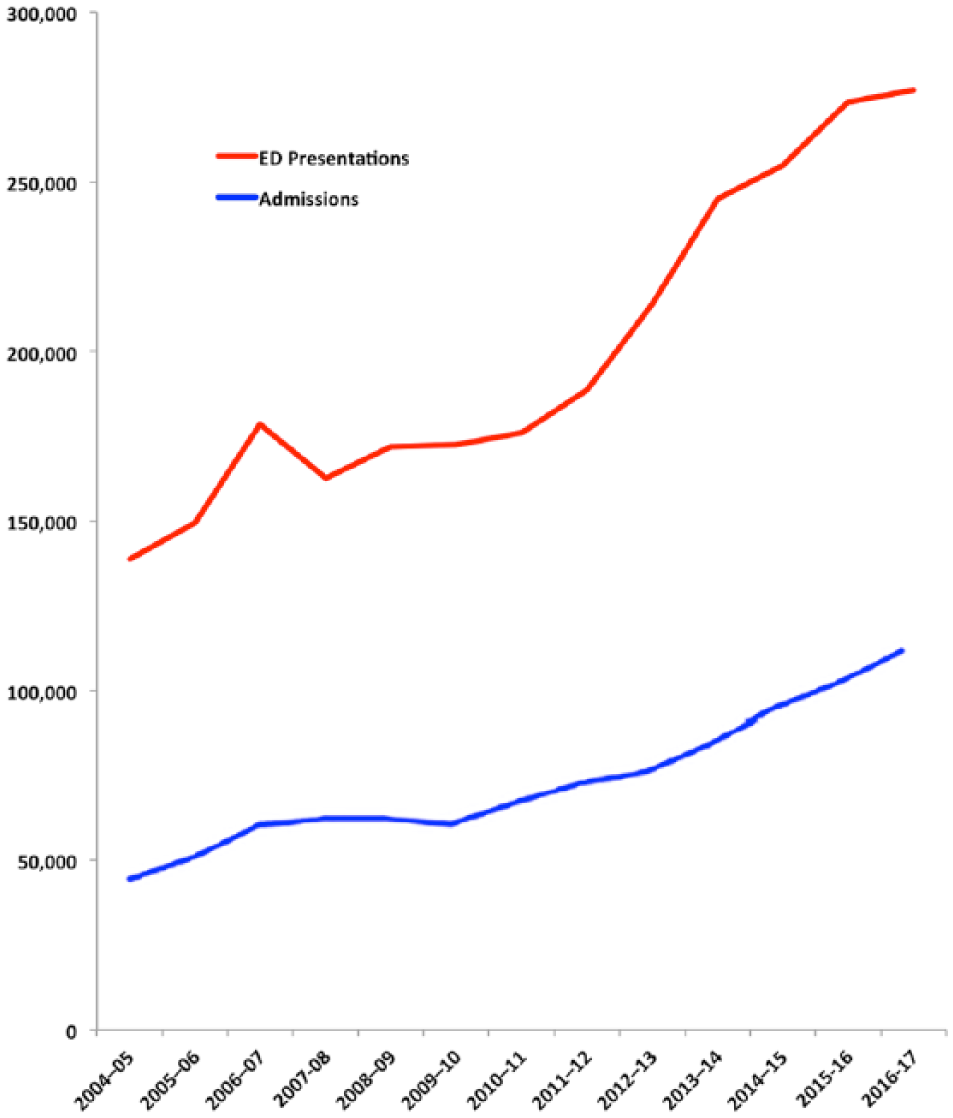
Psychiatric emergency department presentations and admissions to Australian public hospitals.
Significant investment in the community mental health continuum by federal, state and territory governments from 2005 to 2017 − prevention, primary care, early intervention, clinical psychology, pharmaceuticals and community services – failed to prevent the steep rise in ED presentations and admissions.
Figure 1 also illustrates the rising pressures on hospital psychiatrists, ED physicians and trainees. By 2017, the 90th percentile for ED LOS was 11.5 hours. These extended ED stays increased clinical risk, including iatrogenic worsening of the patient’s presenting illness, staff assault, physical restraint and suicide when ED access block obstructed a necessary admission (Allison et al., 2018a, 2018b; Benjamin et al., 2018).
Two planning methods
In 2015–2016, $2.4 billion was spent on mental health services in Australian public hospitals, $2.0 billion was spent on community services and $1.2 billion on Medicare benefits. The National Mental Health Service Planning Framework (NMHSPF) aims to minimise hospital spending and maximise the community continuum, using the available research evidence, heath service data and qualitative opinion (Whiteford, 2017). However, the NMHSPF lacks sufficient research evidence to confidently determine the relative resourcing needed by each component of a mental health service.
Given these gaps in our knowledge, state and territory governments should use a more direct method for estimating the required supply of beds. South Australia provides an instructive example of how to adjust the bed supply, based on hospital data, in order to reduce ED access block. Following an independent review condemning frequent and long periods of patient restraint in the EDs as a human rights violation (www.abc.net.au/news/2015-06-12/shackling-mental-health-patients-condemned-by-review/6543226), the South Australia Government mandated that ED LOS should never exceed 24 hours. Based on estimates drawn from hospital data (ED admission rates, inpatient LOS and the required bed days for various patient cohorts), total inpatient bed numbers (short-stay crisis, acute and forensic) were increased by 11% between 2014 and 2016. Average ED mental health LOS fell from 15 to 8 hours over the period (Allison et al., 2018b).
Conclusion
As the OECD indicated, Australia’s ED access block is related to our low supplies of hospital psychiatric beds, as well as the failure of the community service continuum to prevent the rapid rise in ED presentations and admissions. While continuing to try to find ways to minimise demand, policymakers must also explore the supply side. Australia needs a safe minimum number of public sector beds to prevent further chaos in our EDs (50 per 100,000 population). In the meantime, Australian clinicians should be made aware that these hospital workplace problems are directly related to our relative shortage of psychiatric beds by international standards.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.