
Abstract
Objective:
People affected by schizophrenia spectrum disorders are at a higher risk of offending violently. This study aims to investigate risk factors in relation to the peri-diagnostic period and possible predictors of post-diagnostic violence of people diagnosed for the first time in the public mental health system.
Methods:
The study compared various risk factors for post-diagnostic violence in patients (n = 1453) diagnosed with a schizophrenia spectrum disorder. Patients were grouped according to the occurrence of peri-diagnostic violence. Of the 246 violent offenders, 164 committed their first offence pre-diagnosis. Mental health and criminological variables were evaluated across the lifespan (median age at end of follow-up = 34.22 years, range = 17.02–55.80 years).
Results:
Gender, employment, non-violent offending, family incidents, violent and non-violent victimisation, substance use, personality disorder, number of in-patient admissions and history of non-compliance differed significantly across violent and non-violent subgroups (all p ⩽ 0.01 and at least small effect size). More frequent and longer inpatient admissions were found in the violent subgroups (all p ⩽ 0.01). For the whole sample, sex, number of violent offences, non-violent offences, violent victimisation, substance use and number of inpatient admissions predicted post-diagnostic violence (χ2 (6) = 188.13, p < 0.001). Among patients with a history of pre-diagnostic violence, a history of non-violent offending in the 18-month period pre-diagnosis was the strongest predictor of future violence (odds ratio = 3.08, 95% confidence interval [1.32, 7.21]).
Conclusion:
At triage, violence risk assessment should consider the presence of antisocial behaviour and violent victimisation, substance use, male gender and frequency of inpatient admissions. Common treatment targets for the prevention of post-diagnostic violence include criminality and victimisation. Treatment of positive symptoms should be of greater emphasis for individuals without a history of pre-diagnostic violence.
Introduction
Schizophrenia spectrum disorders encompass syndromes such as schizophrenia, schizoaffective and delusional disorder, which share impairing psychopathology that impacts features of cognition, perception, emotion and behaviour. Among these, schizophrenia is the most prevalent disorder of the spectrum with average worldwide lifetime prevalence rates reported to be around 0.5% (American Psychiatric Association, 2013; Simeone et al., 2015). The current Australian and New Zealand clinical practice guidelines for the management of schizophrenia and related disorders state that individuals meeting diagnosis are at a higher risk of victimisation, suicide and offending violently (Galletly et al., 2016). Although this expert opinion is widely regarded, there is little homogeneity between studies reporting risk of violent offending and the causes for this phenomenon remain uncertain (Fazel et al., 2009). The heterogeneity of risk rates and treatment results appear to differ across subgroups of schizophrenia spectrum disorders (Douglas et al., 2009; Hodgins and Klein, 2017; Volavka and Citrome, 2011).
At least two trajectories appear to impact on the occurrence of violence among people with schizophrenia: one pertains to patients with no prior history of violence who begin engaging in aggressive behaviour at the onset of illness where positive symptoms are thought to explain violence and another with chronic criminogenic disposition who display antisocial and violent behaviour as early as childhood irrespective of mental state (Hodgins and Klein, 2017). Existing studies have tended to compare those with a history of violence, often offenders, to those without a history of violence after the onset of illness or before, but rarely a comprehensive consideration of both periods.
Research shows that approximately 85% of people with schizophrenia spectrum disorders have an onset of illness before age 45 years (McAlpine, 2003) with incidence rates and age of onset varying by specific psychotic disorder experienced (McGrath et al., 2016). Similar variability is reflected in the reported temporal relationship between illness onset and registered crimes. While a majority of males seem to offend before entering the mental health system (Munkner et al., 2003), some research has found that police have been called to intervene within the family in the first 5 years after the onset of psychosis (Onwumere et al., 2011) with considerable rates of severe physical assault (Chan, 2008). Accordingly, the time period before and after the first episode of psychosis remains of critical interest regarding elevated risk of violence in different circumstances (Large and Nielssen, 2011).
Besides diverging subgroups in relation to the onset of violence, and the fact that psychoses appear to have a moderate association with violence (Douglas et al., 2009; Fazel et al., 2009; Wallace et al., 2004), increased risk seems to be influenced by further mediators (Bo et al., 2011). In this context, several distal and proximal risk factors have been highlighted in past research regarding schizophrenia spectrum disorders and violent behaviour encompassed in a range of domains (e.g. socio-demography, psychopathology, mental health care, prior victimisation and comorbidity): male gender and younger age (Bo et al., 2011; Large and Nielssen, 2011), lower education and social living status (Bo et al., 2011; Large and Nielssen, 2011), positive symptoms, longer duration of untreated psychosis and younger age at onset of illness (Volavka and Citrome, 2011; Winsper et al., 2013), involuntary treatment or non-compliance (Large and Nielssen, 2011; Yee et al., 2011), experiences of physical and sexual abuse (Hodgins and Klein, 2017; Swanson et al., 2008b), substance use (Fazel et al., 2009; Ogloff et al., 2015; Volavka and Citrome, 2011; Winsper et al., 2013) and antisocial personality and psychopathy traits (Bo et al., 2011; Hodgins and Müller-Isberner, 2004; Tengström et al., 2001).
Several studies have focused on the efficacy of therapeutic efforts to reduce the risk of violence in schizophrenia spectrum disorders. What can be inferred from these findings is that mental health care can have a generally positive effect on the occurrence of future violent behaviour among people with schizophrenia spectrum disorders (Hodgins and Müller-Isberner, 2004; Keers et al., 2014). However, this effect can be diminished if the criminogenic range of factors relating to offending and violence are not adequately considered over time (Hodgins et al., 2009; Swanson et al., 2008a).
Violent offenders exhibiting pervasive antisocial conduct seem to require a different therapeutic approach compared to those without (Swanson et al., 2008b). Consistent with these assertions, Volavka and Citrome (2011) discerned two historical trajectories: namely, an acute risk cluster calling for pharmacotherapy and psychosocial treatment, and a chronic risk cluster needing criminal justice system interventions. For clinical practice, these results suggest a need to modify existing mental health therapeutic interventions to include interventions to address the criminogenic needs (i.e. characteristics, traits or issues of an individual that directly relate to the individual’s likelihood to re-offend and commit another crime) of the distinct subgroups of patients with a schizophrenia spectrum disorder for them to be effective in reducing violent behaviour (Hodgins et al., 2011). The aim of this study was to assess different patterns of violent and non-violent behaviour, preceding and following diagnosis, in a sample of people diagnosed with a schizophrenia spectrum disorder in the public mental health system. Specifically, the study evaluates the potential proximal and distal risk factors in relation to the peri-diagnostic period and post-diagnostic violence to better inform prevention strategies in mental health care. It was hypothesised that individuals with a higher number of criminogenic factors preceding a diagnosis would have a higher incidence of violent behaviour following a diagnosis, compared to those with a greater illness acuity and a low level of criminogenic factors.
Methods
Sample selection
This study compared various risk factors for pre- and post-diagnostic violence in patients diagnosed with a schizophrenia spectrum disorder in the public mental health system in the years 2000 and 2005. Following previous Victorian-based research (Short et al., 2013; Wallace et al., 2004), ‘schizophrenia spectrum disorder’ was broadly defined and included the various sub-types of schizophrenia, other chronic primary psychotic disorders including delusional disorder, shared psychotic disorder, schizoaffective disorder, paraphrenia and unspecified non-organic psychosis (International Classification of Diseases, 10th Edition [ICD-10] codes F20, F22, F24, F25, F28 and F29). Excluded were affective, organic, transient or drug-induced psychoses. Cases were included only if the diagnosis of a schizophrenia spectrum disorder was upheld on at least 75% of subsequent diagnoses or if there was a clear diagnostic progression to a schizophrenia spectrum disorder. Previous research employing this method of classification demonstrated good diagnostic reliability (Krupinski et al., 1982; Short et al., 2013). To account for possible insidious organic processes (i.e. from dementia), patients with an age of onset of illness above 45 years were excluded from further analysis. The two cohorts comprised 2439 patients (1020 females; 1419 males). After excluding those individuals who were either above the age of 45 years (n = 653) or diagnosed with affective or substance-induced psychoses (n = 333), the final sample comprised 1453 patients.
Data sources and case linkage
Each patient’s psychiatric history was extracted from the Victorian Psychiatric Case Register (VPCR), a statewide register that records the date and nature of all contacts with the public mental health system. Psychiatrists record diagnoses according to the ICD (World Health Organization, 1977), typically at the time of a patient’s discharge from hospital or within 1 month of admission. The VPCR provides excellent data on psychotic disorders, but is less comprehensive for higher prevalence non-psychotic conditions such as substance abuse and personality disorders (Short et al., 2013), most of which are treated by private practitioners. In contrast, virtually everyone with schizophrenia is seen in the public mental health system. Recorded entries on the VPCR were linked through a multistage deterministic-probabilistic approach with those on the Law Enforcement Assistance Program (LEAP), a statewide register that records information on an individual’s contacts with Victoria Police. Where applicable, patients’ dates of death were ascertained through the state Registry of Births, Deaths and Marriages. Mental health and police records were extracted on 19 June 2009 and 13 January 2010, respectively.
Coding of socio-demographic, police, and mental health records, and subgroups
Socio-demographic information was obtained from the VPCR and reflected those details known at the time of the most recent registration with mental health services and were characterised as follows: highest level of education (less and equal to or greater than 12 years of education), employment status (currently employed or unemployed), marital status (married including de facto or not married), accommodation status (stable accommodation or unstable accommodation, that is, homeless or living in hostels), and living status (living alone or with others).
Police records were coded according to the number and type of offences and incidents of victimizations. Incidents of offending and victimisation were assessed as ‘violent’ (any incident involving physical contact or harm to the respective victim, including all assaults and sexual violence, including contact sex offences) or ‘non-violent’ (all other incidents which do not imply physical contact with the respective victim, that is, property offences, threats and non-contact sex offences). Repeated violent offending in the respective peri-diagnostic period was defined as committing two or more violent offences as opposed to singular violent offending. Family incidents (ranging from disputes to physical conflicts) necessitating police involvement were categorised in temporal relationship to the first diagnosis of schizophrenia spectrum disorder and included in the study if the individual was primarily the perpetrator of the family conflict.
Mental health histories were coded according to the presence and type of psychiatric diagnosis (including mostly Cluster B personality disorders and any substance abuse or substance-induced disorders, excluding tobacco- and caffeine-related disorders). Number of admissions, duration of care and incidents of non-compliance (i.e. failure to act in accordance with advice from health care providers) in general and in temporal relation to diagnosis were obtained from mental health records and coded accordingly.
In relationship to the peri-diagnostic period, individuals were coded as ‘non-violent’ (not charged for violent offences at any time), ‘violent pre-diagnosis’ (charged for violent offences before [and possibly after] diagnosis of a schizophrenia spectrum disorder) and ‘violent post-diagnosis’ (charged for violent offences only following diagnosis of schizophrenia spectrum disorder). Time-at-risk was calculated in relation to the respective time period (number of days between date of birth and the date of extraction for mental health data; number of days between the patient’s 10th birthday [age of criminal responsibility in Victoria] and date of extraction for offending data, excluding periods of inpatient care). Since dates of imprisonment were not known, the periods of incarceration could not be excluded from the analysis.
Ethics and statistical analysis
Ethical approval for this study was obtained from the Ethics Committees of the Victoria Police, Monash University, and the Department of Human Services given on the basis that all identifying data were removed once the police and mental health data had been linked. At no point did the researcher have access to identified data from any of the data sources and made use of a unique study identifier.
Data were analysed using the Statistical Package for the Social Sciences (SPSS), version 23.0. The analysis of independence of categorical variables was performed using Pearson’s chi-square test. In case of association, the effect size of the relationship was calculated using Cramer’s V. Population proportions were estimated using adjusted Wald 95% confidence intervals (95% CIs). As the assumptions of normality and/or equal variance were violated or means were heavily influenced by outliers, Mann–Whitney or Kruskal–Wallis with pairwise comparisons and adjusted p-values tests were used to test for differences between groups. Effect sizes for significant differences were calculated based on respective comparisons. Based on the results of the univariate analyses for subgroup differences compared to the non-violent subgroup, variables were included in a backward stepwise (likelihood ratio) logistic regression analysis for post-diagnostic violent offending, if they were significant and had at least a small effect size of 0.1 or above. In case of several variables of a domain meeting these assumptions, risk factors were selected before others in the domain in temporal relation to the date of primary diagnosis as follows: risk factors in the 18-month period preceding diagnosis were selected first, then during time-at-risk preceding diagnosis and last variables with a general history of the domain (total time-at-risk). For analysis of the whole sample and violent pre-diagnosis subgroup, the number of violent offences in the 18-month period preceding diagnosis was to be included additionally according to the literature (Bonta et al., 1998). The most parsimonious model was chosen from the results of the logistic regression analysis using log-likelihood comparisons following Hosmer et al. (2013).
All tests were two-tailed. To account for multiple comparisons in the characteristic domains, non-parametric tests were chosen before parametric tests, and results were regarded only significant when below 1% alpha level (i.e. p < 0.01) and having effect sizes above 0.1. Otherwise a significance level of 5% was chosen (significance of risk factors in logistic regression, Mann–Whitney U tests).
Results
The median age at first diagnosis of the schizophrenia spectrum sample was 27.27 years (range = 12.11–45.97 years) and showed a positively skewed distribution with a median age at end of follow-up of 34.22 years (range = 17.02–55.80 years, bimodal distribution). Median overall time-at-risk was 24.01 years (interquartile range [IQR] = 12.07 years, bimodal distribution) and the median post-diagnostic time-at-risk was 4.93 years (IQR = 4.99 years, bimodal distribution). The sample contained more males (n = 985, 67.8%). The majority of the sample had not completed 12 years of education (n = 890, 61.3%), was not married (n = 1150, 79.1%), was unemployed (n = 953, 65.6%) and living with others (n = 1037, 71.4%) in stable accommodation (n = 1311, 90.2%). Almost one-third (31.9%, n = 464) of the sample had a comorbid diagnosis of substance use, 8.8% (n = 128) were additionally diagnosed with a personality disorder and 21.5% (n = 313) had a history of non-compliance in the public mental health system. Of the whole sample, 11.3% had offended violently before the primary diagnosis (i.e. violent pre-diagnosis subgroup, n = 164, 95% CI [9.8%, 13.0%]), Of the individuals who were not charged for a violent offence before the time point of the primary diagnosis, 6.4% (i.e. violent post-diagnosis subgroup, n = 82, 95% CI [5.2%, 7.8%]) acted violently after the diagnosis.
Significant relationships on cohort subgroup level with at least small effect size were observed in the variables gender, employment, non-violent offending, family incidents, violent and non-violent victimisation, substance use, personality disorder, number of inpatient admissions and history of non-compliance. Higher respective proportions of inpatient admissions and median duration of admissions were found in the violent subgroups. The socio-demographic, offending, victimisation and mental health characteristics are presented in Table 1.
Comparisons of cohort subgroups in relation to peri-diagnostic period – domains overview.
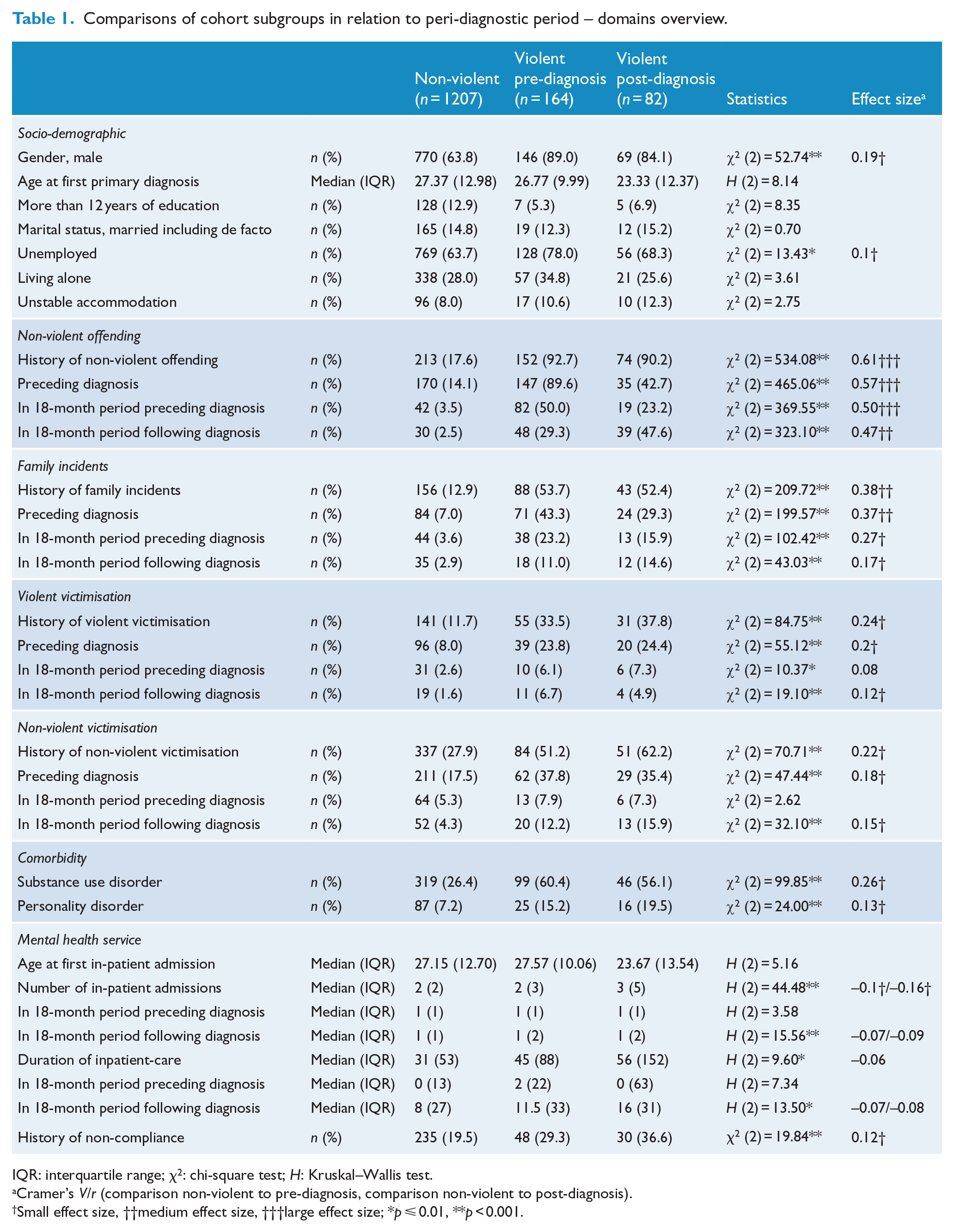
IQR: interquartile range; χ2: chi-square test; H: Kruskal–Wallis test.
Cramer’s V/r (comparison non-violent to pre-diagnosis, comparison non-violent to post-diagnosis).
Small effect size, ††medium effect size, †††large effect size; *p ⩽ 0.01, **p < 0.001.
Violent offending relating to the peri-diagnostic period
Median time-at-risk following diagnosis for the violent post-diagnosis subgroup was 8.21 years (IQR, 4.86 years) compared to 4.71 years (IQR, 4.96 years) for the prior diagnosis subgroup; however, this difference was not significant (U = 7733.0, p = 0.055). Of the individuals who were violent prior to diagnosis, 27.4% (n = 45, 95% CI [21.2%, 34.7%]) recidivated violently following their diagnosis of a schizophrenia form disorder. The rate of violent offending in 3-month intervals, calculated as incidence per 365 days, for the two subgroups with a violent criminal charge pre- and post-diagnosis is shown in Figure 1.
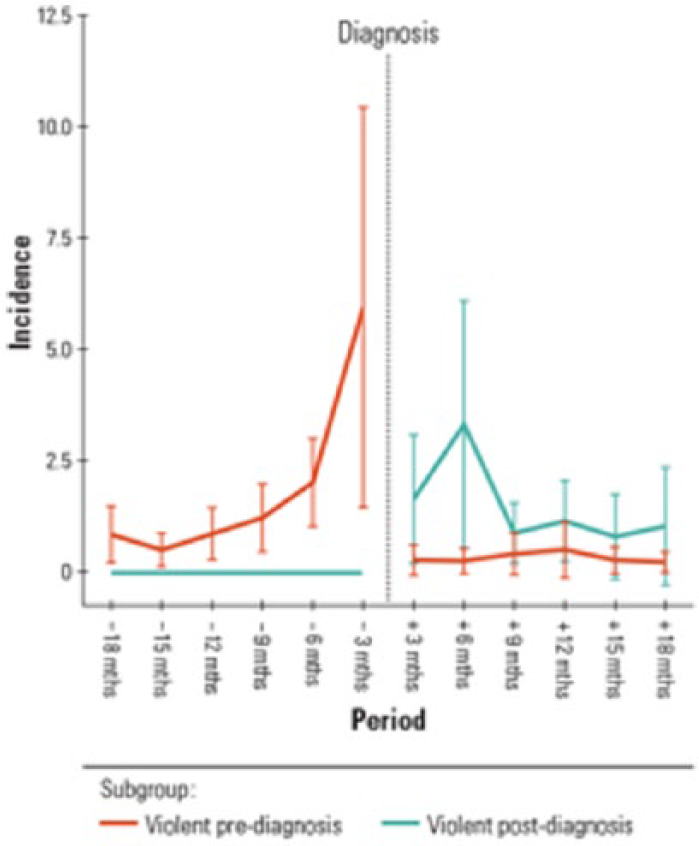
Incidence of violent charges per 365 days in 3-month periods pre- and post-diagnosis.
In the 18 months following diagnosis, the violent post-diagnosis subgroup (mean rank = 147.7, median = 0, IQR = 2) committed violence more frequently than the violent pre-diagnosis subgroup (mean rank = 111.4, median = 0, IQR = 0) and a Mann–Whitney test found this difference to be statistically significant (U = 8708.0, p < 0.001) with a medium effect size (r = 0.33). This result was confirmed for the entire post-diagnostic time-at-risk (violent post-diagnosis subgroup mean rank = 178.1, median = 3, IQR = 5 vs violent pre-diagnosis subgroup mean rank = 96.2, median = 0, IQR = 1, U = 11,200.0, p < 0.001) with a large effect size (r = 0.58).
The violent pre-diagnosis subgroup was less likely to have committed only singular violent offences (n = 30, 18.3%, 95% CI [13.1%, 25.0%]). Following diagnosis, the majority of the violent post-diagnosis subgroup (n = 64, 78.0%, 95% CI [67.9%, 85.7%]), as well as the majority of the re-offenders of the violent pre-diagnosis subgroup (n = 40, 88.9%, 95% CI [76.1%, 95.6%]), offended violently on two or more occasions. The minority of perpetrators offended violently in the 18-month period preceding diagnosis (n = 69, 42.1%, 95% CI [34.8%, 49.7%]). This was also observed in the violent post-diagnosis subgroup and the respective 18-month period (n = 34, 41.4%, 95% CI [31.4%, 52.3%]). Affiliation of subgroup was significantly related to categorical frequency of violent offending in the 18-month period following diagnosis (χ2 = 27.43, p < 0.001) with a medium effect size (Cramer’s V = 0.33); the post-diagnostic offenders had a higher proportion of singular and repeat violent offences (41.5% vs 12.2%). There was no significant association between categorical frequency of violent offending and subgroup affiliation when the non-violent proportion was disregarded. See Table 2 for details including estimated population proportions using Wald adjusted 95% CIs.
Frequencies of violent offending in respective peri-diagnostic period.
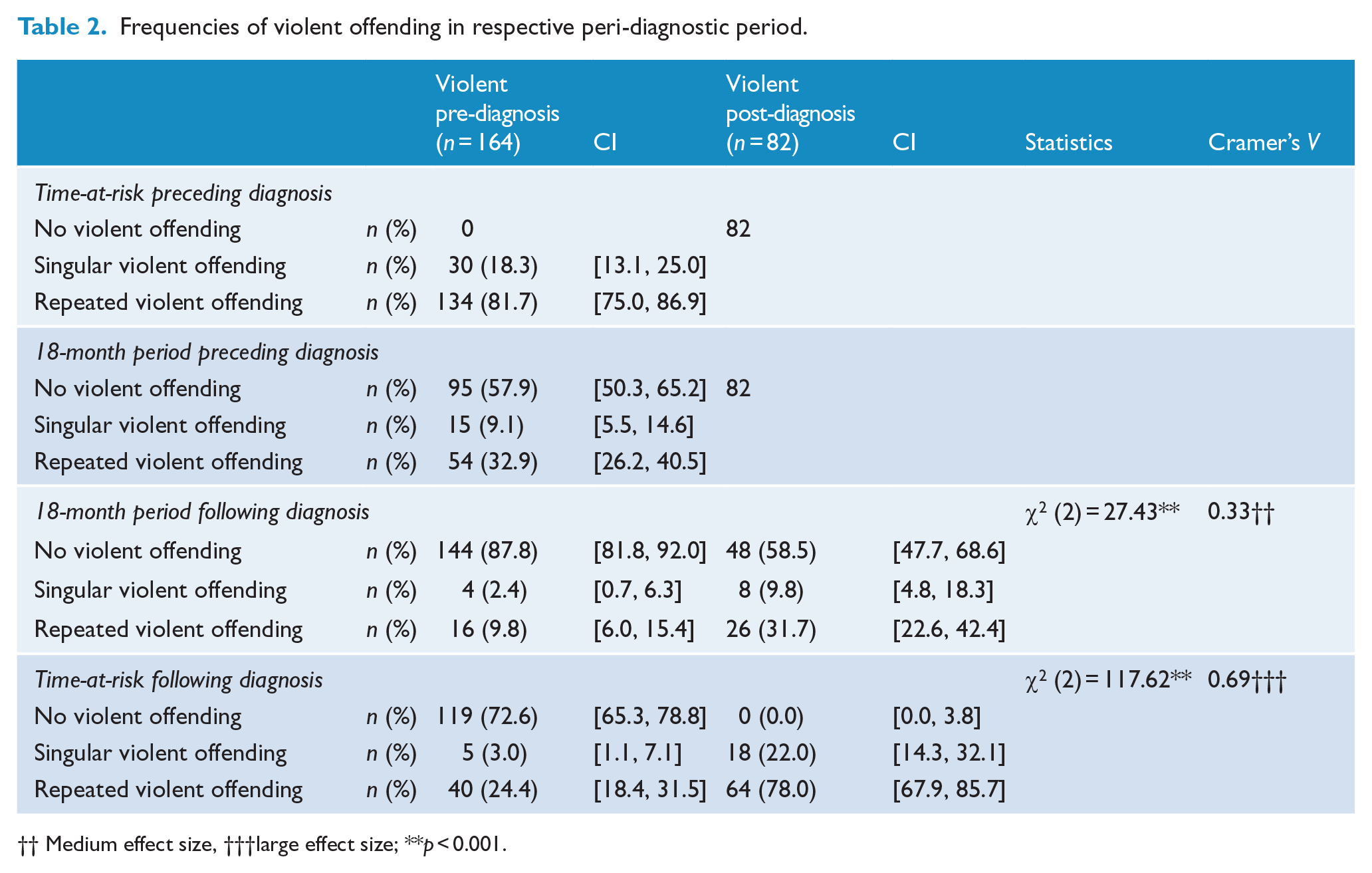
Medium effect size, †††large effect size; **p < 0.001.
Risk factor modelling of future violence following diagnosis
According to the predefined inclusion criteria and procedure, the following independent variables were included in the respective multivariate logistic regression model, based on the results of the univariate analyses: sex, employment status, non-violent offending in 18-month period preceding diagnosis, family incidents in 18-month period preceding diagnosis, violent victimisation preceding diagnosis, non-violent victimisation preceding diagnosis, personality disorder, substance use disorder, number of inpatient admissions and history of non-compliance.
Risk factor modelling of future violence irrespective of offender status (whole sample)
After six backward steps, the final model using sex, number of violent offences, non-violent offences, violent victimisation, substance use and number of inpatient admissions as risk factors was significant (χ2 (6) = 188.13, p < 0.001). The Hosmer–Lemeshow goodness-of-fit test for the final model was non-significant (χ2 (8) = 14.25, p = 0.076), suggesting the model is a good fit for the current data. The model as a whole explained 27% of variance in the violent group (Nagelkerke R2 = 0.27). In total, 19.7% (95% CI [13.2%, 27.7%]) of those violent post-diagnosis were correctly predicted as such (sensitivity), while 99.1% (95% CI [98.4%, 99.5%]) of those non-violent were correctly predicted as such (specificity). The positive predictive value (PPV) was 67.6% (95% CI [51.8%, 80.1%]), and the negative predictive value (NPV) was 92.8% (95% CI [92.2%, 93.4%]). As shown in Table 3, all independent variables contributed significantly to the model. The strongest risk factor for future violent offending was a history of non-violent offending in the 18-month period preceding diagnosis (odds ratio [OR] = 4.43, 95% CI [2.70, 7.29]). Every additional violent offence in that period increased the likelihood of violent offending by 14% as did every additional inpatient admission by 19%, controlling for other factors in the model.
Logistic regression model for post-diagnostic violence.
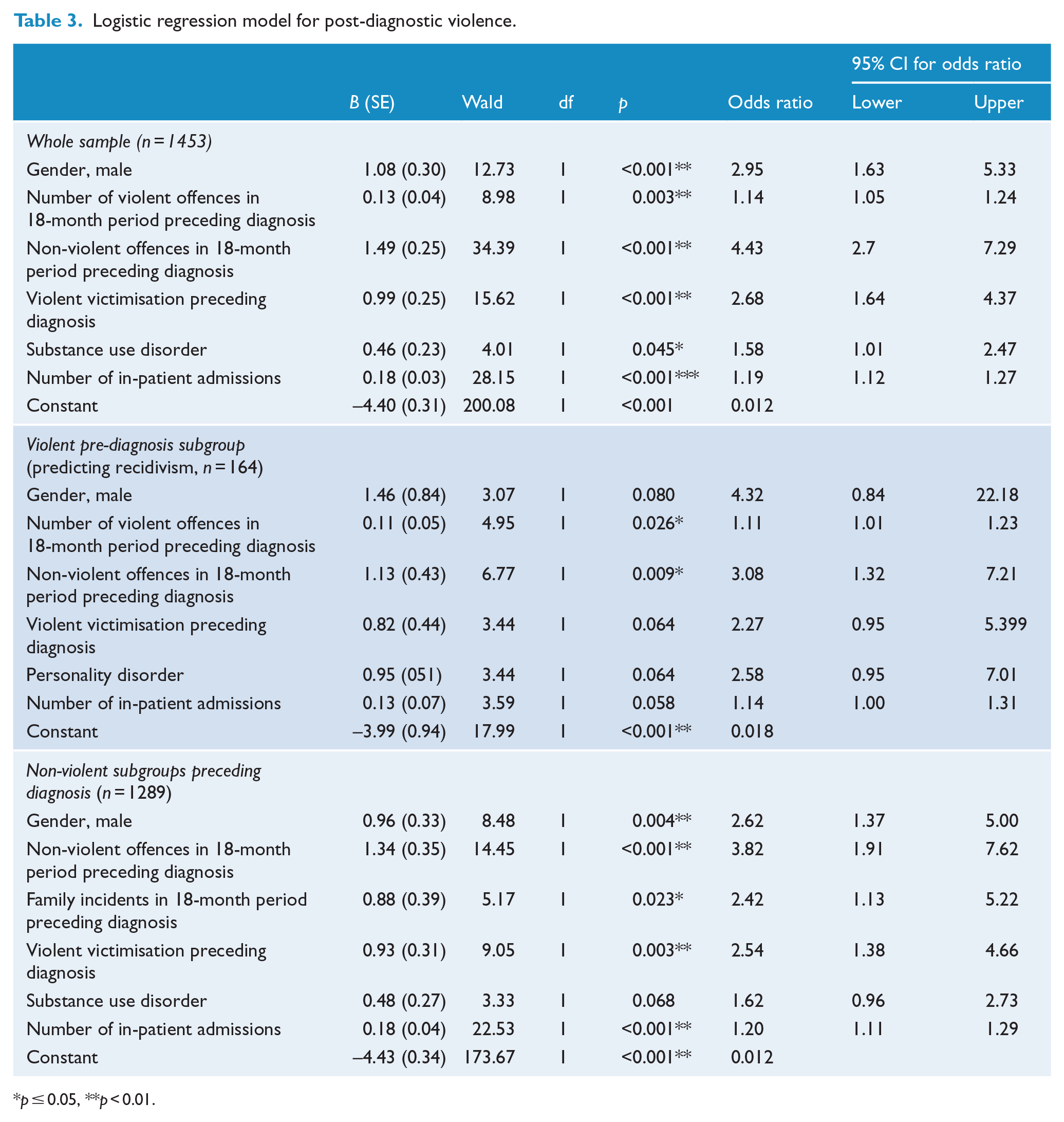
p ⩽ 0.05, **p < 0.01.
Risk factor modelling of violent recidivism in the violent pre-diagnosis subgroup.
After five backward steps, the final model using sex, non-violent offences, family violent victimisation, personality disorder and number of inpatient admissions as risk factors was significant (χ2 (6) = 33.10, p < 0.001). The Hosmer–Lemeshow goodness-of-fit test for the final model was non-significant (χ2 (8) = 11.43, p = 0.179), suggesting the model is a good fit for the current data. The model as a whole explained 27% of variance in the violent group (Nagelkerke R2 = 0.26) and had a sensitivity of 15.2% (95% CI [9.5%, 22.4%]), a specificity of 78.1% (95% CI [60.0%, 90.7%]), PPV of 74.1% (95% CI [57.0%, 86.1%]) and NPV of 18.3% (95% CI [15.5%, 21.4%]). As shown in Table 3, only two of the independent variables contributed significantly to the model. The strongest risk factor for future violent offending was a history of non-violent offending in the 18-month period preceding diagnosis (OR = 3.08, 95% CI [1.32, 7.21]). Every additional violent offence in that period increased the likelihood to recidivate violently by 11%, controlling for other factors in the model.
Risk factor modelling of future violence in the non-violent pre-diagnosis subgroups
After five backward steps, the final model using sex, non-violent offences, family incidents, violent victimisation, substance use disorder and number of inpatient admissions as risk factors was significant (χ2 (6) = 107.31, p < 0.001). The Hosmer–Lemeshow goodness-of-fit test for the final model was non-significant (χ2 (7) = 5.82, p = 0.561), suggesting the model is a good fit for the current data. The model as a whole explained 21% of variance in the violent group (Nagelkerke R2 = 0.21) and had a sensitivity of 0.7% (95% CI [0.3%, 1.3%]), a specificity of 94.9% (95% CI [87.4%, 98.6%]), PPV of 66.7% (95% CI [38.1%, 86.7%]) and NPV of 5.8% (95% CI [5.5%, 6.1%]). As shown in Table 3, only five of the independent variables made a unique statistically significant contribution to the model. The strongest risk factor for future violent offending was a history of non-violent offending in the 18-month period preceding diagnosis, recording an OR of 3.82. Every additional inpatient admission increased the likelihood of post-diagnostic violence by 20%, controlling for other factors in the model.
Discussion
This study analysed officially recorded rates of violent behaviour within a large sample of persons diagnosed for the first time with schizophrenia spectrum disorder with an overall median time-at-risk over 34 years and post-diagnostic period of 5 years. Possible risk factors of violence were compared across three subgroups generated by the presence of violence in relation to the peri-diagnostic period.
Consistent with past research, the majority of individuals with a schizophrenia spectrum disorder who had been charged with a violent offence engaged in violent offending before their first diagnosis (Hodgins and Müller-Isberner, 2004; Munkner et al., 2003). The majority of patients did not act violently before or after diagnosis (approximately 85%). Of those who had engaged in violent behaviour (i.e. 1 in 6), approximately 60% had acted violently before receiving a diagnosis of a schizophrenia spectrum disorder. These proportions are similar to previous meta-analytic findings regarding more serious violence (Large and Nielssen, 2011). Suggesting that while the impact of the violence some individuals experiencing a schizophrenia spectrum disorder engage in can be dramatic, a relatively small proportion of patients pose this risk. In turn, attempts at identifying and intensively intervening with this small proportion could be manageable and cost-effective for resource poor mental health services.
As hypothesised, violent and non-violent people with a schizophrenia spectrum disorder differed significantly on characteristics in several domains, particularly those known to be associated with criminal behaviour (i.e. criminogenic factors). Male gender and unemployment were more prevalent in the violent subgroups, moderating factors already reported in past literature (Bo et al., 2011; Large and Nielssen, 2011; Munkner et al., 2009). Non-violent offending was significantly lower in the non-violent group both before and after the diagnosis, pointing to the important relationship between more general criminal/antisocial behaviour and violence (Hodgins and Klein, 2017; Winsper et al., 2013). If family incidents are to be interpreted as a form of violent behaviour in the social proximity, family conflicts which necessitate police contact might be considered precursors of future more general violent behaviour. This interpretation is supported in this study with lower rates of family incidents in the non-violent group compared to both violent subgroups.
Consistent with prior studies, violent victimisation was less frequent in the non-violent group, mirroring the violent offending-violent victimisation overlap among mentally disordered individuals (Silver et al., 2011). The proportion of violent victimisation is comparable to individuals found elsewhere to be at-risk for psychosis (Purcell et al., 2015). Victimisation in this context is more likely to take place before diagnosis. Therapeutic interventions might therefore have a similar positive effect on violent offending and on future victimisation (Hodgins and Müller-Isberner, 2004; Keers et al., 2014). Comorbidity in the form of personality disorder and substance use disorder is less frequent in the non-violent subgroup, which underlines the importance of these risk factors for violence (Fazel et al., 2009; Volavka and Citrome, 2011). Mental health service utilisation (number of admissions and duration of inpatient care) and compliance (although with relatively small effect sizes) are less burdened in the non-violent group, possibly indicating a lesser load of psychopathology in comparison to the violent subgroups or a more likely inpatient care for individuals with a higher risk profile.
The comparison of the violent subgroups preceding and following diagnosis partially replicated past findings. The proportion of unemployment in the violent pre-diagnosis subgroup was even higher (more than 75%) than for those in the post-diagnosis violent subgroups. This suggests lower levels of social functioning possibly explained by higher degrees of antisocial traits. It was perhaps surprising that the violent post-diagnosis subgroup showed generally similar rates of personality disorder and substance use disorder as the pre-diagnosis group. Nonetheless, adverse outcome characteristics, including non-violent offending, family incidents and victimisation events were reported less frequently prior to the diagnosis, but generally increased after diagnosis. These findings suggest a crucial effect of positive psychotic symptoms in this subgroup as described in previous pathway models (Volavka and Citrome, 2011; Winsper et al., 2013). Further indirect indicators of a more severe course of the disorder in the violent post-diagnosis subgroup include higher numbers of admissions, higher rates of non-compliance and longer durations of inpatient care against the background of a high likelihood of substance use and/or unfavourable personality traits. The result that the frequency of violent offending was higher for the violent post-diagnostic subgroup close to the time of diagnosis might be indicative of a stronger impact of illness onset. Of note, the majority of individuals of both subgroups acted violently repeatedly (i.e. higher numbers of violent offending were not primarily caused by singular offenders).
For the clinician treating individuals with recently diagnosed schizophrenia spectrum disorder, knowing the chance of future violence at the point in time of diagnosis is of relevant interest. Different independent variables made a significant contribution to the respective risk factor modelling of post-diagnostic violence depending on the examined cohort. Taking all patients receiving a schizophrenia spectrum diagnosis, six variables predicted future violence with non-violent offending close to the diagnosis and male gender having the most impact, while frequent inpatient admissions or violent offences preceding diagnosis raised chances of violent offending accordingly. Antisocial behaviour has a known relationship to violence (Volavka and Citrome, 2011; Winsper et al., 2013), and more violence is reported in male gender and samples with more severe positive symptoms (Bo et al., 2011; Large and Nielssen, 2011). Substance use and violent victimisation before diagnosis contribute a considerable impact on odds of acting violently (Fazel et al., 2009; Purcell et al., 2015). To reduce chances of violent victimisation, treatment in general should therefore address positive symptomatology, substance use and criminal behaviour.
When treating a known violent offender, violence following diagnosis can be predicted by non-violent offending and high frequency of violent offending close to the diagnosis. These findings are in line with Bo et al. (2011) and Volavka and Citrome (2011), who report of the primary concern of general antisocial behaviour for offending violently. In this subgroup, while contributing to the regression model, male gender, violent victimisation, personality disorder and number of admissions no longer significantly predicted post-diagnostic violence. Obvious treatment targets to reduce future violent offending for this subgroup necessarily include antisocial behaviours, including non-violent offending most likely in a constellation of a male frequent user of inpatient admissions with personality disorder and risk of victimisation.
In individuals who have no history of charges of violent offences, but higher odds for future violent behaviour are similar to the general regression model. Instead of violent offences in the past, family incidents act as a substitute predictor while substance use is not distinguishing significantly between future violent offender and non-offenders. Clinicians should further be aware of non-violent offences and violent victimisation preceding diagnosis, and repeat inpatient admissions. For the non-violent cohort before diagnosis in order to prevent future violence, treatment should therefore focus on positive symptomatology, criminal behaviour, family interventions and strategies to reduce chances of violent victimisation.
Limitations
The nature of the data collection limits the generalisability of some results. As sequential information of onset of substance use was missing, the precise temporal relationship between the influence of substance use and psychopathology on violent offending could not be determined. As a consequence, the offence trajectory remains unclear. It could be that substance use is present before the primary diagnosis and thus increases risk earlier on. Or conversely, the full onset of the illness may trigger a downward spiral through which substance use is acquired and leads then to a potentiating effect on violence. Furthermore, the rates of personality disorders and substance use disorders are likely to be under-represented and might therefore be of more importance in the prediction of violence than suggested by the prediction models. Most likely, though, the rates are equivalently diminished in the defined subgroups and the relative effect of substance misuse and personality disorder should be reflected accurately. Types of personality disorder were not differentiated further although the majority consisted of Cluster B personalities. A major limitation is the lack of data on the effects of any treatment on the dependent outcome violence post-diagnosis. Regarding the prediction of violence, it is possible that our use of backward stepwise regression led to an optimistic model due to overfitting. However, this bias is reduced as sample size increases (Austin, 2008). In such cases, it can be useful for prediction (Tabachnick et al., 2013). Furthermore, the low base rate of violent offending post-diagnostic led to a reduced sensitivity of the prediction model overall.
Conclusion
Violent schizophrenic offenders can be identified using ‘easily available’ public health information preceding and following diagnosis. Different onsets of violent behaviour in subgroups of people with schizophrenia spectrum disorder were reconfirmed with the majority of violent perpetrators offending before diagnosis. Over time, rising rates of adverse outcomes (non-violent offending, family incidents) in individuals with substance use and unfavourable personality traits were observed. People offending violently following diagnosis did so more often than the other subgroups and had a higher number of inpatient admissions. The treating clinician seeing recently diagnosed schizophrenia spectrum disorder clients could triage patients into different risk bands regarding future violence. When risk factors are absent, the likelihood of future violence is low. However, when the identified risk factors are present, a more comprehensive assessment for violence, using a validated measure such as the HCR-20 V3 (Douglas et al., 2013), would be warranted. A general triage would emphasise on violent and non-violent antisocial behaviour and violent victimisation before diagnosis, substance use, male gender and frequency of inpatient admissions. In non-violent individuals before diagnosis family incidents are a further substitute for violent offending. In known violent offenders, antisocial behaviours before the diagnosis are the most relevant predictors of future violence.
Footnotes
Acknowledgements
The authors wish to thank Stephanie Louise, Swinburne University of Technology, for her valuable input.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.