
Abstract
Objective:
Individuals vary in how they respond to bereavement. Those who experience poor bereavement outcomes often report symptoms from more than one diagnostic category. This study sought to identify groups of individuals who share similar patterns of prolonged grief disorder and posttraumatic stress disorder symptoms to determine whether these profiles are differentially related to negative appraisals thought to contribute to prolonged grief disorder and posttraumatic stress disorder symptomatology.
Methods:
Participants were 185 bereaved adults. Latent class analysis was used to identify subgroups of individuals who showed similar patterns of co-occurrence of prolonged grief disorder and posttraumatic stress disorder symptoms. Multinomial regression was used to examine the extent to which appraisal domains and sociodemographic and loss factors predicted class membership.
Results:
Latent class analysis revealed three classes of participants: a low symptom group, a high prolonged grief disorder symptom group, and a high prolonged grief disorder and posttraumatic stress disorder symptom group. Membership of the prolonged grief disorder group and prolonged grief disorder and posttraumatic stress disorder group was predicted by higher mean negative self-related appraisals. Demographic and loss-related factors did not predict group membership.
Conclusion:
These findings have implications for understanding co-occurrence of prolonged grief disorder and posttraumatic stress disorder symptoms following bereavement. Findings are consistent with theoretical models highlighting the importance of negative self-related beliefs in prolonged grief disorder.
Introduction
Prolonged grief disorder (PGD; or complicated grief or persistent complex bereavement disorder) is a potentially debilitating consequence of bereavement experienced by 7–10% of bereaved individuals (Lundorff et al., 2017; Maciejewski et al., 2016; Nielsen et al., 2017). The syndrome is characterised by intense yearning for the deceased, distress at the lost relationship, disbelief, difficulties with acceptance, avoidance of reminders, a sense that life now lacks meaning or purpose, self-identity confusion, emotional numbness, bitterness, loss of trust and a difficulty re-engaging with life, that is ongoing for more than 6 months, and is associated with functional impairment (Maercker et al., 2013; Prigerson et al., 2009). PGD has been shown to represent a distinguishable syndrome that is linked with a range of negative mental and physical health outcomes independent of bereavement-related depression or anxiety (Barnes et al., 2012; Bonanno et al., 2007, 2010a; Golden and Dalgleish, 2010; Maciejewski et al., 2016; Shear et al., 2011). PGD also responds better to grief-targeted treatments than treatments for depression (Shear et al., 2005, 2016).
There is, however, significant variation in how people respond to bereavement. While some people experience enduring, disabling levels of distress, many experience symptoms that gradually decline, and many experience little or no disruption in functioning (Bonanno and Kaltman, 2001; Galatzer-Levy and Bonanno, 2012; Maccallum et al., 2015). Moreover, syndromes other than PGD are observed following bereavement (e.g. major depressive disorder, posttraumatic stress disorder and other anxiety disorders), and co-morbidity with PGD is common (Shear et al., 2011; Simon et al., 2007). This has led to increased interest in understanding how co-morbid symptoms present in bereaved individuals. Are there subgroups of individuals who present with similar patterns of symptom co-occurrence? and if so, do these subgroups share characteristics that have implications for treatment (e.g. Djelantik et al., 2017; Maccallum et al., 2017; Nickerson et al., 2014)?
There is growing evidence that persistent negative thinking about global themes including the self, life, the world and the future is associated with psychopathology following loss (Boelen et al., 2006a, 2016; Boelen and Van Den Hout, 2008; Lobb et al., 2010; Nolen-Hoeksema, 2003). However, different appraisal domains are thought to relate to different symptom domains: for example, for PGD, emphasis has been placed on negative self-related beliefs, including catastrophic beliefs about grief reactions (Boelen et al., 2006a, 2010; Boelen and Van Den Hout, 2008; Golden and Dalgleish, 2012); whereas for posttraumatic stress disorder (PTSD), emphasis has been placed on the individual’s beliefs about ongoing threat to safety (Ehlers and Clark, 2000). The extent to which subgroups of individuals showing different patterns of PGD and PTSD symptom co-occurrence are characterised by different types of negative appraisals could have important treatment implications but has yet to be explored.
One way to address this issue is using latent class analysis (LCA). LCA seeks to identify homogeneous, qualitatively distinct subgroups of individuals based on similar patterns of responding across a set of common indicators (i.e. symptoms). Boelen et al. (2016) recently reported the results of an LCA examining symptoms of PGD and depression in a sample of individuals bereaved by a traumatic loss. This study identified three subgroups, or classes of participants, a class characterised by the presence of PGD and depressive symptoms, a class characterised by PGD symptoms only, and a class characterised by a low presence of either symptom group. Consistent with the notion that appraisal content may be relevant to symptom profiles, they found different appraisal domains predicted membership of different classes. Negative cognitions about the self, life and grief predicted membership of the combined class, and negative cognitions about grief predicted membership of the PGD only class. Unfortunately, PTSD symptoms were not available for this sample. Studies that have used LCA to explore subgroups based on symptoms of PGD and PTSD in bereaved samples (e.g. Djelantik et al., 2017; Nickerson et al., 2014) have identified separate classes within their samples. For example, Nickerson et al. (2014) identified one class characterised by the presence of PGD symptoms, one class characterised by the presence of PGD and PTSD symptoms, one class characterised by the presence of PTSD symptoms only and a fourth class characterised by a low presence of any symptoms. Furthermore, these analyses have identified socioeconomic and loss characteristics predictive of group membership, for example, both Nickerson et al. (2014) and Djelantik et al. (2017) found that violent cause of death was associated with membership of a combined PGD/PTSD class. However, studies have yet to examine whether appraisal domains differentially predict membership of classes based on PGD and PTSD symptoms. Advancing our understanding of the relationship between the co-occurrence of symptoms and modifiable predictors has significant clinical relevance.
Accordingly, this study sought to extend on previous work by applying LCA to examine the relationship between post-bereavement appraisal dimensions and the co-occurrence of PGD and PTSD symptomatology. We used the Post Traumatic Cognitions Inventory (PTCI; Foa et al., 1999) to assess appraisal domains. The PTCI comprises three subscales that assess negative beliefs about the self, negative beliefs about the world, and beliefs relating to self-blame for the event. It has been shown to differentiate between individuals with and without a diagnosis of PTSD (Beck et al., 2004; Foa et al., 1999) and is sensitive to change following cognitive behaviour therapy for PGD (Bryant et al., 2014). We expected that the LCA would identify subgroups of bereaved individuals characterised by different symptom profiles. Specifically, we expected a class characterised primarily by the presence of PGD symptoms, a class characterised primarily by the presence of PTSD symptoms, a class characterised by the presence of both PGD and PTSD symptoms, and a class characterised by the absence of symptoms (Low). Furthermore, we expected that classes characterised by PGD symptoms would score highly on negative beliefs about the self, compared to the low symptom group. In contrast, because PTSD is associated with schema focused on appraisals of a dangerous world and blame, we expected classes with a high prevalence of PTSD symptoms would be characterised by increased negative appraisals about the world and self-blame. Furthermore, as previous studies have identified sociodemographic and loss-related variables that differentially predict class membership, we included these in our analyses. We expected that individuals who had experienced a traumatic loss would be more likely to be members of the class characterised by the presence of PGD and PTSD symptoms.
Method
Participants and procedures
The sample comprised 185 bereaved individuals (83.2% female) with mean age of M = 50.12 (standard deviation [SD] = 13.85) years. Participants were recruited through advertisements placed in major Sydney newspapers and online recruitment websites seeking bereaved individual interested in participating in a grief treatment trial or research project focused on understanding adaption to bereavement. All participants attended a clinical interview and completed the self-report questionnaires. Participant characteristics are presented in Table 1. In terms of relationship to the deceased, participants had lost a spouse (31.9%), parent (35.7%), child (21.6%), sibling or other close relative (10.8%). In terms of the nature of the death, 78.9% of deaths were the result of medical conditions, and 21.1% were the result of an accident, suicide or homicide. Mean time since loss was M = 3.55 (SD = 3.28) years. Approximately 38% (n = 66) of participants meet diagnostic criteria for PGD according to the PG-13 (measure) (Prigerson et al., 2009). Approximately 30% (n = 55) of participants reported re-experiencing, avoidance and hyperarousal symptoms consistent with Diagnostic and Statistical Manual of Mental Disorders (6th ed.; DSM-IV) diagnostic criteria for PTSD. This research was approved by the Human Research Ethics Committee of Western Sydney Local Health District (HREC/12/WMEAD/99). Participants provided written informed consent.
Participant characteristics.
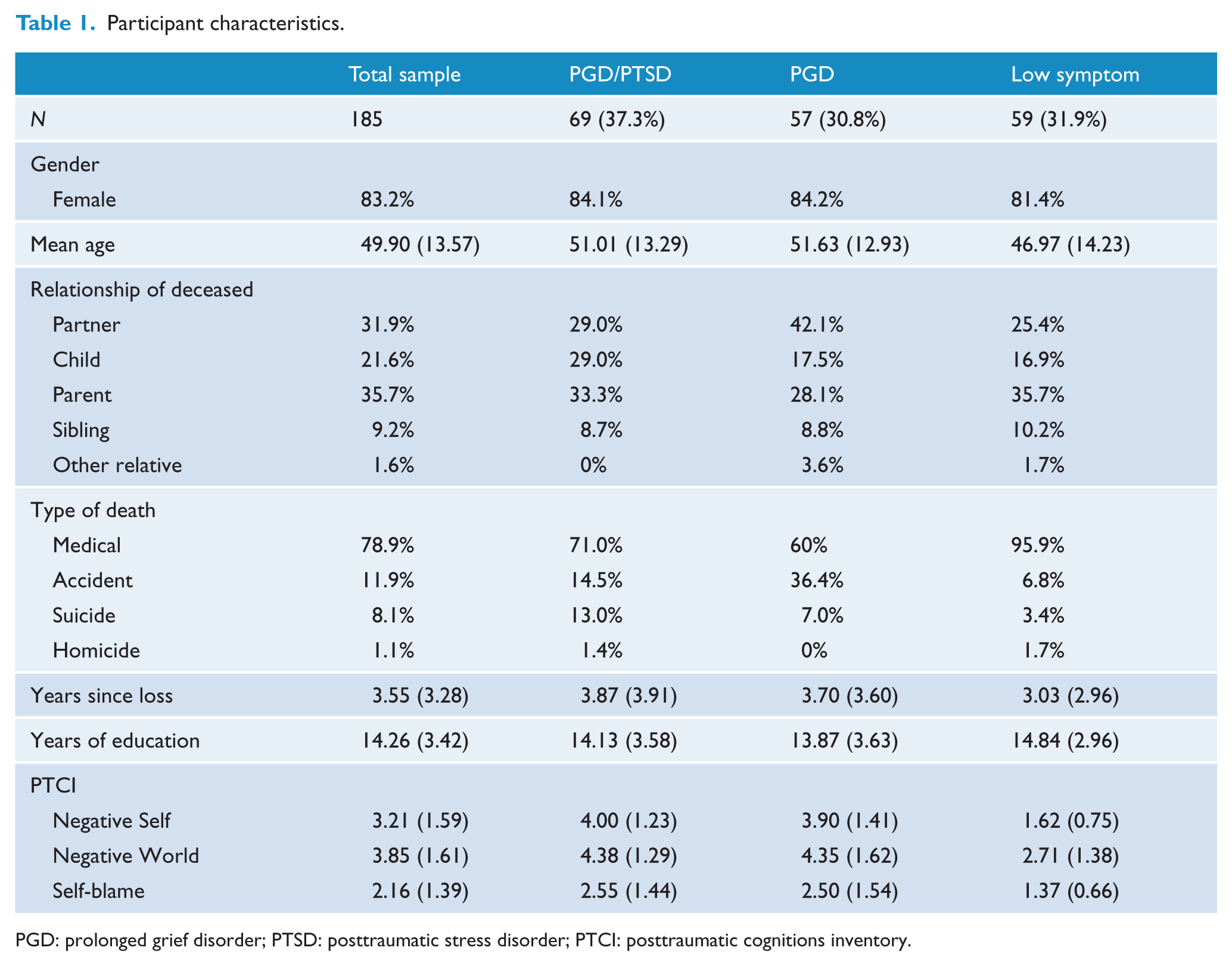
PGD: prolonged grief disorder; PTSD: posttraumatic stress disorder; PTCI: posttraumatic cognitions inventory.
Measures
Prolonged grief assessment
Prolonged grief was assessed using a semi-structured interview based on the PG-13 (Prigerson et al., 2009). The PG-13 assesses for the presence of yearning, emotional distress at the lost relationship, difficulty accepting the death, shock, avoidance of reminders, numbness, bitterness, difficulty engaging in life, identity disturbance, a sense of purposelessness and meaninglessness, and functional impairment. Clinical interviews were conducted by Master’s level trained clinical psychologists. Items were scored by clinician’s on a 5-point scale (1 = not at all, 5 = several times a day/overwhelmingly). A dichotomous indicator variable for each symptom was derived for this study (symptom absent/present). A symptom was considered to be present if it was rated as ⩾3 (at least once a week). This threshold is consistent with comparable studies as reflecting presence of a symptom (Boelen et al., 2016; Djelantik et al., 2017; Nickerson et al., 2014). For the purpose of the LCA, we did not include the item assessing functional impairment because this item relates to the impact of the other items on the person’s functioning rather than representing an individual symptom.
Clinicians Administered PTSD Scale-1
The Clinicians Administered PTSD Scale-1 (CAPS-1) is a structured clinical interview that indexes the 17 symptoms described in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) PTSD criteria (American Psychiatric Association (APA), 1994; Blake et al., 1995). For the purpose of the assessment, the reference event was the death event of the loved one, rather than general events involving the deceased and their absence. All participants were assessed on the CAPS-1 irrespective of whether the circumstances of the death met PTSD diagnostic Criterion A for a traumatic event (APA, 1994). Symptom presence was assessed in the preceding month using a 5-point scale in terms of frequency and intensity. To meet criteria for a symptom to be present, the symptoms must have a frequency of ⩾1 (on a 0–4 scale) and an intensity of ⩾2 (on a 0–4). These dichotomised scores were entered into the LCA.
PTCI
The PTCI is a 36-item self-report questionnaire comprising three subscales: (a) negative cognitions about the self (21 items; for example, I can’t trust that I will do the right thing, If I think about the event I will not be able to handle it); (b) negative cognitions about the world (7 items; for example, I can’t rely on other people, The world is a dangerous place); and (c) self-blame (5 items; for example, The event happened because of the way I acted; Foa et al., 1999). Items are rated on a 7-point scale (1 = totally disagree, 7 = totally agree). The scale demonstrates good internal consistency, discriminant validity and test–retest reliability (Foa et al., 1999). Alpha coefficients for the subscales and the total scale in the current sample were Negative Self α = 0.97, Negative World α = 0.92 and Self-blame = 0.85, Total scale α = 0.97.
Statistical analysis
LCA was used to model symptoms of PG and PTSD using Mplus v.7 with full maximum likelihood estimation. LCA aims to identify the smallest number of unobserved classes that adequately accounts for observed associations between symptoms in the data. LCA assigns individuals with similar symptom profiles to the same class. It is an iterative process. First, the most parsimonious 1-class model is fit, then successive models, increasing in class number are fit to the data to determine the optimal number of latent classes. In this analysis, latent classes were identified on the basis of 11 dichotomous indicators of PGD and 17 dichotomous indicators of PTSD symptoms. We assessed comparative model fit using the following indices: sample size–adjusted Bayesian information criterion (SS-BIC), the Akaike information criterion (AIC) entropy and Lo–Mendell–Rubin test (LRT). Final model selection was based on overall model fit, interpretability and parsimony (Nylund et al., 2007).
To assess predictors of class membership, we conducted multinomial logistic regression analyses in SPSS version 23. Due to the potentially large number of predictors, we first examined the extent to which sociodemographic and variables predicted class membership using one-way analysis of variance (ANOVA) and chi-square analysis. We also examined class differences in appraisals using one-way ANOVA. Next, we entered significant predictors in a multinomial regression to examine the extent to which variables continued to predict membership controlling for shared variance among predictors. For the purpose of these analyses, we created several dummy coded variables. Relationship of the deceased was dummy coded as spouse versus other, parent versus other, and child versus other. The nature of the death was recoded as medical or other (collapsing across accident, suicide and homicide).
Results
Table 1 presents participant characteristics, loss-related variables and mean appraisal scores for each of the LCA classes. Table 2 presents the fit indices for the LCA. Based on fit indices and interpretability of class solutions, a three-class solution was judged the optimal solution. The four-class solution yielded a slightly lower SS-BIC and AIC; however, the non-significant Lo–Mendell–Rubin test indicated that this model failed to fit the data significantly better than a three-class model. This solution comprised a combined PGD/PTSD class, a PGD only class and a Low symptom class. Conditional probabilities of symptom presence for the three-class solution are displayed in Figure 1. Values greater than 0.60 were considered to represent a high probability that the symptom was present in the class (i.e. 60% likelihood), values between 0.15 and 0.59 a moderate probability, and values below 0.15 were considered to represent a low probability that the symptom was present in the class (Nickerson et al., 2014).
Goodness-of-fit statistics for 1–5 class solutions.
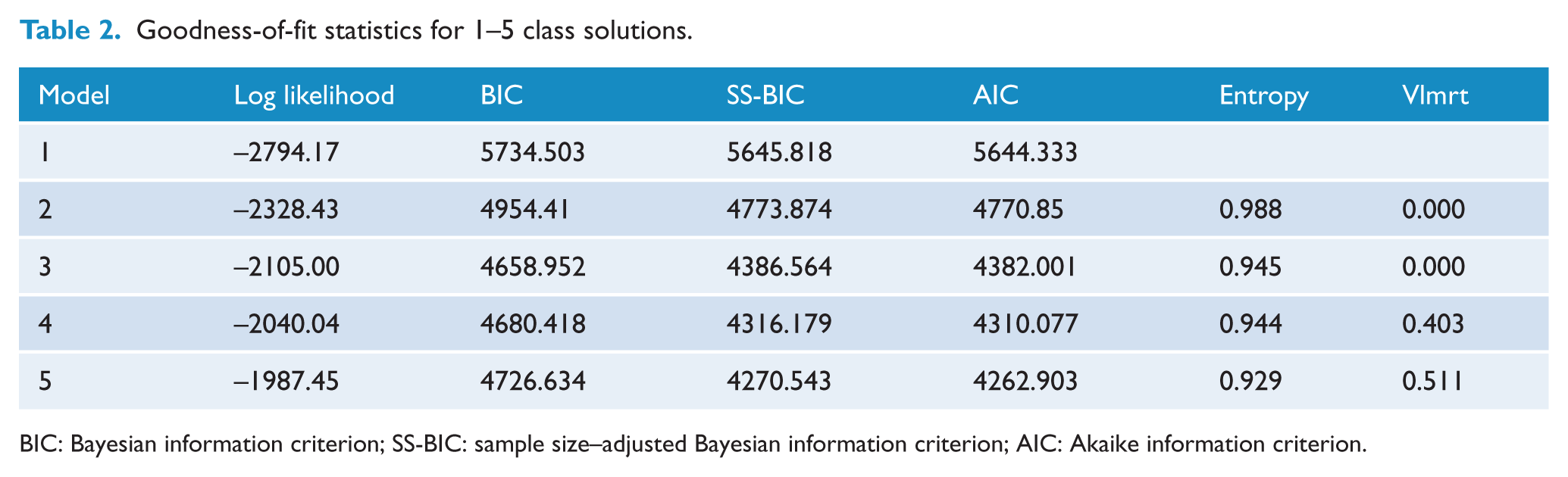
BIC: Bayesian information criterion; SS-BIC: sample size–adjusted Bayesian information criterion; AIC: Akaike information criterion.
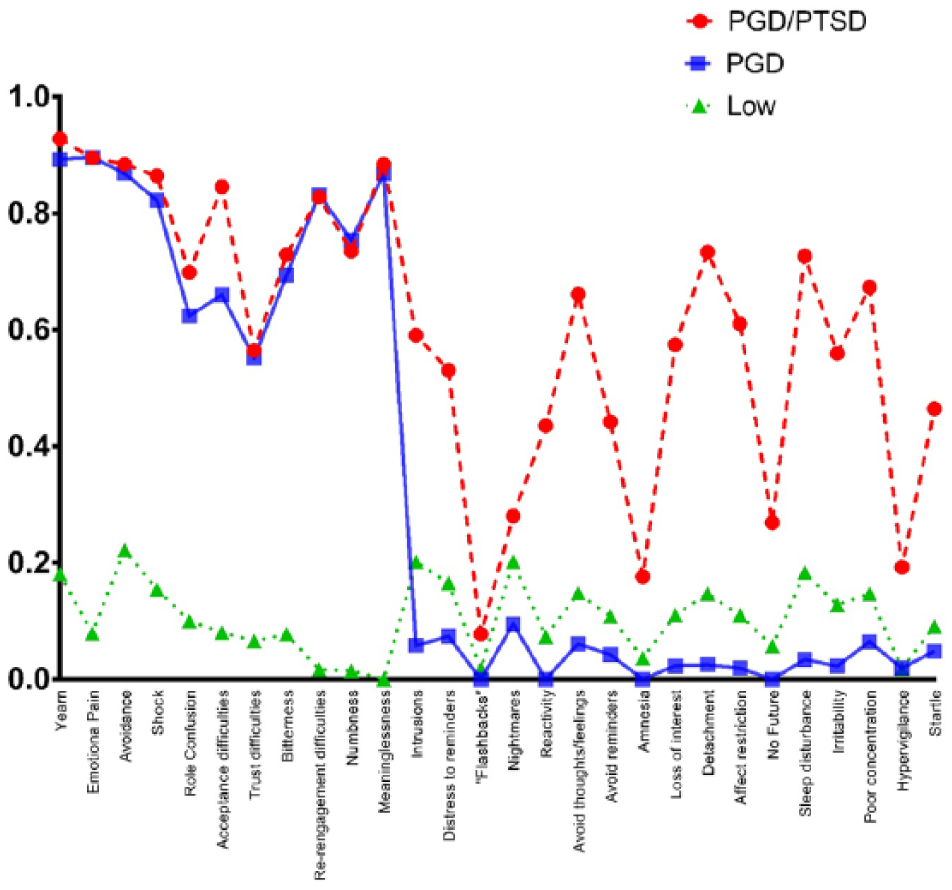
Estimated symptom prevalence for 3-class solution.
As can be seen in Figure 1, the PGD/PTSD class evidenced a high probability of the presence of all PGD symptoms. Trust difficulties, the least prevalent PGD symptom fell just below the high probability threshold. In terms of PTSD symptoms, this group had a high probability of avoidance of thoughts, feelings and conversations, interpersonal detachment, restricted affect, sleep disturbance, and concentration difficulties, and moderate probabilities for intrusive thoughts, distress to reminders, physiological reactivity, avoidance of situations, loss of interest in activities, sense of a foreshortened future, irritability and increased startle response. The probability of flashbacks, hypervigilance and amnesia fell at the low end of the moderate range (<0.20 probability). In contrast, the PGD only class had a high probability of PGD symptoms only; again, the lowest item, trust difficulties, fell just below the high probability threshold. The Low class had low probabilities for most PGD and PTSD symptoms.
Chi-square analysis indicated no significant differences between classes in terms of gender (p < 0.89) or relationship of the deceased (spouse vs other [ p < 0.13], child vs other [ p < 0.17], parent vs other [ p < 0.12]). Nature of the death, medical circumstances compared to accident, suicide or homicide, approached significance (χ2 = 5.60, p < 0.062), with a trend towards the low symptom group being more likely to have experienced a medical loss. A series of one-way ANOVAs indicated that the classes did not differ in terms of age (p < 0.13), years since loss (p < 0.41) or years of education (p < 0.35). There were, however, significant differences between classes on each of the PTCI subscales: Negative Self (F(2, 181) = 78.80, p < 0.001), Negative World (F(2,182) = 26.61, p < 0.001) and Self-blame (F(3, 183) = 16.28, p < 0.001). Follow-up testing indicated that the Low class scored significantly lower than the PGD and PGD/PTSD class on each subscale; the PGD and PGD/PTSD classes did not differ significantly from one another.
Next, we conducted a multinomial logistic regression to examine the extent to which these variables were significant predictors of class membership when accounting for any shared variance. Due to the near significant result for nature of the loss, and potential relevance of this factor for PTSD, we included this variable as a predictor in the model. When appraisals were not included in the model, death by accident, suicide or homicide was a significant predictor of membership of the PGD/PTSD class compared to the Low class (B = –1.11, standard error [SE] = 0.48, odds ratio [OR] = 0.33, p < 0.02, 95% confidence interval [CI] = [0.13, 0.85]). However, it was no longer a significant predictor when appraisals were included in the model. Results of the full model are presented in Table 3. In this table, the PGD only class serves as the reference class. Negative self-related appraisals was the only significant predictor of class membership when all predictors were included in the model. Compared to the PGD class, the Low class had a significantly lower mean level of negative self-related appraisals. This variable did not differentially predict membership PGD/PTSD class compared to the PGD class. To examine differential predictors of the Low compared to PGD/PTSD class, we repeated the analysis with the Low class as the reference class. Consistent with the previous results, higher mean negative self-appraisals significantly predicted membership of the PGD/PTSD (and PGD) compared to the Low class (B = 2.40, SE = 0.43, OR = 11.01, p < 0.000, 95% CI = [4.74, 25.58]).
Multinomial logistic regression predicting class membership.
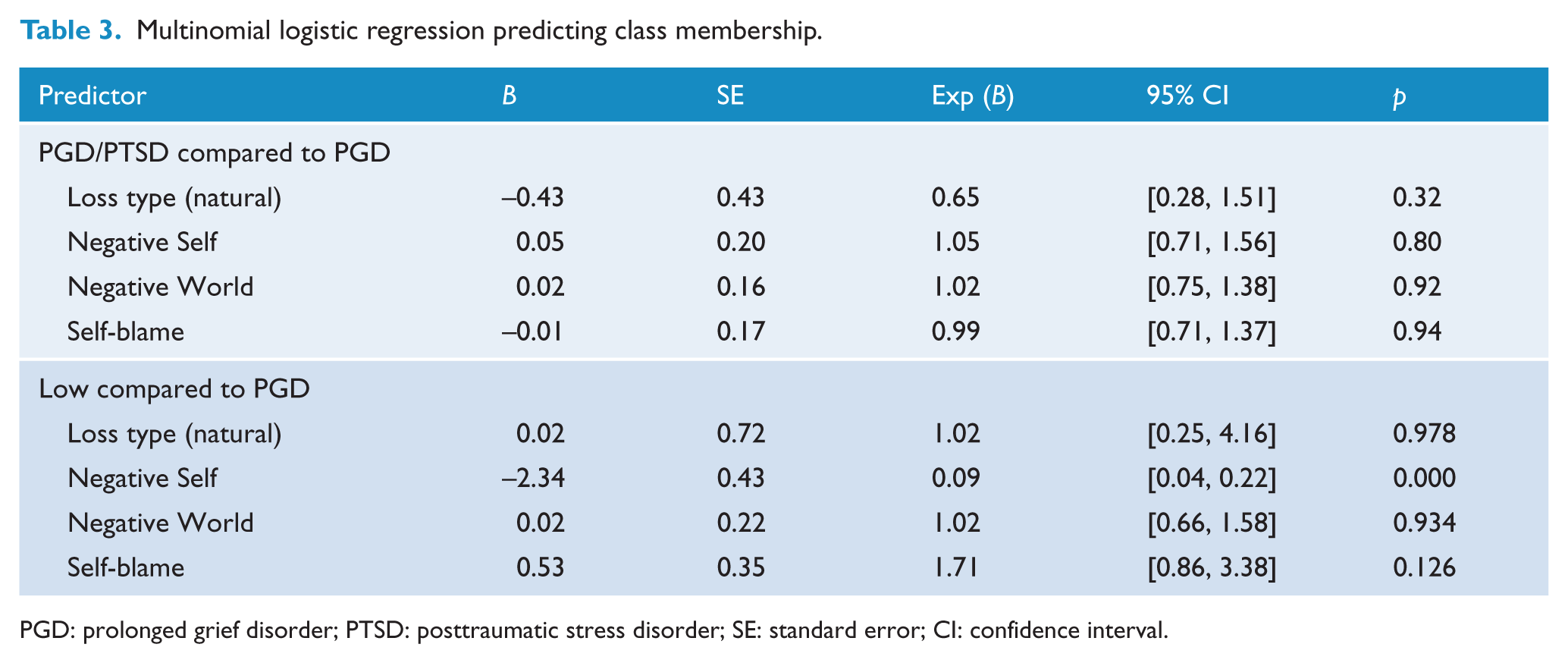
PGD: prolonged grief disorder; PTSD: posttraumatic stress disorder; SE: standard error; CI: confidence interval.
Discussion
This study examined the extent to which negative appraisals were associated with PGD and PTSD symptoms in a sample of bereaved individuals using an LCA approach. We identified three subgroups of participants: a PGD only class, a combined PGD/PTSD class and class with a low probability of any symptoms. Both the PGD and PGD/PTSD classes endorsed negative self-related cognitions, negative world-related cognitions and self-blame cognitions to a greater extent than the Low group. However, only negative self-related cognitions (e.g. I am inadequate, If I think about it I will lose control) uniquely predicted class membership: compared to the Low class, endorsement of greater negative self-related cognitions was a predictor of PGD and PGD/PTSD class membership. Endorsement of negative self-related cognitions did not differentiate the PGD from the PGD/PTSD class. Overall, these findings are consistent with previous studies that found a link between negative self-related beliefs and PGD symptomatology (Boelen et al., 2010, 2016; Golden and Dalgleish, 2012).
A failure to update one’s sense of self to accommodate the reality of the loss is a central feature of theoretical models of PGD (Boelen et al., 2006b; Maccallum and Bryant, 2013; Shear and Shair, 2005). Negative self-related appraisals are thought to play a key role in this process. Maccallum and Bryant (2013) proposed that the degree to which the bereaved person’s self-identity is dependent on, or merged with the deceased, represents a vulnerability factor for the development of PGD symptomatology, having implications for how individuals subsequently evaluate their worth as a person without their loved one, and their ability to cope with the reality of loss. Beliefs about an inability to cope without the deceased are thought to provoke attempts to avoid the reality of the loss (see also Boelen et al., 2006b; Stroebe et al., 2010). Negative self-related beliefs are also hypothesised to interfere with the person’s participation in adaptive activities, which may in turn provide alternative views of the self and assist them in accommodating the loss and developing new sources of meaning.
Appraisal domains did not differentially predict membership of the PGD and PGD/PTSD classes. Our LCA findings were largely consistent with results of two previous LCAs that have examined grief and PTSD symptom profiles among bereaved populations (Djelantik et al., 2017; Nickerson et al., 2014); however, in contrast to Nickerson et al. (2014), we did not observe a PTSD only class. Both symptomatic classes in this analysis were characterised by high probability of the presence of PGD symptoms. One possibility for the lack of differential prediction of PGD and PGD/PTSD classes is that appraisal domains do not differentiate PGD and PTSD symptom clusters. Alternatively, it may be the case that appraisals predictive of the presence of PGD symptoms were more dominant. This study examined the extent to which appraisals about the self and the world were predictive of symptomatology as these have been the focus of much empirical and theoretical investigation (see Boelen et al., 2006a, 2006b; Maccallum and Bryant, 2013). Future research may identify additional relevant appraisal domains.
In terms of PTSD symptoms, although some symptoms had a high probability of being present in the PGD/PTSD class, others had a relatively low probability of presence. Specifically, acting or feeling as if the loss were happening again (‘flashbacks’), an inability to recall aspects of the loss, hypervigilance, and sense of a foreshortened future had low probabilities. Amnesia typically has low endorsement and so this finding is not surprising (Breslau et al., 2005). The relatively low level of endorsement of ‘sense of a foreshortened future’ may be somewhat surprising given the observed difficulties individuals with PGD have in envisaging events in the future in a specific manner (Maccallum and Bryant, 2011; Robinaugh and McNally, 2013). However, this item refers to a sense that life could end at any moment, rather than a difficulty experiencing purpose or meaning associated with the future, and specifically excludes suicidal thoughts; it is worth noting that this item has been removed from Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). The low prevalence of hypervigilance indicates that the PGD/PTSD class was not overly characterised by a fear for their own safety. These findings are consistent with models that argue PGD is not characterised by the fear networks that underpin PTSD (Maccallum and Bryant, 2013; O’Connor et al., 2008). However, it is important to recognise that the symptom clusters derived by LCA do not equate to diagnostic categories, simply the likelihood that symptoms are present. As we were interested in patterns of symptom co-occurrence, we assessed PTSD symptoms in response to the death event, without requiring that the death event met criteria for a Criterion A trauma as defined by DSM (APA, 1994). The absence of a PTSD only class is most likely due to the high frequency of death by illness or medical conditions in our sample. Importantly, however, our findings suggest that trauma symptoms may be present in some bereaved individuals who also show PGD symptoms without necessarily reflecting the presence of the hallmark safety concerns observed in PTSD.
Boelen et al. (2016) found that catastrophic misinterpretations of grief reactions distinguished self-reported PGD and PGD/Dep from the low group and that greater endorsement of negative cognitions about the self and life predicted membership of the PGD/Dep from the PGD alone. The extent to which these groups had co-morbid PTSD symptomatology is unknown. Our analysis examined clinician-rated PGD and PTSD symptomatology. However, as co-morbidity with depression is a feature of both syndromes (Rytwinski et al., 2013; Simon et al., 2007), we cannot rule out an influence of depression on our findings. In contrast to previous studies (Djelantik et al., 2017; Nickerson et al., 2014), we found no sociodemographic predictors of class membership. Class membership was not predicted by gender, age, years of education, time since loss or relationship of the deceased. Consistent with Nickerson et al. (2014) and Djelantik et al. (2017), we found some evidence of differential class membership based on the nature of the loss. Specifically, the PGD/PTSD class was more likely to have lost a loved one following an accident, suicide or homicide than the Low group; however, this was no longer significant when PTCI variables were included in the model. These study differences most likely related to differences in the samples under investigation. LCA is a data determined statistical technique and so the extent to which sociodemographic and loss-related factors predict class membership will be impacted by the population under investigation. Only 20% of our sample had lost a loved one due to accident, suicide or homicide, half of which were due to an accident. It is important to note that strong conclusions regarding the relationship between sociodemographic factors and bereavement outcomes require prospective, population-based longitudinal studies (Lundorff et al., 2017; Maccallum et al., 2015; Nielsen et al., 2017). Nonetheless, our findings that negative self-beliefs independently predicted class membership, when accounting for sample-specific sociodemographic factors, including death characteristics, are consistent with proposals from cognitive models that appraisals play a key role in psychopathology following loss (Boelen et al., 2006b; Maccallum and Bryant, 2013).
There are limitations to the conclusions that can be drawn from this study. As noted LCA is a data-determined statistical approach. The analysis described in this paper was undertaken using a sample of heterogeneous bereaved individuals attending a major Sydney research and treatment clinic. A strength of our sample is that it does contain a large number of individuals with clinical impairment; however, it was characterised predominantly by females who had experienced a medical loss and so does not comprise a population-based representative sample of bereaved individuals. Accordingly, the extent to which findings generalise to other samples awaits further investigation. Also, the analysis was cross sectional in nature. On average, participants had experienced their loss 3½ years prior to assessment. Thus, it was not possible to determine the extent to which appraisals were a cause or consequence of the presence of PGD and PTSD symptoms. Finally, a limitation inherent in LCA is that it classifies individuals into discrete subclasses based on dichotomisation of constructs. An advantage of the approach is that it enables researchers to sort individuals into relatively homogeneous subgroups that are more similar to each other than other subgroups within a sample. In doing so, however, the technique reduces some sources of variation in the data (Bohnke and Croudace, 2015; Miettunen et al., 2016). There has been a recent proliferation in the development of techniques designed to explore patterns of heterogeneity, and each comes with its own limitations (Borsboom et al., 2016). The results of this study are consistent with theoretical models of PGD that highlight the importance of the self in understanding post-bereavement psychopathology. It is through the ongoing application of varied statistical approaches that further insights may be gained into the factors that promote and maintain loss-related symptomatology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was supported by grant 568970 from the National Health and Medical Research Council Program and grant 455341 from the National Health and Medical Research Council Project awarded to R.A.B. F.M. is supported by a National Health and Medical Research Council Early Career Research Fellowship (GNT1053997).