
Abstract

Introduction
Children can develop posttraumatic stress disorder (PTSD) after getting exposed to a variety of traumatic events, including motor vehicle accidents, interpersonal violence and sexual abuse.
The diagnosis of PTSD in children is almost isomorphic to the adult PTSD criteria with matching symptom profile. There is ample evidence to recommend cognitive therapy as an effective intervention for PTSD in children. (Cohen et al., 2004; Deblinger et al., 1999). Most of these randomized controlled trials include children and adolescents of varying age groups, making extrapolation of the results to developmentally lower age group children difficult (the mean age of children studied was 14 ± 2 years). There are case reports of using cognitive therapy for young children with a 12-session manualized program (Scheeringa et al., 2007). But there is an unanswered question whether the same protocol is universally applicable. The cognitive therapy delivered to children differs greatly based on child’s level of cognitive maturity and their comprehension ability. Doing cognitive therapy for younger children is a challenging task. Here, we report a successful imagery-based cognitive therapy outcome in a 6-year-old child who developed PTSD following a fatal incident.
Case description
A 6-year-old male child was referred to psychiatry OPD with history of physical abuse and a ligature mark around the neck. During the interview, he revealed that one of his relatives tried to strangulate him using a cord at school. His father reported that he found his son lying on the floor with froth in mouth and generalized tonic clonic seizures (probably precipitated by hypoxic state resulting from strangulation). He was then admitted in pediatric intensive care unit (ICU) and had good recovery from physical trauma. The child presented to psychiatry OPD with symptoms of difficulty falling asleep, fear that he may be abused again, fear to get back to school. At the time of evaluation, the child was intensely anxious, got vivid images of the traumatic incident flashed before him as he recalled the event. He repeatedly pleaded his father to save him from future anticipated harm, seeking short-term solace. His symptoms qualified for PTSD according to International Classification of Disease, 10th Revision, Diagnostic Criteria for Research (ICD-10-DCR). We planned to intervene his psychological trauma using cognitive therapy in an imagery-focused method with the aid of Play-based techniques. Psychotropic medications were not prescribed. The child’s pre-therapy score on Child PTSD symptom scale was 26. The cut-off score of clinical significance is 12.
The initial session was initiated by introducing different toys and games to establish rapport and engage the child in therapeutic process. Second session was directed toward establishing base line character description for imagery-based therapy. The therapy was directed toward character stabilization and to target hotspots of traumatic memories that infuse strong distress. In this session, super hero ‘bheem’ was chosen for role-play (child could easily relate with the character). The role-play consisted of different characters—strong and brave person, wise person (adult figure), negative character and supportive roles. Situations relevant to the child’s milieu were chosen for the role-play.
In the subsequent session, the therapist followed the child’s lead during the role-play and focused on creating resilience and adopting a winning role. The session also focused on the activity ‘party hat on the monster’ in which he was asked to draw a nice and scary figure and turn the scary art into fun art. In the next session, he was asked to draw his favorite person which helped in establishing nurturer image. In pretend play, he took the role of a strong person and a safe place was created for him.
The closing session was used for transition from traumatic victimized stage to a healthy survivor stage. He was initially asked to pictorially represent the trauma. Then the same situation was enacted in the role-play. Few hotspots were observed. In vivo exposure was attempted by adding new events and aspects in the memory of the trauma. Then, imagery was used to relive and alter the experience. He was asked to use the techniques learned to apply for the problems as and when they occur.
At the end of the therapy, ‘blue print’ was developed for the child. Set of strategies like bubble breathing, imagery technique, support from nurturer and focusing on inner strength were framed. Parents were educated on using the technique to deal with possible setbacks.
The final score on Child PTSD symptom scale (post therapy) is 6 (see Figure 1) and the total number of sessions offered was 5. The child remains symptom free during follow-up evaluation (over a period of 2 months), attends school regularly and performs adequately in academics.
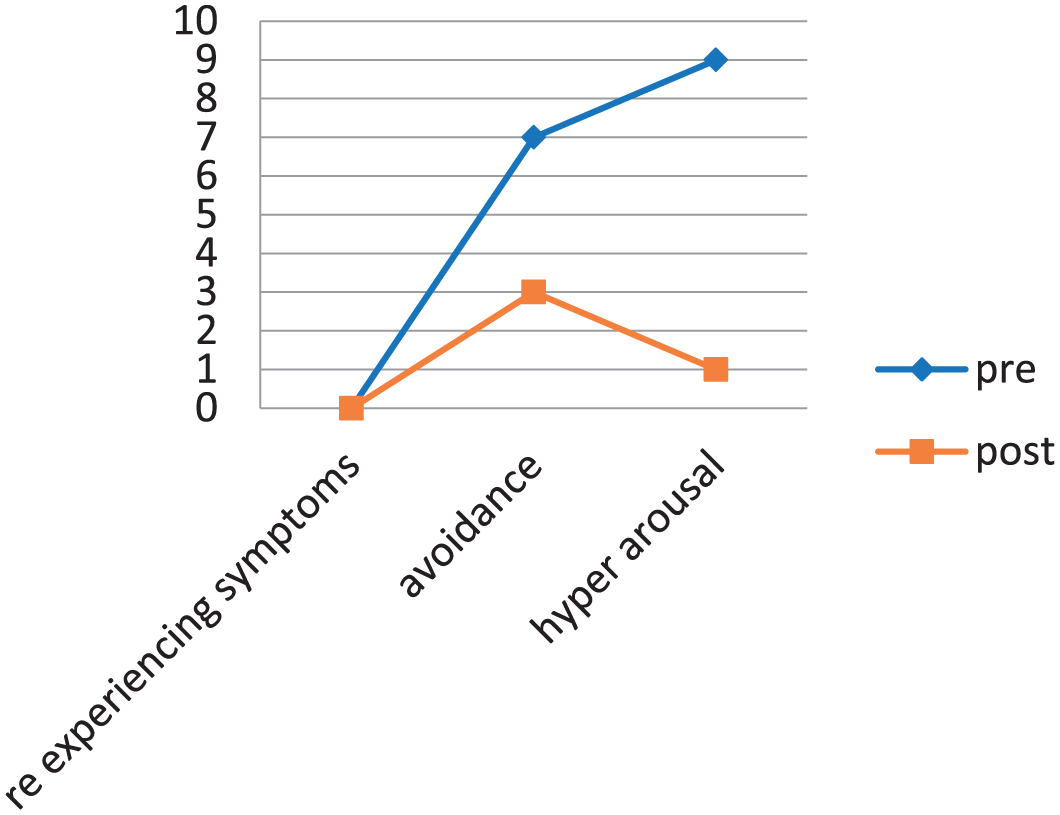
Graphical representation of pre- and post-therapy assessment.
Discussion
Clinical presentation of single-incident traumas differs from experience of repeated traumas. Hence, they can be managed with brief therapeutic programs instead of highly specialized cognitive behavioral therapy (CBT) protocols (Feeny et al., 2004). In the various studies involving cognitive therapy for childhood PTSD, a variety of different methods within the realm of CBT have been used, and the critical elements within the treatment remains elusive because children occupy a distinct position in tailor-made therapy by virtue of highly variable and developing cognitive structures. Imagery-based cognitive therapy offers simple ways of handling the cognitive disturbances of PTSD that is comprehensible by a child who is so young to understand other cognition-based interventions. Four groups of factors are considered to moderate a child’s short-term reaction to a trauma. These include (a) proximal trauma reminders (e.g. internal and external cues, physiological excitability); (b) proximal secondary stresses (e.g. changes in family dynamics and societal approach following the incident); (c) the ‘ecology’ of child (parental, peer group and school factors); and (d) factors intrinsic to child’s psychological makeup (genetic vulnerability and developmental acquisitions). The therapy specifically addressed the proximal trauma reminders and the child was equipped to handle the ‘Hot spots’ (memories that elicit strong emotions; Meiser-Stedman, 2002). This report demonstrates that child’s developmental age is an important factor that decides the selection of appropriate cognitive technique and means of delivering it for optimum response.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.