
Abstract
Lone actor attacks like those at Port Arthur and Parklands High School Florida remain rare events though more frequent year by year. Psychiatrist are unlikely to see such killers either before or after an attack. What they do encountered on occasion are patients threatening to commit such a massacre. These threats need to be taken seriously primarily because they usually indicate significant distress but also because there is a remote chance they may try and act on the threat. Threats state an intention with the chances of enactment depending on the degree of commitment. Commitment is reflected in the level of preoccupation, plausibility, planning and preparation. Most threats have no commitment to act being an end in themselves motivated by such things as the desire to express an emotion, the wish to frighten, the attempt to manipulate others, though just occasionally they are a warning with some level of commitment to act. The assessment of threats to commit a massacre is considered in terms of the motivation and apparent commitment. Those who threaten mass killings also differ significantly from Lone Actor Attackers in their clinical pictures which further assists assessment of risk. There are some where doubts remain about the level of threat they present. The management of this group is discussed.
I intended to go and wreak great vengeance … I was hoping to kill at least seven or eight people, but unfortunately I didn’t get around to doing all of that. And I was hoping to be killed by one of your people. I didn’t get around to that either, so I fucked it up completely.
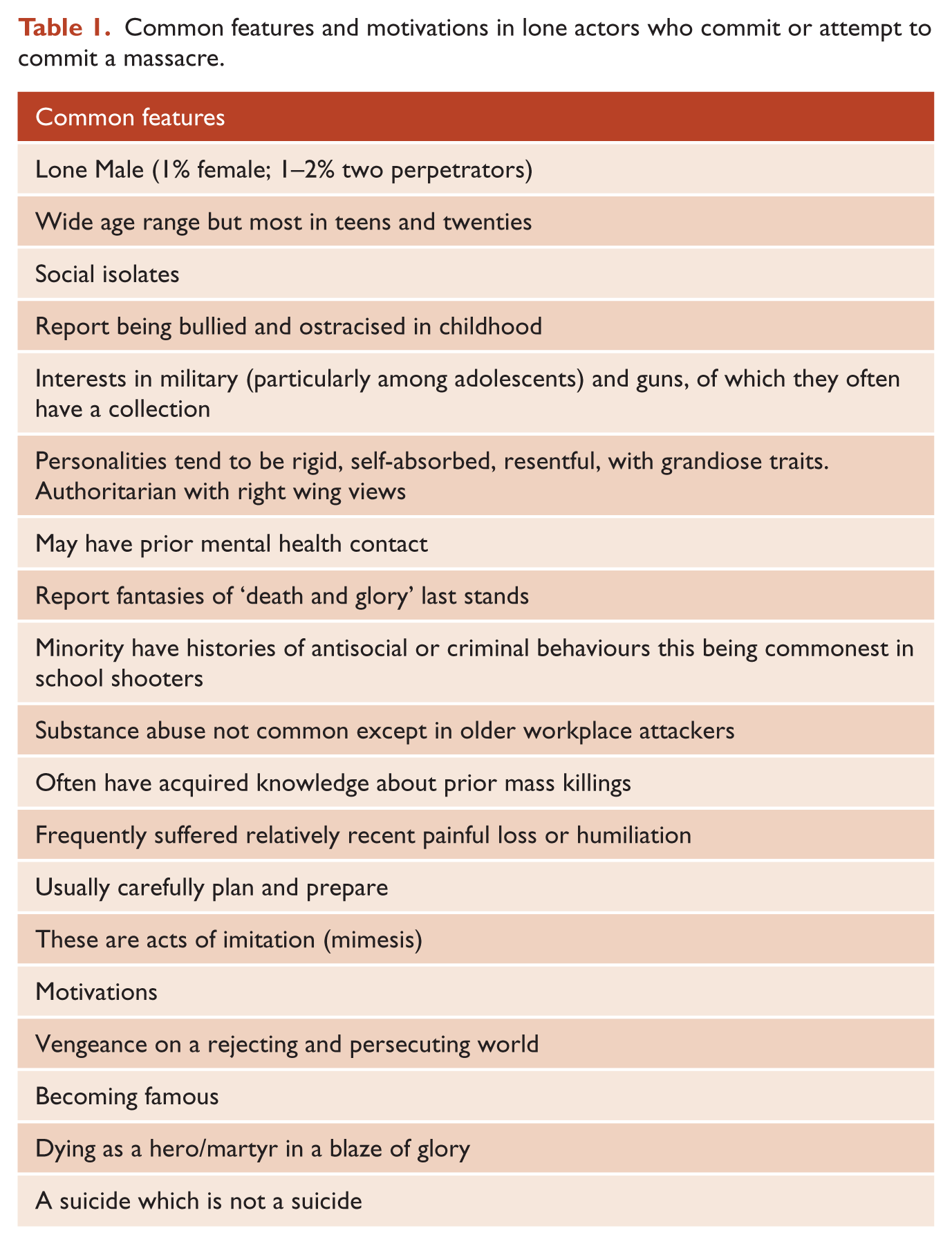
The paper of Haeney et al. (this issue) addresses school shootings. Events in which a person goes out with the intention of killing and maiming people, chosen largely at random, in a single continuous slaughter, was once rare in Western cultures. Sadly it is rapidly becoming all too common, and not just in the United States. These attackers have been given various names such as lone wolves, active shooters, and lone actors. The massacres can occur in public spaces, workplaces, and educational establishments, with some killers claiming political or religious motivations. The perpetrators of these massacres share many of the same characteristics irrespective of the chosen venue or claimed motivation (see Tables 1 and 2) (Mullen, 2004). The documents left behind and the statements of those who survive suggest nearly all intend to die among their victims, with some 70% succeeding.
Common features and motivations in lone actors who commit or attempt to commit a massacre.
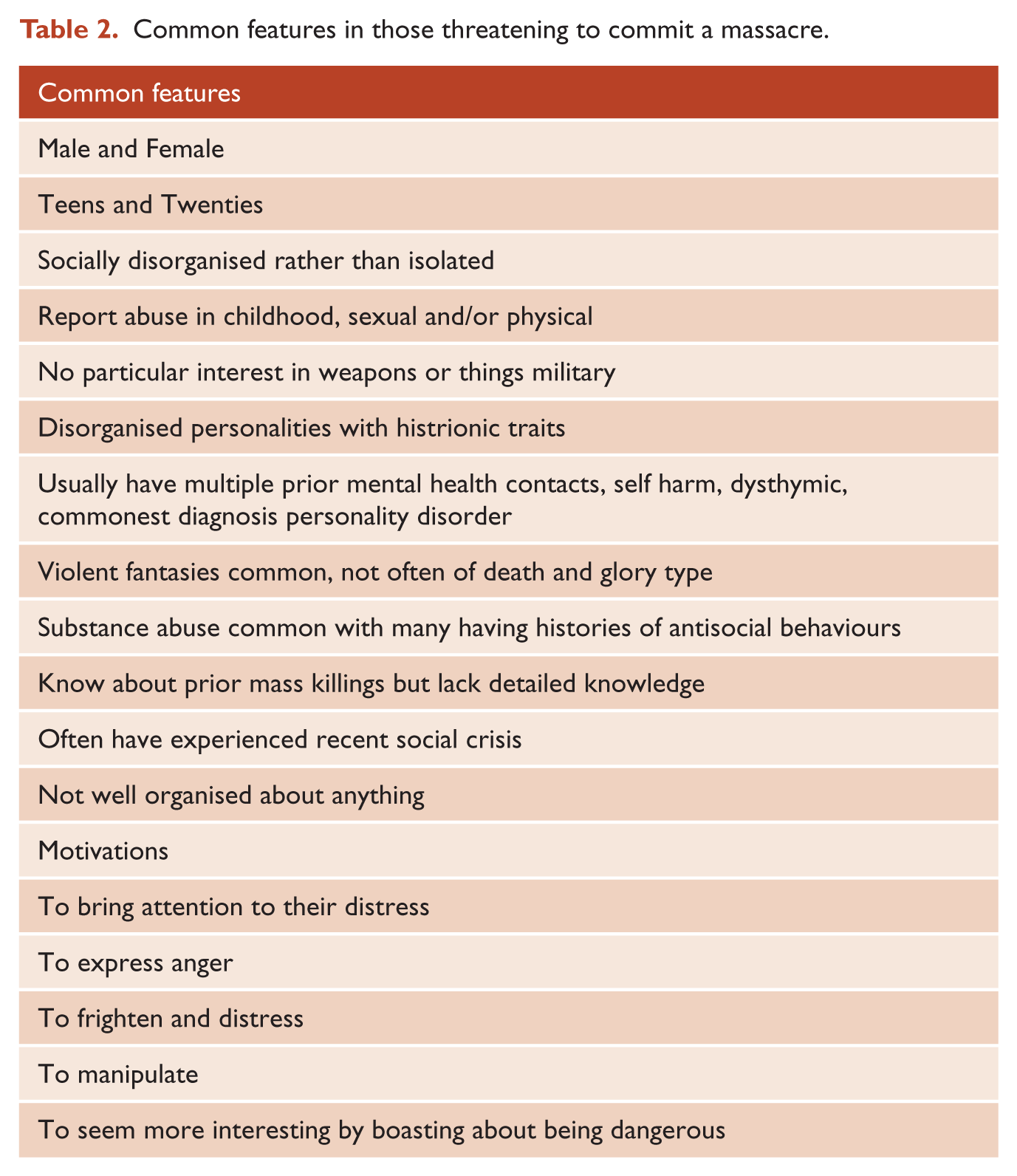
Common features in those threatening to commit a massacre.
The nature and extent of the psychopathology among lone actor killers is not easy to establish, in part because so few survive, in part because of the resistance of mental health professionals to releasing case notes, particularly in the United States, in part because of the political and legal discourses around these events which either want to blame mental disorder or claim wrongly that well-planned and executed attacks are incompatible with psychotic disorders. Some of the better studies suggest that around 40% had some form of prior mental health contact. The commonest diagnosis is depression though 10–15% of these killers probably had psychotic disorders (Gill et al., 2017).
Don’t panic, since there is only a remote chance of a psychiatrist encountering someone like the man quoted above who will go on to commit a massacre, but they may well see patients whose utterances seem to indicate a predisposition to act in this way. For each attack, there are probably hundreds, if not thousands, who threaten mass murder. We and our colleagues regularly saw such cases in our community forensic service. Such threats may be expressed directly or indirectly as well as in desires to emulate previous mass killers or communicating fantasies about such actions. The anxieties created by such utterances may be the reason for the referral or the issue may emerge in ongoing treatment. The threat is usually communicated in vague terms rather than as a specific threat to kill a named person or clearly defined group. There is usually an upswing in such threats after a widely reported massacre. The majority of those indicating they are considering committing a massacre are attempting to draw attention to their current distress. They are waving a very large red flag which should be difficult to ignore. As with threats of suicide, the clinician needs to explore not just the probability of acting on the implied threat but also the sources of the current distress and disturbance. The threat and the threatener must always be taken seriously, however, remote may initially seem the possibility of their acting, and however often they have made suicidal or homicidal threats in the past. A response which is dismissive or lacks appropriate concern amounts to a challenge to prove the threat is serious, which can risk precipitating a suicidal or homicidal rejoinder. Failure to take threats seriously also ignores the underlying desperation to which they often give voice.
Threats express intentions, but their enactment depends on the individual’s level of commitment. Commitment can be expressed through the level of preoccupation, plausibility, planning and preparation which accompanies the threat. In everyday life most threats to kill are an end in themselves with no attendant commitment to act. Threats can be expressions of feelings (Screamers), attempts to frighten (Shockers), to manipulate others (Schemer), but just occasionally they warn about real possibilities (Warren et al., 2014).
Lone actor mass killers have almost always spent long periods fantasising about violent last stands and dying in a blaze of glory. Threateners may also occasionally indulge in violent flights of fantasy but rarely of this type. Those who commit massacres often research prior mass killings through searches on the Internet and books. The Hoddle Street attacker had researched prior massacres in great detail, an American school shooter had gone on a pilgrimage to the site of a prior school massacre, the Munich shooter chose to honour his hero by launching an attack on the anniversary of the Utoya slaughter, and even the Port Arthur killer had named his parrot Rambo. Such preoccupations are uncommon among threateners. Actual massacres have usually been carefully planned and meticulously prepared including acquiring the weapons and skills in their use. The Aramoana killer had been practising his shooting and military tactics weeks prior to the attack, and even the female partner in the San Bernadino shooting had put aside her habitual hijab to practice at the local gun club. Lone actor massacres, particularly those in workplaces and high schools, can occasionally be hastily prepared or even impulsive. The commonest instrument used in mass casualty attacks is a gun, but knives can be used, as in the Tokyo attack which left 19 dead. Most troubling is the emergence of a script employing motor vehicles as instruments of mass murder, as the Nice, Berlin, New York City, London and Melbourne attacks tragically illustrate. It is rare to find a history of plausible preparation among threateners though some claim to have, or know how to acquire, guns. Such claims rarely stand up to scrutiny. All, however, have access to bladed instruments and motor vehicles so making threats to use these adds plausibility.
There are differences between the characteristics of most lone actor mass killers and those seen by professionals who threaten such behaviour, but there can be similarities (Table 2). Those who perpetrate lone actor attacks are almost all social isolates (offline, at least) who experience themselves as victims of injustice and rejection about which they harbour intense resentment. Threateners, though they also tend to see themselves as victims of a malevolent world, tend to hope, if not demand, that this change. Both groups tend to harbour suicidal intentions. Lone actor attackers are often rigid and obsessive combined with tendencies to grandiosity, whereas threateners tend to be disorganised and vacillating individuals with poor self-esteem. Threateners, unlike most attackers, often have histories of self-harm, of substance use, and of antisocial attitudes and behaviour. Unfortunately, most of the standardised instruments to estimate the risk of future offending would probably rate those who launch attacks as low-risk, whereas those who just threaten would be more likely to fall into the high or medium high-risk categories.
Attempts have been made to increase the recognition of those at risk of perpetrating a lone actor massacre by monitoring Internet traffic or, as in the United States, having publicity campaigns like ‘see something say something’ to increase reporting. This inevitably generates large numbers of false positives which may have played a part in the failure of the Federal Bureau of Investigation (FBI) to recognise and act on the threat presented by the Florida school shooter. In that case, there was probably scope to have at least removed the guns and even organised mental health and social support to this distressed and disturbed teenager who had recently lost his mother. There have also been attempts using retrospective analysis of actual lone actor attacks to try and discern what might have given warning. One such was the proposal of leakage. In reality, this amounts to little more than looking out for threats, and in any case, these threats are not leaks but usually cries for help interspersed with the occasional boast. What are leakages are the content of Internet traffic pertinent to a possible attack.
The focus on ascertainment of potential lone actor mass killers has tended to obscure the difficulties of assessing and managing such cases if and when they are recognised. The Virginia Tech killer offers a prime example. He had been recognised during his school years to be preoccupied with the possibility of committing a mass shooting. He had received counselling and psychiatric treatment which was believed to have improved the situation. At University, on more than one occasion he wrote essays which raised anxiety about his committing an attack. He was admitted compulsorily for a mental health assessment, but the psychologist who saw him did not consider he had a disorder justifying further detention. He was offered outpatient treatment but never attended and there was no follow-up. The University knowing both of the threats and of other disturbing behaviour offered counselling, which he declined. The decision to exclude him from the University was considered, but the institution generously decided to give him another chance. These decisions all seem to have been made in ignorance of his having acquired weapons including a semiautomatic rifle, though this may have occurred only shortly before the attack. In retrospect, this seems like a catalogue of errors, but at the time, there were severe limitations on what could have been done without his cooperation, combined with the understandable fear of inflaming the situation. The expulsion of the Florida school shooter did not prevent the massacre, and we can only hope it did not contribute. Making threats which are not directed at a specific individual or individuals is not an offence in most jurisdictions unless linked to terrorist ideologies. The law’s ability to intervene is therefore limited. In Australasia, there is no legally imposed duty to warn in these cases, unlike in child abuse, and given the almost universal lack of specificity it is unclear who you might warn. Conversely, you would be covered ethically and legally if you broke confidentiality to discuss the situation with appropriate colleagues or agencies. Compelling treatment is only possible if there is a reasonable case for the individual falling within the Mental Health Act. Removing guns is sometimes possible, but, at least in the United States preventing the acquisition of further weapons is not so easy. The best hope, in our opinion, comes from recognising these threats are not leaks but potentially cries for help. Why would loners make public their intentions if not in the hope that someone will help them avoid travelling down this path to the death of others and yourself?
The motivation of those who make threats to commit a massacre is usually obvious. The majority are distressed and disturbed people who, seeing no way out of their current dilemma, had been driven to consider suicide. Typically, they feel they have been failed by the mental health services who have not taken their despair seriously. Occasionally there are other reasons. One young man in treatment for schizophrenias when angered by a comment from his community nurse wrote a letter to the consultant threatening a massacre. Some simply want revenge, as with the young woman whose treatment was ended by her psychologist following a tantrum in which she trashed the office. She responded by writing a letter outlining her murderous plans, blaming the rejection, and of course sending a copy to the local newspaper. Another young man en route to becoming the school Dux confided his intention to come with a machine gun to slaughter his fellow pupils. He carefully chose someone guaranteed to rush immediately with the story to the teachers. In this case, he was attempting to manipulate the school and his parents into accepting his choice of future university course rather than fulfilling their high ambitions. The majority of such cases can be managed by general psychiatrists without necessarily involving forensic services, though an assessment by a forensic specialist may assist in sharing the burden. Buried among the relatively straightforward cases are those where the threat could be a warning and in which some evidence of a commitment to act may seem to be present. This type of presentation is probably best dealt with by the forensic mental health service.
The following case, a composite of several cases, illustrates this dilemma. A man was referred after revealing to his counsellor he had been thinking about committing a massacre. He gave a history of years of indulging in violent fantasies, often of the ‘death and glory’ type. He had acquired from the Internet and other research considerable knowledge about prior lone actor attacks. He had marked obsessional traits which had caused him difficulties in the work situation. He had a history of a prior suicide attempt. He expressed considerable resentment against a number of individuals and organisations who not only failed to recognise his manifest excellence but had exposed him to rejection and humiliation. His current mental state was marked by despair and despondency which he blamed on others. There was also evidence of anxiety with occasional panic attacks. He had considered possible venues for a massacre, but he would not identify the sites. He did not have any weapons but claimed he could acquire the guns. Clearly, this was an anxiety-provoking case. The only bright spot was when asked if he had made the threat in the hope of being stopped he responded ‘course I bloody did’. He declined the offer of admission but was agreeable to outpatient management.
The options for intervention in this case were limited. Technically, he had not committed an offence. He denied possessing guns. He was a disturbed and distressed man, but it would have been a stretch to admit him under the Mental Health Act. This might still have occurred had it not been considered that all that would have been achieved was a brief period in hospital and the almost certain loss of any future cooperation. In the event, he was managed through our community service. He was already on sick leave and he had not specified his workplace as a possible target. The short-term aim was first to engage him in treatment on the basis of assisting him in resisting his suicidal and homicidal intentions, and second to persuade him to take a selective serotonin reuptake inhibitor (SSRI) antidepressant which he had previously declined. He was seen by both a psychiatrist and a clinical psychologist initially twice weekly with additional sessions available at his request. The longer-term aim was to work on overcoming his social isolation and improving his capacity to cope with both his despondency and the limitations created by his obsessional personality. He is still seen monthly. There has been no recurrence of either suicidal or homicidal ideas.
Fixated Threat Assessment Centres (FTAC) also offer a potential resource in dealing with the cases where a real probability seems to exist of an attack. FTACs exist in Queensland, New South Wales and Victoria, with an FTAC in Canberra for high office holders. FTAC capabilities are also being developed in other Australian states and territories as well as New Zealand. These joint police mental health organisations were first developed in the United Kingdom in response to the findings of a research team, which included the authors, on those who stalked, threatened, or attempted to intrude upon or attack members of the British Royal Family and parliamentarians (James et al., 2010; Mullen et al., 2009). Some 70% of these people had psychotic disorders, though most were either unknown to, or had fallen out of contact with, services. In most cases, establishing and maintaining mental health treatment put an end to the problematic behaviours. This is a mental health solution to a security threat. This approach has been expanded to include potential lone actor terrorists with overt mental disorders (Pathé et al., 2018), based on a robust body of research indicating that lone actor terrorists and other forms of lone actor attackers have high levels of psychotic and non-psychotic disorders (Gill, 2015). Given the many similarities between lone actor terrorists and other forms of lone actor attackers, the FTACs are well placed to assist and should be involved whenever the threat is combined with claims of a political or religious justification.
Conclusion
Lone actor massacres are rare events which have until recently almost always involved guns, but a script is emerging where vehicles and even bladed weapons are the instruments of mass murder. Threats to commit a massacre are relatively common. Such threateners usually have histories of mental health problems, and their initial assessment often falls to psychiatrists. Most are disturbed and disordered people seeking to dramatise their plight. They need to be taken seriously and provided with care and support. A thorough assessment can usually exclude almost any substantial chance of their acting on the murderous threat, but just occasionally doubts remain. In these cases, it is probably wise to involve forensic mental health services who may in turn seek the assistance of FTAC capabilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.